
Factors Determining the Occurrence of Frailty Syndrome in Hospitalized Older Patients
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Measurements
2.2.1. Frailty Syndrome
2.2.2. Handgrip Strength Measurements
2.2.3. Functional Ability Test
2.2.4. Emotional Status Assessment
2.2.5. Statistical Analysis
2.2.6. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
6. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Clinical Consortium on Healthy Ageing. Report of Consortium Meeting 1–2 December 2016 in Geneva, Switzerland; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Donatelli, N.S.; Somes, J. What is Frailty? J. Emerg. Nurs. 2017, 43, 272–274. [Google Scholar] [CrossRef]
- Chen, X.; Mao, G.; Leng, S.X. Frailty syndrome: An overview. Clin. Interv. Aging 2014, 9, 433–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.-C.; Li, T.-C.; Li, C.-I.; Liu, C.-S.; Lin, W.-Y.; Lin, C.-H.; Yang, C.-W.; Yang, S.-Y.; Lin, C.-C. Frailty, transition in frailty status and all-cause mortality in older adults of a Taichung community-based population. BMC Geriatr. 2019, 19, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the Concepts of Disability, Frailty, and Comorbidity: Implications for Improved Targeting and Care. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, M255–M263. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, N.; Mandel, R.; Fain, M.J. Frailty: An Emerging Geriatric Syndrome. Am. J. Med. 2007, 120, 748–753. [Google Scholar] [CrossRef]
- Nowak, A.; Hubbard, R.E. Falls and frailty: Lessons from complex systems. J. R. Soc. Med. 2009, 102, 98–102. [Google Scholar] [CrossRef] [Green Version]
- Ensrud, K.E.; Ewing, S.K.; Cawthon, P.M.; Fink, H.A.; Taylor, B.; Cauley, J.A.; Dam, T.-T.; Marshall, L.M.; Orwoll, E.; Cummings, S.R.; et al. A Comparison of Frailty Indexes for the Prediction of Falls, Disability, Fractures, and Mortality in Older Men. J. Am. Geriatr. Soc. 2009, 57, 492–498. [Google Scholar] [CrossRef] [Green Version]
