
Predicting Return to Work Following Myocardial Infarction: A Prospective Longitudinal Cohort Study


Abstract
:1. Introduction
Review of the Literature
2. Materials and Methods
2.1. Aims
- (1)
- What proportion of patients with myocardial infarction returned to work by three-months post-discharge in South Korea?
- (2)
- What demographic, behavioral, and clinical factors predicted these patients’ return to work?
2.2. Design
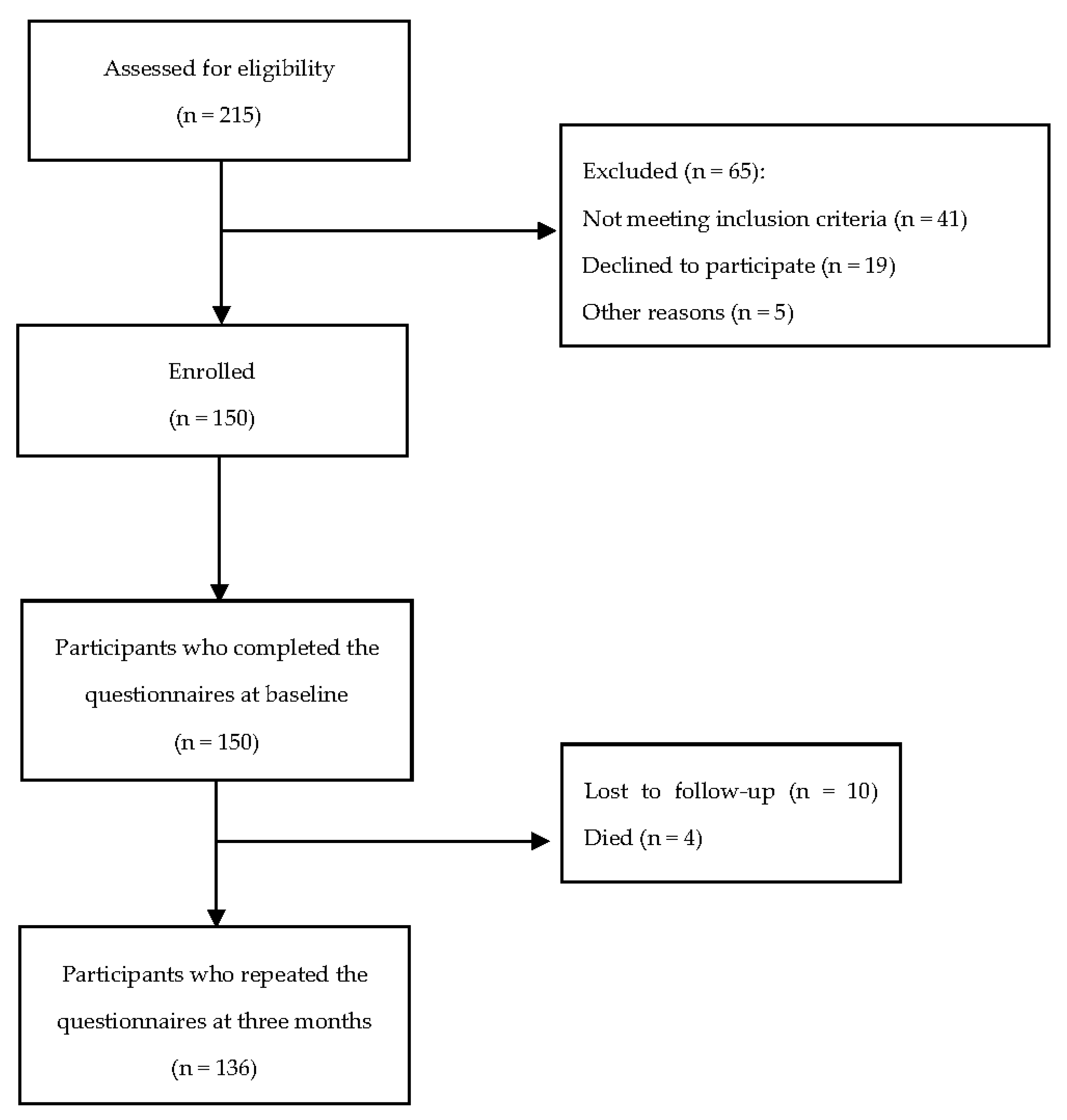
2.3. Participants
2.4. Data Collection
2.5. Data Collection Instruments
2.5.1. Demographic, Behavioral, and Clinical Data
2.5.2. Depression, Anxiety, and Stress Scale
2.5.3. The ENRICHD Social Support Inventory
2.6. Ethical Considerations
2.7. Data Analysis
3. Results
3.1. Baseline Characteristics
3.2. Demographic, Behavioral, Clinical, and Psychosocial Characteristics at Three Months Post-Discharge
3.3. Return to Work at Three Months Follow-Up
3.4. Predictors of Return to Work at Three Months Follow-Up
4. Discussion
4.1. Implications
4.1.1. Clinical Practice
4.1.2. Education for Healthcare Providers and Patients
4.1.3. Policy Making
4.1.4. Future Research
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UK Factsheet. Available online: https://www.bhf.org.uk/-/media/files/research/heart-statistics/bhf-cvd-statistics-uk-factsheet.pdf?la=en&rev=0236a2601cee471f92581ec3e34877b3&hash=A57E69DEDC391138A8D652B1B31BE7B8C2AA1554 (accessed on 25 March 2021).
