1. Introduction
Human influenza has become a severe global health problem in recent years. According to the World Health Organization estimation, influenza can cause 3–5 million severe illnesses and approximately 300,000 deaths each year [
1]. The World Health Organization re-emphasizes the importance of influenza monitoring and has established a set of standards for sentinel surveillance after suffering great losses in both the economy and people’s health during the influenza A (H1N1) pandemic in 2009 [
2]. Influenza surveillance networks for monitoring different indicators or targeting different populations are being set up worldwide [
3,
4]. The sanitation department collects and processes these data to provide policymakers with feasible prevention and control strategies.
The influenza vaccination program was considered a cost-effective measure and was recommended as the priority method against influenza. However, the accurate prediction of the start of the epidemic was correlated with the protective effect of the vaccine [
5,
6]. Setting up the epidemic threshold is one of the methods for disease prediction [
7]. Several studies have provided empirical or statistical methods to establish the epidemic threshold, such as the Serfling regression model [
8] and the moving logistic regression method [
9], or defined the epidemic threshold as 10% of the influenza detection rate [
10]. However, these methods cannot evaluate the intensity levels between seasons and have requirements for the form of data. In addition, the changes of epidemic patterns in different seasons led to the invalidity of a fixed proportion of the influenza detection rate. The moving epidemic method (MEM) was first put forward in Spain [
11] and has been adopted as a routine surveillance program to establish the epidemic threshold and intensity levels in some temperate countries [
12,
13]. Increasing studies in other climate zones have also demonstrated the high goodness of fit of the threshold established by the MEM [
14,
15,
16,
17]. In China, there is no standard method for setting epidemic thresholds, so introducing a practical method for early influenza detection will be helpful to reduce the disease burden for Chinese people.
Children are considered to be one of the high-risk populations for influenza. A previous study demonstrated that the school-aged children had a higher incidence rate than adults [
18], and school-aged children might have acted as the primary transmitter during the epidemic [
19]. A contact mode study in eight European countries indicated that it might be due to the high contact frequency in this age group [
20]. Offering the start time of the influenza epidemic in school-aged children can help the sanitation department take early and proper measures and reduce the disease burden in the whole population. However, most MEM studies have only concentrated on the general population. The epidemic threshold of school-aged children has not been discussed.
In this study, we analyzed the characteristics of influenza in Hubei Province from the season 2010/2011 to 2018/2019. Subsequently, we established the epidemic thresholds and intensity levels for the school-aged populations and compared the goodness of fit between the models established by different age group data. The feasibility of the moving epidemic method was evaluated by the cross-validation process.
2. Materials and Methods
2.1. Case Identification
Influenza-like illness (ILI) was described as a patient whose body temperature was above 38 °C with either cough or sore throat, with the lack of other experimental diagnoses. A period of high body temperature should happen in the course of the acute fever.
