
Assessing Nursing Students’ Self-Perceptions about Safe Medication Management: Design and Validation of a Tool, the NURSPeM

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Background
3. Research Question
4. Study Design
5. Method
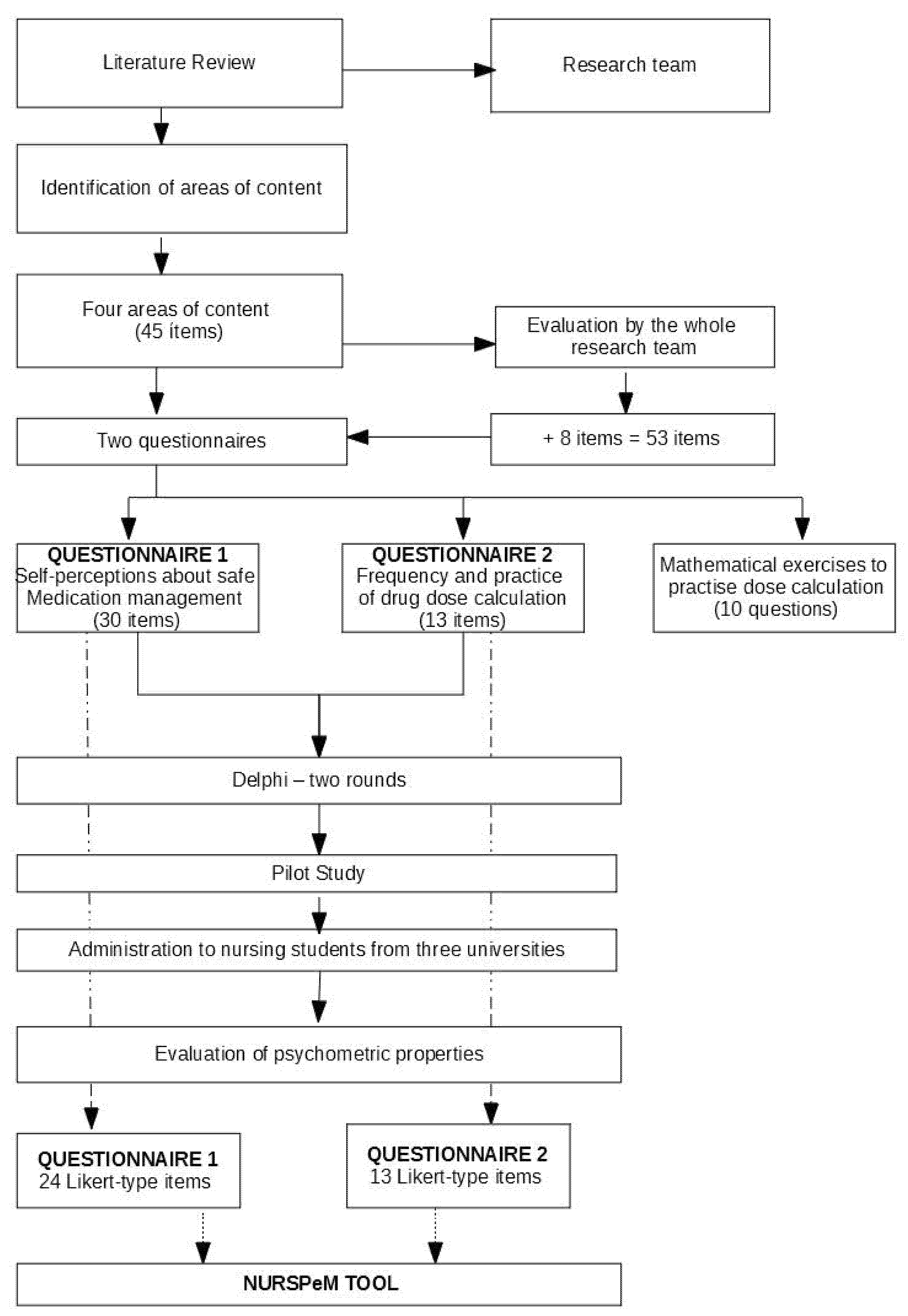
5.1. Phase 1: Defining the Construct ‘Self-Perceptions about Safe Medication Management’ and Its Dimensions
5.2. Phase 2: Development of the Tool: Items and Dimensions
5.3. Phase 3: Content Validity
5.4. Phase 4: Psychometric Evaluation of the Tool
6. Analysis
7. Ethics
8. Results
8.1. Construct Validity
8.2. Reliability Analysis
9. Discussion
Development and Content of the Tool
10. Future Research
11. Limitations
12. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Makary, M.A.; Daniel, M. Medical Error—The Third Leading Cause of Death in the US. BMJ 2016, 353, i2139. [Google Scholar] [CrossRef]
- Ministerio de Sanidad, Servicios Sociales e Igualdad [Spanish Ministry of Health, Social Services and Equality]. Estrategia de Seguridad del Paciente del Sistema Nacional de Salud [Patient Safety Strategy for the National Health Service] (Madrid, 2016). Available online: https://seguridaddelpaciente.es/resources/documentos/2015/Estrategia%20Seguridad%20del%20Paciente%202015-2020.pdf (accessed on 13 June 2021).
