
Persistent Symptoms among Frontline Health Workers Post-Acute COVID-19 Infection

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
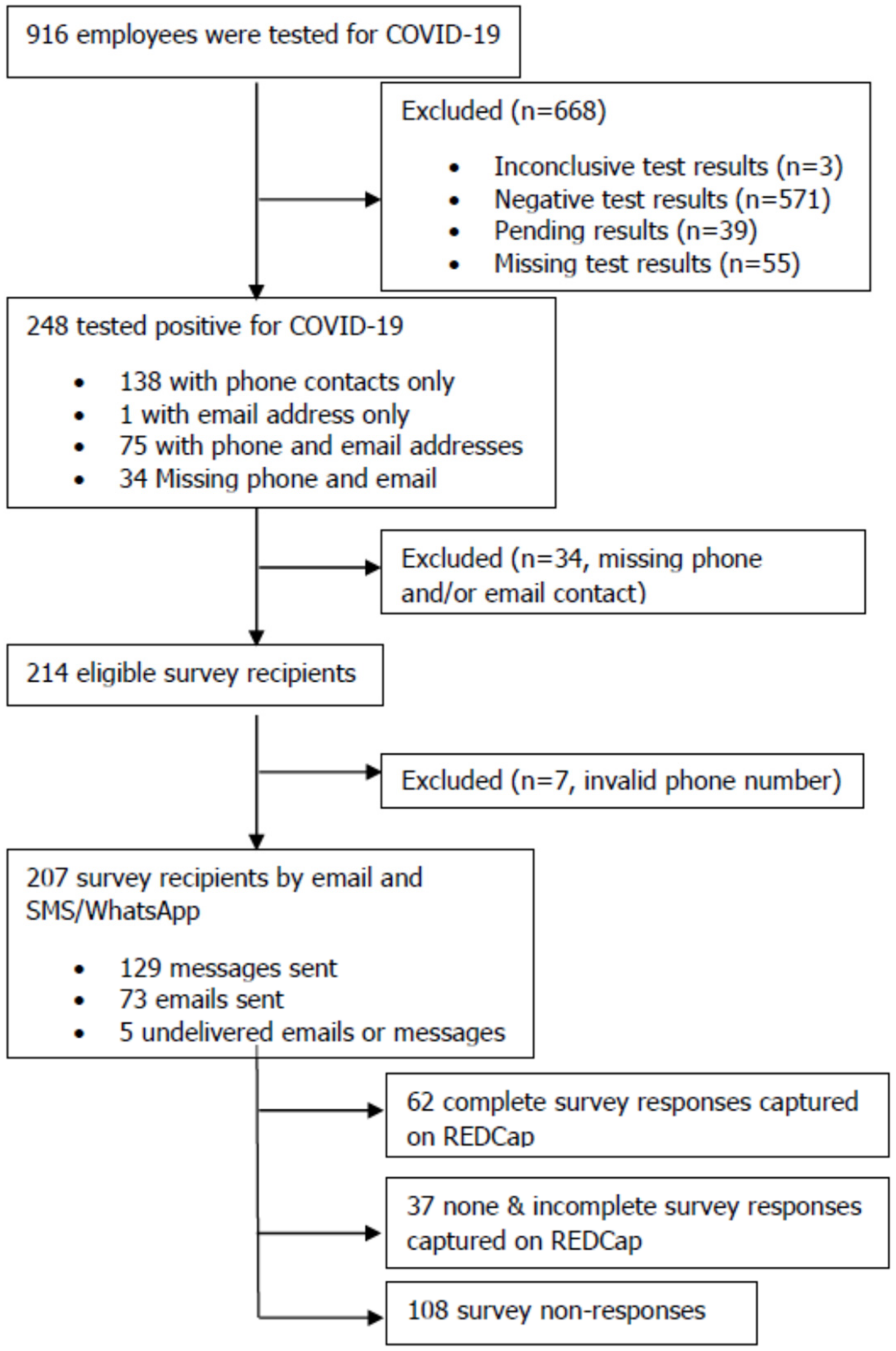
2.1. Design and Participants
2.2. Research Setting
2.3. Survey Instrument
