
Risk Factors for Cancer Mortality in Spain: Population-Based Cohort Study

 and
and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Baseline Measurements
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Main Findings
4.2. Comparison with Other Studies
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2020; Available online: https://gco.iarc.fr/today (accessed on 25 September 2021).
- ECIS—European Cancer Information System. European Union, 2021. Available online: https://ecis.jrc.ec.europa.eu (accessed on 2 November 2021).
- De Angelis, R.; Sant, M.; Coleman, M.P.; Francisci, S.; Baili, P.; Pierannunzio, D.; Tarama, A.; Visser, O.; Brenner, H.; Ardanaz, E.; et al. Cancer survival in Europe 1999–2007 by country and age: Results of EUROCARE--5-a population-based study. Lancet Oncol. 2014, 15, 23–34. [Google Scholar] [CrossRef]
- Estimaciones de la Incidencia del Cáncer en España, 2021. Red Española de Registros de Cáncer (REDECAN). 2021. Available online: https://redecan.org/storage/documents/b05bfad2-4b48-4519-9f56-6aad911e80b0.pdf (accessed on 4 October 2021).
- Bernard, W.; Stewart Christopher, P. World Cancer Report 2014; International Agency for Research on Cancer: Lyon, France, 2014. [Google Scholar]
- Benhamou, S. Cancers related to tobacco smoking. Rev Prat. 1993, 43, 1214–1217. [Google Scholar] [PubMed]
- WHO Regional Office for Europe. Alcohol and Cancer in the WHO European Reagion: An Appeal for the Better Prevention; WHO Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- Hashibe, M.; Brennan, P.; Chuang, S.C.; Boccia, S.; Castellsague, X.; Chen, C.; Curado, M.P.; Dal Maso, L.; Daudt, A.W.; Fabianova, E.; et al. Interaction between tobacco and alcohol use and the risk of head and neck cancer: Pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. Cancer Epidemiol. Biomark. Prev. 2009, 18, 541–550. [Google Scholar] [CrossRef] [Green Version]
- van Elsland, D.; Neefjes, J. Bacterial infections and cancer. EMBO Rep. 2018, 19, e46632. [Google Scholar] [CrossRef]
- Matthews, C.E.; Moore, S.C.; Arem, H.; Cook, M.B.; Trabert, B.; Håkansson, N.; Larsson, S.C.; Wolk, A.; Gapstur, S.M.; Lynch, B.M.; et al. Amount and Intensity of Leisure-Time Physical Activity and Lower Cancer Risk. J. Clin. Oncol. 2020, 38, 686–697. [Google Scholar] [CrossRef]
- Moore, S.C.; Lee, I.M.; Weiderpass, E.; Campbell, P.T.; Sampson, J.N.; Kitahara, C.M.; Keadle, S.K.; Arem, H. Association of Leisure-Time Physical Activity with Risk of 26 Types of Cancer in 1.44 Million Adults. JAMA Intern. Med. 2016, 176, 816–825. [Google Scholar] [CrossRef]
- Inoue, M.; Yamamoto, S.; Kurahashi, N.; Iwasaki, M.; Sasazuki, S.; Tsugane, S. Japan Public Health Center-based Prospective Study Group. Daily total physical activity level and total cancer risk in men and women: Results from a large-scale population-based cohort study in Japan. Am. J. Epidemiol. 2008, 168, 391–403. [Google Scholar] [CrossRef] [Green Version]
- McTiernan, A.; Friedenreich, C.M.; Katzmarzyk, P.T.; Powell, K.E.; Macko, R.; Buchner, D.; Pescatello, L.S.; Bloodgood, B.; Tennant, B.; Vaux-Bjerke, A.; et al. Physical Activity in Cancer Prevention and Survival: A Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1252–1261. [Google Scholar] [CrossRef]
- European Core Health Indicators (ECHI). Comisión Europea, 2021. Available online: https://ec.europa.eu/health/indicators_data/indicators_es (accessed on 9 September 2021).