- World Health Organization. Global Patient Safety Challenge: Medication without harm. Global Patient Safety Challenge on Medication Safety. Geneva. 2017. Medication without Harm. Available online: https://www.who.int/initiatives/medication-without-harm (accessed on 13 June 2021).
- Jiménez Muñoz, A.B.; Martínez Mondéjar, B.; Muiño Miguez, A.; Romero Ayuso, D.; Saiz Ladera, G.M.; Criado Álvarez, J.J. 2019. Errores de Prescripción, Trascripción Y Administración Según Grupo Farmacológico En El Ámbito Hospitalario. Rev. Española De Salud Pública 2019, 93. Available online: https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1135-57272019000100073 (accessed on 13 June 2021).
- Sutherland, A.; Canobbio, M.; Clarke, J.; Randall, M.; Skelland, T.; Weston, E. Incidence and prevalence of intravenous medication errors in the UK: A systematic review. Eur. J. Hosp. Pharm. 2018, 27, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Wolf, Z.R.; Hughes, R.G. Best Practices to Decrease Infusion-Associated Medication Errors. J. Infus. Nurs. 2019, 42, 183–192. [Google Scholar] [CrossRef]
- Vaismoradi, M.; Griffiths, P.; Turunen, H.; Jordan, S. Transformational leadership in nursing and medication safety education: A discussion paper. J. Nurs. Manag. 2016, 24, 970–980. [Google Scholar] [CrossRef] [Green Version]
- Rohde, E.; Domm, E. Nurses’ clinical reasoning practices that support safe medication administration: An integrative review of the literature. J. Clin. Nurs. 2017, 27, e402–e411. [Google Scholar] [CrossRef]
- Cruz Almaguer, A.Y.; Medina González, I.; Ávila Sánchez, M. Relaciones Entre La Gestión Del Riesgo y El Proceso de Atención de Enfermería Para Su Integración Práctica. Rev. Cuba. De Enfermería 2020, 36. Available online: http://www.revenfermeria.sld.cu/index.php/enf/article/view/3208/597 (accessed on 17 March 2022).