2.4. Data Collection
2.5. Statistical Analysis
3. Results
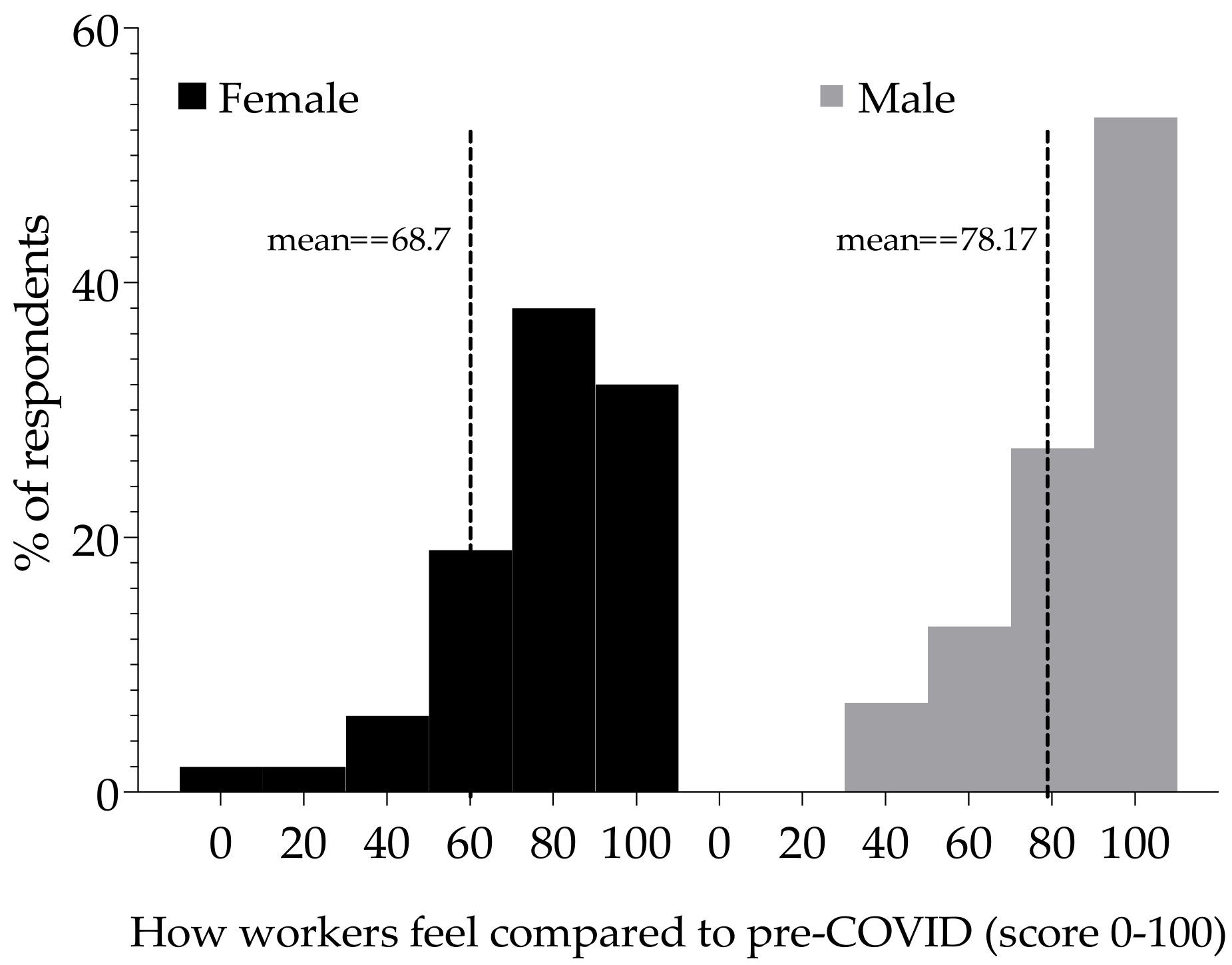
3.1. Demographics
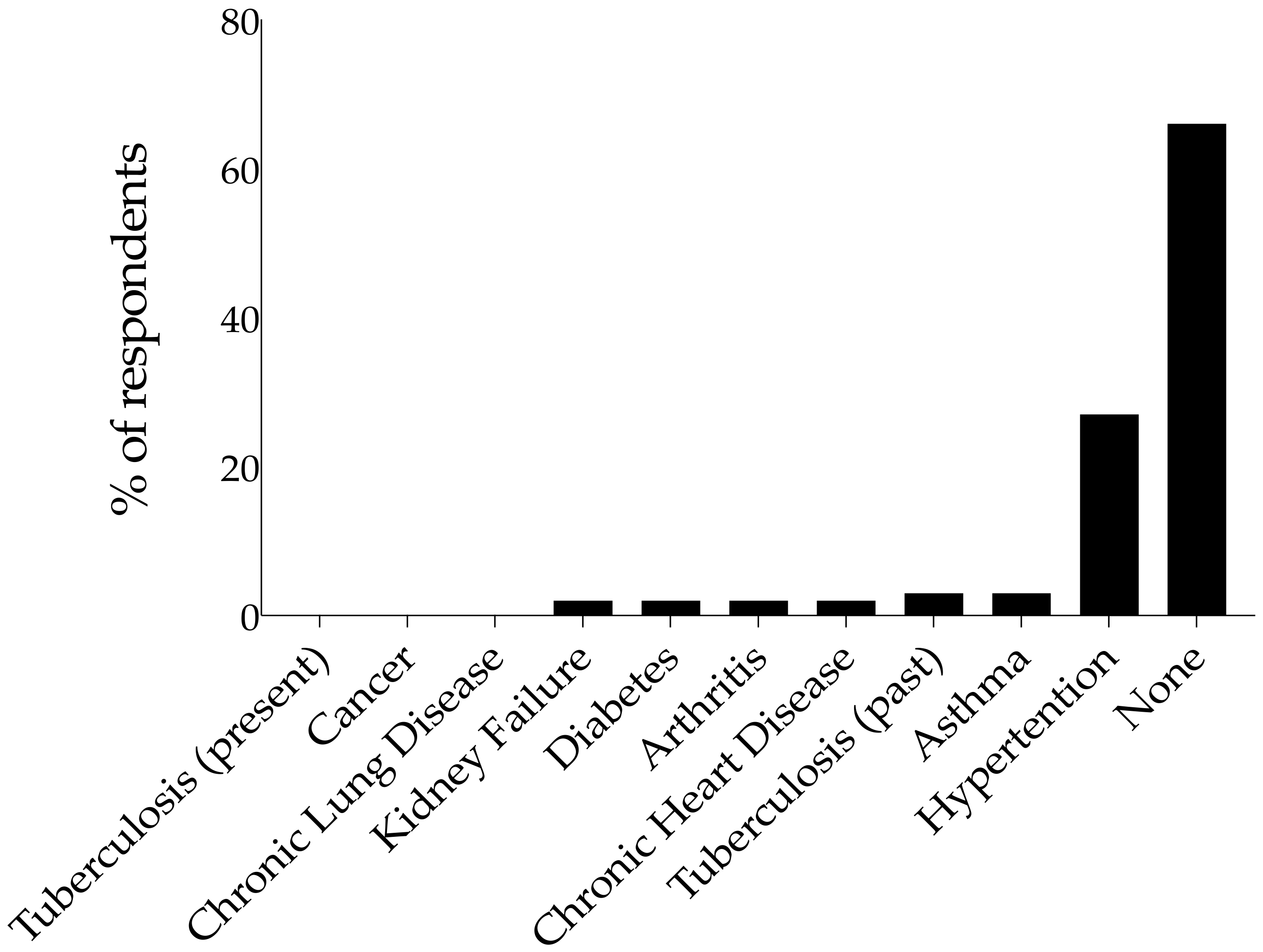
3.2. Co-Morbidities
3.3. Clinical Manifestations and Management of Acute COVID-19 Infection