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2021 Update: A Report from the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef] [PubMed]
- Causes of Death, Australia. Available online: https://www.abs.gov.au/statistics/health/causes-death/causes-death-australia/latest-release (accessed on 23 October 2020).
- Lee, S.W.; Kim, H.C.; Lee, H.S.; Suh, I. Thirty-Year Trends in Mortality from Cardiovascular Diseases in Korea. Korean Circ. J. 2015, 45, 202–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jayaraj, J.C.; Davatyan, K.; Subramanian, S.S.; Priya, J. Epidemiology of myocardial infarction. In Myocardial Infarction; Pamukçu, B., Ed.; IntechOpen: London, UK, 2019; pp. 9–19. [Google Scholar]
- Health Status: Health Conditions. Available online: https://www.aihw.gov.au/reports-data/australias-health-performance/australias-health-performance-framework/national/all-australia/conditions/health-conditions/3_1_1 (accessed on 25 March 2021).
- Kang, K.; Gholizadeh, L.; Han, H.-R. Health-related Quality of Life and Its Predictors in Korean Patients with Myocardial Infarction in the Acute Phase. Clin. Nurs. Res. 2019, 30, 161–170. [Google Scholar] [CrossRef]
- Kang, K.; Gholizadeh, L.; Inglis, S.C.; Han, H.-R. Correlates of health-related quality of life in patients with myocardial infarction: A literature review. Int. J. Nurs. Stud. 2017, 73, 1–16. [Google Scholar] [CrossRef]
- Warraich, H.J.; Kaltenbach, L.A.; Fonarow, G.C.; Peterson, E.D.; Wang, T.Y. Adverse Change in Employment Status after Acute Myocardial Infarction: Analysis from the TRANSLATE-ACS study. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004528. [Google Scholar] [CrossRef]
- Dreyer, R.P.; Xu, X.; Zhang, W.; Du, X.; Strait, K.M.; Bierlein, M.; Bucholz, E.M.; Geda, M.; Fox, J.; D’Onofrio, G.; et al. Return to Work after Acute Myocardial Infarction: Comparison between young women and men. Circ. Cardiovasc. Qual. Outcomes 2016, 9, S45–S52. [Google Scholar] [CrossRef] [Green Version]
- Mirmohammadi, S.J.; Sadr-Bafghi, S.M.; Mehrparvar, A.H.; Gharavi, M.; Davari, M.H.; Bahaloo, M.; Mostaghaci, M.; Sadr-Bafghi, S.A.; Shokouh, P. Evaluation of the return to work and its duration after myocardial infarction. ARYA Atheroscler. 2014, 10, 137–140. [Google Scholar]
- Jiang, Z.; Dreyer, R.P.; Spertus, J.A.; Masoudi, F.A.; Li, J.; Zheng, X.; Li, X.; Wu, C.; Bai, X.; Hu, S.; et al. Factors Associated with Return to Work after Acute Myocardial Infarction in China. JAMA Netw. Open 2018, 1, e184831. [Google Scholar] [CrossRef]
- Stendardo, M.; Bonci, M.; Casillo, V.; Miglio, R.; Giovannini, G.; Nardini, M.; Campo, G.; Fucili, A.; Boschetto, P. Predicting return to work after acute myocardial infarction: Socio-occupational factors overcome clinical conditions. PLoS ONE 2018, 13, e0208842. [Google Scholar] [CrossRef]
- Benefits of Returning to Work. Available online: https://www.worksafe.qld.gov.au/rehabilitation-and-return-to-work/getting-back-to-work/benefits-of-returning-to-work (accessed on 7 September 2020).
