
Characterizing Subjects Exposed to Humidifier Disinfectants Using Computed-Tomography-Based Latent Traits: A Deep Learning Approach
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Human Subject Data and Image Processing
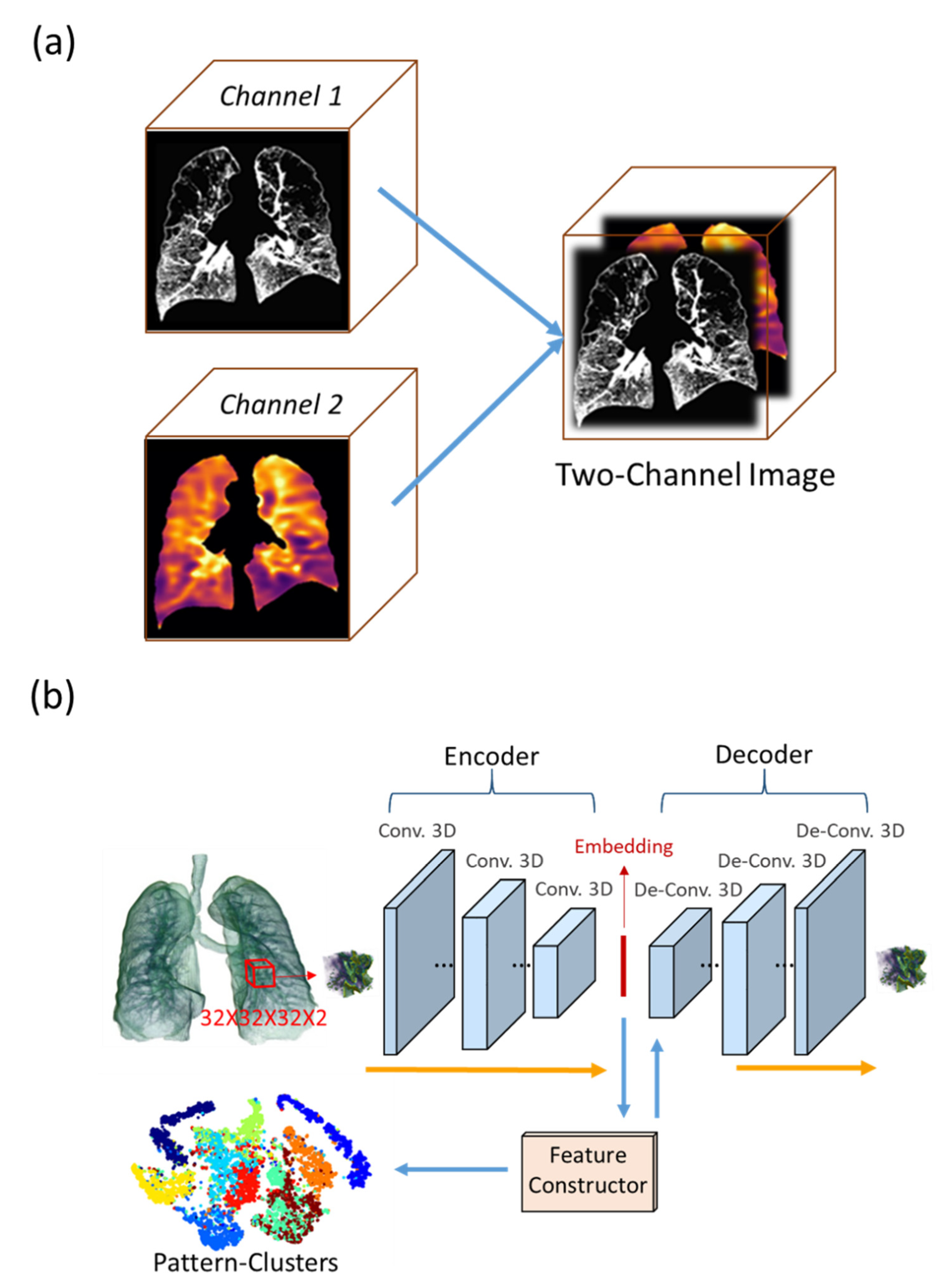
2.2. 3D Convolutional Autoencoder (CAE) and Feature Constructor (FC)
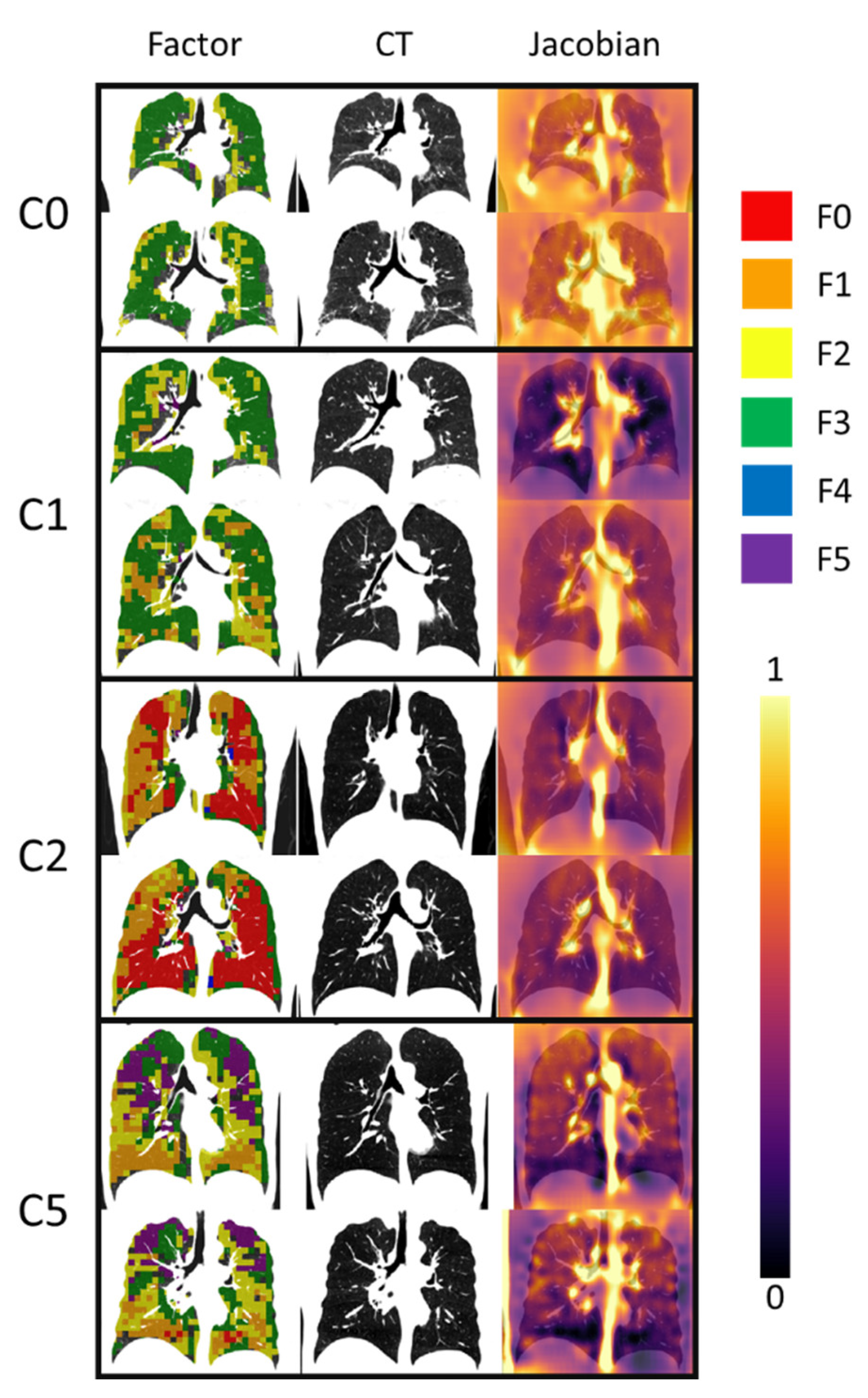
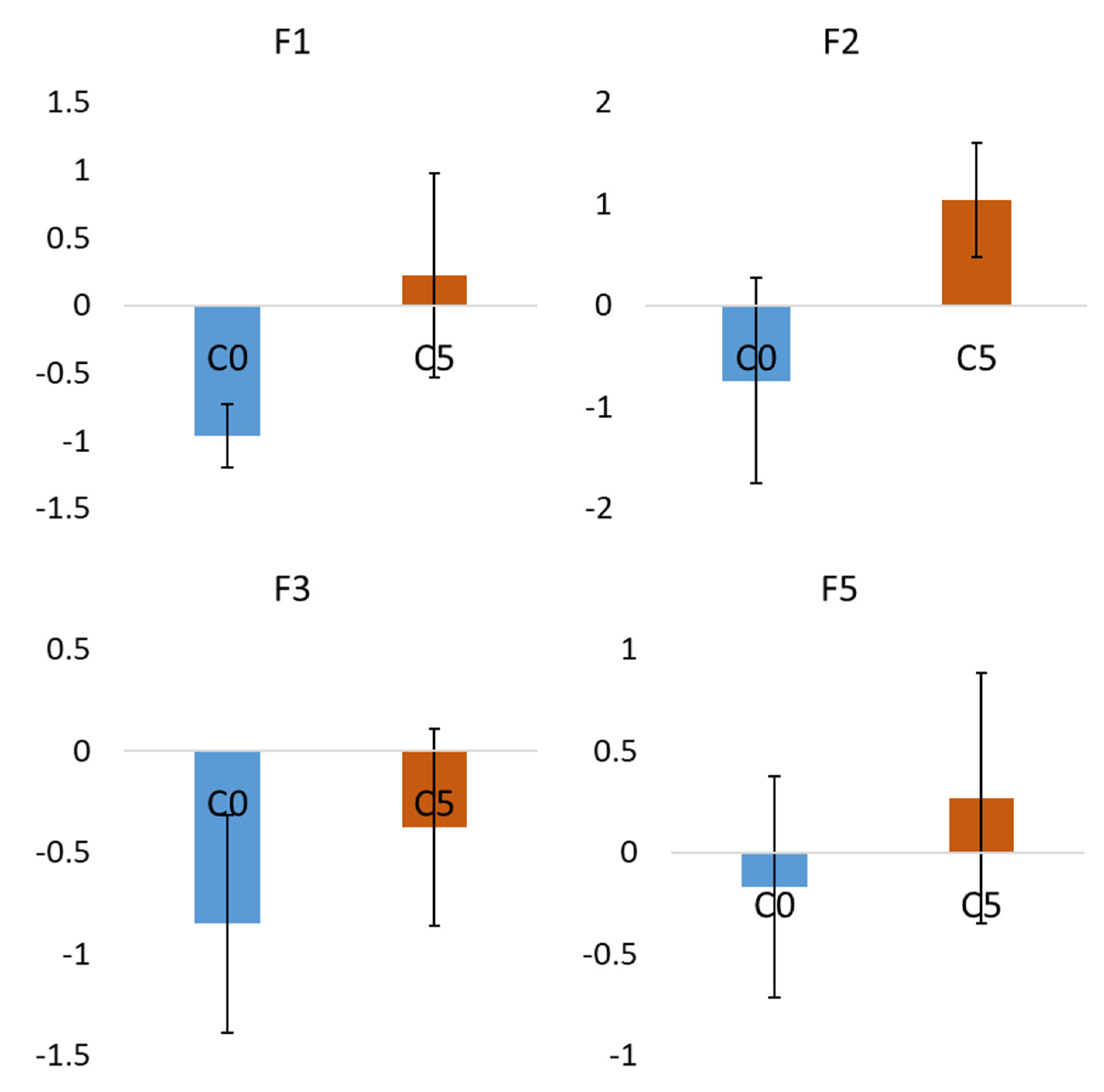
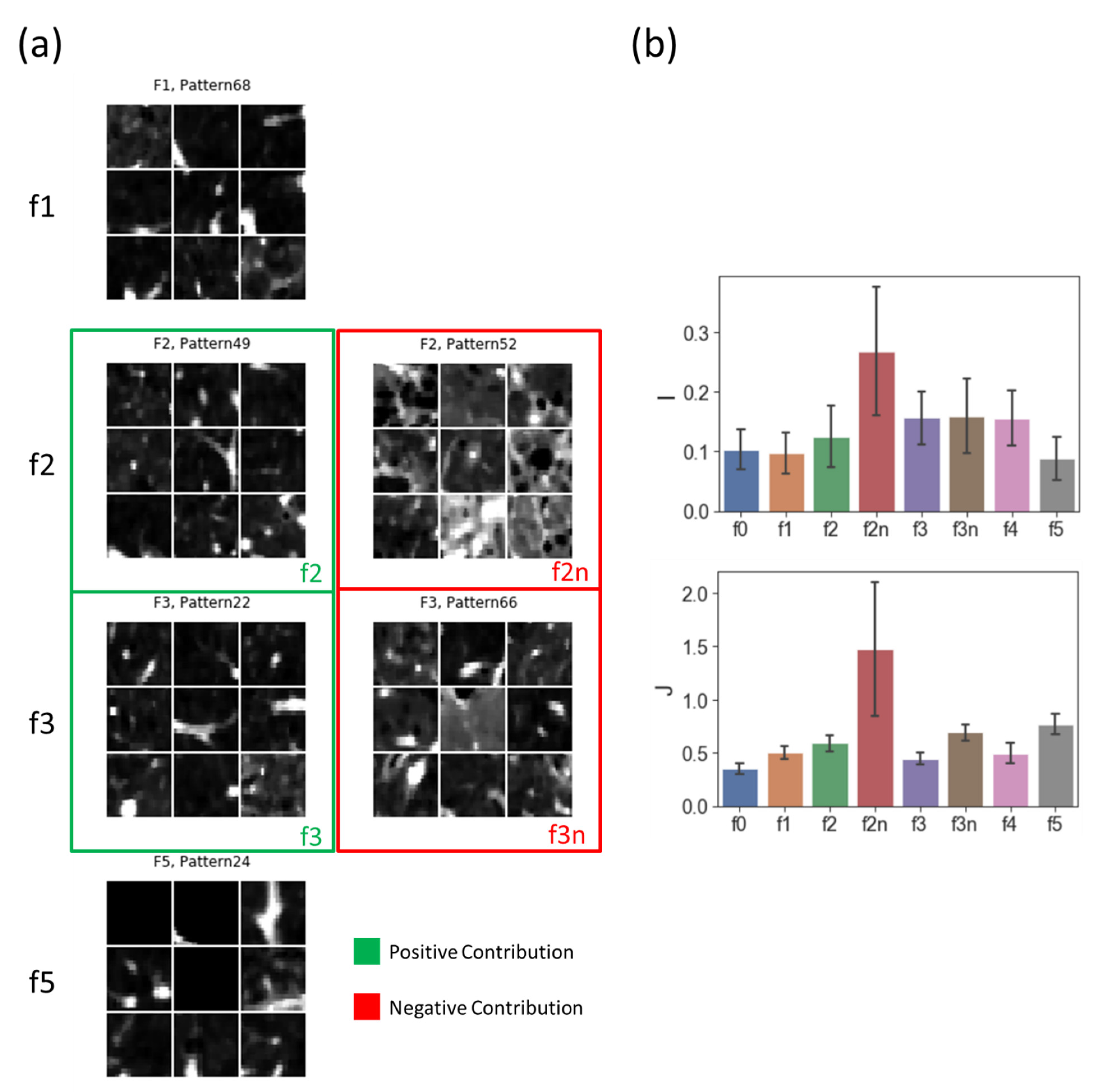
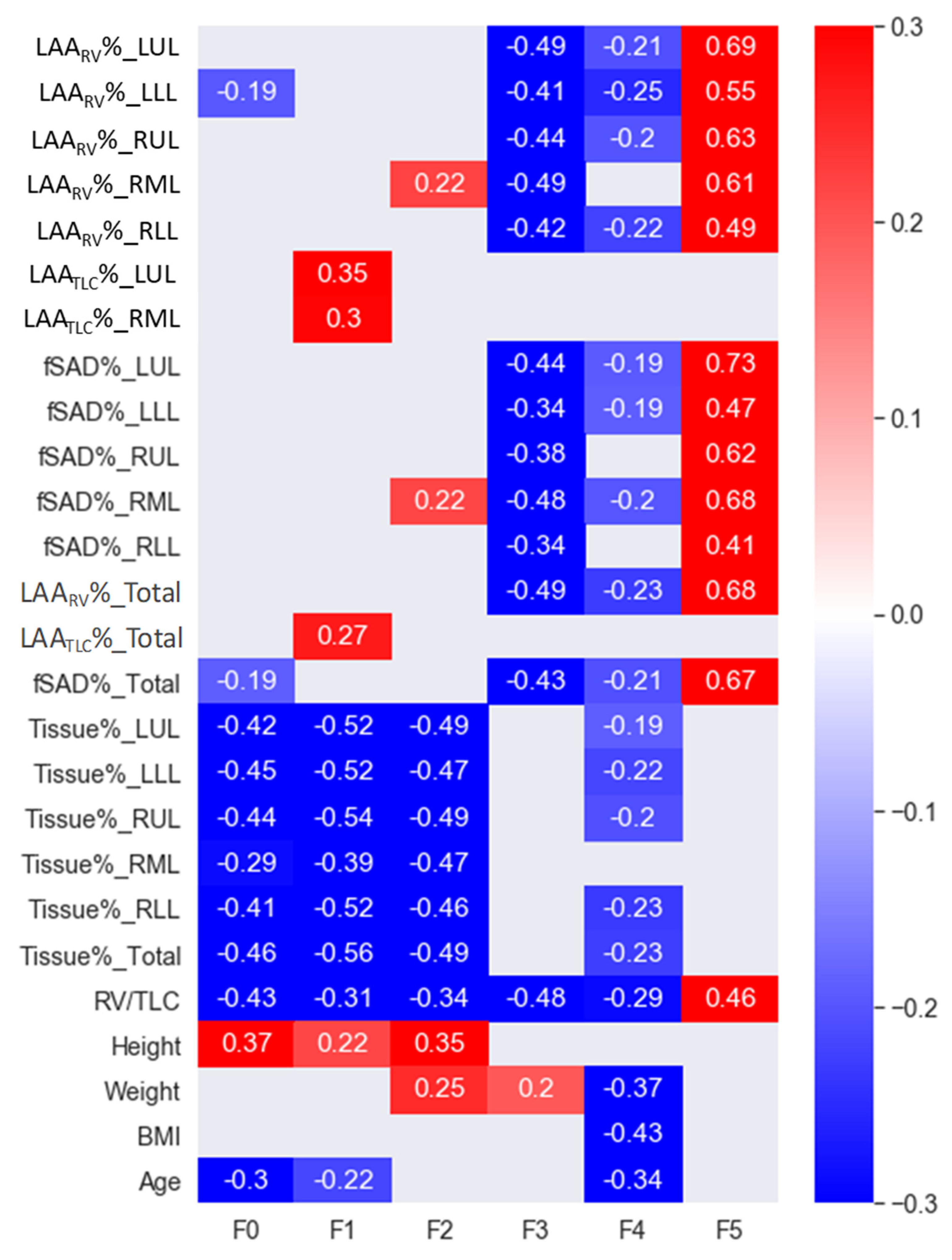
2.3. Factor Interpretation
2.4. Identification of the Subject Clusters
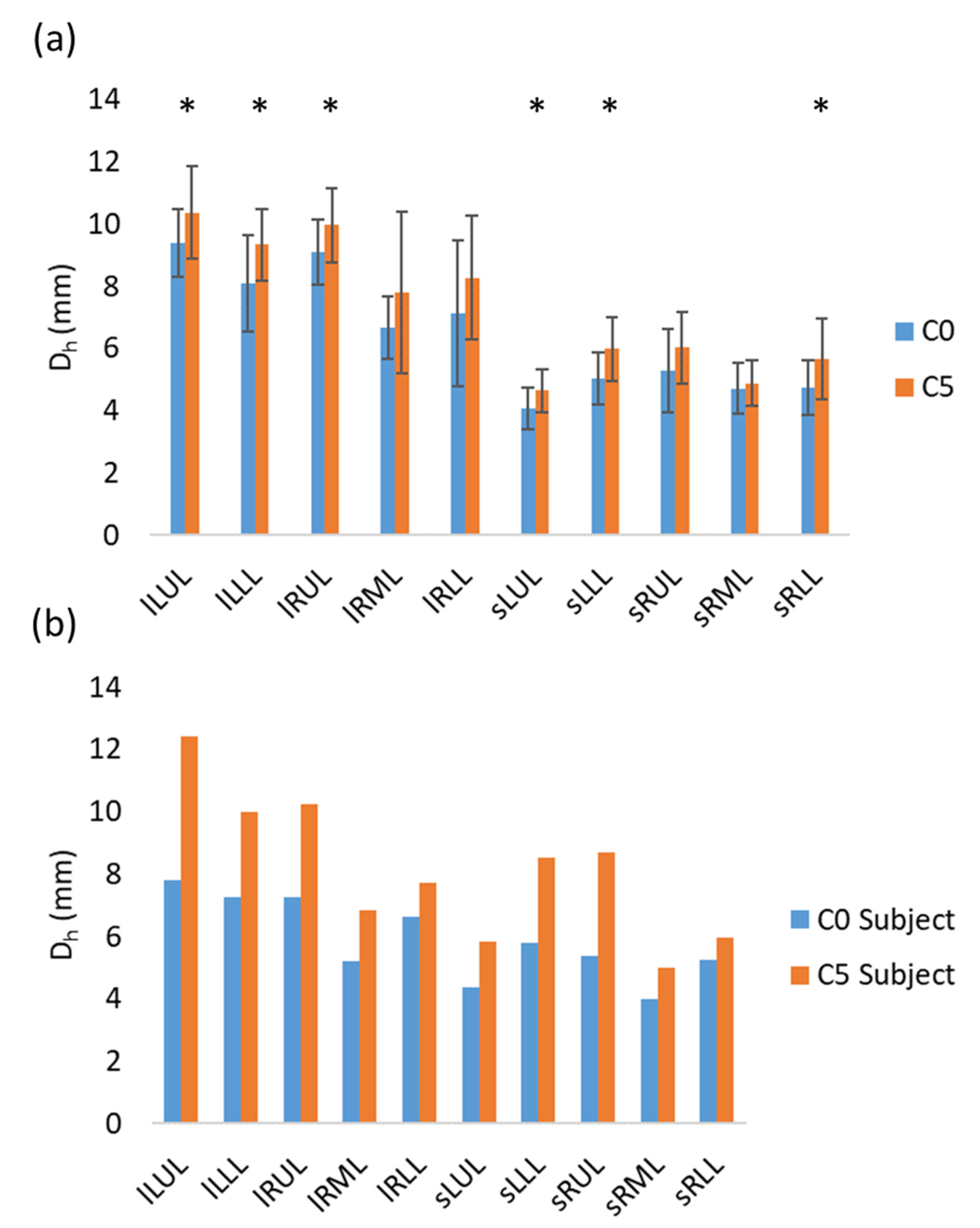
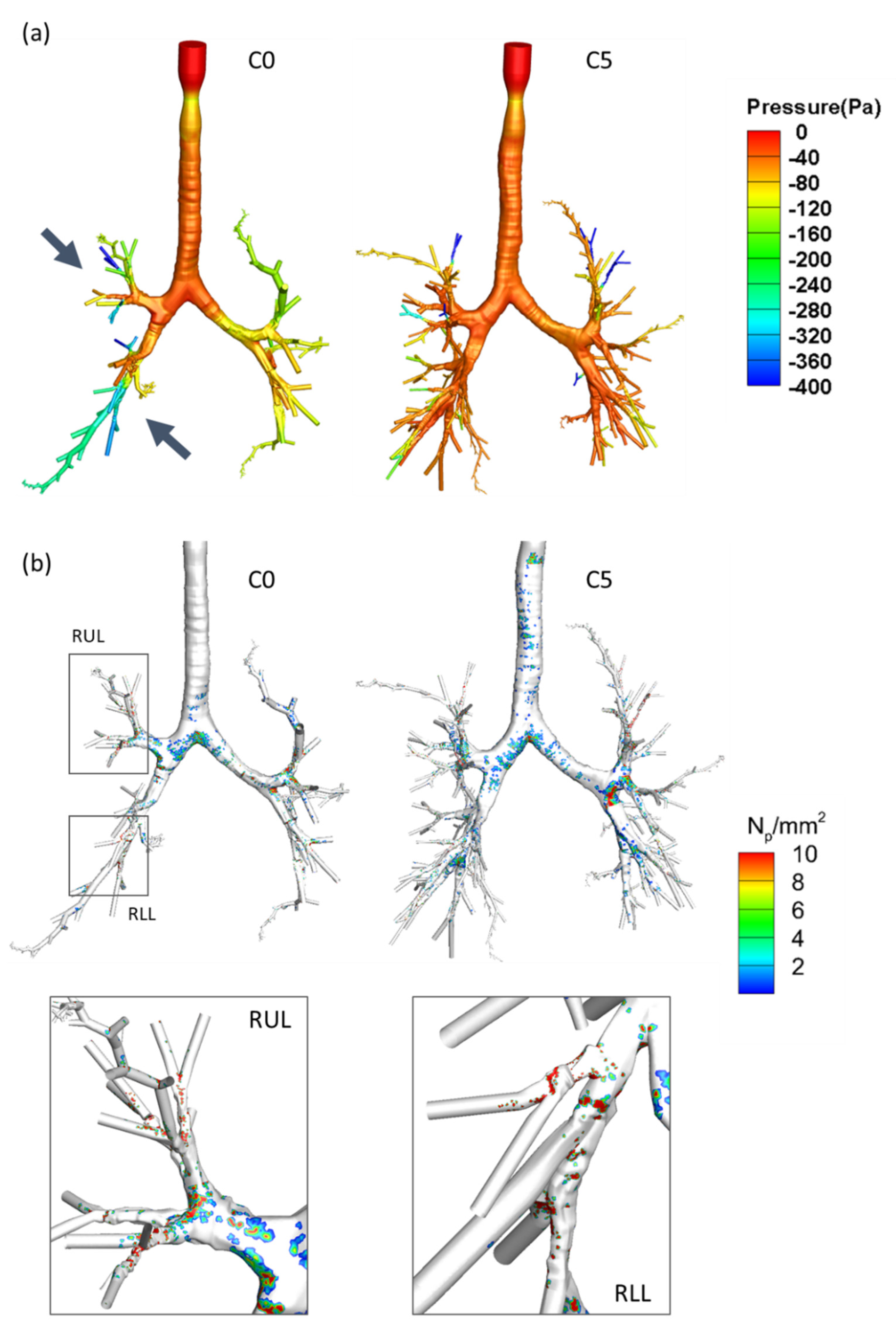
2.5. Simulations of Airflow in the Airways Using CFPD
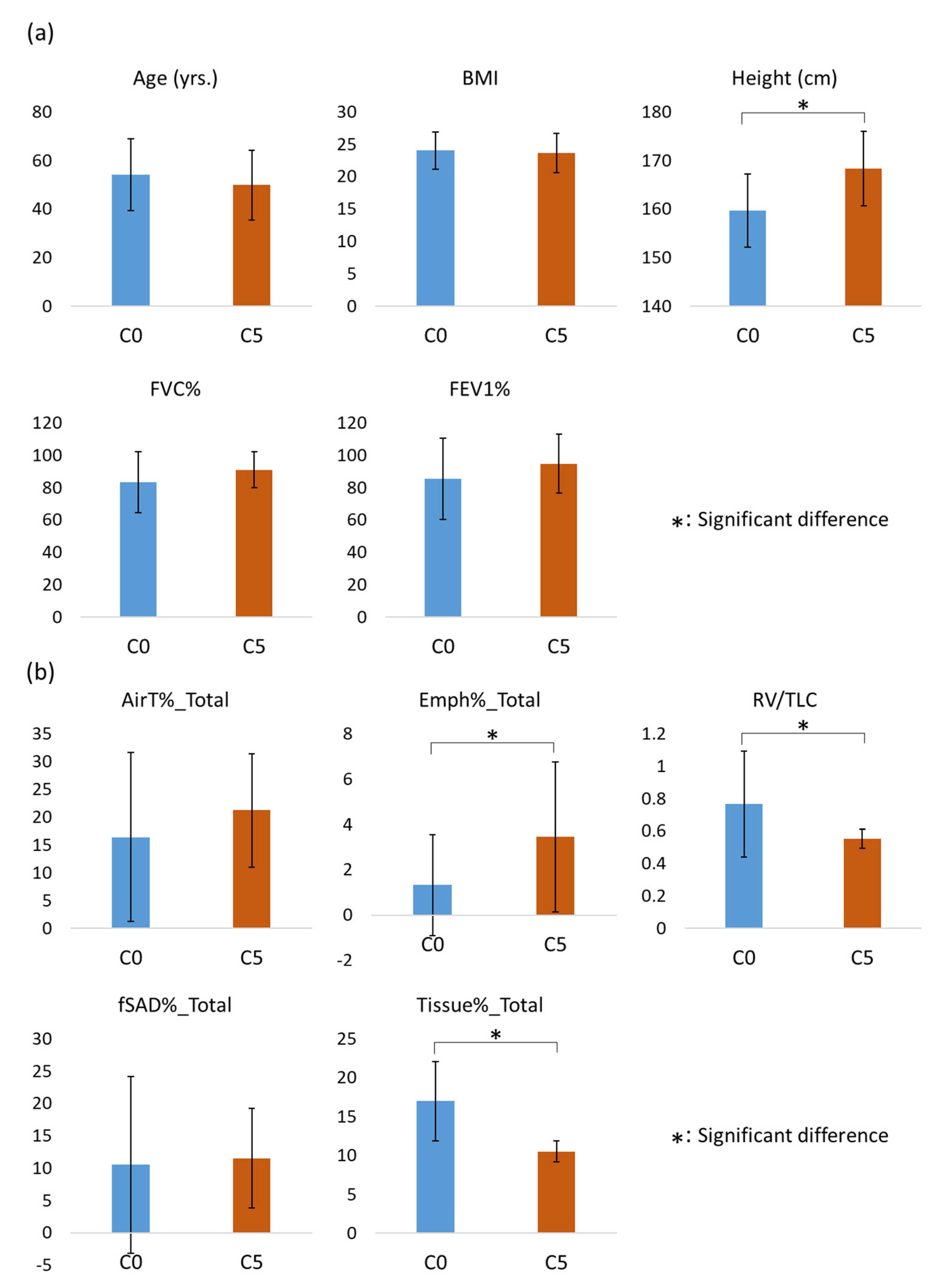
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| PFT | Pulmonary function test |
| EX | Expiration |
| IN | Inspiration |