2.2. Sample Source
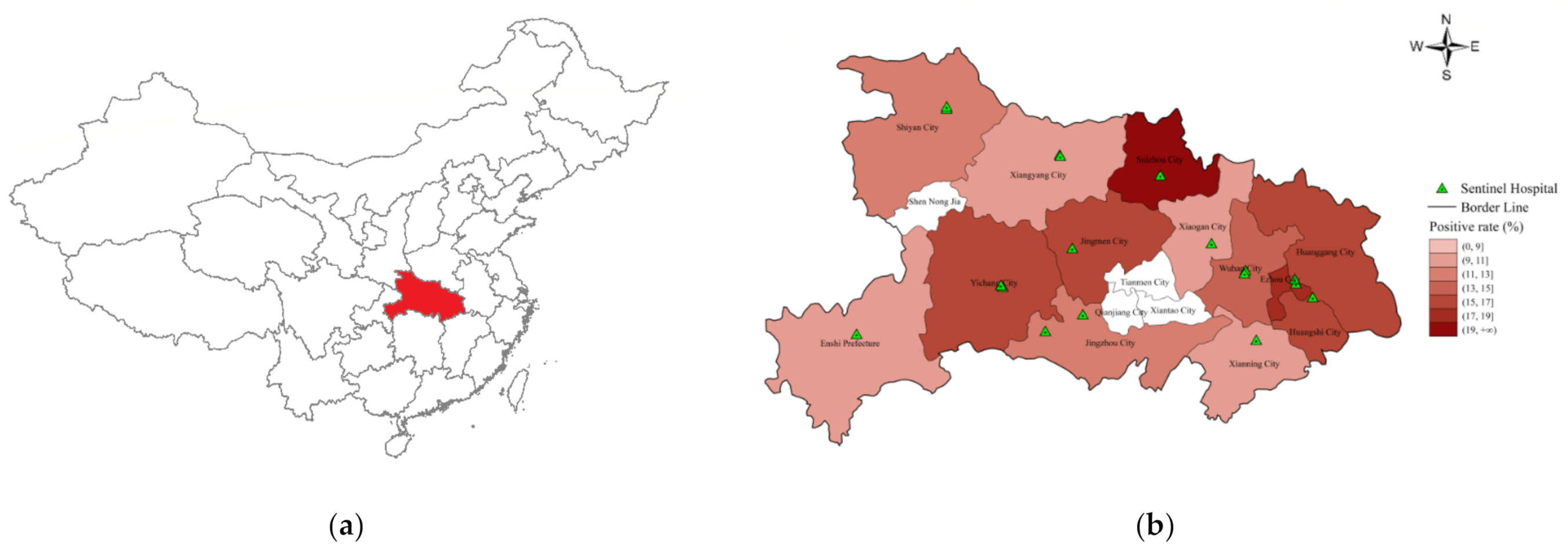
Hubei Province is a subtropical area located in Central China (108°21′–116°07′ E, 29°01′–33°6′ N), including twelve cities, one prefecture and four administrative cities directly under the jurisdiction of the province. It covers an area of 185,900 km2, with 55,750,000 permanent residents, including more than 8,610,000 school-aged children.
Sentinel hospitals were set up in 2000 to collect influenza-like illness visitors’ information, and the locations of the national sentinel hospitals are shown in
Figure 1. The absence of a sentinel hospital in some cities was due to the small size of the population (Shen Nong Jia) or that they were directly under the governance of Hubei Province (Qianjiang City, Tianmen City and Xiantao City). Each sentinel hospital was asked to collect 20 swab samples (including throat swabs, nasal swabs and nasopharyngeal swabs) per surveillance week from ILI patients. The swab samples were collected in sampling tubes and stored at 2–8 °C and then transported to the laboratory of a local municipal center for disease control and prevention (CDC) for further testing. Real-time reverse transcription-polymerase chain reaction (RT-PCR) was used to identify the subtypes of the influenza virus, and the results were submitted to the national influenza surveillance network. The quality of the test results of each city was reviewed by the influenza reference laboratory of Hubei CDC.
2.3. Data Collection
In mainland China, children above three years old are able to attend kindergarten. According to the living environment and social contact mode, we roughly divided the whole population into three age groups. We defined the population below three years old as pre-school children and the population above eighteen years old as adults, while the rest were defined as school-aged children, who spent most of the time in a classroom and had more opportunities to interact with others.