- Armstrong, G.E.; Dietrich, M.; Norman, L.; Barnsteiner, J.; Mion, L. Nurses’ Perceived Skills and Attitudes About Updated Safety Concepts. J. Nurs. Care Qual. 2017, 32, 226–233. [Google Scholar] [CrossRef]
- Manzo, B.F.; Brasil, C.L.G.B.; Reis, F.F.T.; Corrêa, A.D.R.; Simão, D.A.D.S.; Costa, A.C.L. Segurança na administração de medicamentos: Investigação sobre a prática de enfermagem e circunstâncias de erros. Enfermería Glob. 2019, 18, 19–56. [Google Scholar] [CrossRef]
- Berdot, S.; Roudot, M.; Schramm, C.; Katsahian, S.; Durieux, P.; Sabatier, B. Interventions to reduce nurses’ medication administration errors in inpatient settings: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2015, 53, 342–350. [Google Scholar] [CrossRef]
- Hayes, C.; Power, T.; Davidson, P.M.; Daly, J.; Jackson, D. Nurse Interrupted: Development of a Realistic Medication Administration Simulation for Undergraduate Nurses. Nurse Educ. Today 2015, 35, 981–986. [Google Scholar] [CrossRef]
- Parry, A.M.; Barriball, K.L.; While, A.E. Factors contributing to Registered Nurse medication administration error: A narrative review. Int. J. Nurs. Stud. 2015, 52, 403–420. [Google Scholar] [CrossRef]
- Wright, K. Do calculation errors by nurses cause medication errors in clinical practice? A literature review. Nurse Educ. Today 2010, 30, 85–97. [Google Scholar] [CrossRef]
- Härkänen, M.; Voutilainen, A.; Turunen, E.; Vehviläinen-Julkunen, K. Systematic Review and Meta-Analysis of Educational Interventions Designed to Improve Medication Administration Skills and Safety of Registered Nurses. Nurse Educ. Today 2016, 41, 36–43. [Google Scholar] [CrossRef]
- Sulosaari, V.; Suhonen, R.; Leino-Kilpi, H. An integrative review of the literature on registered nurses’ medication competence. J. Clin. Nurs. 2011, 20, 464–478. [Google Scholar] [CrossRef]
- Kelly, S.H.; Koharchik, L.; Henry, R.; Cippel, M.; Hardner, S.; Kolesar, A.; Clark, B. An Advanced Medication Administration Experience to Promote Students’ Knowledge Acquisition in the Skill of Administering Medications. Teach. Learn. Nurs. 2018, 13, 104–107. [Google Scholar] [CrossRef]
- Latimer, S.; Hewitt, J.; Stanbrough, R.; McAndrew, R. Reducing medication errors: Teaching strategies that increase nursing students’ awareness of medication errors and their prevention. Nurse Educ. Today 2017, 52, 7–9. [Google Scholar] [CrossRef]
- Sulosaari, V.; Huupponen, R.; Hupli, M.; Puukka, P.; Torniainen, K.; Leino-Kilpi, H. Factors associated with nursing students’ medication competence at the beginning and end of their education. BMC Med. Educ. 2015, 15, 223. [Google Scholar] [CrossRef]
- Armstrong, G.E.; Dietrich, M.; Norman, L.; Barnsteiner, J.; Mion, L. Development and Psychometric Analysis of a Nurses’ Attitudes and Skills Safety Scale. J. Nurs. Care Qual. 2017, 32, E3–E10. [Google Scholar] [CrossRef] [Green Version]
- Henneman, E.A.; Gawlinski, A.; Blank, F.S.; Henneman, P.L.; McKenzie, J.B.; Jordan, D. Strategies Used by Critical Care Nurses to Identify, Interrupt, and Correct Medical Errors. Am. J. Crit. Care 2010, 19, 500–509. [Google Scholar] [CrossRef]
- Manias, E.; Aitken, R.; Dunning, T. Decision-making models used by ‘graduate nurses’ managing patients’ medications. J. Adv. Nurs. 2004, 47, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Dickson, G.L.; Flynn, L. Nurses’ Clinical Reasoning. Qual. Health Res. 2011, 22, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Folkmann, L.; Rankin, J. Nurses’ medication work: What do nurses know? J. Clin. Nurs. 2010, 19, 3218–3226. [Google Scholar] [CrossRef]
