
The Effect of 12-Weeks Recreational Football (Soccer) for Health Intervention on Functional Movement in Older Adults
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
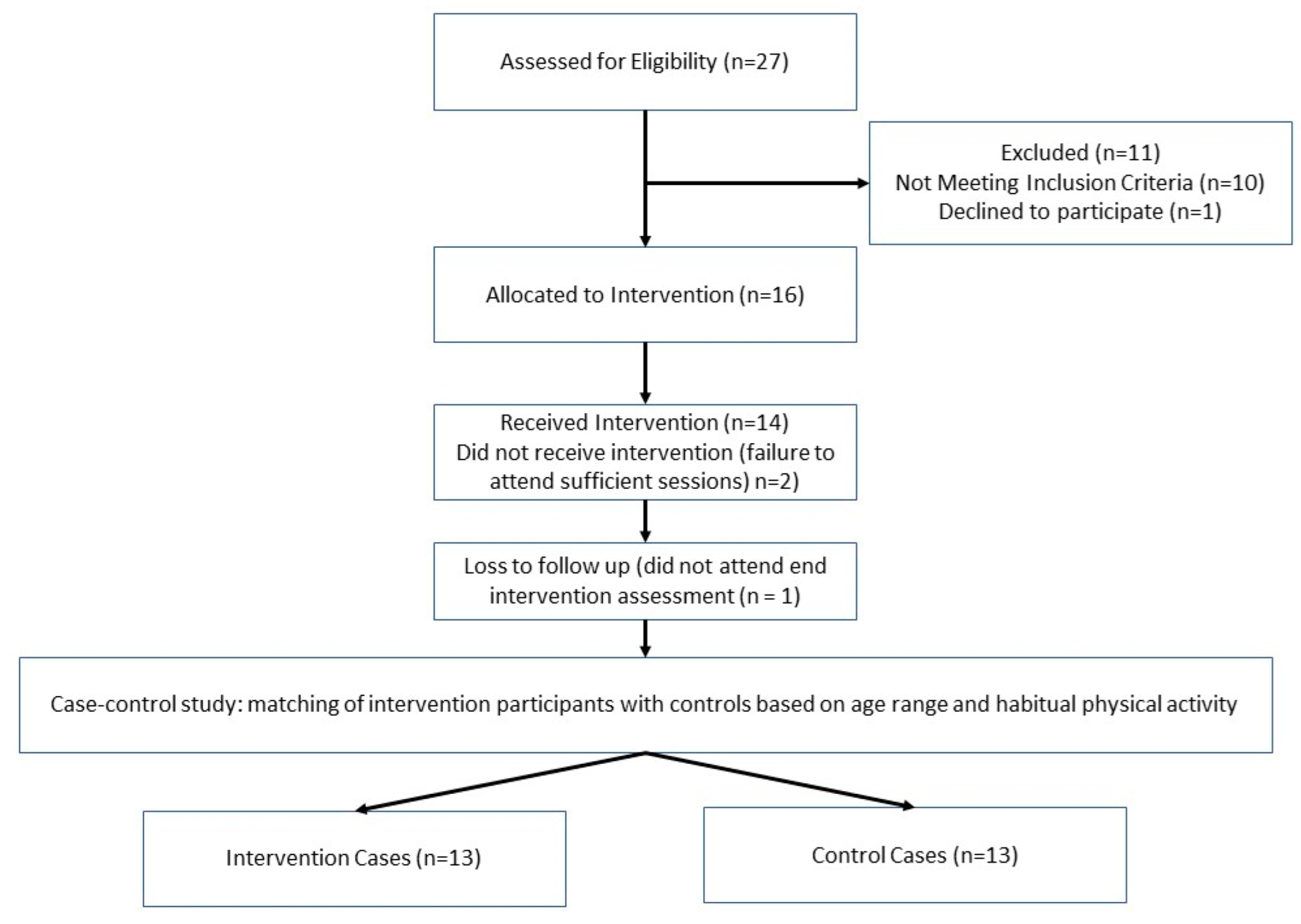
2.1. Participants
2.2. Procedure
2.2.1. Assessment of Functional Movement
2.2.2. Recreational Football for Health Intervention
2.2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krustrup, P.; Parnell, D. Football as Medicine: Prescribing Football for Global Health Promotion; Routledge: London, UK, 2019. [Google Scholar]
- Krustrup, P.; Christensen, J.F.; Randers, M.B.; Pedersen, H.; Sundstrup, E.; Jakobsen, M.D.; Krustrup, B.R.; Nielsen, J.J.; Suetta, C.; Nybo, L.; et al. Muscle adaptations and performance enhancements of soccer training for untrained men. Eur. J. Appl. Physiol. 2010, 108, 1247–1258. [Google Scholar] [CrossRef] [PubMed]
- Krustrup, P.; Dvorak, J.; Junge, A.; Bangsbo, J. Executive summary: The health and fitness benefits of regular participation in small-sided football games. Scand. J. Med. Sci. Sport. 2010, 20, 132–135. [Google Scholar] [CrossRef]
- Luo, H.; Newton, R.U.; Maayah, F.; Galvão, D.A.; Taaffe, D.T. Recreational soccer as sport medicine for middle-aged and older adults: A systematic review. BMJ Open Sport Exerc. Med. 2018, 4, e000336. [Google Scholar] [CrossRef] [PubMed]
- Milanović, Z.; Pantelić, S.; Čović, N.; Sporiš, G.; Krustrup, P. Is Recreational Soccer Effective for Improving VO2max? A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 1339–1353. [Google Scholar] [PubMed] [Green Version]