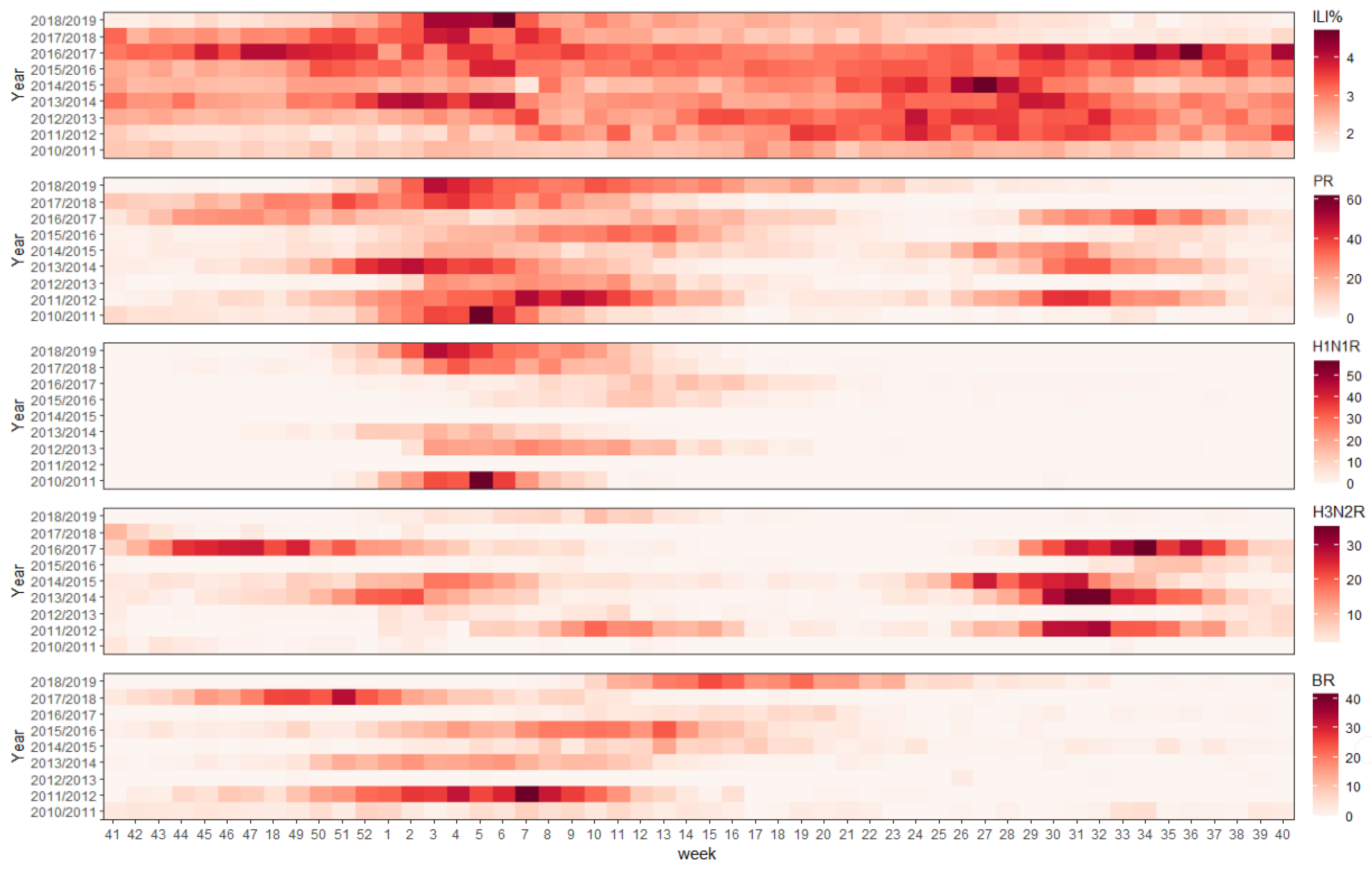
In Hubei Province, all three influenza strains occurred in the winter, while influenza A(H3N2) intermittently occurred in the summer. To include the entire prevalence curve of each strain, we defined the epidemic surveillance period of Hubei Province as week 40 to week 41 of the following calendar year. This study obtained the surveillance data from season 2010/2011 to 2018/2019, with 468 epidemic weeks. Due to the technical limitations, the influenza A strains in the first several surveillance seasons contained many untyped samples. We did not further divide these data like in another study [
21] to avoid potential confounding factors.