- Encuesta Nacional de Salud de España 2011. Instituto Nacional de Estadistica, 2021. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176783&menu=resultados&idp=1254735573175#!tabs-1254736195295 (accessed on 10 October 2021).
- Putter, H.; Fiocco, M.; Geskus, R.B. Tutorial in biostatistics: Competing risks and multi-state models. Stat. Med. 2007, 26, 2389–2430. [Google Scholar] [CrossRef]
- Moore, D.F. Applied Survival Analysis Using R; Springer: New York, NY, USA, 2016. [Google Scholar]
- Gómez-Beneyto, M.; Nolasco, A.; Moncho, J.; Pereyra-Zamora, P.; Tamayo-Fonseca, N.; Munarriz, M.; Salazar, J.; Tabarés-Seisdedos, R.; Girón, M. Psychometric behaviour of the strengths and difficulties questionnaire (SDQ) in the Spanish national health survey 2006. BMC Psychiatry 2013, 13, 95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, M.; Cioffi, G.; Wang, J.; Waite, K.A.; Ostrom, Q.T.; Kruchko, C.; Lathia, J.D.; Rubin, J.B.; Berens, M.E.; Connor, J.; et al. Sex Differences in Cancer Incidence and Survival: A Pan-Cancer Analysis. Cancer Epidemiol. Biomark. Prev. 2020, 29, 1389–1397. [Google Scholar] [CrossRef] [PubMed]
- Goldman, N.; Glei, D.A.; Weinstein, M. What Matters Most for Predicting Survival? A Multinational Population-Based Cohort Study. PLoS ONE 2016, 11, e0159273. [Google Scholar] [CrossRef] [PubMed]
- Cook, M.B.; McGlynn, K.A.; Devesa, S.S.; Freedman, N.D.; Anderson, W.F. Sex disparities in cancer mortality and survival. Cancer Epidemiol. Biomarkers Prev. 2011, 20, 1629–1637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, T. Educational initiatives in geriatric oncology—Who, why, and how? J. Geriatr. Oncol. 2016, 7, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2015. CA Cancer J. Clin. 2015, 65, 5–29. [Google Scholar] [CrossRef]
- Zinger, A.; Cho, W.C.; Ben-Yehuda, A. Cancer and Aging—the Inflammatory Connection. Aging Dis. 2017, 8, 611–627. [Google Scholar] [CrossRef] [Green Version]
- Levitz, J.S.; Bradley, T.P.; Golden, A.L. Overview of smoking and all cancers. Med. Clin. North Am. 2004, 88, 1655–1675. [Google Scholar] [CrossRef]
- Harris, J.E.; Thun, M.J.; Mondul, A.M.; Calle, E.E. Cigarette tar yields in relation to mortality from lung cancer in the cancer prevention study II prospective cohort, 1982–1988. BMJ 2004, 328, 72. [Google Scholar] [CrossRef] [Green Version]