- Boyd, C.M.; Xue, Q.-L.; Simpson, C.F.; Guralnik, J.M.; Fried, L.P. Frailty, hospitalization, and progression of disability in a cohort of disabled older women. Am. J. Med. 2005, 118, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Santos-Eggimann, B.; Karmaniola, A.; Seematter-Bagnoud, L.; Spagnoli, J.; Büla, C.; Cornuz, J.; Rodondi, N.; Vollenweider, P.; Waeber, G.; Pécoud, A. The Lausanne cohort Lc65+: A population-based prospective study of the manifestations, determinants and outcomes of frailty. BMC Geriatr. 2008, 8, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, R.; Kuh, D.; Cooper, C.; Gale, C.R.; Lawlor, D.A.; Matthews, F.; Hardy, R. The FALCon and HALCyon Study Teams. Objective measures of physical capability and subsequent health: A systematic review. Age Ageing 2011, 40, 14–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landi, F.; Cruz-Jentoft, A.J.; Liperoti, R.; Russo, A.; Giovannini, S.; Tosato, M.; Capoluongo, E.D.; Bernabei, R.; Onder, G. Sarcopenia and mortality risk in frail older persons aged 80 years and older: Results from ilSIRENTE study. Age Ageing 2013, 42, 203–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos-Eggimann, B.; Cuénoud, P.; Spagnoli, J.; Junod, J. Prevalence of Frailty in Middle-Aged and Older Community-Dwelling Europeans Living in 10 Countries. J. Gerontol. Ser. A 2009, 64A, 675–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, Q.-L. The Frailty Syndrome: Definition and Natural History. Clin. Geriatr. Med. 2011, 27, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMillan, G.J.; Hubbard, R.E. Frailty in older inpatients: What physicians need to know. QJM Int. J. Med. 2012, 105, 1059–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bledowski, P.; Grodzicki, T.; Mossakowska, M.; Zdrojewski, T. Examination of Individual Areas of the Health Condition of the Elderly, Including Health-Related Quality of Life; Gdanski Uniwersytet Medyczny: Gdansk, Poland, 2021. [Google Scholar]
- Bieniek, J.; Szewieczek, J. Frailty diagnostic problems in geriatric patients. A preliminary report. Gerontol. Pol. 2015, 2, 47–53. [Google Scholar]
- Kojima, G. Frailty as a predictor of hospitalisation among community-dwelling older people: A systematic review and meta-analysis. J. Epidemiol. Community Health 2016, 70, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Hartgerink, J.M.; Cramm, J.M.; Bakker, T.J.; van Eijsden, A.M.; Mackenbach, J.P.; Nieboer, A.P. The importance of multidisciplinary teamwork and team climate for relational coordination among teams delivering care to older patients. J. Adv. Nurs. 2014, 70, 791–799. [Google Scholar] [CrossRef]