2.4. Moving Epidemic Method
The MEM procedure could be divided into three steps: The first step was to define the epidemic period. The maximum accumulated rates percentage method (MAP) was applied to divide the season into the pre-epidemic, epidemic, and post-epidemic periods. The epidemic period defined by this algorithm was the real epidemic period. The details can be found in a previous study [
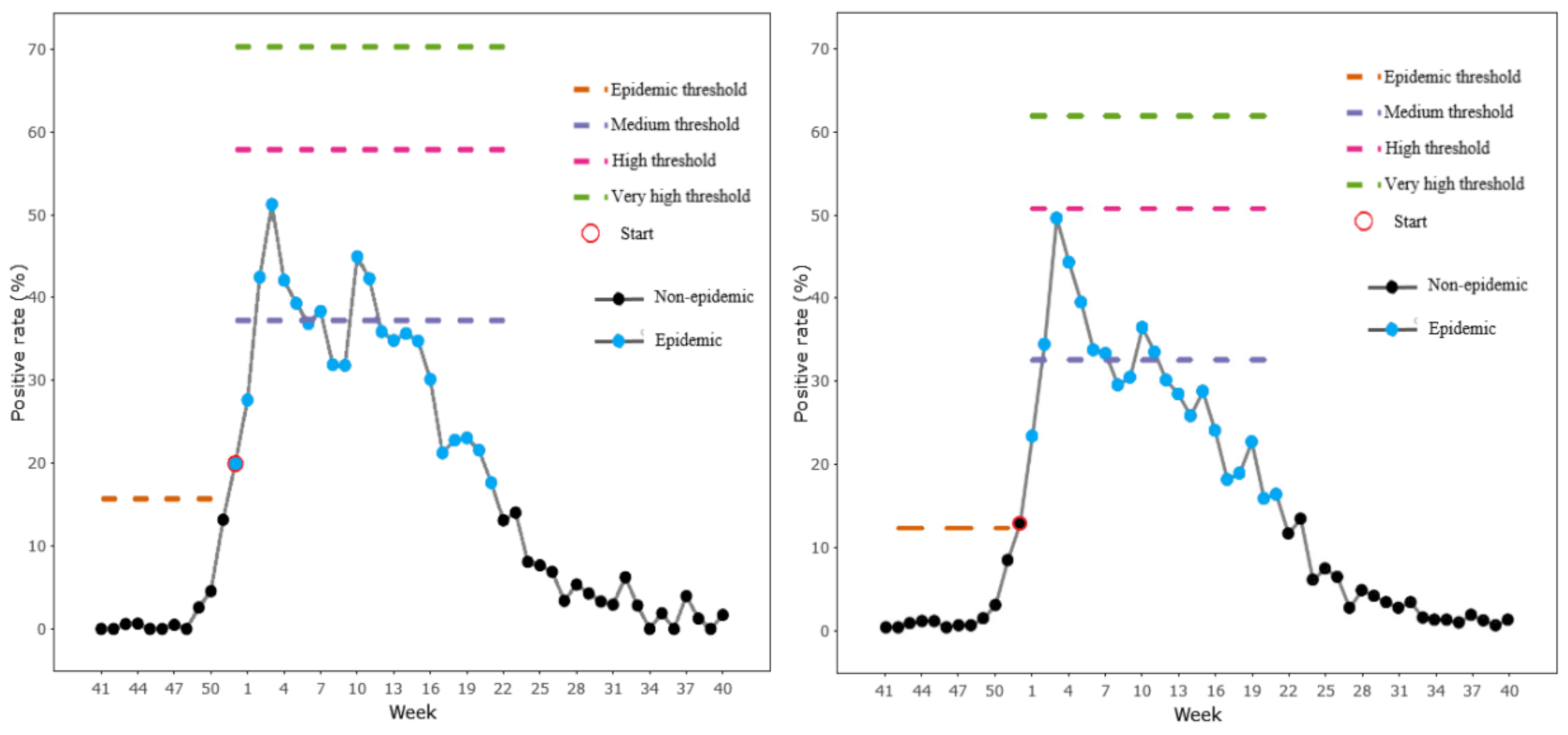
11]. Parameter δ plays a vital role in this step, as this is a pre-defined parameter recommended to range from 2.0% to 4.0%, and the proper value was chosen by the criteria of the highest Youden’s Index (YI). The second step was to establish the epidemic and the intensity thresholds. The epidemic thresholds were calculated as the upper limits of the 95% one-sided confidence interval of the arithmetic mean of the 30 highest weekly values of the pre-epidemic and post-epidemic periods. The epidemic intensity thresholds were calculated as the upper limits of the 40%, 90% and 97.5% one-sided confidence intervals of the geometric mean of the 30 highest weekly values of the epidemic period. The medium intensity, the high intensity and the very high intensity were defined as 40%, 90% and 97.5%, respectively. The final step was to assess the performance of the model. The MEM adopted a cross-validation procedure to estimate the epidemic thresholds and assess the goodness of fit. This cross-validation procedure was performed by extracting every epidemic season from the historical data and using the remaining seasons to calculate the threshold of the extracted one. When the weekly positive rate exceeded the epidemic threshold for two consecutive weeks, the first week was defined as the alert week. The timeliness was the number of weeks between the alert week and the first week of the epidemic period defined in the first step. If the alert week was after the real start week, it was defined as the detection lag. Sensitivity (Se) was calculated as the number of weeks above the epidemic and post-epidemic thresholds divided by the number of real epidemic weeks, and specificity (Sp) was defined as the number of weeks below the epidemic and post-epidemic thresholds divided by the number of real nonepidemic weeks. Similar indicators, such as the positive predictive value (PPV), negative predictive value (NPV) and Youden’s Index (YI = Sp + Se − 1), were further developed to assess the performance of the model.
Influenza epidemics occur twice per season in Hubei Province. We applied the two-wave transformation tool offered by the R package “memapp” [