- Katzmarzyk, P.T.; Powell, K.E.; Jakicic, J.M.; Troiano, R.P.; Piercy, K.; Tennant, B.; 2018 Physical Activity Guidelines Advisory Committee. Sedentary Behavior and Health: Update from the 2018 Physical Activity Guidelines Advisory Committee. Med. Sci. Sports Exerc. 2019, 51, 1227–1241. [Google Scholar] [CrossRef] [PubMed]
- Papandreou, C.; Becerra-Tomás, N.; Bulló, M.; Martínez-González, M.Á.; Corella, D.; Estruch, R.; Ros, E.; Arós, F.; Schroder, H.; Fitó, M.; et al. Legume consumption and risk of all-cause, cardiovascular, and cancer mortality in the PREDIMED study. Clin. Nutr. 2019, 38, 348–356. [Google Scholar] [CrossRef] [Green Version]
- Zhong, X.S.; Ge, J.; Chen, S.W.; Xiong, Y.Q.; Ma, S.J.; Chen, Q. Association between Dietary Isoflavones in Soy and Legumes and Endometrial Cancer: A Systematic Review and Meta-Analysis. J. Acad. Nutr. Diet. 2018, 118, 637–651. [Google Scholar] [CrossRef] [PubMed]
- Pehrsson, S.K.; Linnersjö, A.; Hammar, N. Cancer risk of patients with ischaemic syndromes. J. Intern. Med. 2005, 258, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Dreyer, L.; Olsen, J.H. Cancer risk of patients discharged with acute myocardial infarct. Epidemiology 1998, 9, 178–183. [Google Scholar] [CrossRef]
- Rinde, L.B.; Småbrekke, B.; Hald, E.M.; Brodin, E.E.; Njølstad, I.; Mathiesen, E.B.; Løchen, M.L.; Wilsgaard, T.; Brækkan, S.K.; Vik, A.; et al. Myocardial infarction and future risk of cancer in the general population-the Tromsø Study. Eur. J. Epidemiol. 2017, 32, 193–201. [Google Scholar] [CrossRef]
- Ross, J.S.; Stagliano, N.E.; Donovan, M.J.; Breitbart, R.E.; Ginsburg, G.S. Atherosclerosis and cancer: Common molecular pathways of disease development and progression. Ann. N. Y. Acad. Sci. 2001, 947, 271–292; discussion 292–293. [Google Scholar] [CrossRef]
- Mellemkjaer, L.; Linet, M.S.; Gridley, G.; Frisch, M.; Møller, H.; Olsen, J.H. Rheumatoid arthritis and cancer risk. Eur. J. Cancer. 1996, 32A, 1753–1757. [Google Scholar] [CrossRef]
- Gridley, G.; McLaughlin, J.K.; Ekbom, A.; Klareskog, L.; Adami, H.O.; Hacker, D.G.; Hoover, R.; Fraumeni, J.F., Jr. Incidence of cancer among patients with rheumatoid arthritis. J. Natl. Cancer Inst. 1993, 85, 307–311. [Google Scholar] [CrossRef]
- Abásolo, L.; Júdez, E.; Descalzo, M.A.; González-Alvaro, I.; Jover, J.A.; Carmona, L.; EMECAR Study Group. Cancer in rheumatoid arthritis: Occurrence, mortality, and associated factors in a South European population. Semin. Arthritis Rheum. 2008, 37, 388–397. [Google Scholar] [CrossRef]