- Arnold, J.T.; Bruce-Low, S.; Sammut, L. The Impact of 12 Weeks Walking Football on Health and Fitness in Males over 50 Years of Age. BMJ Open Sport Exerc. Med. 2015, 1, bmjsem-2015-000048. [Google Scholar] [CrossRef] [Green Version]
- Hubball, H.; Reddy, P. The Impact of Walking Football: Effective Team Strategies for High Performance Veteran Players. J. Sports Pedagog. Phys. Educ. 2015, 6, 13–27. [Google Scholar] [CrossRef]
- Reddy, P.; Dias, I.; Holland, C.; Campbell, N.; Nagar, I.; Connolly, L.; Krustrup, P.; Hubball, H. Walking football as sustainable exercise for older adults—A pilot investigation. Eur. J. Sport Sci. 2017, 17, 638–645. [Google Scholar] [CrossRef] [Green Version]
- Andersen, T.R.; Schmidt, J.F.; Nielsen, J.J.; Randers, M.B.; Sundstrup, E.; Jakobsen, M.D.; Andersen, L.L.; Suetta, C.; Aagaard, P.; Bangsbo, J.; et al. Effect of Football or Strength Training on Functional Ability and Physical Performance in Untrained Old Men. Scand. J. Med. Sci. Sports 2014, 24 (Suppl. 1), 76–85. [Google Scholar] [CrossRef]
- Mohr, M.; Lindenskov, A.; Holm, P.M.; Nielsen, H.P.; Mortensen, J.; Weihe, P.; Krustrup, P. Football training improves cardiovascular health profile in sedentary, premenopausal hypertensive women. Scand. J. Med. Sci. Sports 2014, 24 (Suppl. 1), 36–42. [Google Scholar] [CrossRef]