- Fukuoka, Y.; Dracup, K.; Takeshima, M.; Ishii, N.; Makaya, M.; Groah, L.; Kyriakidis, E. Effect of job strain and depressive symptoms upon returning to work after acute coronary syndrome. Soc. Sci. Med. 2009, 68, 1875–1881. [Google Scholar] [CrossRef]
- Haennel, R.G.; Tomczak, C.R. Exercise rehabilitation and return to work following a cardiac event. In Ergonomics for Rehabilitation Professionals, 1st ed.; Kumar, S., Ed.; CRC Press: Boca Raton, FL, USA, 2009; pp. 243–269. [Google Scholar]
- Hämäläinen, H.; Mäki, J.; Virta, L.; Keskimäki, I.; Mähönen, M.; Moltchanov, V.; Salomaa, V. Return to work after first myocardial infarction in 1991–1996 in Finland. Eur. J. Public Health 2004, 14, 350–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutton, J.M.; Perkins, S.J. A qualitative study of men’s experience of myocardial infarction. Psychol. Health Med. 2008, 13, 87–97. [Google Scholar] [CrossRef]
- Sjöström-Strand, A.; Ivarsson, B.; Sjöberg, T. Women’s experience of a myocardial infarction: 5 years later. Scand. J. Caring Sci. 2010, 25, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Johansson, A.; Dahlberg, K.; Ekebergh, M. Living with Experiences Following a Myocardial Infarction. Eur. J. Cardiovasc. Nurs. 2003, 2, 229–236. [Google Scholar] [CrossRef]
- Woodruffe, S.; Neubeck, L.; Clark, R.A.; Gray, K.; Ferry, C.; Finan, J.; Sanderson, S.; Briffa, T.G. Australian Cardiovascular Health and Rehabilitation Association (ACRA) Core Components of Cardiovascular Disease Secondary Prevention and Cardiac Rehabilitation 2014. Heart Lung Circ. 2015, 24, 430–441. [Google Scholar] [CrossRef]
- Du, R.; Wang, P.; Ma, L.; Larcher, L.M.; Wang, T.; Chen, C. Health-related quality of life and associated factors in patients with myocardial infarction after returning to work: A cross-sectional study. Health Qual. Life Outcomes 2020, 18, 190. [Google Scholar] [CrossRef]
- Yonezawa, R.; Masuda, T.; Matsunaga, A.; Takahashi, Y.; Saitoh, M.; Ishii, A.; Kutsuna, T.; Matsumoto, T.; Yamamoto, K.; Aiba, N.; et al. Effects of Phase II Cardiac Rehabilitation on Job Stress and Health-Related Quality of Life after Return to Work in Middle-Aged Patients with Acute Myocardial Infarction. Int. Heart J. 2009, 50, 279–290. [Google Scholar] [CrossRef] [Green Version]
- Sun, W.; Gholizadeh, L.; Perry, L.; Kang, K.; Heydari, M. Factors associated with return to work following myocardial infarction: A systematic review of observational studies. J. Clin. Nurs. 2020, 30, 323–340. [Google Scholar] [CrossRef]
- Kang, K.; Gholizadeh, L.; Han, H.-R.; Inglis, S.C. Predictors of health-related quality of life in korean patients with myocardial infarction: A longitudinal observational study. Heart Lung 2018, 47, 142–148. [Google Scholar] [CrossRef]
- Caruana, E.J.; Roman, M.; Hernández-Sánchez, J.; Solli, P. Longitudinal studies. J. Thorac. Dis. 2015, 7, E537–E540. [Google Scholar] [CrossRef]
- South Korea Retirement Age-Men. Available online: https://tradingeconomics.com/south-korea/retirement-age-men (accessed on 2 April 2020).
