
Using Ambulatory Care Sensitive Conditions to Assess Primary Health Care Performance during Disasters: A Systematic Review

 , , ,
, , ,  ,
,  and
and 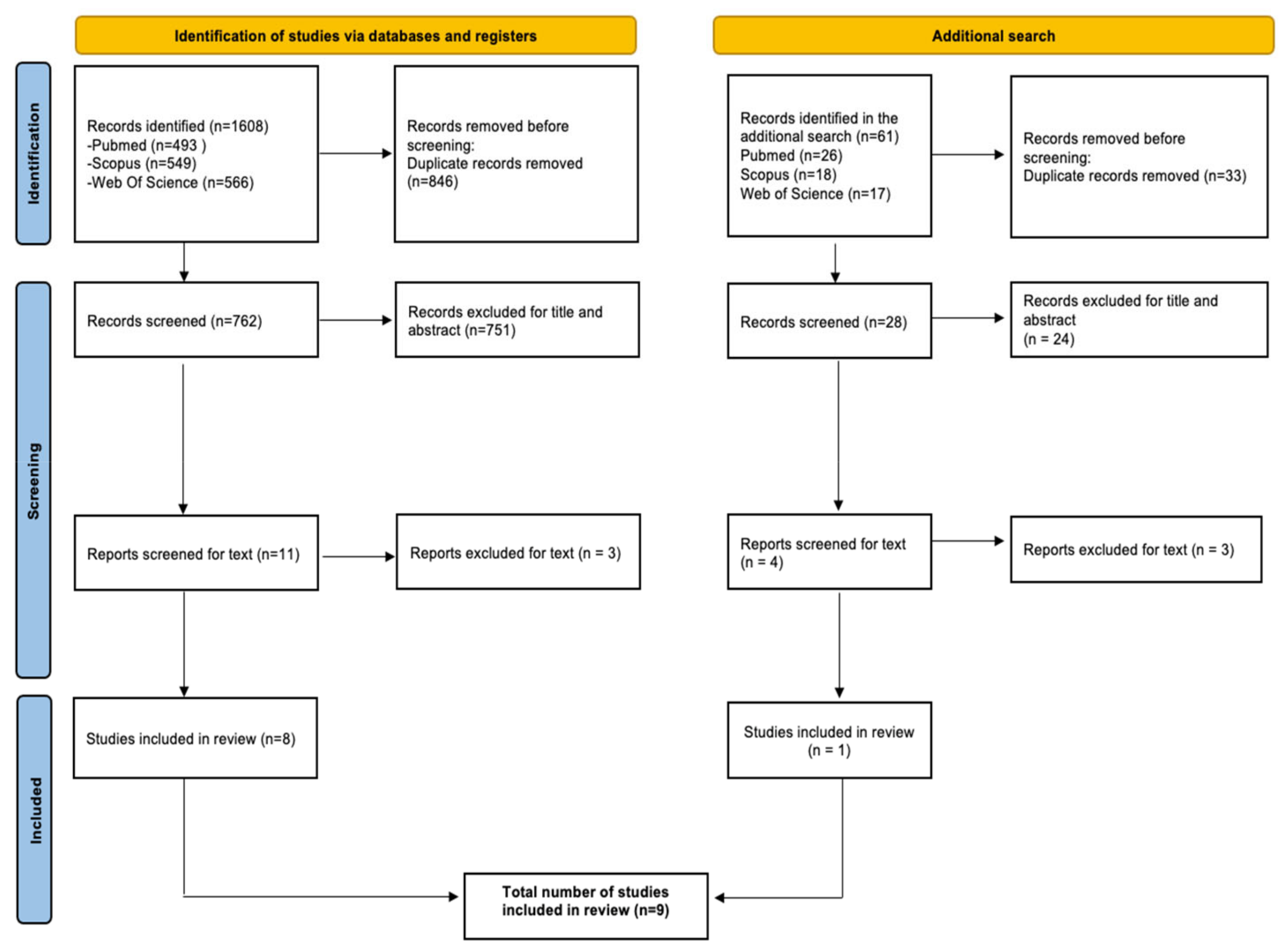{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Eligibility Criteria
2.2. Data Extraction and Synthesis
3. Results
3.1. Target Populations
3.2. Types of ACSCs
3.3. Studies’ Objectives and Main Results
3.4. Vulnerable Populations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bayntun, C. A Health System Approach to All-Hazards Disaster Management: A Systematic Review. PLoS Curr. 2012, 4, e50081cad5861d. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Health Emergency and Disaster Risk Management Framework; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Redwood-Campbell, L.; Abrahams, J. Primary Health care and Disasters—The Current State of the Literature: What We Know, Gaps and Next Steps. Prehospital Disaster Med. 2011, 26, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Runkle, J.D.; Brock-Martin, A.; Karmaus, W.; Svendsen, E.R. Secondary Surge Capacity: A Framework for Understanding Long-Term Access to Primary Care for Medically Vulnerable Populations in Disaster Recovery. Am. J. Public Health 2012, 102, e24–e32. [Google Scholar] [CrossRef] [PubMed]
- OECD. Health at a Glance 2015; OECD Indicators; OECD Publishing: Paris, France, 2015. [Google Scholar] [CrossRef]
- Caminal, J.; Starfield, B.; Sánchez, E.; Casanova, C.; Morales, M. The role of primary care in preventing ambulatory care sensitive conditions. Eur. J. Public Health 2004, 14, 246–251. [Google Scholar] [CrossRef] [Green Version]
- Muenchberger, H.; Kendall, E. Predictors of preventable hospitalization in chronic disease: Priorities for change. J. Public Health Policy 2010, 31, 150–163. [Google Scholar] [CrossRef]
- Berlin, C.; Busato, A.; Rosemann, T.; Djalali, S.; Maessen, M. Avoidable hospitalizations in Switzerland: A small area analysis on regional variation, density of physicians, hospital supply and rurality. BMC Health Serv. Res. 2014, 14, 289. [Google Scholar] [CrossRef] [Green Version]
- Billings, J.; Anderson, G.M.; Newman, L.S. Recent Findings on Preventable Hospitalizations. Health Aff. 1996, 15, 239–249. [Google Scholar] [CrossRef]
- Rosano, A.; Loha, C.A.; Falvo, R.; Van Der Zee, J.; Ricciardi, W.; Guasticchi, G.; De Belvis, A.G. The relationship between avoidable hospitalization and accessibility to primary care: A systematic review. Eur. J. Public Health 2013, 23, 356–360. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization Regional Office for Europe. Assessing Health Services Delivery Performance with Hospitalizations for Ambulatory Care Sensitive Conditions Working Document; WHO Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Sarmento, J.; Rocha, J.V.M.; Santana, R. Defining ambulatory care sensitive conditions for adults in Portugal. BMC Health Serv. Res. 2020, 20, 754. [Google Scholar] [CrossRef]