22] to separate these double-peak data. However, a three-peak epidemic pattern was observed in season 2016/2017. We excluded this season from calculating the total influenza thresholds, because the transformation tool could not separate this season. For the type-specific strain, we followed the examples of the study in Guangdong Province and Scotland [
17,
23], and the epidemic threshold was calculated using weekly data in the seasons when the proportion of the strain exceeded 20%. We defined the last season as the test set for each influenza strain, while the other was the training data. The MEM package version 2.16 of R language software performed the procedure.
2.5. Statistical Method
The influenza positive rates and the proportions of the different age groups were compared using the Pearson chi-square test. The intensity levels, the average start week and the duration were compared by the Mann–Whitney U test. These procedures were conducted by IBM SPSS Statistics 25 (SPSS Inc., Chicago, IL, USA).
4. Discussion
This study described the influenza epidemiology characteristics in Hubei Province from season 2010/2011 to 2018/2019, established the epidemic thresholds for the general and age-specific groups and assessed the MEM performance between these groups. Our study proved the feasibility of applying the MEM in Hubei Province and proposed that the school-aged children could replace the general population for influenza routine surveillance. To our knowledge, this study is one of the first attempts in applying the MEM to establish the thresholds for age-specific groups in the subtropical region.
Choosing proper indicators can help with improving the effectiveness of the model. This study applied the virology data rather than the ILI incidence rate to fit the MEM. Previous studies have proved the feasibility of a series of indicators to establish the influenza prediction model, including the ILI incidence rate or cases [
24], virology data [
21], excess mortality rate [
25] and school absenteeism rate [
26]. In Hubei Province, a poor correlation was found between the positive and ILI incidence rates, and the ILI seemed to provide less seasonality. ILI could be affected by multiple factors, such as the coinfection of other respiratory viruses with similar symptoms, the willingness of parents to send their children to medical care and the criteria used to define ILI. These findings suggested that the ILI incidence rate may not be a suitable indicator for establishing the influenza model in tropical and subtropical areas, which was in line with other studies. [
27,
28].