- Organization for Economic Cooperation and Development. Ageing and Employment Policies: Working Better with Age: Korea; OECD Publishing: Paris, France, 2018; pp. 35–50. [Google Scholar]
- Henry, J.D.; Crawford, J.R. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2005, 44, 227–239. [Google Scholar] [CrossRef] [Green Version]
- Di Giacomo, M.; Davidson, P.M.; VanderPluym, A.; Snell, R.; Worrall-Carter, L. Depression, anxiety and stress in women following acute coronary syndrome: Implications for secondary prevention. Aust. Crit. Care 2007, 20, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Jun, D.; Johnston, V.; Kim, J.-M.; O’Leary, S. Cross-cultural adaptation and validation of the Depression, Anxiety and Stress Scale-21 (DASS-21) in the Korean working population. Work 2018, 59, 93–102. [Google Scholar] [CrossRef]
- Lee, E.-H.; Moon, S.H.; Cho, M.S.; Park, E.S.; Kim, S.Y.; Han, J.S.; Cheio, J.H. The 21-Item and 12-Item Versions of the Depression Anxiety Stress Scales: Psychometric Evaluation in a Korean Population. Asian Nurs. Res. 2019, 13, 30–37. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, P.H.; Powell, L.; Blumenthal, J.; Norten, J.; Ironson, G.; Pitula, C.R.; Froelicher, E.S.; Czajkowski, S.; Youngblood, M.; Huber, M.; et al. A Short Social Support Measure for Patients Recovering from Myocardial Infarction: The ENRICHD Social Support Inventory. J. Cardiopulm. Rehabil. Prev. 2003, 23, 398–403. [Google Scholar] [CrossRef]
- VaglioJr, J.; Conard, M.; Poston, W.S.; O’Keefe, J.; Haddock, C.K.; House, J.; Spertus, J.A. Testing the performance of the ENRICHD Social Support Instrument in cardiac patients. Health Qual. Life Outcomes 2004, 2, 24. [Google Scholar] [CrossRef] [Green Version]
- Attarchi, M.; Rigi, A.A.; Mirzamohammadi, E.; Mohammadi, S. Assessment of the main factors influencing return to work following myocardial infarction: A longitudinal study. Int. J. Collab. Res. Intern. Med. Public Health 2012, 4, 1305–1314. [Google Scholar]
- de Jonge, P.; Zuidersma, M.; Bültmann, U. The presence of a depressive episode predicts lower return to work rate after myocardial infarction. Gen. Hosp. Psychiatry 2014, 36, 363–367. [Google Scholar] [CrossRef] [Green Version]
- Jernberg, T.; Hasvold, P.; Henriksson, M.; Hjelm, H.; Thuresson, M.; Janzon, M. Cardiovascular risk in post-myocardial infarction patients: Nationwide real world data demonstrate the importance of a long-term perspective. Eur. Heart J. 2015, 36, 1163–1170. [Google Scholar] [CrossRef] [Green Version]
- Kytö, V.; Prami, T.; Khanfir, H.; Hasvold, P.; Reissell, E.; Airaksinen, J. Usage of PCI and long-term cardiovascular risk in post-myocardial infarction patients: A nationwide registry cohort study from Finland. BMC Cardiovasc. Disord. 2019, 19, 123. [Google Scholar] [CrossRef] [Green Version]
- Dreyer, R.P.; Wang, Y.; Strait, K.M.; Lorenze, N.P.; D’Onofrio, G.; Bueno, H.; Lichtman, J.H.; Spertus, J.A.; Krumholz, H.M. Gender Differences in the Trajectory of Recovery in Health Status among Young Patients with Acute Myocardial Infarction: Results from the variation in recovery: Role of gender on outcomes of young AMI patients (VIRGO) study. Circulation 2015, 131, 1971–1980. [Google Scholar] [CrossRef] [Green Version]
- Freisinger, E.; Sehner, S.; Malyar, N.M.; Suling, A.; Reinecke, H.; Wegscheider, K. Nationwide Routine-Data Analysis of Sex Differences in Outcome of Acute Myocardial Infarction. Clin. Cardiol. 2018, 41, 1013–1021. [Google Scholar] [CrossRef] [Green Version]