- Hodgson, K.; Deeny, S.R.; Steventon, A. Ambulatory Care-Sensitive Conditions: Their Potential Uses and Limitations. BMJ Qual. Saf. 2019, 28, 429–433. [Google Scholar] [CrossRef] [Green Version]
- Rocha, J.V.M.; Sarmento, J.; Moita, B.; Marques, A.P.; Santana, R. Comparative research aspects on hospitalizations for ambulatory care sensitive conditions: The case of Brazil and Portugal. Ciência Saúde Coletiva 2020, 25, 1375–1388. [Google Scholar] [CrossRef]
- Helmer, D.A.; Dwibedi, N.; Rowneki, M.; Tseng, C.-L.; Fried, D.; Rose, D.; Jani, N.; Sambamoorthi, U. Mental Health Conditions and Hospitalizations for Ambulatory Care Sensitive Conditions Among Veterans with Diabetes. Am. Health Drug Benefits 2020, 13, 61. [Google Scholar]
- Phillips, K.G.; Wishengrad, J.S.; Houtenville, A.J. Ambulatory Care Sensitive Conditions among All-Payer Claimants with Intellectual and Developmental Disabilities. Am. J. Intellect. Dev. Disabil. 2021, 126, 203–215. [Google Scholar] [CrossRef]
- Dias, B.M.; Zanetti, A.C.B.; Pereira, A.C. Expenses of Hospitalization for Ambulatory Care Sensitive Conditions in the Health Regional Offices of the State of São Paulo. Einstein 2021, 19, eGS5817. [Google Scholar] [CrossRef]
- Fischbach, D. Hospital Costs of Ambulatory Care-Sensitive Conditions in Germany. Gesundheitswesen 2016, 78, 168–174. [Google Scholar] [CrossRef]
- Roos, L.L.; Dragan, R.; Schroth, R.J. Pediatric ambulatory care sensitive conditions: Birth cohorts and the socio-economic gradient. Can. J. Public Health 2017, 108, e257–e264. [Google Scholar] [CrossRef]
- Anderson, T.S.; Karliner, L.S.; Lin, G.A. Association of Primary Language and Hospitalization for Ambulatory Care Sensitive Conditions. Med. Care 2019, 58, 45–51. [Google Scholar] [CrossRef]
- Leventer-Roberts, M.; Cohen-Stavi, C.; Hoshen, M.; Gofer, I.; Sherf, M.; Balicer, R. Analyzing admission rates for multiple ambulatory care–sensitive conditions. Am. J. Manag. Care 2020, 26, e155–e161. [Google Scholar] [CrossRef]
- Walsh, M.E.; Cronin, S.; Boland, F.; Ebell, M.H.; Fahey, T.; Wallace, E. Geographical variation of emergency hospital admissions for ambulatory care sensitive conditions in older adults in Ireland 2012–2016. BMJ Open 2021, 11, e042779. [Google Scholar] [CrossRef]
- Leuchter, R.K.; Villaflores, C.W.A.; Norris, K.C.; Sorensen, A.; Vangala, S.; Sarkisian, C.A. Racial Disparities in Potentially Avoidable Hospitalizations During the COVID-19 Pandemic. Am. J. Prev. Med. 2021, 61, 235–239. [Google Scholar] [CrossRef]