- Mattos, I.E.; do Carmo, C.N.; Santiago, L.M.; Luz, L.L. Factors associated with functional incapacity in elders living in long stay institutions in Brazil: A cross-sectional study. BMC Geriatr. 2014, 14, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero-Ortuno, R.; Walsh, C.D.; Lawlor, B.A.; Kenny, R.A. A Frailty Instrument for primary care: Findings from the Survey of Health, Ageing and Retirement in Europe (SHARE). BMC Geriatr. 2010, 10, 57. [Google Scholar] [CrossRef]
- Muszalik, M.; Borowiak, E.; Kotarba, A.; Puto, G.; Doroszkiewicz, H.; Kędziora-Kornatowska, K. Adaptation and reliability testing of the SHARE-FI instrument for the assessment of risk of frailty syndrome among older Polish patients. Fam. Med. Prim. Care Rev. 2018, 20, 36–40. [Google Scholar] [CrossRef]
- SHARE-FI Calculator Females v. 1.0. Available online: https://sites.google.com/a/tcd.ie/share-frailty-instrument-calculators/translated-calculators (accessed on 20 July 2022).
- Rantanen, T.; Guralnik, J.M.; Foley, D.; Masaki, K.; Leveille, S.; Curb, J.D.; White, L. Midlife Hand Grip Strength as a Predictor of Old Age Disability. JAMA 1999, 281, 558–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawton, M.P.; Brody, E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Sheikh, J.I. Geriatric Depression Scale (GDS). Clin. Gerontol. 1986, 5, 165–173. [Google Scholar] [CrossRef]
- Sokołowski, R.; Ciesielska, N.; Czajkowska, A.; Bentryn, D.; Węgrzyn, E.; Oleksy, P.; Zukow, W. Patogenesis of Frailty Syndrome. J. Health Sci. 2014, 4, 197–204. [Google Scholar]
- Sternberg, S.; Levin, R.; Dkaidek, S.; Edelman, S.; Resnick, T.; Menczel, J. Frailty and osteoporosis in older women—A prospective study. Osteoporos. Int. 2014, 25, 763–768. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Li, Y.-X.; Wu, C. Incidence of frailty among community-dwelling older adults: A nationally representative profile in China. BMC Geriatr. 2019, 19, 378. [Google Scholar] [CrossRef] [Green Version]