For the general population, the influenza epidemic threshold in season 2018/2019 was defined as 12.10%, lower than the thresholds established for all subtropical cities in China [
29]. A difference was also found between the epidemic thresholds for Guangdong Province and its climate zone [
17]. These results may be attributed to the large territory in China, which leads to climate and economic differences among provinces, finally resulting in various influenza epidemic patterns of regions even in the same climate zones. However, we found that, when there was a double-peak influenza pattern in Hubei Province, a similar phenomenon could also be observed in all studied cities of Hubei Province, implying that the epidemiological differences between cities may not be as great as the differences at the provincial level. This assumption was also supported by Yu and his colleagues [
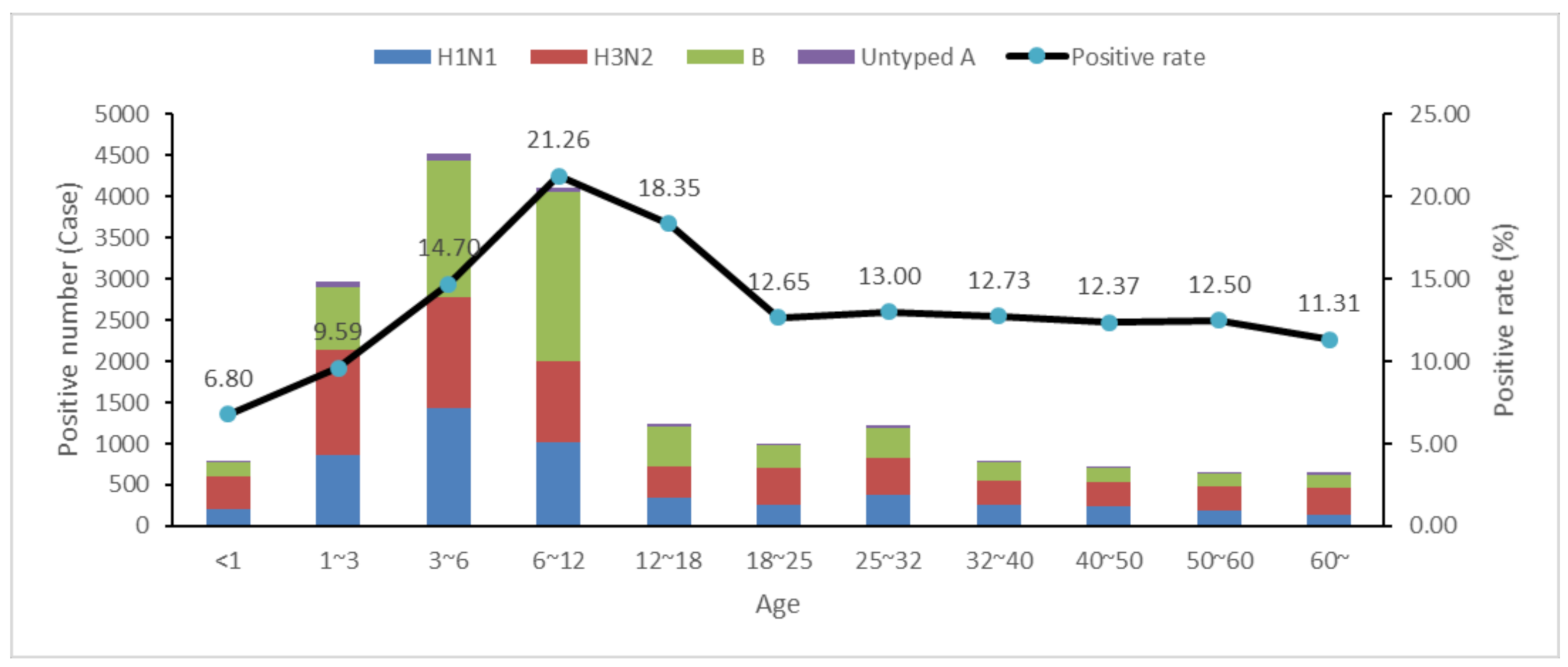
30], which made it possible to establish the influenza thresholds at the provincial level. Nevertheless, we also observed that the positive rate of influenza among cities in Hubei Province was varied, ranging from 9.18% to 19.06%. Nevertheless, using virology data to establish the epidemic thresholds for each city was not feasible due to the lack of ILI samples sent for laboratory testing per week. If we want to establish more accurate thresholds for influenza detection, we will have to increase the number of test samples, which requires a higher laboratory testing capacity. In the current situation, where the laboratory testing capacity was relatively fixed, adapting a specific population for testing may be one of the solutions. According to our observations, most test samples came from 1–6 year old, but the 6–12 age group had the highest infection rate. A similar phenomenon was also observed in Niger [
31] and several states of the United States [
24]. Moreover, the cross-validation analysis showed that school-aged children performed better in MEM. These findings suggest that school-aged children might be a worthy and suitable population to study the influenza prevalence. In Hubei Province, the comparison of the start week provided slight differences among the different age groups. This phenomenon was also observed in Canada and Korea [
32,
33], making it possible for countries that do not have enough laboratory testing capacity to substitute school-aged children for the whole population surveillance.
The concept of a school-based surveillance system was proposed 20 years ago [
34], and its effectiveness has been proven in studies in different countries [
26,
35,