- Eisenhauer, L.A.; Hurley, A.C.; Dolan, N. Nurses’ Reported Thinking During Medication Administration. J. Nurs. Sch. 2007, 39, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Martyn, J.-A.; Paliadelis, P.; Perry, C. The safe administration of medication: Nursing behaviours beyond the five-rights. Nurse Educ. Pract. 2019, 37, 109–114. [Google Scholar] [CrossRef]
- Asensi-Vicente, J.; Jiménez-Ruiz, I.; Vizcaya-Moreno, M.F. Medication Errors Involving Nursing Students: A Systematic Review. Nurse Educ. 2018, 43, E1–E5. [Google Scholar] [CrossRef] [PubMed]
- García-Gámez, M.; Morales-Asencio, J.M.; García-Mayor, S.; Kaknani-Uttumchandani, S.; Marti-Garcia, C.; Lopez-Leiva, I.; León-Campos, Á.; Fernandez-Ordoñez, E.; García-Guerrero, A.; Iglesias-Parra, M.R. A scoping review of safety management during clinical placements of undergraduate nursing students. Nurs. Outlook 2019, 67, 765–775. [Google Scholar] [CrossRef]
- Stolic, S.; Ng, L.; Southern, J.; Sheridan, G. Medication errors by nursing students on clinical practice: An integrative review. Nurse Educ. Today 2022, 112, 105325. [Google Scholar] [CrossRef]
- Elonen, I.; Salminen, L.; Brasaitė-Abromė, I.; Fuster, P.; Kukkonen, P.; Leino-Kilpi, H.; Löyttyniemi, E.; Noonan, B.; Stubner, J.; Svavarsdóttir, M.H.; et al. Medication calculation skills of graduating nursing students within European context. J. Clin. Nurs. 2021. [Google Scholar] [CrossRef]
- Luokkamäki, S.; Härkänen, M.; Saano, S.; Vehviläinen-Julkunen, K. Registered Nurses’ medication administration skills: A systematic review. Scand. J. Caring Sci. 2020, 35, 37–54. [Google Scholar] [CrossRef]
- Schroers, G.; Ross, J.G.; Moriarty, H. Nurses’ Perceived Causes of Medication Administration Errors: A Qualitative Systematic Review. Jt. Comm. J. Qual. Patient Saf. 2020, 47, 38–53. [Google Scholar] [CrossRef] [PubMed]
- Grugnetti, A.M.; Bagnasco, A.; Rosa, F.; Sasso, L. Effectiveness of a Clinical Skills Workshop for drug-dosage calculation in a nursing program. Nurse Educ. Today 2014, 34, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Moloney, M.; Kingston, L.; Doody, O. Fourth year nursing students’ perceptions of their educational preparation in medication management: An interpretative phenomenological study. Nurse Educ. Today 2020, 92, 104512. [Google Scholar] [CrossRef] [PubMed]
- Gladstone, J. Drug administration errors: A study into the factors underlying the occurrence and reporting of drug errors in a district general hospital. J. Adv. Nurs. 1995, 22, 628–637. [Google Scholar] [CrossRef]
- Güneş, Ü.Y.; Gürlek, Ö.; Sönmez, M. Factors contributing to medication errors in Turkey: Nurses’ perspectives. J. Nurs. Manag. 2014, 22, 295–303. [Google Scholar] [CrossRef]
- Wakefield, D.S.; Wakefield, B.J.; Uden-Holman, T.; Blegen, M.A. Perceived Barriers in Reporting Medication Administration Errors. Best Pract. Benchmarking Healthc. A Pract. J. Clin. Manag. Appl. 1996, 1, 191–197. [Google Scholar]
- Márquez-Hernández, V.V.; Fuentes-Colmenero, A.L.; Cañadas-Núñez, F.; Di Muzio, M.; Giannetta, N.; Gutiérrez-Puertas, L. Factors related to medication errors in the preparation and administration of intravenous medication in the hospital environment. PLoS ONE 2019, 14, e0220001. [Google Scholar] [CrossRef]
- Ginsburg, L.; Castel, E.; Tregunno, D.; Norton, P.G. The H-PEPSS: An instrument to measure health professionals’ perceptions of patient safety competence at entry into practice. BMJ Qual. Saf. 2012, 21, 676–684. [Google Scholar] [CrossRef]
- Aggar, C.; Dawson, S. Evaluation of student nurses’ perception of preparedness for oral medication administration in clinical practice: A collaborative study. Nurse Educ. Today 2014, 34, 899–903. [Google Scholar] [CrossRef]
- Caboral-Stevens, M.; Ignacio, R.V.; Newberry, G. Undergraduate nursing students’ pharmacology knowledge and risk of error estimate. Nurse Educ. Today 2020, 93, 104540. [Google Scholar] [CrossRef]