- Kurpas, D.; Szwammel, K.; Bujnowska-Fedak, M. Frailty syndrome—Guidelines for diagnosis, therapy and prevention. Terapia 2017, 2, 1–8. [Google Scholar]
- Muszalik, M.; Kotarba, A.; Borowiak, E.; Puto, G.; Cybulski, M.; Kȩdziora-Kornatowska, K. Socio-Demographic, Clinical and Psychological Profile of Frailty Patients Living in the Home Environment and Nursing Homes: A Cross-Sectional Study. Front. Psychiatry 2021, 12, 736804. [Google Scholar] [CrossRef]
- Thinuan, P.; Siviroj, P.; Lerttrakarnnon, P.; Lorga, T. Prevalence and Potential Predictors of Frailty among Community-Dwelling Older Persons in Northern Thailand: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 4077. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Puts, M.; Jiang, F.; Zhou, C.; Tang, S.; Chen, S. Physical frailty and its associated factors among elderly nursing home residents in China. BMC Geriatr. 2020, 20, 294. [Google Scholar] [CrossRef] [PubMed]
- Saum, K.; Schöttker, B.; Meid, A.D.; Holleczek, B.; Haefeli, W.E.; Hauer, K.; Brenner, H. Is Polypharmacy Associated with Frailty in Older People? Results from the ESTHER Cohort Study. J. Am. Geriatr. Soc. 2017, 65, e27–e32. [Google Scholar] [CrossRef] [PubMed]
- Ozer, F.F.; Akin, S.; Soysal, T.; Gokcekuyu, B.M.; Durmus, N.S. Depression in Frail Older Adults: Associations and Gender Difference. North. Clin. Istanb. 2022, 9, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Boyer, S.; Trimouillas, J.; Cardinaud, N.; Gayot, C.; Laubarie-Mouret, C.; Dumoitier, N.; Rudelle, K.; Druet-Cabanac, M.; Laroche, M.-L.; Tchalla, A. Frailty and functional dependence in older population: Lessons from the FREEDOM Limousin—Nouvelle Aquitaine Cohort Study. BMC Geriatr. 2022, 22, 128. [Google Scholar] [CrossRef]
- Aprahamian, I.; Suemoto, C.K.; Lin, S.M.; de Siqueira, A.S.S.; Biella, M.M.; de Melo, B.A.R.; Jacob-Filho, W. Depression is associated with self-rated frailty in older adults from an outpatient clinic: A prospective study. Int. Psychogeriatr. 2019, 31, 425–434. [Google Scholar] [CrossRef]
- Collard, R.M.; Arts, M.H.L.; Schene, A.H.; Naarding, P.; Voshaar, R.O.; Comijs, H.C. The impact of frailty on depressive disorder in later life: Findings from the Netherlands Study of depression in older persons. Eur. Psychiatry 2017, 43, 66–72. [Google Scholar] [CrossRef]