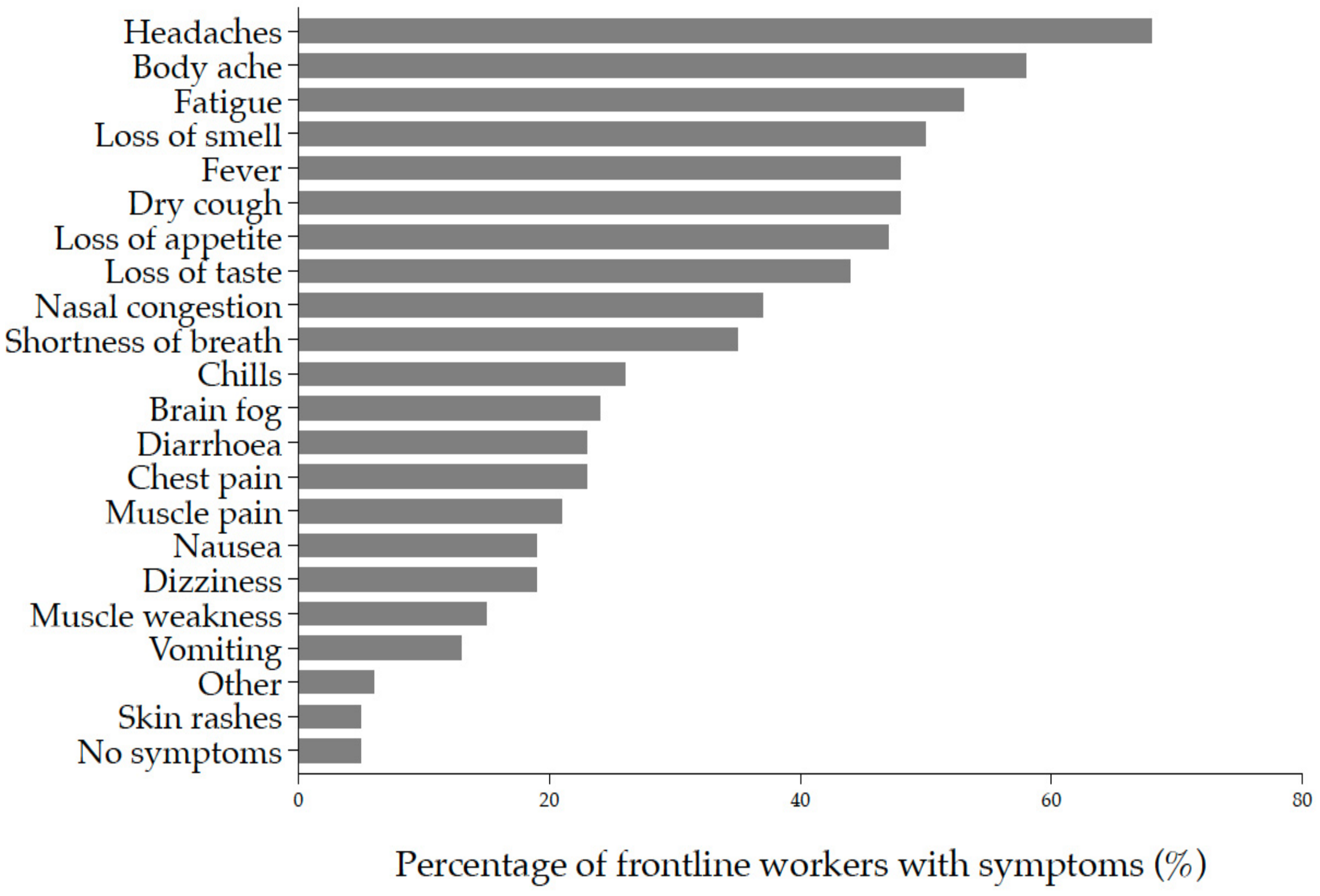
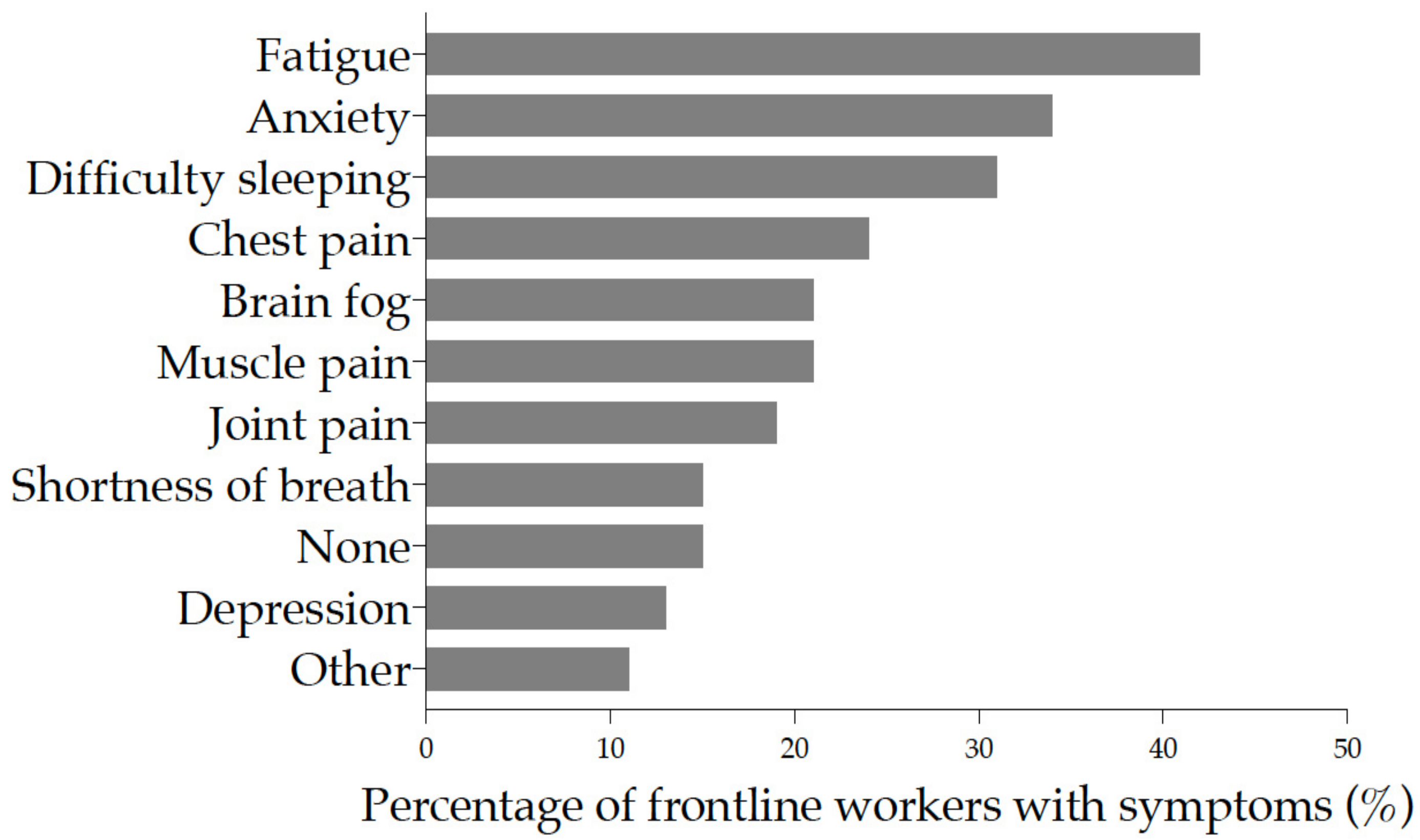
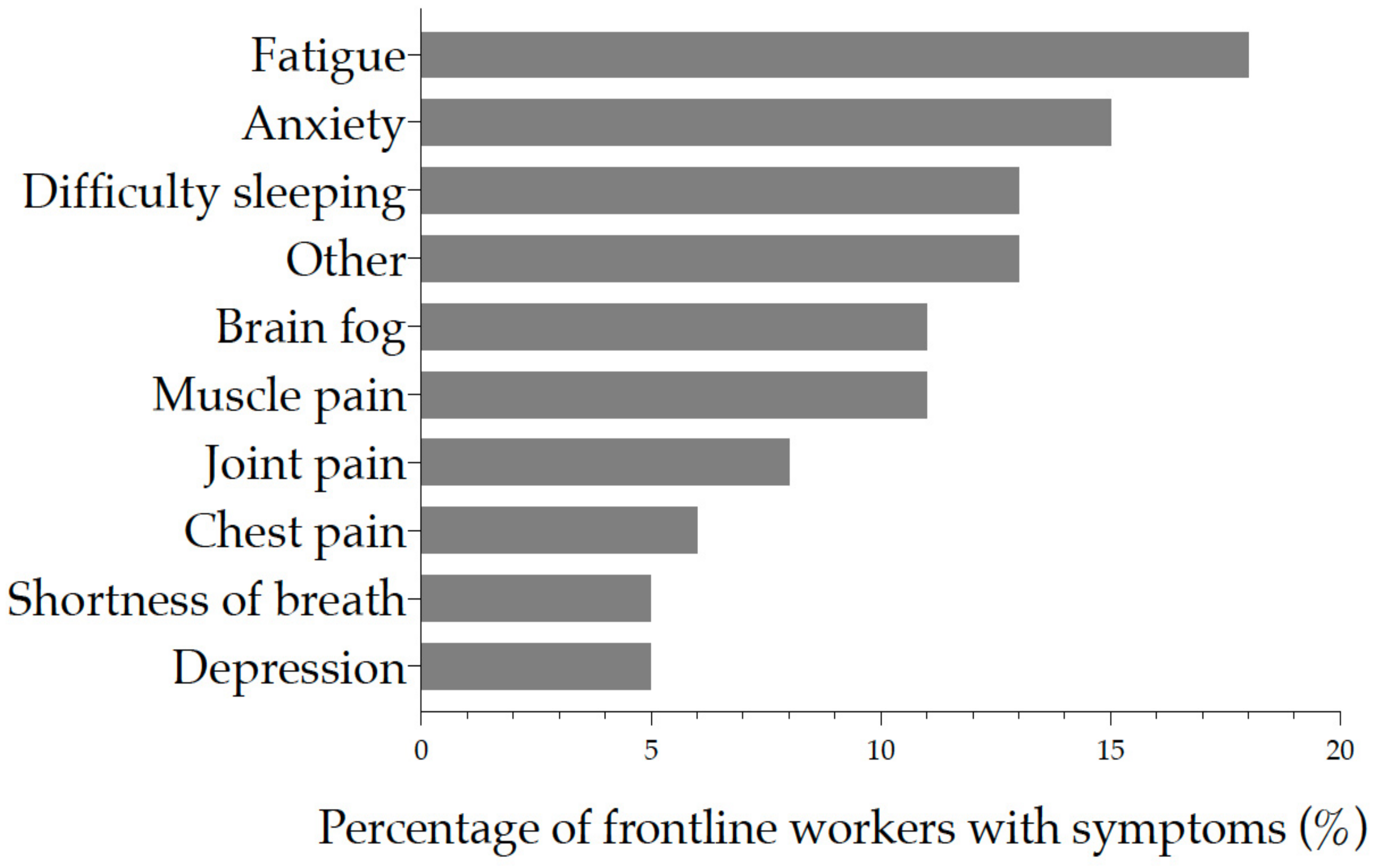
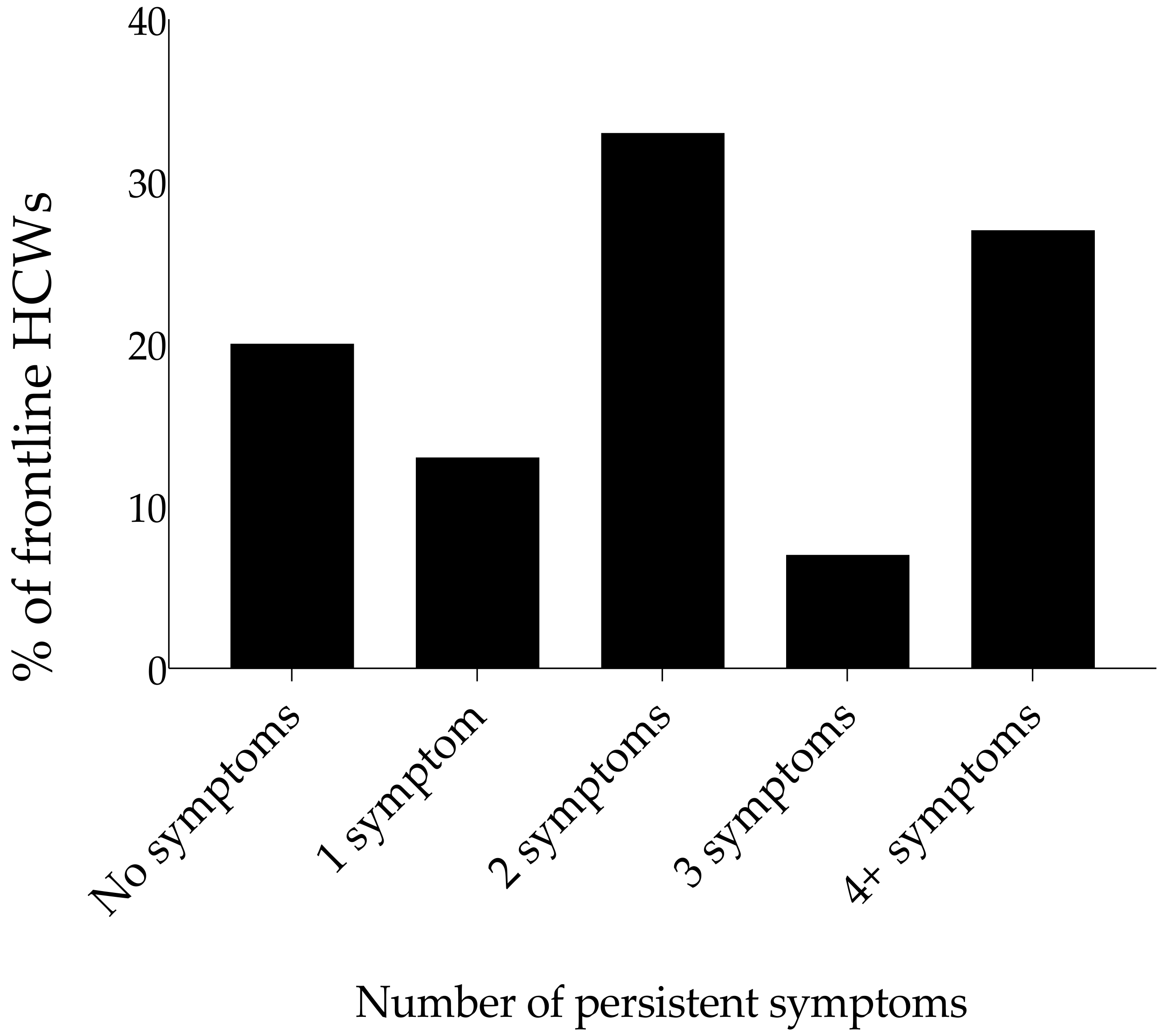
3.4. Clinical Symptoms Post-Acute COVID-19
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Ladds, E.; Rushforth, A.; Wieringa, S.; Taylor, S.; Rayner, C.; Husain, L.; Greenhalgh, T. Persistent symptoms after COVID-19: Qualitative study of 114 “long Covid” patients and draft quality principles for services. BMC Health Serv. Res. 2020, 20, 1144. [Google Scholar] [CrossRef] [PubMed]
- Carfì, A.; Bernabei, R.; Landi, F.; Gemelli against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. Available online: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)32656-8/fulltext (accessed on 30 March 2022). [CrossRef]
- News24. Available online: https://www.news24.com/news24/SouthAfrica/News/coronavirus-511-health-workers-positive-26-hospitalised-and-2-have-died-zweli-mkhize-20200506 (accessed on 30 March 2022).