| FEV1 | Forced expiratory volume in one second |
| FVC | Forced vital capacity |
| HD | Humidifier disinfectant |
| HDLI | HD-associated lung injuries |
| CT | Computed tomography |
| EFA | Exploratory factor analysis |
| IRB | Institutional review boards |
| ROI | Regions of interest |
| CAE | Convolutional autoencoder |
| FC | Feature constructor |
| AWV% | Airway tree to lung volume ratio |
| RV/TLC | Residual volume to total lung capacity ratio |
| CFPD | Computational fluid and particle dynamics |
| LES | Large eddy simulation |
| F0 | Factor 0 |
| F1 | Factor 1 |
| F2 | Factor 2 |
| F3 | Factor 3 |
| F4 | Factor 4 |
| F5 | Factor 5 |
| C0 | Cluster 0 |
| C1 | Cluster 1 |
| C2 | Cluster 2 |
| C3 | Cluster 3 |
| C4 | Cluster 4 |
| C5 | Cluster 5 |
| Variables below measured at different locations are denoted by {Variable}_{Location}. | |
| Variable | |
| Dh | Hydraulic luminal diameter |
| LAARV% | Low attenuation area percentage at residual volume |
| LAATLC% | Low attenuation area percentage at total lung capacity |
| fSAD% | Functional small airway disease percentage |
| J | Determinant of the Jacobian matrix |
| Location | |
| LUL | Left upper lobe |
| LLL | Left lower lobe |
| RUL | Right upper lobe |
| RML | Right middle lobe |
| RLL | Right lower lobe |
| Total | Total lung |
| sLUL | Sub-lobar subset airways at LUL |
| sLLL | Sub-lobar subset airways at LLL |
| sRUL | Sub-lobar subset airways at RUL |
| sRML | Sub-lobar subset airways at RML |
| sRLL | Sub-lobar subset airways at RLL |
| lLUL | Lobar airway at LUL |
| lLLL | Lobar airway at LLL |
| Lobar airway at RUL | Lobar airway at RUL |
| Lobar airway at RML | Lobar airway at RML |
| Lobar airway at RLL | Lobar airway at RLL |
References