- Andersen, T.R.; Schmidt, J.F.; Thomassen, M.; Hornstrup, T.; Frandsen, U.; Randers, M.B.; Hansen, P.R.; Krustrup, P.; Bangsbo, J. A preliminary study: Effects of football training on glucose control, body composition, and performance in men with type 2 diabetes. Scand. J. Med. Sci. Sports 2014, 24 (Suppl. 1), 43–56. [Google Scholar] [CrossRef]
- Uth, J.; Fristrup, B.; Haahr, R.D.; Brasso, K.; Helge, J.; Rørth, M.; Midtgaard, J.; Krustrup, P. Football training over 5 years is associated with preserved femoral bone mineral density in men with prostate cancer. Scand. J. Med. Sci. Sports 2018, 28 (Suppl. 1), 61–73. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.F.; Hansen, P.R.; Andersen, T.R.; Andersen, L.J.; Hornstrup, T.; Krustrup, P.; Bangsbo, J. Cardiovascular adaptations to 4 and 12 months of football or strength training in 65- to 75-year-old untrained men. Scand. J. Med. Sci. Sports 2014, 24 (Suppl. 1), 86–97. [Google Scholar] [CrossRef] [PubMed]
- Helge, E.W.; Andersen, T.R.; Schmidt, J.F.; Jørgensen, N.R.; Hornstrup, T.; Krustrup, P.; Bangsbo, J. Recreational football improves bone mineral density and bone turnover marker profile in elderly men. Scand. J. Med. Sci. Sports 2014, 24 (Suppl. 1), 98–104. [Google Scholar] [CrossRef] [PubMed]
- Unhjem, R.; van den Hoven, L.T.; Nygård, M.; Hoff, J.; Wang, E. Functional Performance With Age: The Role of Long-Term Strength Training. J. Geriatr. Phys. Ther. 2019, 42, 115–122. [Google Scholar] [CrossRef]
- American College of Sports Medicine; Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med. Sci. Sport. Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Duncan, M.J.; Minatto, G.; Wright, S.L. Dose-response between pedometer assessed physical activity, functional fitness, and fatness in healthy adults aged 50–80 years. Am. J. Hum. Biol. 2016, 28, 890–894. [Google Scholar] [CrossRef]