- Rodda, J.; Walker, Z.; Carter, J. Depression in older adults. BMJ 2011, 343, d5219. [Google Scholar] [CrossRef]
- Ytterstad, E. Frailty in Survival Analysis of Widowhood Mortality. J. Probab. Stat. 2018, 2018, 5. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Quantitative Variables | All n = 141 | Women n = 78 | Men n = 63 | Mann-Whitney U-Test/Chi2 p-Value |
|---|---|---|---|---|
| Demography | ||||
| Age [years] | 73 (68–81) | 73 (67–81) | 73 (68–80) | ns |
| Education [n, %] | ns | |||
| Higher | 21 (14.9) | 10 (12.8) | 11 (17.5) | |
| Secondary | 61 (43.3) | 35 (44.9) | 26 (41.3) | |
| Vocational | 31 (22) | 19 (24.4) | 12 (19.1) | |
| Primary | 28 (19.9) | 14 (18) | 14 (22.2) | |
| Place of living [n, %] | ns | |||
| Urban | 118 (83.7) | 65 (83.3) | 53 (84.1) | |
| Rural | 23 (16.3) | 13 (16.7) | 10 (15.9) | |
| Living status [n, %] | ns | |||
| Alone | 65 (46.1) | 38 (48.7) | 27 (42.9) | |
| With family | 76 (53.9) | 40 (51.3) | 36 (57.1) | |
| Marital status [n, %] | ns | |||
| married | 62 (44) | 30 (38.5) | 32 (50.8) | |
| not married/single | 14 (9.9) | 7 (9) | 7 (11.1) | |
| widowed | 65 (46.1) | 41 (52.6) | 24 (38.1) | |
| Economic status [n, %] | ns | |||
| very good | 9 (6.4) | 4 (5.1) | 5 (7.9) | |
| good | 56 (39.7) | 36 (46.2) | 20 (31.8) | |
| average | 75 (53.2) | 38 (48.7) | 37 (58.7) | |
| bad | 1 (0.7) | 0 | 1 (1.6) | |
| Anthropometry and state of health | ||||
| BMI [kg/m2] | 25.3 (22.6–29.7) | 25.3 (22.8–29.3) | 24.9 (21.8–32) | ns |
| IADL [number of points] | 24 (20–27) | 24 (20–26) | 24 (21–27) | ns |
| IADL Category [n, %] | ns | |||
| low | 2 (1.4) | 1 (1.3) | 1 (1.6) | |
| medium | 26 (18.4) | 14 (18) | 12 (19.1) | |
| high | 113 (80.1) | 63 (80.8) | 50 (79.4) | |
| Mobility [n, %] | ns | |||
| independent | 108 (76.6) | 59 (76) | 49 (77.8) | |
| cart | 3 (2.1) | 2 (2.6) | 1 (1.6) | |
| balcony | 7 (5) | 5 (6.4) | 2 (3.2) | |
| crutches | 16 (11.3) | 8 (10.3) | 8 (12.7) | |
| lying patient | 7 (5) | 4 (5.1) | 3 (4.8) | |
| HGS max. [kg] | 22 (18–30) | 20 (15–28) | 30 (20–35) | 0.0004 |
| GDS [number of points] | 3 (1–7) | 3 (1–6) | 2 (1–7) | ns |