- Turner, M.C. Epidemiological evidence: IgE and solid tumors. In Cancer and IgE: Introducing the Concept of AllergoOncology; Penichet, M.L., Jensen-Jarolim, E., Eds.; Springer: New York, NY, USA, 2010; pp. 47–77. [Google Scholar]
- Josephs, D.H.; Spicer, J.F.; Corrigan, C.J.; Gould, H.J.; Karagiannis, S.N. Epidemiological associations of allergy, IgE and cancer. Clin. Exp. Allergy 2013, 43, 1110–1123. [Google Scholar] [CrossRef] [PubMed]
- Skillrud, D.M.; Offord, K.P.; Miller, R.D. Higher risk of lung cancer in chronic obstructive pulmonary disease. A prospective, matched, controlled study. Ann. Intern. Med. 1986, 105, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Kuller, L.H.; Ockene, J.; Meilahn, E.; Svendsen, K.H. Relation of forced expiratory volume in one second (FEV1) to lung cancer mortality in the Multiple Risk Factor Intervention Trial (MRFIT). Am. J. Epidemiol. 1990, 132, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Hansson, L.E.; Nyrén, O.; Hsing, A.W.; Bergström, R.; Josefsson, S.; Chow, W.H.; Fraumeni, J.F., Jr.; Adami, H.O. The risk of stomach cancer in patients with gastric or duodenal ulcer disease. N. Engl. J. Med. 1996, 335, 242–249. [Google Scholar] [CrossRef]
- Graham, D.Y. History of Helicobacter pylori, duodenal ulcer, gastric ulcer and gastric cancer. World J. Gastroenterol. 2014, 20, 5191–5204. [Google Scholar] [CrossRef]
- El-Serag, H.B.; Rudolph, K.L. Hepatocellular carcinoma: Epidemiology and molecular carcinogenesis. Gastroenterology 2007, 132, 2557–2576. [Google Scholar] [CrossRef]
- Fattovich, G.; Stroffolini, T.; Zagni, I.; Donato, F. Hepatocellular carcinoma in cirrhosis: Incidence and risk factors. Gastroenterology 2004, 127 (Suppl. 1), S35–S50. [Google Scholar] [CrossRef]
- Kalaitzakis, E.; Gunnarsdottir, S.A.; Josefsson, A.; Björnsson, E. Increased risk for malignant neoplasms among patients with cirrhosis. Clin. Gastroenterol Hepatol. 2011, 9, 168–174. [Google Scholar] [CrossRef]
- McGinty, E.E.; Zhang, Y.; Guallar, E.; Ford, D.E.; Steinwachs, D.; Dixon, L.B.; Keating, N.L.; Daumit, G.L. Cancer incidence in a sample of Maryland residents with serious mental illness. Psychiatr. Serv. 2012, 63, 714–717. [Google Scholar] [CrossRef] [Green Version]