- UK Health Security Agency. Case Control Study: Comparative Studies; UK Health Security Agency: London, UK, 2021. Available online: https://www.gov.uk/guidance/case-control-study-comparative-studies (accessed on 10 September 2022).
- Rikli, R.E.; Jones, C.J. Development and validation of a functional fitness test for community—Residing older adults. J. Aging. Phys. Act. 2001, 7, 127–159. [Google Scholar] [CrossRef]
- Syed-Abdul, M.M.; Soni, D.S.; Barnes, J.T.; Wagganer, J. D Comparative analysis of BIA, IBC and DXA for determining body fat in American Football players. J. Sports Med. Phys. Fit. 2021, 61, 687–692. [Google Scholar] [CrossRef]
- Heyward, V.H. Advanced Fitness Assessment and Exercise Prescription; Human Kinetics: Champaign, IL, USA, 1991. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- IPAQ. The International Physical Activity Questionnaire—Long Form. 2001. Available online: http://www.ipaq.ki.se (accessed on 10 September 2022).
- Rikli, R.E.; Jones, C.J. Functional fitness normative scores for community-residing older adults, ages 60–94. J. Aging Phys. Act. 1999, 7, 162–181. [Google Scholar] [CrossRef]
- Sundstrup, E.; Jakobsen, M.D.; Andersen, L.L.; Andersen, T.R.; Randers, M.B.; Helge, J.W.; Suetta, C.; Schmidt, J.F.; Bangsbo, J.; Krustrup, P.; et al. Positive effects of 1-year football and strength training on mechanical muscle function and functional capacity in elderly men. Eur. J. Appl. Physiol. 2016, 116, 1127–1138. [Google Scholar] [CrossRef] [PubMed]