| GDS Category [n, %] | ns | |||
| normal mood | 104 (73.8) | 59 (75.6) | 45 (71.4) | |
| risk of depressive symptoms | 26 (18.4) | 14 (18) | 12 (19.1) | |
| severe depressive symptoms | 11 (7.8) | 5 (6.4) | 6 (9.5) | |
| Fraility score | 2.02 (1.02–3.1) | 2.22 (1.27–3.02) | 1.98 (0.5–3.2) | ns |
| Diseases | ||||
| Number of diseases | 3 (2–5) | 3 (2–5) | 3 (2–5) | ns |
| Number of medications taken | 6 (3–8.5) | 6 (3–9) | 6 (3–8) | ns |
| Use of a hearing aid | 19 (13.5) | 7 (9) | 12 (19.1) | ns |
| Use of glasses | 112 (79.4) | 61 (78.2) | 51 (81) | ns |
| Heart diseases, n [%] | 42 (29.8) | 29 (38.2) | 13 (20.6) | 0.03 |
| Hypertension, n [%] | 85 (60.3) | 52 (66.7) | 33 (52.4) | ns |
| High blood cholesterol, n [%] | 20 (14.2) | 8 (10.4) | 12 (19.1) | ns |
| Stroke, n [%] | 9 (6.4) | 6 (7.7) | 3 (4.8) | ns |
| Diabetes, n [%] | 42 (29.8) | 22 (28.2) | 20 (31.8) | ns |
| Respiratory system diseases, n [%] | 17 (12.1) | 4 (5.1) | 13 (20.6) | 0.005 |
| Cancer, n (%) | 12 (8.5) | 5 (6.4) | 7 (11.1) | ns |
| Stomach or duodenal ulcer, n [%] | 9 (6.4) | 6 (7.7) | 3 (4.8) | ns |
| Quantitative Variables | Frail n = 55 | Pre-frail n = 52 | Control n = 34 | Kruskal–Wallis p-Value |
|---|---|---|---|---|
| Demography | ||||
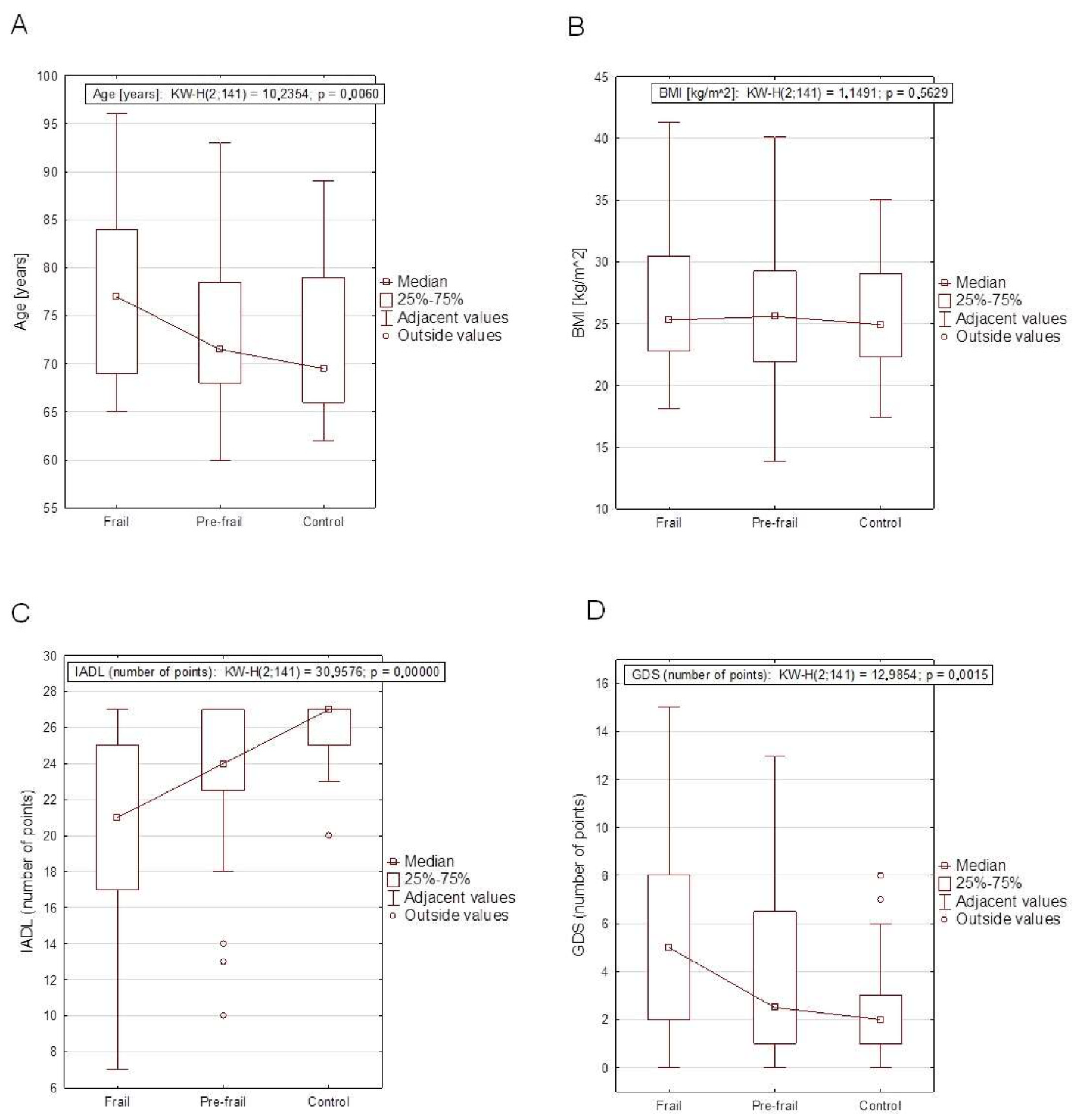
| Age [years] | 77(69–84) | 71.5 (68–78.5) | 69.5 (66–79) | 0.006 b |
| Men [n, %] | 19 (35) | 24 (46.2) | 20 (58.8) | ns |
| Education [n, %] | ns | |||
| Higher | 11 (20) | 6 (53.8) | 4 (11.8) | |
| Secondary | 17 (30.9) | 28 (3.9) | 16 (47.1) | |
| Vocational | 12 (21.8) | 11 (21.2) | 8 (23.5) | |
| Primary | 15 (27.3) | 7 (13.5) | 6 (17.7) | |
| Place of living [n, %] | ns | |||
| Urban | 44 (80) | 45 (86.6) | 29 (85.3) | |
| Rural | 11 (20) | 7 (13.5) | 5 (14.7) | |
| Living status [n, %] | ns | |||
| Alone | 31 (56.4) | 20 (38.5) | 14 (41.2) | |
| With family | 24 (43.6) | 32 (61.5) | 20 (58.8) | |
| Marital status [n, %] | 0.006 | |||
| married | 14 (25.5) | 29 (55.8) | 19 (55.9) | |
| not married/single | 7 (12.7) | 6 (11.5) | 1 (2.9) | |
| widowed | 34 (61.8) | 17 (32.7) | 14 (41.2) | |
| Economic status [n, %] | ns | |||
| very good | 5 (9.1) | 4 (7.7) | 0 | |