- Ahn, J.-J. The humidifier disinfectant incident and the selfexamination of environmental toxicology and public health experts. Environ. Health Toxicol. 2015, 30, e2015016. [Google Scholar] [CrossRef] [PubMed]
- Ha, M.; Lee, S.Y.; Hwang, S.S.; Park, H.; Sheen, S.; Cheong, H.K.; Choi, B.Y. Evaluation report on the causal association between humidifier disinfectants and lung injury. Epidemiol. Health 2016, 38, e2016037. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.R.; Hwang, G.W.; Naganuma, A.; Chung, K.H. Adverse health effects of humidifier disinfectants in korea: Lung toxicity of polyhexamethylene guanidine phosphate. J. Toxicol. Sci. 2016, 41, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.-J.; Kim, H.-J.; Yu, J.; Lee, E.; Jung, Y.-H.; Kim, H.-Y.; Seo, J.-H.; Kwon, G.-Y.; Park, J.-H.; Gwack, J.; et al. Inhalation Toxicity of Humidifier Disinfectants as a Risk Factor of Children’s Interstitial Lung Disease in Korea: A Case-Control Study. PLoS ONE 2013, 8, e64430. [Google Scholar] [CrossRef] [PubMed]
- Park, D.-U.; Ryu, S.-H.; Roh, H.-S.; Lee, E.; Cho, H.-J.; Yoon, J.; Lee, S.-Y.; Cho, Y.A.; Do, K.-H.; Hong, S.-J. Association of high-level humidifier disinfectant exposure with lung injury in preschool children. Sci. Total Environ. 2017, 616–617, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Lee, M.S.; Hong, S.B.; Huh, J.W.; Do, K.H.; Jang, S.J.; Lim, C.M.; Chae, E.J.; Lee, H.; Jung, M.; et al. A cluster of lung injury cases associated with home humidifier use: An epidemiological investigation. Thorax 2014, 69, 703–708. [Google Scholar] [CrossRef]
- Kim, K.W.; Ahn, K.; Yang, H.J.; Lee, S.; Park, J.D.; Kim, W.K.; Kim, J.T.; Kim, H.H.; Rha, Y.H.; Park, Y.M.; et al. Humidifier disinfectant-associated children’s interstitial lung disease. Am. J. Respir. Crit. Care Med. 2014, 189, 48–56. [Google Scholar] [CrossRef]
- Yoon, J.; Kang, M.; Jung, J.; Ju, M.J.; Jeong, S.H.; Yang, W.; Choi, Y.-H. Humidifier disinfectant consumption and humidifier disinfectant-associated lung injury in South Korea: A nationwide population-based study. Int. J. Environ. Res. Public Health 2021, 18, 6136. [Google Scholar] [CrossRef]
- Kim, H.R.; Lee, K.; Park, C.W.; Song, J.A.; Shin, D.Y.; Park, Y.J.; Chung, K.H. Polyhexamethylene guanidine phosphate aerosol particles induce pulmonary inflammatory and fibrotic responses. Arch. Toxicol. 2016, 90, 617–632. [Google Scholar] [CrossRef]
- Binder, P.; Batmanghelich, N.K.; Estepar, R.S.J.; Golland, P. Unsupervised Discovery of Emphysema Subtypes in a Large Clinical Cohort. In Machine Learning in Medical Imaging; Springer: Berlin/Heidelberg, Germany, 2016; pp. 180–187. Available online: http://link.springer.com/10.1007/978-3-319-47157-0_22 (accessed on 1 October 2016).