- Julin, M.; Duncan, M.; Randers, M.; Belli, A.; Munoz, I. 6–0! Recreational Football, Practical Guide with Exercises and Drills; Laurea University: Vantaa, Finland, 2020. [Google Scholar]
- Jeffreys, I. Warm up revisited—The ‘ramp’ method of optimising performance preparation. Prof. Strength Cond. 2007, 6, 12–18. [Google Scholar]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Salem, G.J.; Wang, M.Y.; Young, J.T.; Marion, M.; Greendale, G.A. Knee strength and lower- and higher-intensity functional performance in older adults. Med. Sci. Sport. Exerc. 2000, 32, 1679–1684. [Google Scholar] [CrossRef] [PubMed]
- Liew, B.X.W.; Rugamer, D.; Duffy, K.; Taylor, M.; Jackson, J. The mechanical energetics of walking across the adult lifespan. PLoS ONE 2021, 16, e0259817. [Google Scholar] [CrossRef] [PubMed]
- Kline, P.W.; Williams, D.S.B. Effects of normal aging on lower extremity loading and coordination during running in males and females. Int. J. Sport. Phys. Ther. 2015, 10, 901–909. [Google Scholar]
- Ortega, J.D.; Beck, O.N.; Roby, J.M.; Turney, A.L.; Kram, R. Running for exercise mitigates age-related deterioration of walking economy. PLoS ONE 2014, 9, e113471. [Google Scholar]
- Bennike, S.; Ottsen, L.; Gronlund Rasmussen, K.; Krustrup, B.; Midtgaard, J. The implementation of football fitness. In Football as Medicine: Prescribing Football for Global Health Promotion; Krustrup, P., Parnell, D., Eds.; Routledge: London, UK, 2019; pp. 157–172. [Google Scholar]