- Han, Q.; Lin, Q.; Jin, S.; You, L. Coronavirus 2019-nCoV: A brief perspective from the front line. J. Infect. 2020, 80, 373–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Fact Sheets on Physical Activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 20 October 2021).
- Centres for Disease Control and Prevention. Interim Guidelines for Collecting, Handling, and Testing Clinical Specimens from Persons for Coronavirus Disease 2019 (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-nCoV/lab/guidelines-clinical-specimens.html (accessed on 30 March 2022).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 30 March 2022).
- Nilsson 2016. Coloured by Race: A Study about Making Coloured Identities in South Africa. Available online: https://www.diva-portal.org/smash/get/diva2:939226/FULLTEXT01.pdf (accessed on 30 March 2022).
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef] [PubMed]
- Ayoubkhani, D.; Khunti, K.; Nafilyan, V.; Maddox, T.; Humberstone, B.; Diamond, I.; Banerjee, A. Post-COVID syndrome in individuals admitted to hospital with COVID-19: Retrospective cohort study. BMJ 2021, 372, n693. [Google Scholar] [CrossRef]
- Clift, A.K.; Coupland, C.; Keogh, R.H.; Diaz-Ordaz, K.; Williamson, E.; Harrison, E.M.; Hayward, A.; Hemingway, H.; Horby, P.; Mehta, N.; et al. Living risk prediction algorithm (QCOVID) for risk of hospital admission and mortality from coronavirus 19 in adults: National derivation and validation cohort study. BMJ 2020, 371, m3731. [Google Scholar] [CrossRef]
- Sani, G.; Janiri, D.; Di Nicola, M.; Janiri, L.; Ferretti, S.; Chieffo, D. Mental health during and after the COVID-19 emergency in Italy. Psychiatry Clin. Neurosci. 2020, 74, 372. [Google Scholar] [CrossRef] [Green Version]
- Garrigues, E.; Janvier, P.; Kherabi, Y.; Le Bot, A.; Hamon, A.; Gouze, H.; Doucet, L.; Berkani, S.; Oliosi, E.; Mallart, E.; et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J. Infect. 2020, 81, e4–e6. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, V.; Battaglia, G.; Giustino, V.; Gagliardo, A.; D’Aleo, M.; Giannini, O.; Palma, A.; Brighina, F. Significant reduction of physical activity in patients with neuromuscular disease during COVID-19 pandemic: The long-term consequences of quarantine. J. Neurol. 2021, 268, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Augustin, M.; Schommers, P.; Stecher, M.; Dewald, F.; Gieselmann, L.; Gruell, H.; Horn, C.; Vanshylla, K.; DiCristanziano, V.; Osebold, L.; et al. Post-COVID Syndrome in Non-Hospitalised Patients with COVID-19: A Longitudinal Prospective Cohort Study. Lancet Reg. Health Eur. 2021, 6, 100122. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Shalash, A.; Roushdy, T.; Essam, M.; Fathy, M.; Dawood, N.L.; Abushady, E.M.; Elrassas, H.; Helmi, A.; Hamid, E. Mental Health, Physical Activity, and Quality of Life in Parkinson’s Disease During COVID-19 Pandemic. Mov. Disord. Off. J. Mov. Disord. Soc. 2020, 35, 1097–1099. [Google Scholar] [CrossRef] [PubMed]
- Mendelsohn, A.S.; De Sá, A.; Morden, E.; Botha, B.; Boulle, A.; Paleker, M.; Davies, M.A. COVID-19 wave 4 in Western Cape Province, South Africa: Fewer hospitalisations, but new challenges for a depleted workforce. S. Afr. Med. J. 2022, 1, 13496. [Google Scholar] [CrossRef]