- Thelen, M.A. Medication competence: A concept analysis. Nurse Educ. Today 2022, 111, 105292. [Google Scholar] [CrossRef] [PubMed]
- Badia, X.; Baró, M.S.; Alonso, J. (Eds.) La Medida de la Salud: Guía de Escalas de Medición en Español, 4th ed.; Editec: Barcelona, Spain, 2007. [Google Scholar]
- Arribas, M. Diseño y Validación de Cuestionarios. Matronas Profesión 2004, 5, 23–29. [Google Scholar]
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S.L. Best Practices for Developing and Validating Scales for Health, Social, and Behavioral Research: A Primer. Front. Public Health 2018, 6, 149. [Google Scholar] [CrossRef] [PubMed]
- Gorgich, E.A.C.; Barfroshan, S.; Ghoreishi, G.; Yaghoobi, M. Investigating the Causes of Medication Errors and Strategies to Prevention of Them from Nurses and Nursing Student Viewpoint. Glob. J. Health Sci. 2015, 8, 220–227. [Google Scholar] [CrossRef] [Green Version]
- Manias, E.; Bullock, S. The educational preparation of undergraduate nursing students in pharmacology: Clinical nurses’ perceptions and experiences of graduate nurses’ medication knowledge. Int. J. Nurs. Stud. 2002, 39, 773–784. [Google Scholar] [CrossRef]
- Vaillancourt, R.; Khoury, C.; Pouliot, A. Validation of Pictograms for Safer Handling of Medications: Comprehension and Recall among Pharmacy Students. Can. J. Hosp. Pharm. 2018, 71, 258–266. [Google Scholar] [CrossRef]
- Villa, A.; Manuel, P. Aprendizaje Basado en Competencias: Una Propuesta Para la Evaluación de las Competencias Genéricas; Universidad de Deusto: Bilbao, Spain, 2007. [Google Scholar]
- Polit, D.F.; Beck, C.T. Essentials of Nursing Research: Appraising Evidence for Nursing Practice, 10th ed.; Wolters Kluwer: Tokyo, Japan, 2021. [Google Scholar]
- Hearnshaw, H.M.; Harker, R.M.; Cheater, F.M.; Baker, R.H.; Grimshaw, G.M. Expert consensus on the desirable characteristics of review criteria for improvement of health care quality. Qual. Health Care 2001, 10, 173–178. [Google Scholar] [CrossRef]
- Lloret-Segura, S.; Ferreres-Traver, A.; Hernandez, A.; Tomás, I. El análisis factorial exploratorio de los ítems: Una guía práctica, revisada y actualizada. An. De Psicol./Ann. Psychol. 2014, 30, 1151–1169. [Google Scholar] [CrossRef]
- Hair, J.F.; William, C.; Black, B.; Babin, J.; Rolph, E.A. Multivariate Data Analysis, 8th ed.; Cengage: Boston, MA, USA, 2018. [Google Scholar]
- Gropelli, T.; Shanty, J.A. Nursing Students’ Perceptions of Safety and Communication Issues in the Clinical Setting. J. Nurs. Educ. 2018, 57, 287–290. [Google Scholar] [CrossRef]
- Tella, S.; Smith, N.-J.; Jamookeeah, D.; Lamidi, M.-L.; Partanen, P.; Turunen, H. Learning to ensure patient safety in clinical settings: Comparing Finnish and British nursing students’ perceptions. J. Clin. Nurs. 2015, 24, 2954–2964. [Google Scholar] [CrossRef]
- Lee, S.E.; Quinn, B.L. Incorporating medication administration safety in undergraduate nursing education: A literature review. Nurse Educ. Today 2018, 72, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Palominos, E.; Levett-Jones, T.; Power, T.; Martinez-Maldonado, R. Healthcare students’ perceptions and experiences of making errors in simulation: An integrative review. Nurse Educ. Today 2019, 77, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Preston, P.; Leone-Sheehan, D.; Keys, B. Nursing student perceptions of pharmacology education and safe medication administration: A qualitative research study. Nurse Educ. Today 2018, 74, 76–81. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Patient Safety Curriculum Guide: Multi-Professional Edition. 2011. Available online: http://www.who.int/patientsafety/education/curriculum/curriculum-guide_SP.pdf?ua=1 (accessed on 10 January 2022).