- Runkle, J.R.; Zhang, H.; Karmaus, W.; Brock-Martin, A.; Svendsen, E.R. Long-Term Impact of Environmental Public Health Disaster on Health System Performance. South. Med. J. 2013, 106, 74–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Runkle, J.D.; Zhang, H.; Karmaus, W.; Martin, A.B.; Svendsen, E.R. Prediction of Unmet Primary Care Needs for the Medically Vulnerable Post-Disaster: An Interrupted Time-Series Analysis of Health System Responses. Int. J. Environ. Res. Public Health 2012, 9, 3384–3397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, N.V.; Karmakar, M.; Tipirneni, R.; Ayanian, J.Z. Trends in Hospitalizations for Ambulatory Care–Sensitive Conditions During the COVID-19 Pandemic. JAMA Netw. Open 2022, 5, e222933. [Google Scholar] [CrossRef] [PubMed]
- Wright, B.; Anderson, D.; Whitaker, R.; Shrader, P.; Bettger, J.P.; Wong, C.; Shafer, P. Comparing health care use and costs among new Medicaid enrollees before and during the COVID-19 pandemic. BMC Health Serv. Res. 2021, 21, 1152. [Google Scholar] [CrossRef] [PubMed]
- Sasabuchi, Y.; Matsui, H.; Yasunaga, H.; Fushimi, K. Increase in avoidable hospital admissions after the Great East Japan Earthquake. J. Epidemiol. Community Health 2017, 71, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Sasabuchi, Y.; Matsui, H.; Kotani, K.; Lefor, A.K.; Yasunaga, H. Effect of the 2016 Kumamoto earthquakes on preventable hospital admissions: A retrospective cohort study in Japan. BMJ Open 2018, 8, e021294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.-T.; Lee, Y.-C.; Hsiao, C.-J. Hospitalization for Ambulatory-care-sensitive Conditions in Taiwan Following the SARS Outbreak: A Population-based Interrupted Time Series Study. J. Formos. Med. Assoc. 2009, 108, 386–394. [Google Scholar] [CrossRef] [Green Version]
- Rennert-May, E.; Leal, J.; Thanh, N.X.; Lang, E.; Dowling, S.; Manns, B.; Wasylak, T.; Ronksley, P.E. The impact of COVID-19 on hospital admissions and emergency department visits: A population-based study. PLoS ONE 2021, 16, e0252441. [Google Scholar] [CrossRef]
- Johnston, S.; Sorel, M.E.; Sidney, S. Effects of the September 11th attacks on urgent and emergent medical evaluations in a Northern California managed care plan. Am. J. Med. 2002, 113, 556–562. [Google Scholar] [CrossRef]
- Saxena, S.; George, J.; Barber, J.; Fitzpatrick, J.; Majeed, A. Association of population and practice factors with potentially avoidable admission rates for chronic diseases in London: Cross sectional analysis. J. R. Soc. Med. 2006, 99, 81–89. [Google Scholar] [CrossRef] [Green Version]