- Khan, E.; Brieger, D.; Amerena, J.; Atherton, J.J.; Chew, D.P.; Farshid, A.; Ilton, M.; Juergens, C.P.; Kangaharan, N.; Rajaratnam, R.; et al. Differences in management and outcomes for men and women with ST-elevation myocardial infarction. Med. J. Aust. 2018, 209, 118–123. [Google Scholar] [CrossRef]
- Lin, W.-C.; Ho, C.-H.; Tung, L.-C.; Ho, C.-C.; Chou, W.; Wang, C.-H. Differences between Women and Men in Phase I Cardiac Rehabilitation after Acute Myocardial Infarction: A nationwide population-based analysis. Medicine 2016, 95, e2494. [Google Scholar] [CrossRef]
- Grande, G.; Romppel, M. Gender Differences in Recovery Goals in Patients after Acute Myocardial Infarction. J. Cardiopulm. Rehabil. Prev. 2011, 31, 164–172. [Google Scholar] [CrossRef]
- Symons, R.; Masci, P.G.; Francone, M.; Claus, P.; Barison, A.; Carbone, I.; Agati, L.; Galea, N.; Janssens, S.; Bogaert, J. Impact of active smoking on myocardial infarction severity in reperfused ST-segment elevation myocardial infarction patients: The smoker’s paradox revisited. Eur. Heart J. 2016, 37, 2756–2764. [Google Scholar] [CrossRef] [Green Version]
- Reinstadler, S.J.; Eitel, C.; Fuernau, G.; De Waha, S.; Desch, S.; Mende, M.; Metzler, B.; Schuler, G.; Thiele, H.; Eitel, I. Association of smoking with myocardial injury and clinical outcome in patients undergoing mechanical reperfusion for ST-elevation myocardial infarction. Eur. Heart J.-Cardiovasc. Imaging 2016, 18, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Rakowski, T.; Siudak, Z.; Dziewierz, A.; Dubiel, J.S.; Dudek, D. Impact of smoking status on outcome in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention. J. Thromb. Thrombolysis 2012, 34, 397–403. [Google Scholar] [CrossRef] [Green Version]
- Biery, D.W.; Berman, A.N.; Singh, A.; Divakaran, S.; DeFilippis, E.M.; Collins, B.L.; Gupta, A.; Fatima, A.; Qamar, A.; Klein, J.; et al. Association of Smoking Cessation and Survival among Young Adults with Myocardial Infarction in the Partners YOUNG-MI Registry. JAMA Netw. Open 2020, 3, e209649. [Google Scholar] [CrossRef]
- Buchanan, D.M.; Arnold, S.V.; Gosch, K.L.; Jones, P.G.; Longmore, L.S.; Spertus, J.A.; Cresci, S. Association of Smoking Status with Angina and Health-Related Quality of Life after Acute Myocardial Infarction. Circ. Cardiovasc. Qual. Outcomes 2015, 8, 493–500. [Google Scholar] [CrossRef] [Green Version]
- Haig, C.; Carrick, D.; Carberry, J.; Mangion, K.; Maznyczka, A.; Wetherall, K.; McEntegart, M.; Petrie, M.C.; Eteiba, H.; Lindsay, M.; et al. Current Smoking and Prognosis after Acute ST-Segment Elevation Myocardial Infarction: New pathophysiological insights. JACC Cardiovasc. Imaging 2018, 12, 993–1003. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Vaez, M.; Dorner, T.E.; Rahman, S.; Helgesson, M.; Ivert, T.; Mittendorfer-Rutz, E. Risk factors for subsequent work disability in patients with acute myocardial infarction. Eur. J. Public Health 2019, 29, 531–540. [Google Scholar] [CrossRef] [PubMed]