- Grassi, L.; Riba, M. Cancer and severe mental illness: Bi-directional problems and potential solutions. Psycho-Oncol. 2020, 29, 1445–1451. [Google Scholar] [CrossRef]


{kind=link}
| Variables | n | % | |
|---|---|---|---|
| Mortality | Survived | 19,290 | 94.6% |
| Death due to neoplasm | 340 | 1.7% | |
| Death from other cause | 767 | 3.8% | |
| Age group (years) | <50 | 12,015 | 58.9% |
| 50–59 | 3106 | 15.2% | |
| 60–69 | 2393 | 11.7% | |
| 70–79 | 1767 | 8.7% | |
| ≥80 | 1115 | 5.5% | |
| Sex | Male | 9942 | 48.7% |
| Female | 10,455 | 51.3% | |
| Body mass index | Normal (<25 kg/m2) | 9019 | 44.2% |
| Overweight (25.0 to <30 kg/m2) | 6803 | 33.4% | |
| Obese (≥30 kg/m2) | 3144 | 15.4% | |
| NA | 1431 | 7.0% | |
| Tobacco use | Never smoker | 10,908 | 53.5% |
| Ex-smoker | 3971 | 19.5% | |
| Smoker | 5518 | 27.1% | |
| Alcohol intake | None | 10,857 | 53.2% |
| Low risk (≤20 g/week women and ≤40 g/week men) | 9029 | 44.3% | |
| Risky drinking (>20 g/week women and >40 g/week men) | 511 | 2.5% | |
| Physical activity | Sedentary | 9051 | 44.4% |
| Occasional physical activity | 6735 | 33.0% | |
| Frequent physical activity | 2668 | 13.1% | |
| Athletic training | 1943 | 9.5% | |
| Vegetable intake | Daily | 9566 | 46.9% |
| ≥3 servings a week | 6990 | 34.3% | |
| 1–2 servings a week | 2761 | 13.5% | |
| <1 serving a week | 690 | 3.4% | |
| Rarely or never | 390 | 1.9% | |
| Intake of legumes | Daily | 312 | 1.5% |
| ≥3 servings a week | 4738 | 23.2% | |
| 1–2 servings a week | 12,161 | 59.6% | |
| <1 serving a week | 2400 | 11.8% | |
| Rarely or never | 786 | 3.9% | |
| Self-perceived health | Very good | 4396 | 21.6% |
| Good | 10,413 | 51.0% | |
| Okay | 4065 | 19.9% | |
| Bad | 1224 | 6.0% | |
| Very bad | 299 | 1.5% | |
| Comorbidities | Hypertension | 4278 | 21.0% |
| Diabetes mellitus | 1465 | 7.2% | |
| Malignant tumor | 575 | 2.8% | |
| Health services use | Hospital admission in previous 12 months | 1695 | 8.3% |
| Primary care visit in previous 30 days | 5719 | 28.0% | |
| CT scan in previous 12 months | 1536 | 7.5% | |
| Ultrasound in previous 12 months | 2925 | 14.3% | |
| MRI in previous 12 months | 1513 | 7.4% |
| Variable | Beta | Error | HR | 95% CI | p Value | |
|---|---|---|---|---|---|---|
| Autonomous communities | Murcia | 0 | – | 1 | ||
| Andalusia | 0.785 | 0.227 | 2.19 | (1.40–3.42) | 0.001 | |
| Castilla y León | 0.736 | 0.239 | 2.09 | (1.31–3.33) | 0.002 | |