- Pedersen, M.T.; Vorup, J.; Nistrup, A.; Wikman, J.M.; Alstrøm, J.M.; Melcher, P.S.; Pfister, G.U.; Bangsbo, J. Effect of team sports and resistance training on physical function, quality of life, and motivation in older adults. Scand. J. Med. Sci. Sports 2017, 27, 852–864. [Google Scholar] [CrossRef]
- Phillips, L.H. Sports injury incidence. Br. J. Sport. Med. 2000, 34, 133–136. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention | Control | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre–Post X Group Interactions | ||||||||||
| M | SD | 95% CI | M | SD | 95% CI | M | SD | 95% CI | M | SD | 95% CI | p | Pƞ2 | |
| Physical activity (MET.min.week) | 3020.3 | 1178.0 | 3118.3 | 1310.2 | ||||||||||
| BMI (kg/m2) | 28.8 | 5.4 | 26.5–31.2 | 28.6 | 5.4 | 26.2–30.9 | 26.4 | 2.6 | 23.1–27.8 | 26.4 | 2.4 | 23.0–27.8 | >0.05 | 0.007 |
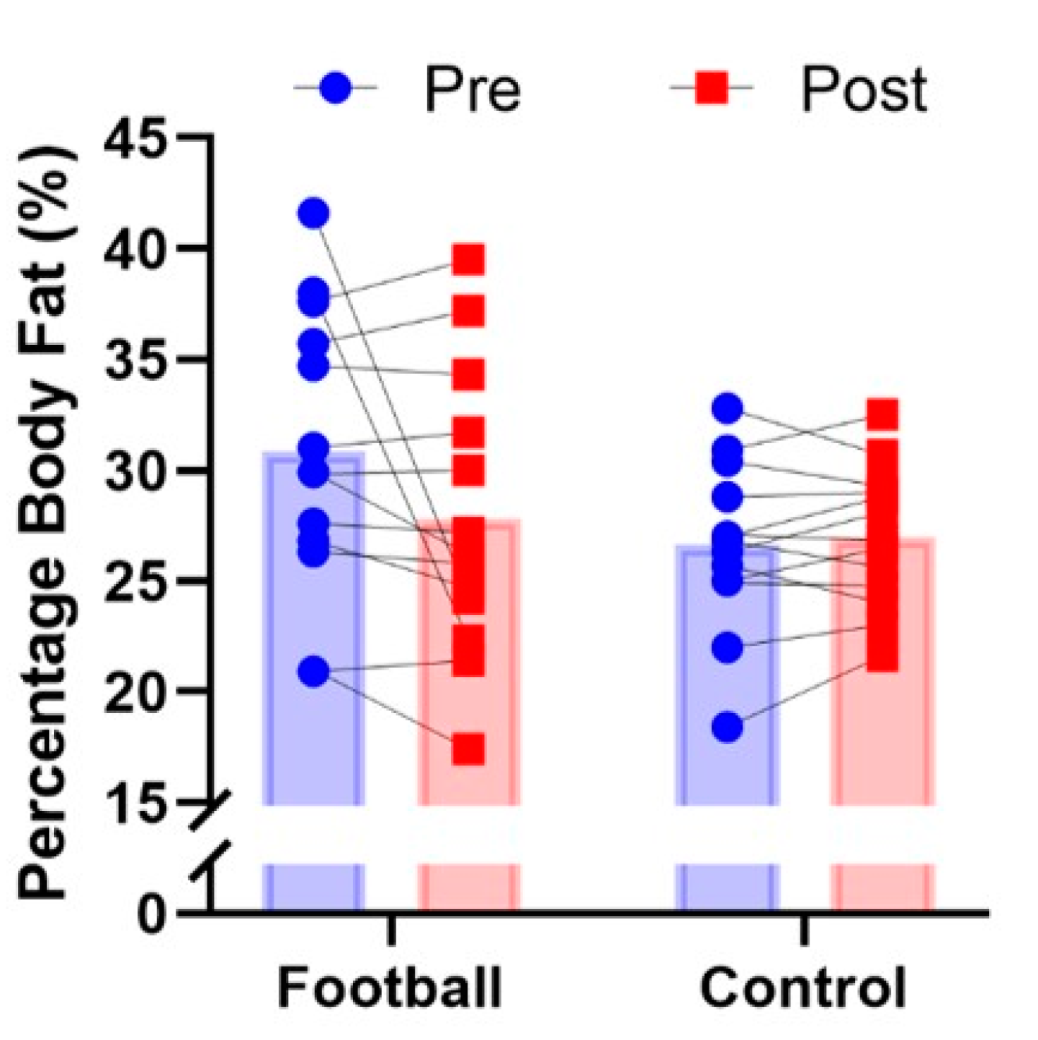
| Body fat (%) | 30.8 | 6.4 | 27.8–33.8 | 27.8 | 6.4 | 24.9–30.7 | 26.6 | 3.8 | 23.6–29.6 | 26.9 | 3.1 | 24.1–29.8 | 0.07 | 0.127 |
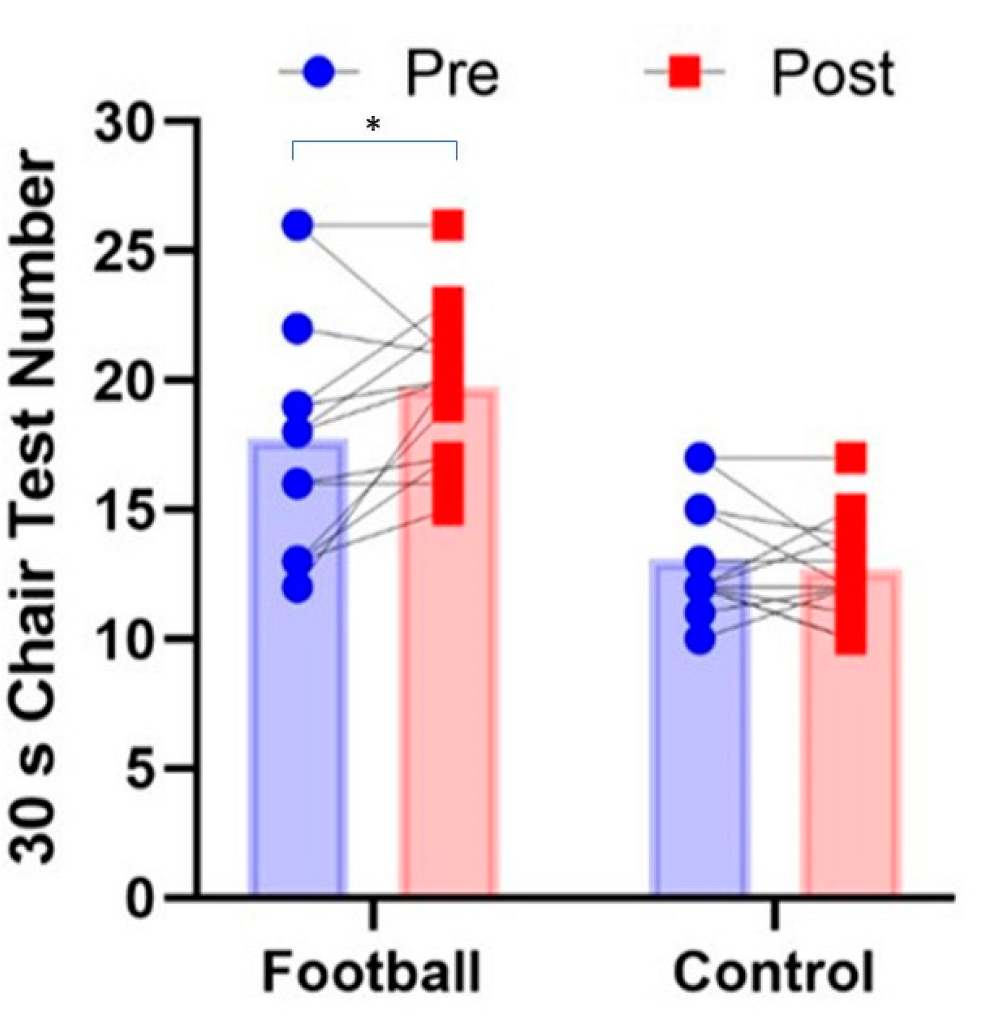
| 30 s chair stand (reps) | 17.8 | 4.7 | 15.6–19.8 | 19.8 | 3.3 | 18.3–21.2 | 14.0 | 2.2 | 10.9–15.2 | 12.7 | 2.9 | 11.2–14.2 | 0.038 | 0.168 |
| 30 s arm curl test (reps) | 23.5 | 3.9 | 21.6–25.3 | 23.9 | 4.2 | 21.8–25.8 | 14.2 | 2.2 | 12.4–16.1 | 15.3 | 2.8 | 13.3–17.3 | >0.05 | 0.009 |
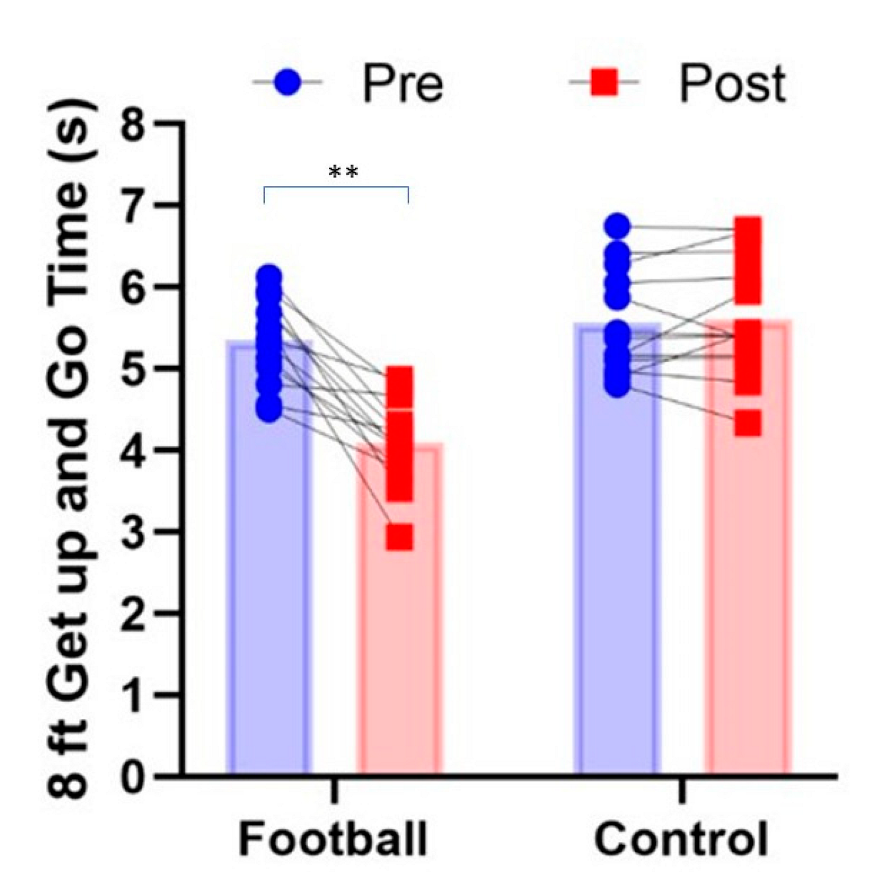