- AbuRuz, M.E. Patients with ST segment elevation myocardial infarction: Moderating effect of perceived control on the relationship between depression and in-hospital complications. BMC Cardiovasc. Disord. 2019, 19, 143. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Song, J.; Shao, M.; Gao, X.; Ji, F.; Tian, H.; Xu, Y.; Zhuo, C. Depression predicts the risk of adverse events after percutaneous coronary intervention: A meta-analysis. J. Affect. Disord. 2020, 266, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Feng, H.-P.; Chien, W.-C.; Cheng, W.-T.; Chung, C.-H.; Cheng, S.-M.; Tzeng, W.-C. Risk of anxiety and depressive disorders in patients with myocardial infarction: A nationwide population-based cohort study. Medicine 2016, 95, e4464. [Google Scholar] [CrossRef] [PubMed]
- Şahan, C.; Demiral, Y.; Kilic, B.; Aslan, O. Changes in Employment Status after Myocardial Infarction among Men. Balk. Med. J. 2016, 33, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Waszkowska, M.; Szymczak, W. Return to work after myocardial infarction: A retrospective study. Int. J. Occup. Med. Environ. Health 2009, 22, 373–381. [Google Scholar] [CrossRef]
- Bucholz, E.M.; Strait, K.M.; Dreyer, R.P.; Geda, M.; Spatz, E.S.; Bueno, H.; Lichtman, J.H.; D’Onofrio, G.; Spertus, J.A.; Krumholz, H.M. Effect of Low Perceived Social Support on Health Outcomes in Young Patients with Acute Myocardial Infarction: Results from the Variation in Recovery: Role of Gender on Outcomes of Young AMI Patients (VIRGO) Study. J. Am. Heart Assoc. 2014, 3, e001252. [Google Scholar] [CrossRef] [Green Version]
- Leifheit-Limson, E.C.; Reid, K.J.; Kasl, S.V.; Lin, H.; Buchanan, D.M.; Jones, P.G.; Peterson, P.N.; Parashar, S.; Spertus, J.A.; Lichtman, J.H. Changes in social support within the early recovery period and outcomes after acute myocardial infarction. J. Psychosom. Res. 2012, 73, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Baechli, C.; Koch, D.; Bernet, S.; Gut, L.; Wagner, U.; Mueller, B.; Schuetz, P.; Kutz, A. Association of comorbidities with clinical outcomes in patients after acute myocardial infarction. IJC Heart Vasc. 2020, 29, 100558. [Google Scholar] [CrossRef]
- Chen, H.Y.; Saczynski, J.S.; McManus, D.D.; Lessard, D.; Yarzebski, J.; Lapane, K.L.; Gore, J.M.; Goldberg, R.J. The impact of cardiac and noncardiac comorbidities on the short-term outcomes of patients hospitalized with acute myocardial infarction: A population-based perspective. Clin. Epidemiol. 2013, 5, 439–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McManus, D.D.; Nguyen, H.L.; Saczynski, J.S.; Tisminetzky, M.; Bourell, P.; Goldberg, R.J. Multiple cardiovascular comorbidities and acute myocardial infarction: Temporal trends (1990–2007) and impact on death rates at 30 days and 1 year. Clin. Epidemiol. 2012, 4, 115–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bataille, V.; Ferrières, J.; Danchin, N.; Puymirat, E.; Zeller, M.; Simon, T.; Carrie, D. Increased mortality risk in diabetic patients discharged from hospital with insulin therapy after an acute myocardial infarction: Data from the FAST-MI 2005 registry. Eur. Heart J. Acute Cardiovasc. Care 2017, 8, 218–230. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhao, T.; Wei, X.; Lu, H.; Lin, X. The prevalence of 30-day readmission after acute myocardial infarction: A systematic review and meta-analysis. Clin. Cardiol. 2019, 42, 889–898. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| BASELINE | FOLLOW-UP | ||||
|---|---|---|---|---|---|
| Variables | n | % | Variables | n | % |
| Demographic factors | Demographic factors | ||||
| Age | Self-rated financial status | ||||
| ≤59 | 45 | 33.00 | Excellent | 2 | 1.50 |
| 60–69 | 41 | 30.10 | Good | 13 | 9.60 |
| 70–79 | 40 | 29.40 | Only fair | 92 | 67.60 |