- Wong, L.E.; Hawkins, J.; Langness, S.; Karen, L.; Murrell, P.; Sammann, A. Where Are All the Patients? Addressing Covid-19 Fear to Encourage Sick Patients to Seek Emergency Care. NEJM Catal. 2020, 1, 1–12. [Google Scholar] [CrossRef]
- Lima, C.K.T.; Carvalho, P.M.D.M.; Lima, I.D.A.A.S.; Nunes, J.V.A.D.O.; Saraiva, J.S.; de Souza, R.I.; da Silva, C.G.L.; Neto, M.L.R. The emotional impact of Coronavirus 2019-nCoV (new Coronavirus disease). Psychiatry Res. 2020, 287, 112915. [Google Scholar] [CrossRef]
- Lu, T.-H.; Chou, Y.-J.; Liou, C.-S. Impact of SARS on healthcare utilization by disease categories: Implications for delivery of healthcare services. Health Policy 2007, 83, 375–381. [Google Scholar] [CrossRef]
- McCabe, R.; Schmit, N.; Christen, P.; D’Aeth, J.C.; Løchen, A.; Rizmie, D.; Nayagam, S.; Miraldo, M.; Aylin, P.; Bottle, A.; et al. Adapting hospital capacity to meet changing demands during the COVID-19 pandemic. BMC Med. 2020, 18, 1–12. [Google Scholar] [CrossRef]
- Jones, R. Oxford Textbook of Primary Medical Care: Clinical Management; Oxford University Press: Oxford, UK, 2004; Volume 2, pp. 3–9. [Google Scholar]
- Fonseca, V.A.; Smith, H.; Kuhadiya, N.; Leger, S.M.; Yau, C.L.; Reynolds, K.; Shi, L.; McDuffie, R.H.; Thethi, T.; John-Kalarickal, J. Impact of a Natural Disaster on Diabetes: Exacerbation of Disparities and Long-Term Consequences. Diabetes Care 2009, 32, 1632–1638. [Google Scholar] [CrossRef] [Green Version]
- Islam, T.; Muntner, P.; Webber, L.S.; Morisky, D.E.; Krousel-Wood, M.A. Cohort Study of Medication Adherence in Older Adults (CoSMO): Extended Effects of Hurricane Katrina on Medication Adherence among Older Adults. Am. J. Med. Sci. 2008, 336, 105–110. [Google Scholar] [CrossRef] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamberti-Castronuovo, A.; Valente, M.; Aleni, C.; Hubloue, I.; Ragazzoni, L.; Barone-Adesi, F. Using Ambulatory Care Sensitive Conditions to Assess Primary Health Care Performance during Disasters: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 9193. https://doi.org/10.3390/ijerph19159193
Lamberti-Castronuovo A, Valente M, Aleni C, Hubloue I, Ragazzoni L, Barone-Adesi F. Using Ambulatory Care Sensitive Conditions to Assess Primary Health Care Performance during Disasters: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(15):9193. https://doi.org/10.3390/ijerph19159193
Chicago/Turabian StyleLamberti-Castronuovo, Alessandro, Martina Valente, Chiara Aleni, Ives Hubloue, Luca Ragazzoni, and Francesco Barone-Adesi. 2022. "Using Ambulatory Care Sensitive Conditions to Assess Primary Health Care Performance during Disasters: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 15: 9193. https://doi.org/10.3390/ijerph19159193