| 8-foot get up and go (secs) | 5.4 | 0.5 | 5.0–5.7 | 4.1 | 0.5 | 3.7–4.6 | 5.5 | 0.6 | 5.2–5.8 | 5.6 | 0.7 | 5.2–5.9 | 0.001 | 0.577 |
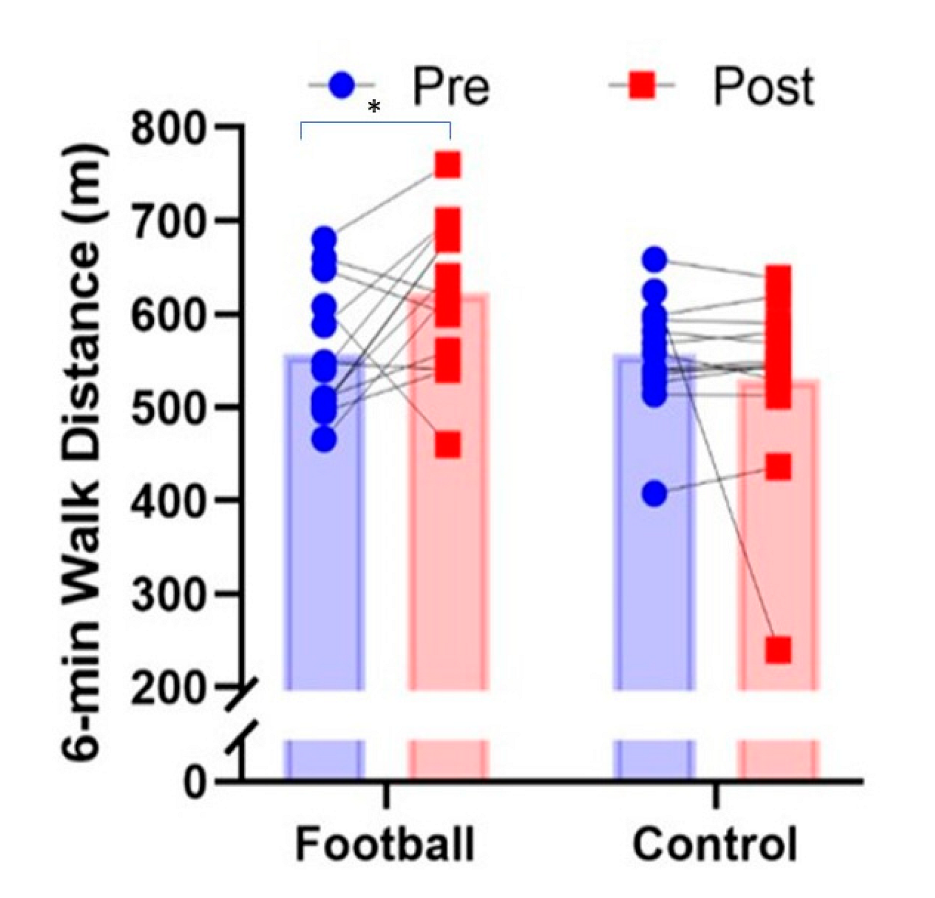
| 6 min walk test (m) | 557.9 | 71.3 | 519.9–595.8 | 623.1 | 82.8 | 570.4–675.8 | 557.2 | 61.0 | 518.2–590.1 | 530.5 | 100.6 | 477.7–583.2 | 0.036 | 0.171 |
| Grip strength (kg) | 36.6 | 9.1 | 31.7–41.6 | 37.5 | 6.9 | 32.9–42.1 | 32.5 | 7.9 | 27.6–37.4 | 31.3 | 9.0 | 26.7–35.8 | >0.05 | 0.011 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duncan, M.J.; Mowle, S.; Noon, M.; Eyre, E.; Clarke, N.D.; Hill, M.; Tallis, J.; Julin, M. The Effect of 12-Weeks Recreational Football (Soccer) for Health Intervention on Functional Movement in Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 13625. https://doi.org/10.3390/ijerph192013625
Duncan MJ, Mowle S, Noon M, Eyre E, Clarke ND, Hill M, Tallis J, Julin M. The Effect of 12-Weeks Recreational Football (Soccer) for Health Intervention on Functional Movement in Older Adults. International Journal of Environmental Research and Public Health. 2022; 19(20):13625. https://doi.org/10.3390/ijerph192013625
Chicago/Turabian StyleDuncan, Michael J., Sophie Mowle, Mark Noon, Emma Eyre, Neil D. Clarke, Mathew Hill, Jason Tallis, and Mikko Julin. 2022. "The Effect of 12-Weeks Recreational Football (Soccer) for Health Intervention on Functional Movement in Older Adults" International Journal of Environmental Research and Public Health 19, no. 20: 13625. https://doi.org/10.3390/ijerph192013625