- Haghighi, B.; Choi, S.; Choi, J.; Hoffman, E.A.; Comellas, A.P.; Newell, J.D.; Lee, C.H.; Barr, R.G.; Bleecker, E.; Cooper, C.B.; et al. Imaging-based clusters in former smokers of the COPD cohort associate with clinical characteristics: The SubPopulations and intermediate outcome measures in COPD study (SPIROMICS). Respir. Res. 2019, 20, 153. [Google Scholar] [CrossRef] [Green Version]
- Haghighi, B.; Choi, S.; Choi, J.; Hoffman, E.A.; Comellas, A.P.; Newell, J.D.; Graham Barr, R.; Bleecker, E.; Cooper, C.B.; Couper, D.; et al. Imaging-based clusters in current smokers of the COPD cohort associate with clinical characteristics: The SubPopulations and Intermediate Outcome Measures in COPD Study (SPIROMICS) 11 Medical and Health Sciences 1102 Cardiorespiratory Medicine and Haemato. Respir. Res. 2018, 19, 178. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Choi, J.; Zou, C.; Newell, J.D., Jr.; Comellas, A.P.; Lee, C.H.; Ko, H.; Barr, R.G.; Bleecker, E.R.; Cooper, C.B.; et al. Latent traits of lung tissue patterns in former smokers derived by dual channel deep learning in computed tomography images. Sci. Rep. 2021, 11, 4916. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.; Lee, S.-Y.; Lee, S.-H.; Kim, E.M.; Jung, S.; Cho, H.-J.; Lee, E.; Yang, S.-I.; Hong, S.-J. Exposure to Humidifier Disinfectants Increases the Risk for Asthma in Children. Am. J. Respir. Crit. Care Med. 2018, 198, 1583–1586. [Google Scholar] [CrossRef]
- Song, J.-H.; Ahn, J.; Park, M.Y.; Park, J.; Lee, Y.M.; Myong, J.-P.; Koo, J.-W.; Lee, J. Health Effects Associated With Humidifier Disinfectant Use: A Systematic Review for Exploration. J. Korean Med. Sci. 2022, 37, e257. [Google Scholar] [CrossRef] [PubMed]
- Haghighi, B.; DEllingwood, N.; Yin, Y.; Hoffman, E.A.; Lin, C.L. A GPU-based symmetric non-rigid image registration method in human lung. Med. Biol. Eng. Comput. 2018, 56, 355–371. [Google Scholar] [CrossRef]
- Yin, Y.; Hoffman, E.A.; Lin, C.L. Mass preserving nonrigid registration of CT lung images using cubic B-spline. Med. Phys. 2009, 36, 4213–4222. [Google Scholar] [CrossRef]
- Webb, W.R. Thin-section CT of the secondary pulmonary lobule: Anatomy and the image. Radiology 2006, 239, 322–338. [Google Scholar] [CrossRef]
- Horn, J. Factors in Factor Analysis. Psychometrika 1965, 30, 179–185. [Google Scholar] [CrossRef]
- Marsh, S.; Aldington, S.; Williams, M.V.; Nowitz, M.; Kingzett-Taylor, A.; Weatherall, M.; Shirtcliffe, P.; Pritchard, A.; Beasley, R. Physiological associations of computerized tomography lung density: A factor analysis. Int. J. Chronic Obstr. Pulm. Dis. 2006, 1, 181–187. [Google Scholar] [CrossRef]
- Costello, A.B.; Osborne, J.W. Best practices in exploratory factor analysis: Four recommendations for getting the most from your analysis. Pract. Assess. Res. Eval. 2005, 10, 7. [Google Scholar]
- Smith, B.M.; Kirby, M.; Hoffman, E.A.; Kronmal, R.A.; Aaron, S.D.; Allen, N.B.; Bertoni, A.; Coxson, H.O.; Cooper, C.; Couper, D.J.; et al. Association of Dysanapsis with Chronic Obstructive Pulmonary Disease among Older Adults. JAMA 2020, 323, 2268–2280. [Google Scholar] [CrossRef] [PubMed]
- Tanabe, N.; Sato, S.; Oguma, T.; Shima, H.; Sato, A.; Muro, S.; Hirai, T. Associations of airway tree to lung volume ratio on computed tomography with lung function and symptoms in chronic obstructive pulmonary disease. Respir. Res. 2019, 20, 77. [Google Scholar] [CrossRef] [PubMed]
- Arjomandi, M.; Zeng, S.; Barjaktarevic, I.; Barr, R.G.; Bleecker, E.R.; Bowler, R.P.; Buhr, R.G.; Criner, G.J.; Comellas, A.P.; Cooper, C.B.; et al. Radiographic lung volumes predict progression to COPD in smokers with preserved spirometry in SPIROMICS. Eur. Respir. J. 2019, 54, 1802214. [Google Scholar] [CrossRef] [PubMed]
- The Acute Respiratory Distress Syndrome Network. Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [CrossRef]
- Choi, S.; Choi, J.; Miyawaki, S.; Hoffman, E.A.; Lin, C.L. Improved Estimations Of Flow Distribution Using A 1-D Resistance Network Model In Asthmatic Airways. Am. Thorac. Soc. 2016, 193, A2495. [Google Scholar]
- Miyawaki, S.; Hoffman, E.A.; Lin, C.-L. Effect of static vs. dynamic imaging on particle transport in CT-based numerical models of human central airways. J. Aerosol Sci. 2016, 100, 129–139. [Google Scholar] [CrossRef]
- Yeh, H.C.; Schum, G.M. Models of human lung airways and their application to inhaled particle deposition. Bull. Math. Biol. 1980, 42, 461–480. [Google Scholar] [CrossRef]
- Schum, M.; Yeh, H.C. Theoretical evaluation of aerosol deposition in anatomical models of mammalian lung airways. Bull. Math. Biol. 1980, 42, 1–15. [Google Scholar] [CrossRef]
- Tawhai, M.H.; Hunter, P.; Tschirren, J.; Reinhardt, J.; McLennan, G.; Hoffman, E. CT-based geometry analysis and finite element models of the human and ovine bronchial tree. J. Appl. Physiol. 2004, 97, 2310–2321. [Google Scholar] [CrossRef]