| Asturias | 0.735 | 0.251 | 2.09 | (1.28–3.41) | 0.003 | |
| Rioja | 0.727 | 0.261 | 2.07 | (1.24–3.45) | 0.005 | |
| Extremadura | 0.717 | 0.252 | 2.05 | (1.25–3.36) | 0.004 | |
| Balearic Islands | 0.547 | 0.284 | 1.73 | (0.99–3.02) | 0.054 | |
| Basque Country | 0.530 | 0.252 | 1.70 | (1.04–2.78) | 0.036 | |
| Canary Islands | 0.512 | 0.264 | 1.67 | (1.00–2.80) | 0.052 | |
| Valencian Community | 0.490 | 0.236 | 1.63 | (1.03–2.59) | 0.038 | |
| Madrid | 0.455 | 0.240 | 1.58 | (0.98–2.52) | 0.058 | |
| Aragon | 0.439 | 0.247 | 1.55 | (0.96–2.52) | 0.075 | |
| Catalonia | 0.283 | 0.233 | 1.33 | (0.84–2.10) | 0.22 | |
| Castilla-La Mancha | 0.273 | 0.249 | 1.31 | (0.81–2.14) | 0.27 | |
| Navarra | 0.245 | 0.286 | 1.28 | (0.73–2.24) | 0.39 | |
| Cantabria | 0.156 | 0.267 | 1.17 | (0.69–1.97) | 0.56 | |
| Galicia | 0.042 | 0.244 | 1.04 | (0.65–1.68) | 0.86 | |
| Ceuta-Melilla | −0.020 | 0.361 | 0.98 | (0.48–1.99) | 0.96 | |
| Age group (years) | <50 | 0 | – | 1 | ||
| 50–59 | 2.188 | 0.389 | 8.92 | (4.16–19.11) | <0.001 | |
| 60–69 | 2.848 | 0.371 | 17.25 | (8.34–35.70) | <0.001 | |
| 70–79 | 3.336 | 0.378 | 28.10 | (13.39–58.94) | <0.001 | |
| ≥80 | 3.819 | 0.391 | 45.58 | (21.18–98.09) | <0.001 | |
| Sex | Male | 0.443 | 0.095 | 1.56 | (1.29–1.88) | <0.001 |
| Tobacco use | Never smoker | 0 | – | – | ||
| Ex-smoker | 0.366 | 0.169 | 1.44 | (1.04–2.01) | 0.030 | |
| Smoker | 0.603 | 0.233 | 1.83 | (1.16–2.89) | 0.010 | |
| Physical activity | Sedentary | 0 | – | 1 | ||
| Occasional physical activity | −0.549 | 0.094 | 0.58 | (0.48–0.69) | <0.001 | |
| Frequent physical activity | −0.703 | 0.296 | 0.50 | (0.28–0.88) | 0.017 | |
| Athletic training | −0.593 | 0.247 | 0.55 | (0.34–0.90) | 0.017 | |
| Intake of legumes | Daily | 0 | – | 1 | ||
| ≥3 servings a week | 0.075 | 0.366 | 1.08 | (0.53–2.21) | 0.84 | |
| 1–2 servings a week | 0.045 | 0.356 | 1.05 | (0.52–2.10) | 0.90 | |
| <1 serving a week | 0.222 | 0.377 | 1.25 | (0.60–2.61) | 0.56 | |
| Rarely or never | 0.824 | 0.403 | 2.28 | (1.03–5.02) | 0.041 | |
| Self-perceived health | Very good | 0 | – | 1 | ||
| Good | 0.498 | 0.216 | 1.65 | (1.08–2.51) | 0.021 | |
| Okay | 0.916 | 0.221 | 2.50 | (1.62–3.85) | <0.001 | |
| Bad | 1.035 | 0.239 | 2.82 | (1.76–4.50) | <0.001 | |
| Very bad | 1.365 | 0.270 | 3.91 | (2.31–6.64) | <0.001 | |