- Mendelsohn, A.S.; Nath, N.; De Sá, A.; Von Pressentin, K.B. Two months follow-up of patients with non-critical COVID-19 in Cape Town, South Africa. S. Afr. Fam. Pract. 2022, 10, e1–e6. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | % | |
|---|---|---|
| Age (median {IQR}) | 33.5 (30–44) | |
| Sex | ||
| Female | 47 | 75.8 |
| Male | 15 | 24.2 |
| Missing | 0 | 0.0 |
| Age Groups | ||
| 23–33 | 31 | 50.0 |
| 34–44 | 17 | 27.4 |
| 45–55 | 9 | 14.5 |
| ≥56 | 5 | 8.1 |
| Missing | 0 | 0.0 |
| Ethnicity | ||
| African | 54 | 87.1 |
| Caucasian | 2 | 3.2 |
| Coloured * | 6 | 9.7 |
| Missing | 0 | 0.0 |
| Smoking Status | ||
| Current smoker | 4 | 6.4 |
| Never smoker | 53 | 85.5 |
| Past smoker | 8 | 8.1 |
| Missing | 0 | 0.0 |
| Alcohol Intake | ||
| Daily | 2 | 3.2 |
| Occasional | 24 | 38.7 |
| Not at all | 36 | 58.1 |
| Missing | 0 | 0.0 |
| Recreational Drug Use | ||
| Daily | 1 | 1.6 |
| Occasional | 1 | 1.6 |
| Not at all | 60 | 96.8 |
| Missing | 0 | 0.0 |
| Demographics | N | Long COVID-19 | p-Value | |
|---|---|---|---|---|
| No n (%), 47 (75.8) | Yes n (%), 15 (24.2) | |||
| Median Age (IQR) | 33.5 (30–44) | 32 (29–43) | 40 (34–54) | |
| Age Groups | 0.02 | |||
| 23–33 | 31 (50.0) | 28 (59.6) | 3 (20.0) | |
| 34–44 | 17 (27.4) | 11 (23.4) | 6 (40.0) | |
| 45–55 | 9 (14.5) | 6 (12.8) | 3 (20.0) | |
| ≥56 | 5 (8.1) | 2 (4.2) | 3 (20.0) | |
| Sex | 0.48 | |||
| Female | 47 (75.8) | 35 (74.5) | 12 (80.0) | |
| Male | 15 (24.2) | 12 (25.5) | 3 (20.0) | |
| Ethnicity | 0.47 | |||
| African | 54 (87.1) | 42 (892.4) | 12 (80.0) | |
| Caucasian | 2 (3.2) | 1 (2.1) | 1 (6.7) | |
| Coloured | 6 (9.7) | 4 (8.5) | 2 (13.3) | |
| Smoking Status | 0.09 | |||
| Current smoker | 4 (6.4) | 4 (8.5) | 0 (0.0) | |
| Never smoker | 53 (85.5) | 41 (87.2) | 12 (80.0) | |
| Past smoker | 5 (8.1) | 2 (4.3) | 3 (20.0) | |
| Alcohol Intake | 0.07 | |||
| Daily | 2 (3.2) | 0 (0.0) | 2 (13.3) | |
| Occasional | 24 (38.7) | 20 (42.6) | 4 (26.7) | |
| Not at all | 36 (58.1) | 27 (57.4) | 9 (60.0) | |
| Recreational Drug Use | 0.06 | |||
| Daily | 1 (1.6) | 0 (0.0) | 1 (6.7) | |
| Occasional | 1 (1.6) | 0 (0.0) | 1 (6.6) | |
| Not at all | 60 (96.8) | 47 (100.0) | 13 (86.7) | |
| Total | 62 | 47 | 15 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wose Kinge, C.; Hanekom, S.; Lupton-Smith, A.; Akpan, F.; Mothibi, E.; Maotoe, T.; Lebatie, F.; Majuba, P.; Sanne, I.; Chasela, C. Persistent Symptoms among Frontline Health Workers Post-Acute COVID-19 Infection. Int. J. Environ. Res. Public Health 2022, 19, 5933. https://doi.org/10.3390/ijerph19105933
Wose Kinge C, Hanekom S, Lupton-Smith A, Akpan F, Mothibi E, Maotoe T, Lebatie F, Majuba P, Sanne I, Chasela C. Persistent Symptoms among Frontline Health Workers Post-Acute COVID-19 Infection. International Journal of Environmental Research and Public Health. 2022; 19(10):5933. https://doi.org/10.3390/ijerph19105933
Chicago/Turabian StyleWose Kinge, Constance, Susan Hanekom, Alison Lupton-Smith, Francis Akpan, Eula Mothibi, Thapelo Maotoe, Floyd Lebatie, Pappie Majuba, Ian Sanne, and Charles Chasela. 2022. "Persistent Symptoms among Frontline Health Workers Post-Acute COVID-19 Infection" International Journal of Environmental Research and Public Health 19, no. 10: 5933. https://doi.org/10.3390/ijerph19105933