| good | 26 (47.3) | 21 (40.4) | 9 (26.5) | |
| average | 24 (43.6) | 26 (50) | 25 (73.5) | |
| bad | 0 | 1 (1.9) | 0 | |
| Anthropometry and state of health | ||||
| BMI [kg/m2] | 25.3 (22.8–30.5) | 25.6 (21.9–29.3) | 24.9 (22.3–29.1) | ns |
| IADL [number of points] | 21 (17–25) | 24 (22.5–27) | 27 (25–27) | <0.001 a.b.c |
| IADL Category [n, %] | 0.0075 | |||
| low | 2 (3.6) | 0 | 0 | |
| medium | 17 (30.1) | 7 (13.5) | 2 (5.9) | |
| high | 36 (65.5) | 45 (86.5) | 32 (94.1) | |
| Mobility [n, %] | 0.019 | |||
| independent | 35 (63.6) | 40 (76.9) | 33 (97) | |
| cart | 1 (1.8) | 1 (1.9) | 1(2.9) | |
| balcony | 3 (5.5) | 4 (7.7) | 0 | |
| crutches | 10 (18.2) | 6 (11.5) | 0 | |
| lying patient | 6 (10.9) | 1 (1.9) | 0 | |
| HGS max. [kg] | 20 (13–25) | 25 (20–32.5) | 32 (24–42) | <0.001 a.b.c |
| GDS [number of points] | 5 (2–8) | 2.5 (1–6.5) | 2 (1–3) | 0.0015 b |
| GDS Category [n, %] | ns | |||
| normal mood | 35 (63.6) | 40 (77) | 20 (85.3) | |
| risk of depressive symptoms | 14 (25.5) | 10 (19.2) | 2 (5.9) | |
| severe depressive symptoms | 6 (10.9) | 2 (3.9) | 3 (8.8) | |
| Fraility score | 3.54 (2.69–4.15) | 1.68 (1.42–2.11) | 0.05 (−0.66–0.5) | 0.0001 a.b.c |
| Diseases | ||||
| Number of diseases | 4 (3–6) | 3 (2–3.5) | 3 (2–5) | 0.0001 b.c |
| Number of medications taken | 8 (6–10) | 5 (2.5–7) | 5 (3–7) | 0.0003 b.c |
| Use of a hearing aid | 9 (16.4) | 6 (11.5) | 4 (11.8) | ns |
| Use of glasses | 48 (87.3) | 39 (75) | 25 (73.5) | ns |
| Heart diseases, n [%] | 23 (41.8) | 13 (26) | 6 (17.7) | 0.039 |
| Hypertension, n [%] | 34 (61.8) | 28 (53.9) | 23 (67.7) | ns |
| High blood cholesterol, n [%] | 11 (20) | 4 (7.84) | 5 (14.7) | ns |
| Stroke, n [%] | 7 (12.7) | 2 (3.85) | 0 | ns |
| Diabetes, n [%] | 19 (34.6) | 15 (28.9) | 8 (23.5) | ns |
| Respiratory system diseases, n [%] | 8 (14.5) | 4 (7.7) | 5 (14.7) | ns |
| Cancer, n [%] | 6 (10.9) | 5 (9.6) | 1 (2.9) | ns |
| Stomach or duodenal ulcer, n [%] | 5 (9.1) | 1 (1.9) | 3 (8.8) | ns |
| Quantitative Variables | Spearman’s Rank Correlation Coefficient in All | Spearman’s Rank Correlation Coefficient in Women | Spearman’s Rank Correlation Coefficient in Men |
|---|---|---|---|
| Age [years] | 0.2384 ** | 0.3352 ** | 0.1217 |