- Benner, P.E. From Novice to Expert: Excellence and Power in Clinical Nursing Practice; Addison-Wesley Publishing Company, Nursing Division: Menlo Park, CA, USA, 1984. [Google Scholar]


{kind=link}
| Areas of Content | Description of Content |
|---|---|
| Drug knowledge and safety | Knowledge about the drug, its dose(s), administration routes, and administration protocols and guidelines |
| Thinking process | Reflection on the process of drug administration (prior preparation, administration, checking the effect, contextualizing the patient), including information, communication, reading the physician’s orders, dose scheduling, and informing patients about their treatment. |
| Training in safe medication management | In-service training, updating knowledge, sources of information, awareness of responsibility in clinical practice |
| Medication administration skills | Dose calculation, dilutions, and volumes, material needed for drug administration, contextualizing the individual patient, frequency, and practice of drug-dose calculations. |
| N (%) | |
|---|---|
| University | |
| A | 175 (31.3) |
| B | 133 (23.8) |
| C | 251 (44.9) |
| Female | 448 (80.1) |
| Age [mean (SD)] | 22.1 (4.8) |
| Experience working in health service (yes) | 168 (30.1) |
| Currently working in the health service (yes) | 66 (39.1) |
| Academic year * | |
| Second | 228 (40.9) |
| Third | 191 (34.2) |
| Fourth | 139 (24.9) |
| Dimension | No. Items | % Variance | Cronbach’s Alpha |
|---|---|---|---|
| Questionnaire 1 | 0.882 | ||
| Safety in drug prescription | 4 | 23.525 | 0.828 |
| Familiarity with pharmacological concepts | 4 | 2.028 | 0.800 |
| Relevance for professional practice | 1 * | 10.843 | 0.850 |
| Factors associated with risk of error | 3 | 6.668 | 0.789 |
| Importance of administering medication as prescribed | 4 | 2.490 | 0.649 |
| Verifications prior to drug administration | 3 | 5.452 | 0.762 |
| Thinking process in relation to medication management | 5 | 2.963 | 0.778 |
| Questionnaire 2 | 0.893 | ||
| Frequency of drug dose calculation | 11 | 36.11 | 0.886 |
| Learning drug dose calculation | 2 ** | 8.22 | 0.772 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fuster-Linares, P.; Alfonso-Arias, C.; Gallart Fernández-Puebla, A.; Rodríguez-Higueras, E.; García-Mayor, S.; Font-Jimenez, I.; Llaurado-Serra, M. Assessing Nursing Students’ Self-Perceptions about Safe Medication Management: Design and Validation of a Tool, the NURSPeM. Int. J. Environ. Res. Public Health 2022, 19, 4663. https://doi.org/10.3390/ijerph19084663
Fuster-Linares P, Alfonso-Arias C, Gallart Fernández-Puebla A, Rodríguez-Higueras E, García-Mayor S, Font-Jimenez I, Llaurado-Serra M. Assessing Nursing Students’ Self-Perceptions about Safe Medication Management: Design and Validation of a Tool, the NURSPeM. International Journal of Environmental Research and Public Health. 2022; 19(8):4663. https://doi.org/10.3390/ijerph19084663
Chicago/Turabian StyleFuster-Linares, Pilar, Cristina Alfonso-Arias, Alberto Gallart Fernández-Puebla, Encarna Rodríguez-Higueras, Silvia García-Mayor, Isabel Font-Jimenez, and Mireia Llaurado-Serra. 2022. "Assessing Nursing Students’ Self-Perceptions about Safe Medication Management: Design and Validation of a Tool, the NURSPeM" International Journal of Environmental Research and Public Health 19, no. 8: 4663. https://doi.org/10.3390/ijerph19084663