| 80≤ | 10 | 7.50 | Poor | 29 | 21.30 |
| Gender | Behavioral factors | ||||
| Male | 100 | 73.50 | Physical activity status | ||
| Female | 36 | 26.50 | Moderate physical activity, at least 30 min most or all days of the week | 49 | 36.00 |
| Marriage status | |||||
| Married | 119 | 87.50 | |||
| Never married/Separated/Divorced/Widowed | 17 | 12.50 | Moderate physical activity, less than 30 min less than 5 days per week | 27 | 19.90 |
| Educational level | Not physically active | 60 | 44.10 | ||
| Primary school | 35 | 25.70 | Smoking status | ||
| Middle school | 22 | 16.30 | Smoker | 81 | 59.60 |
| High school | 49 | 36.00 | Non-smoker | 26 | 19.10 |
| Undergraduate study or more | 30 | 22.00 | Quit smoking | 29 | 21.30 |
| Drinks alcohol | |||||
| Employment status | Yes | 40 | 29.40 | ||
| Regular employee | 30 | 22.10 | No | 96 | 70.60 |
| Casual employee | 3 | 2.20 | Clinical factors | ||
| Self-employed | 23 | 16.90 | Readmission to hospital | ||
| Unpaid family worker | 24 | 17.60 | Yes | 18 | 13.20 |
| Retired/unemployed | 56 | 41.20 | No | 118 | 86.80 |
| Self-rated financial status | Frequency of visiting a doctor within three months | ||||
| Excellent | 3 | 2.20 | |||
| Good | 15 | 11.00 | Less or equal to 3 times | 117 | 86.00 |
| Only fair | 82 | 60.30 | |||
| Poor | 36 | 26.50 | More than 3 times | 16 | 12.00 |
| Clinical factors | Unknown | 3 | 2.00 | ||
| Type of MI | Frequency of chest pain | ||||
| NSTEMI | 79 | 58.10 | No pain most days | 117 | 86.00 |
| STEMI | 57 | 41.90 | Mild pain most days | 17 | 12.50 |
| Time from MI to intervention | Moderate pain most days | 2 | 1.50 | ||
| Less than 2 h | 50 | 36.80 | Psychosocial factors | ||
| More than 2 h | 47 | 34.60 | Depression scores | ||
| Unknown | 39 | 28.60 | Not depressed | 104 | 76.50 |
| LVEF at admission | Mild/Moderate depression | 26 | 19.10 | ||
| ≥55% | 53 | 39.00 | Severe/extremely severe depression | 6 | 4.40 |
| 40–54% | 66 | 48.50 | Anxiety scores | ||
| 35–39% | 8 | 5.90 | No anxiety | 116 | 85.30 |
| <35% | 9 | 6.60 | Mild/moderate anxiety | 15 | 11.00 |
| Type of intervention | Severe/extremely severe anxiety | 5 | 3.70 | ||
| Medical antithrombotic therapy | 20 | 14.70 | Stress scores | ||
| Not stressed | 122 | 89.70 | |||
| Angioplasty | 112 | 82.30 | Mild/moderate stress | 14 | 10.30 |
| CABG | 4 | 3.00 | Severe/extremely severe stress | 0 | 0 |
| Number of comorbidities | |||||
| Zero | 44 | 32.40 | |||
| One | 47 | 34.60 | |||
| Two | 41 | 30.10 | |||
| Three | 4 | 2.90 | |||
| Previous MI | |||||
| Yes | 106 | 77.90 | |||
| No | 30 | 22.10 | |||
| Hypertension | |||||
| Yes | 66 | 48.50 | |||
| No | 70 | 51.50 | |||
| Diabetes | |||||
| Yes | 41 | 30.10 | |||
| No | 95 | 69.90 | |||
| CATEGORICAL FACTORS | |||||
|---|---|---|---|---|---|
| Variables | 3 Months Post Discharge (n = 136) | Chi-Square & p-Value | |||
| RTW (n = 49) | NRTW (n = 87) | ||||
| Demographic factors | |||||
| Gender | Fisher’s exact p < 0.001 | ||||
| Female | 3 | 33 | |||
| Male | 46 | 54 | |||
| Marriage status | Fisher’s exact p = 0.110 | ||||
| Married | 46 | 73 | |||
| Never married/Separated/Divorced/ Widowed | 3 | 14 | |||
| Educational level | χ2 = 22.199 p < 0.001 | ||||
| Primary school | 2 | 33 | |||
| Middle school | 7 | 15 | |||
| High school | 23 | 26 | |||
| Undergraduate study or more | 17 | 13 | |||
| Self-rated financial status at 3 months | Fisher’s exact p = 0.001 | ||||