| Number of diseases | 0.3089 *** | 0.4565 *** | 0.1417 |
| Number of medications taken | 0.2164 * | 0.2723 * | 0.1488 |
| BMI [kg/m2] | 0.1236 | 0.0335 | 0.2081 |
| IADL [number of points] | −0.4686 *** | −0.3766 *** | −0.5642 *** |
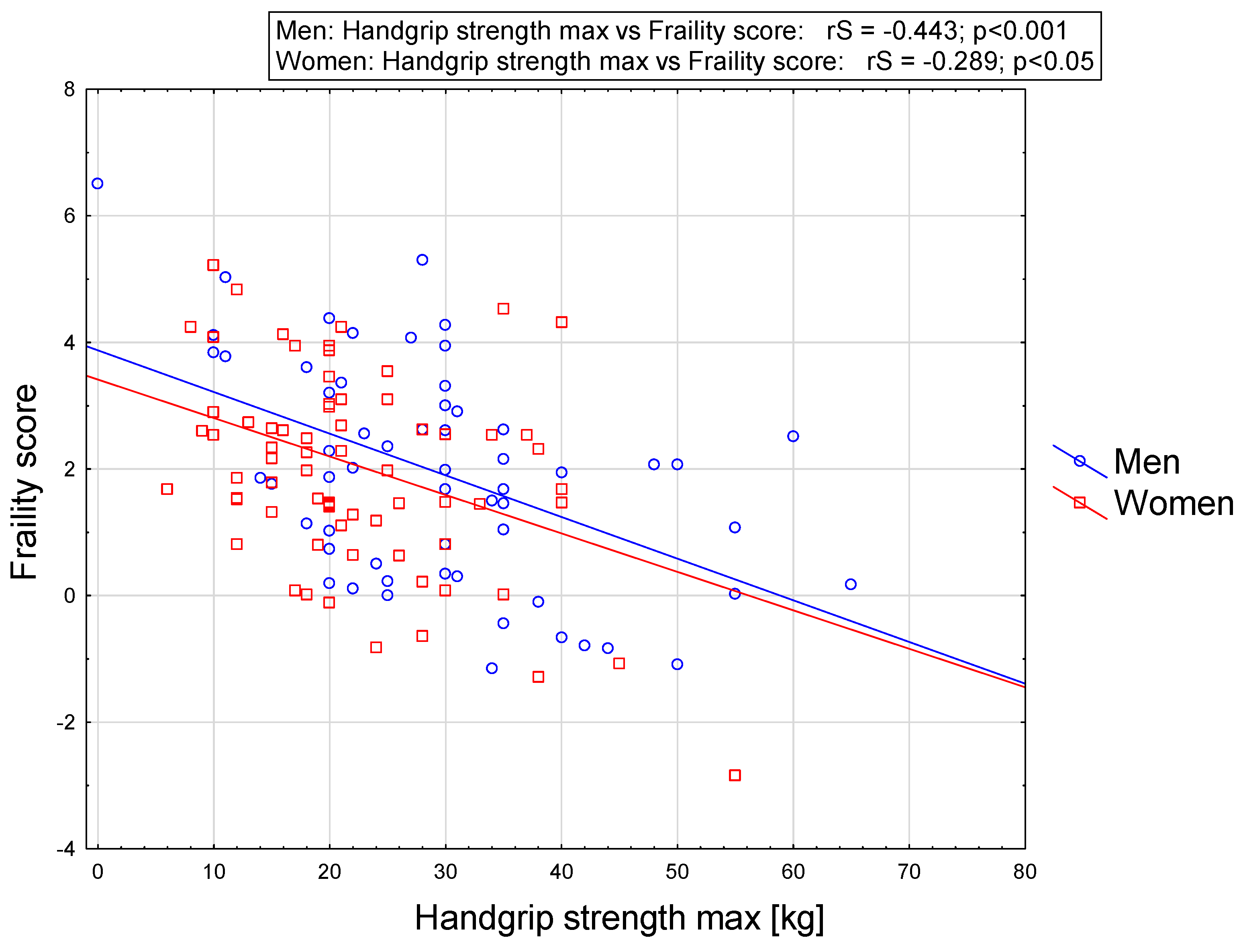
| HGS max. [kg] | −0.3485 *** | −0.2891 * | −0.4430 *** |
| GDS [number of points] | 0.3159 *** | 0.2443 * | 0.3810 ** |
| Quantitative Variables | Odds Ratio | 95% Confidence Intervals | p-Value |
|---|---|---|---|
| Women (reference group) | 1 | ||
| Men | 0.50 | 0.25–1.01 | ns |
| Age [years] | 1.06 | 1.02–1.11 | 0.0036 |
| Married (reference group) | 1 | ||
| Not married/single | 3.43 | 1.03–11.44 | 0.0451 |
| Widowed | 3.76 | 1.74–8.11 | 0.0007 |
| Witout heart diseases (reference group) | 1 | ||
| Heart diseases | 2.46 | 1.17–5.16 | 0.0172 |
| Number of diseases | 1.41 | 1.17–1.69 | 0.0003 |
| BMI [kg/m2] | 1.04 | 0.98–1.11 | ns |
| IADL [number of points] | 0.82 | 0.75–0.90 | 0.0000 |
| GDS [number of points] | 1.13 | 1.03–1.25 | 0.0096 |
| HGS max. [kg] | 0.90 | 0.86–0.94 | 0.0000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kozicka, I.; Guligowska, A.; Chrobak-Bień, J.; Czyżewska, K.; Doroba, N.; Ignaczak, A.; Machała, A.; Spałka, E.; Kostka, T.; Borowiak, E. Factors Determining the Occurrence of Frailty Syndrome in Hospitalized Older Patients. Int. J. Environ. Res. Public Health 2022, 19, 12769. https://doi.org/10.3390/ijerph191912769
Kozicka I, Guligowska A, Chrobak-Bień J, Czyżewska K, Doroba N, Ignaczak A, Machała A, Spałka E, Kostka T, Borowiak E. Factors Determining the Occurrence of Frailty Syndrome in Hospitalized Older Patients. International Journal of Environmental Research and Public Health. 2022; 19(19):12769. https://doi.org/10.3390/ijerph191912769
Chicago/Turabian StyleKozicka, Izabela, Agnieszka Guligowska, Joanna Chrobak-Bień, Katarzyna Czyżewska, Natalia Doroba, Anna Ignaczak, Anna Machała, Ewelina Spałka, Tomasz Kostka, and Ewa Borowiak. 2022. "Factors Determining the Occurrence of Frailty Syndrome in Hospitalized Older Patients" International Journal of Environmental Research and Public Health 19, no. 19: 12769. https://doi.org/10.3390/ijerph191912769