| Physical limitations in previous 30 days | Severely limited | 0 | – | 1 | ||
| Moderately limited | −0.453 | 0.126 | 0.64 | (0.50–0.81) | <0.001 | |
| Not limited | −0.745 | 0.140 | 0.48 | (0.36–0.62) | <0.001 | |
| Myocardial infarction | 0.318 | 0.143 | 1.37 | (1.04–1.82) | 0.026 | |
| Arthrosis or arthritis | −0.651 | 0.153 | 0.52 | (0.39–0.70) | <0.001 | |
| Chronic allergy | −0.424 | 0.135 | 0.66 | (0.50–0.85) | 0.002 | |
| COPD | 0.476 | 0.113 | 1.61 | (1.29–2.01) | <0.001 | |
| Gastrointestinal ulcer | −0.307 | 0.137 | 0.74 | (0.56–0.96) | 0.025 | |
| Cirrhosis | 0.482 | 0.194 | 1.62 | (1.11–2.37) | 0.013 | |
| Mental health problems | 0.698 | 0.159 | 2.01 | (1.47–2.75) | <0.001 | |
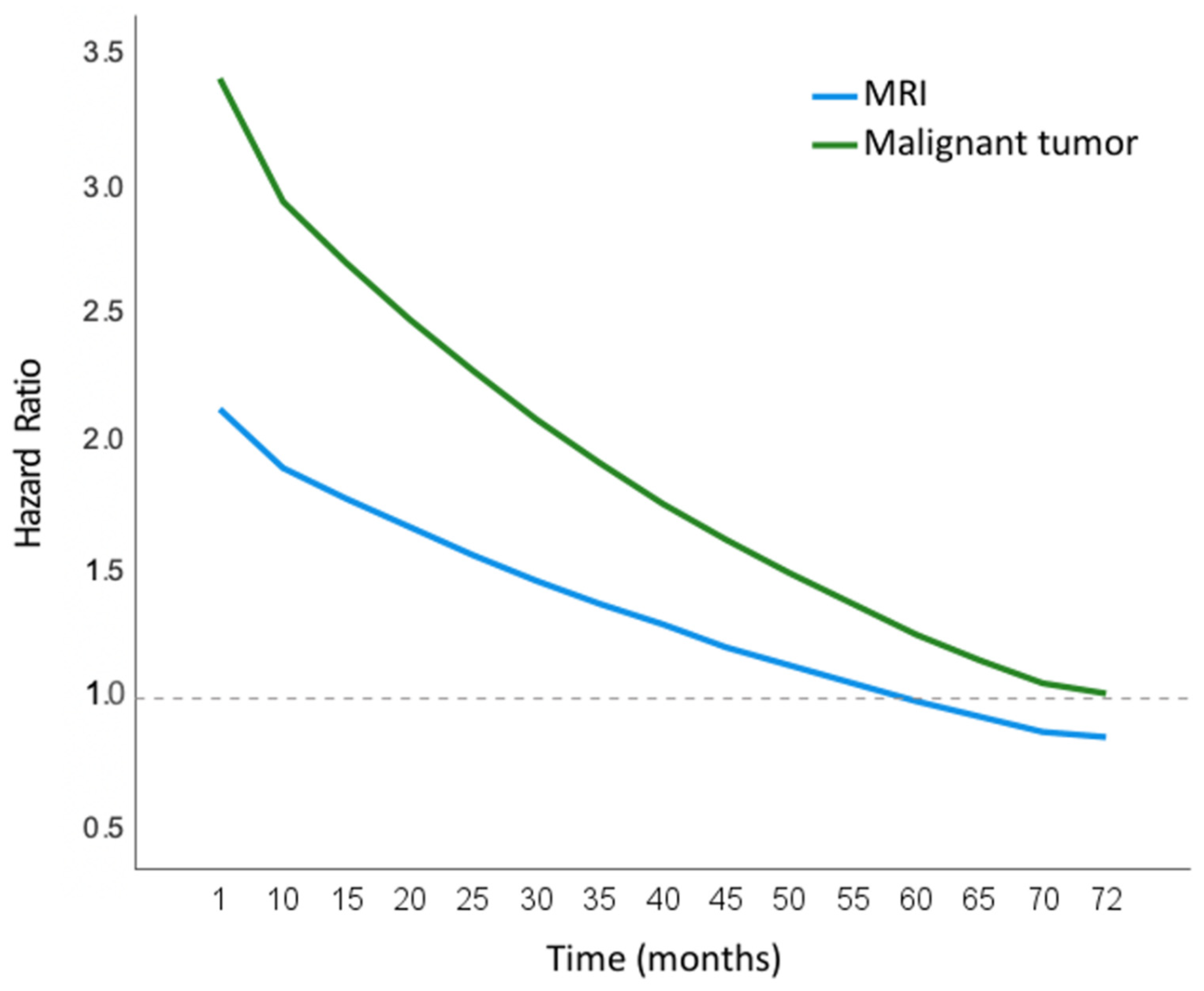
| Malignant tumor | 1.247 | 0.258 | 3.48 | (2.10–5.77) | <0.001 | |
| MRI in previous 12 months | 0.771 | 0.289 | 2.16 | (1.23–3.81) | 0.008 | |
| Malignant tumors × T | −0.017 | 0.006 | 0.98 | (0.97–1.00) | 0.004 | |
| MRI in previous 12 months × T | −0.013 | 0.006 | 0.99 | (0.98–1.00) | 0.039 | |
| Age group: | <50 | 0 | 1 | |||
| others causes | 50–59 | −1.408 | 0.504 | 0.25 | (0.09–0.66) | 0.005 |
| 60–69 | −1.070 | 0.459 | 0.34 | (0.14–0.84) | 0.020 | |
| 70–79 | −0.304 | 0.459 | 0.74 | (0.30–1.81) | 0.51 | |
| ≥80 | 0.426 | 0.464 | 1.53 | (0.62–3.80) | 0.36 | |
| Tobacco: | Never smoker | 0 | 1 | |||
| others causes | Ex-smoker | −0.436 | 0.192 | 0.65 | (0.44–0.94) | 0.023 |
| Smoker | −0.229 | 0.290 | 0.80 | (0.45–1.40) | 0.43 | |
| Arthrosis: others causes | Yes | 0.489 | 0.176 | 1.63 | (1.16–2.30) | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lázaro-Sánchez, A.D.; Juárez Marroquí, A.; Quesada Rico, J.A.; Orozco-Beltrán, D. Risk Factors for Cancer Mortality in Spain: Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 9852. https://doi.org/10.3390/ijerph19169852
Lázaro-Sánchez AD, Juárez Marroquí A, Quesada Rico JA, Orozco-Beltrán D. Risk Factors for Cancer Mortality in Spain: Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(16):9852. https://doi.org/10.3390/ijerph19169852
Chicago/Turabian StyleLázaro-Sánchez, Antonio D., Asunción Juárez Marroquí, Jose Antonio Quesada Rico, and Domingo Orozco-Beltrán. 2022. "Risk Factors for Cancer Mortality in Spain: Population-Based Cohort Study" International Journal of Environmental Research and Public Health 19, no. 16: 9852. https://doi.org/10.3390/ijerph19169852