- Kligerman, S.J.; Henry, T.; Lin, C.T.; Franks, T.J.; Galvin, J.R. Mosaic attenuation: Etiology, methods of differentiation, and pitfalls. Radiographics 2015, 35, 1360–1380. [Google Scholar] [CrossRef]
- Kouranos, V.; Jacob, J.; Nicholson, A.; Renzoni, E. Fibrotic Hypersensitivity Pneumonitis: Key Issues in Diagnosis and Management. J. Clin. Med. 2017, 6, 62. [Google Scholar] [CrossRef] [PubMed]
- Ryu, H.; Choi, Y.H.; Kim, E.; Park, J.; Lee, S.; Yoon, J.; Jo, E.K.; Choe, Y.; Heo, J.; Yang, W. Misclassification and characterization of exposure to humidifier disinfectants using a questionnaire. BMC Public Health 2021, 21, 1458. [Google Scholar] [CrossRef] [PubMed]
- Paek, D.; Koh, Y.; Park, D.-U.; Cheong, H.-K.; Do, K.-H.; Lim, C.-M.; Hong, S.-J.; Kim, Y.-H.; Leem, J.-H.; Chung, K.H.; et al. Nationwide study of humidifier disinfectant lung injury in South Korea, 1994–2011 incidence and dose-response relationships. Ann. Am. Thorac. Soc. 2015, 12, 1813–1821. [Google Scholar] [CrossRef]
- Dunlap, J.W.; Thurstone, L.L. The Vectors of the Mind. Am. J. Psychol. 1937, 49, 329. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exposed (n = 96) | Non-Exposed (n = 25) | Total (n = 121) | p | |
|---|---|---|---|---|
| Age (yrs.) | 49.86 | 45.44 | 48.95 | 0.116 |
| (15.43) | (11.38) | (14.75) | ||
| BMI (kg/cm2) | 23.40 | 24.72 | 23.67 | 0.057 |
| (3.21) | (2.94) | (3.19) | ||
| Height (cm) | 163.95 | 169.96 | 165.20 | 0.002 |
| (7.89) | (8.15) | (8.28) | ||
| Weight (kg) | 63.11 | 71.76 | 64.91 | 0.003 |
| (10.94) | (12.06) | (11.68) | ||
| FVC (% of pred) | 87.16 | 99.28 | 89.68 | <0.001 |
| (16.64) | (7.17) | (15.92) | ||
| FEV1 (% of pred) | 89.53 | 107.72 | 93.32 | <0.001 |
| (20.86) | (10.51) | (20.52) | ||
| Gender (%) | 45.8/54.2 | 16.0/84.0 | 39.7/60.3 | 0.013 |
| (Female/Male) |
| C0 | C1 | C2 | C5 | p | |
|---|---|---|---|---|---|
| Age (yrs.) | 54.41 | 48.96 | 40.89 | 49.91 | 0.005 |
| (15.55) | (14.43) | (12.03) | (14.36) | ||
| BMI (kg/cm2) | 23.74 | 25.14 | 22.29 | 23.65 | 0.038 |
| (3.19) | (2.69) | (3.37) | (3.03) | ||
| Height (cm) | 161.55 | 163.35 | 166.96 | 168.33 | <0.001 |
| (8.40) | (7.44) | (8.32) | (7.61) | ||
| Weight (kg) | 62.16 | 67.43 | 62.65 | 67.25 | 0.142 |
| (10.81) | (11.12) | (13.24) | (10.96) | ||
| FVC (% pred) | 81 | 93.7 | 94.75 | 91 | 0.104 |
| (18.34) | (16.74) | (14.60) | (11.17) | ||
| FEV1 (% pred) | 82.58 | 98.48 | 101.18 | 94.76 | 0.064 |
| (24.40) | (17.38) | (13.86) | (18.15) | ||
| Gender (%) | 59.4/40.6 | 52.2/47.8 | 39.3/60.7 | 15.2/84.8 | <0.001 |
| (Female/Male) | |||||
| Exposure (%) | 96.9/3.1 | 87.0/13.0 | 82.1/17.9 | 51.5/48.5 | <0.001 |
| (Yes/No) | |||||
| Time of Exposure (hrs.) | 15,075.72 | 11,293.16 | 10,459.82 | 15,928.53 | 0.61 |
| (18,150.32) | (10,507.95) | (10,561.51) | (21,145.16) | ||
| PHMG or PGH (Count) | 17 | 14 | 13 | 9 | 0.65 |
| CMIT or MIT (Count) | 1 | 2 | 1 | 0 | |
| PHMG AND CMIT (Count) | 9 | 2 | 5 | 6 | |
| Other HDs (Count) | 2 | 1 | 3 | 2 |
| Exposure | No | Yes | Total |
|---|---|---|---|
| Cluster | |||
| C0 | 1 | 31 | 32 |
| C1 | 3 | 20 | 23 |
| C2 | 5 | 23 | 28 |
| C3 | 0 | 1 | 1 |
| C4 | 0 | 4 | 4 |
| C5 | 16 | 17 | 33 |
| C0 | C1 | C2 | C5 | |
|---|---|---|---|---|
| Height | -- | -- | - | |
| BMI | + | |||
| FVC % pred | ||||
| FEV1 % pred | ||||
| RV/TLC | + | - | - | |
| RV | - | - | - | |
| TLC | --- | |||
| LAARV% | - | -- | -- | |
| fSAD% | - | -- | -- | |
| Tissue% | +++ | ++ | ||
| LAATLC% | -- | -- | - | |
| F1 | +++ | |||
| F2 | -- | +++ | ||
| F3 | --- | +++ | ||
| F5 | +++ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, F.; Choi, J.; Zhang, X.; Rajaraman, P.K.; Lee, C.-H.; Ko, H.; Chae, K.-J.; Park, E.-K.; Comellas, A.P.; Hoffman, E.A.; et al. Characterizing Subjects Exposed to Humidifier Disinfectants Using Computed-Tomography-Based Latent Traits: A Deep Learning Approach. Int. J. Environ. Res. Public Health 2022, 19, 11894. https://doi.org/10.3390/ijerph191911894
Li F, Choi J, Zhang X, Rajaraman PK, Lee C-H, Ko H, Chae K-J, Park E-K, Comellas AP, Hoffman EA, et al. Characterizing Subjects Exposed to Humidifier Disinfectants Using Computed-Tomography-Based Latent Traits: A Deep Learning Approach. International Journal of Environmental Research and Public Health. 2022; 19(19):11894. https://doi.org/10.3390/ijerph191911894
Chicago/Turabian StyleLi, Frank, Jiwoong Choi, Xuan Zhang, Prathish K. Rajaraman, Chang-Hyun Lee, Hongseok Ko, Kum-Ju Chae, Eun-Kee Park, Alejandro P. Comellas, Eric A. Hoffman, and et al. 2022. "Characterizing Subjects Exposed to Humidifier Disinfectants Using Computed-Tomography-Based Latent Traits: A Deep Learning Approach" International Journal of Environmental Research and Public Health 19, no. 19: 11894. https://doi.org/10.3390/ijerph191911894