| Excellent/Good | 13 | 5 | |||
| Only fair/Poor | 36 | 82 | |||
| Behavioral factors | |||||
| Physical activity status at 3 months | χ2 = 5.668 p = 0.059 | ||||
| Moderate physical activity, at least 30 min | 22 | 27 | |||
| most or all days of the week | |||||
| Moderate physical activity, less than 30 min | 12 | 15 | |||
| less than 5 days per week | |||||
| Not physically active | 15 | 45 | |||
| Smoking status at 3 months | χ2 = 13.494 p = 0.001 | ||||
| Never smoked | 61 | 20 | |||
| Quit smoking | 15 | 11 | |||
| Smoker | 11 | 18 | |||
| Drinking alcohol at 3 months | χ2 = 14.127 p < 0.001 | ||||
| Yes | 24 | 16 | |||
| No | 25 | 71 | |||
| Clinical factors | |||||
| Diabetes | Fisher’s exact p = 0.011 | ||||
| Yes | 41 | 54 | |||
| No | 8 | 33 | |||
| Hypertension | Fisher’s exact p = 0.373 | ||||
| Yes | 25 | 42 | |||
| No | 21 | 45 | |||
| Number of comorbidities | χ2 = 7.543 p = 0.023 | ||||
| None | 23 | 21 | |||
| One | 14 | 33 | |||
| Two and more | 12 | 33 | |||
| Previous MI | Fisher’s exact p = 0.052 | ||||
| Yes | 43 | 63 | |||
| No | 6 | 24 | |||
| Type of MI | Fisher’s exact p = 0.593 | ||||
| NSTEMI | 30 | 49 | |||
| STEMI | 19 | 38 | |||
| Time from MI to intervention | Fisher’s exact p = 0.437 | ||||
| Less than 2 h | 24 | 26 | |||
| More than 2 h | 20 | 27 | |||
| Unknown | 5 | 34 | |||
| Type of intervention | χ2 = 0.885 p = 0.642 | ||||
| Medical antithrombotic therapy | 41 | 70 | |||
| Angioplasty | 2 | 2 | |||
| CABG | 6 | 15 | |||
| Readmission to Hospital | Fisher’s exact p = 0.018 | ||||
| Yes | 2 | 16 | |||
| No | 47 | 71 | |||
| Frequencies of visiting a doctor within 3 months | Fisher’s exact p = 1.000 | ||||
| Less or equal to 3 times | 43 | 74 | |||
| More than 3 times | 6 | 10 | |||
| Frequency of chest pain within 3 months | Fisher’s exact p = 0.536 | ||||
| No/Mild pain most days | 49 | 85 | |||
| Moderate/Severe pain most days | 0 | 2 | |||
| CONTINUOUS FACTORS | |||||
| Have you returned to your normal work? | Mean | Standard deviation | t | pvalue | |
| Demographic factors | |||||
| Age | No | 68.33 | 11.452 | 5.985 | p < 0.001 |
| Yes | 57.27 | 8.015 | |||
| Clinical factors | |||||
| LVEF | No | 49.8490 | 11.29764 | −1.469 | p = 0.144 |
| Yes | 52.6502 | 9.45999 | |||
| Psychosocial factors | |||||
| Social support at 3 months | No | 27.11 | 5.850 | −2.746 | p = 0.007 |
| Yes | 29.49 | 4.169 | |||
| Anxiety | No | 2.10 | 2.215 | 2.042 | p = 0.043 |
| Yes | 1.31 | 2.133 | |||
| Stress | No | 3.26 | 3.208 | −0.331 | p = 0.741 |
| Yes | 3.45 | 2.973 | |||
| Depression | No | 3.93 | 4.120 | 4.485 | p < 0.001 |
| Yes | 1.14 | 1.848 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, W.; Gholizadeh, L.; Perry, L.; Kang, K. Predicting Return to Work Following Myocardial Infarction: A Prospective Longitudinal Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 8032. https://doi.org/10.3390/ijerph19138032
Sun W, Gholizadeh L, Perry L, Kang K. Predicting Return to Work Following Myocardial Infarction: A Prospective Longitudinal Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(13):8032. https://doi.org/10.3390/ijerph19138032
Chicago/Turabian StyleSun, Weizhe, Leila Gholizadeh, Lin Perry, and Kyoungrim Kang. 2022. "Predicting Return to Work Following Myocardial Infarction: A Prospective Longitudinal Cohort Study" International Journal of Environmental Research and Public Health 19, no. 13: 8032. https://doi.org/10.3390/ijerph19138032