36]. In China, school-based surveillance has been incorporated into community influenza surveillance. However, the current school-based surveillance system only concentrates on syndromic indicators such as absenteeism and ILI rates. Compared with other age groups, the student samples were easier to obtain and manage. Establishing a school-based virology surveillance system could help to quickly identify the circulating strain and utilize relatively small samples for influenza monitoring.
A vaccination program among school-aged children was recommended in the United States [
18,
37] and Europe [
38]. In China, the health insurance system does not cover the influenza vaccination [
39], partly responsible for the low levels of vaccine coverage. Our study revealed that influenza B was most prevalent in school-aged children. Quadrivalent influenza vaccination among this age group might have considerable efficacy. However, the timings of influenza B epidemics are highly variable, so accurate predictions of the onset of an epidemic is crucial for vaccination.
The MEM provided a simple approach for establishing the epidemic threshold to detect the epidemic start week and has a relatively low data requirement. A study in England suggested that the MEM was more suitable than the empirical percentile methods for monitoring the onset of an epidemic [
40] and has been utilized for influenza routine surveillance in Europe. However, we found that seasons with low intensities could affect the MEM performance. Taking influenza B as an example, after excluding season 2010/2011 from the training set, all the indexes reflecting a goodness of fit increased significantly. These results suggested that the historical data should be filtered before applying it to the MEM model. The robustness of the MEM will be increased while using relatively stable historical data. However, no study has provided a formal method for season selection. Further research on the inclusion criteria should be conducted in the future.
This study had several limitations. First, the virology data of Hubei Province did not divide the B lineages into influenza B (Yamagata) and influenza B (Victoria), which have different timings of the onset and epidemic periods [
41] and may lead to the false identification of the long and low intensities of influenza B activity. With the reduction in the cost of laboratory tests [
42], more specific data was enabled to be well-documented. Second, establishing the epidemic thresholds by the MEM requires the training set to include enough seasons. However, while we applied the virology data of the type-specific strain, the seasons included in the training set of each strain were less than five seasons [
11], which may have decreased the robustness of the model.




{kind=link}
{kind=link}
{kind=link}
{kind=link}



