
Exploring the Protective Function of Positivity and Regulatory Emotional Self-Efficacy in Time of Pandemic COVID-19

 , , , , ,
, , , , ,
Abstract
:1. Introduction
1.1. Positivity
1.2. Regulatory Emotional Self-Efficacy
1.3. The Present Research
2. Materials and Methods
2.1. Procedure
2.2. Measures
2.2.1. Positivity
2.2.2. Regulatory Emotional Self-Efficacy
2.2.3. State Anxiety
2.2.4. Depressive Symptoms
2.2.5. Self-Efficacy in Complying with the Containment Measures
2.2.6. Control Variables
2.3. Strategy of Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Preliminary Analyses
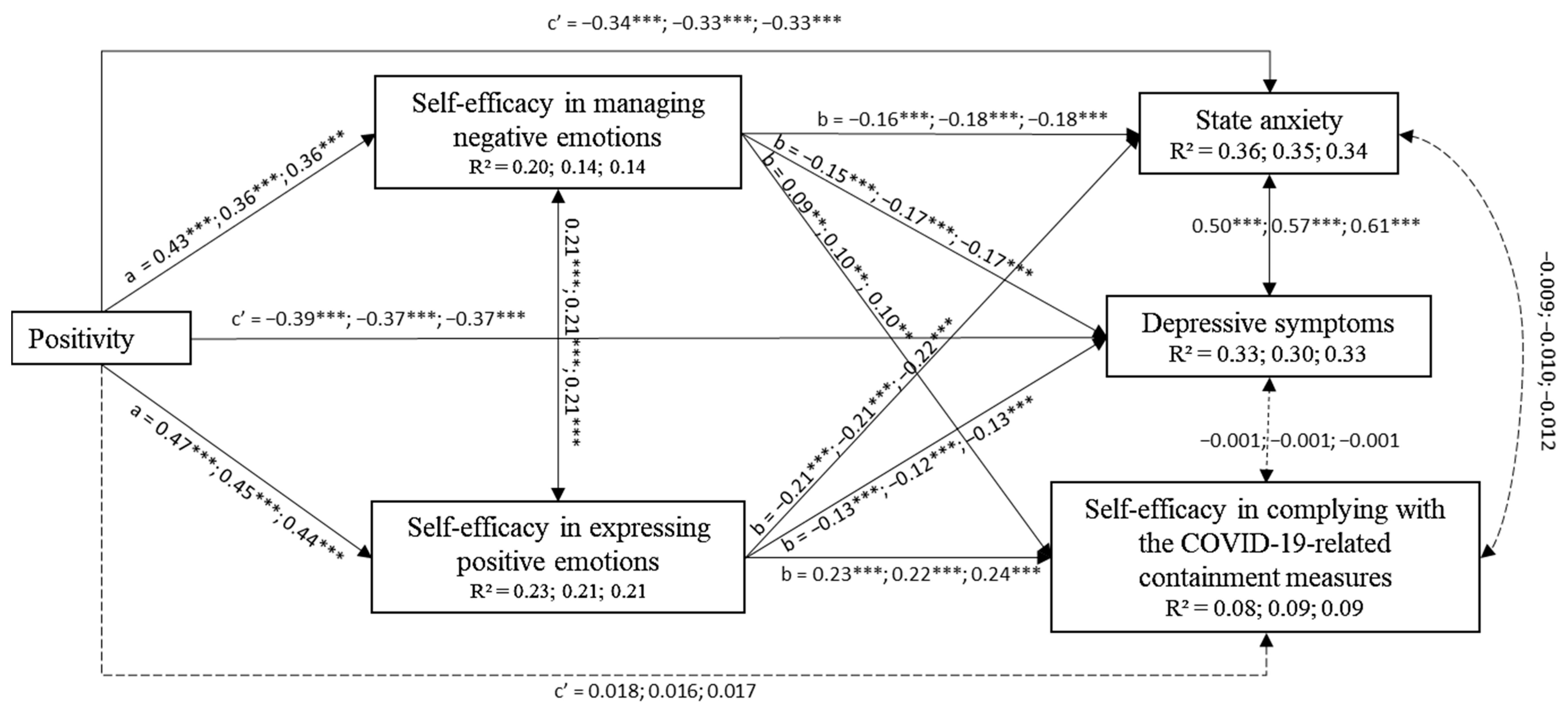
3.3. The Mediational Multi-Groups Path Analysis Model
3.3.1. Positivity, Regulatory Emotional Self-Efficacy, Anxiety, and Depression Symptoms
3.3.2. Positivity, Regulatory Emotional Self-Efficacy, and Perceived Self-Efficacy Beliefs in Complying with the Containment Measures
3.3.3. The Effects of Gender and SES
3.4. Alternative Model
4. Discussion
4.1. Direct Effects of Positivity on Mental Health Outcomes
4.2. Direct Effects of Regulation Emotional Self-Efficacy Beliefs on Mental Health Outcomes
4.3. The Mediation Effect of Regulatory Emotional Self-Efficacy on the Relation of Positivity and Mental Health Outcomes
4.4. The Moderation Effect of Age
4.5. The Effects of the Gender and SES
5. Conclusions
6. Limitations and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- ISTAT (Italian National Statistic Institute). Impatto Dell’epidemia COVID-19 sulla Mortalità Totale della Popolazione Residente. Anno 2020 e Gennaio–Aprile 2021. 2021. Available online: https://www.istat.it/it/files//2021/06/Report_ISS_Istat_2021_10_giugno.pdf (accessed on 10 June 2021).
- Signorelli, C.; Scognamiglio, T.; Odone, A. COVID-19 in Italy: Impact of containment measures and prevalence estimates of infection in the general population. Acta Biomed. 2020, 91, 175–179. [Google Scholar] [CrossRef]
- Odone, A.; Lugo, A.; Amerio, A.; Borroni, E.; Bosetti, C.; Carreras, G.; Cavalieri d’Oro, L.; Colombo, P.; Fanucchi, T.; Ghislandi, S.; et al. COVID-19 lockdown impact on lifestyle habits of Italian adults. Acta Biomed. 2020, 91, 87–89. [Google Scholar] [PubMed]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Fiorillo, A.; Gorwood, P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur. Psychiatry 2020, 63, e32. [Google Scholar] [CrossRef] [Green Version]
- Adhanom Ghebreyesus, T. Addressing mental health needs: An integral part of COVID-19 response. World Psychiatry 2020, 19, 129–130. [Google Scholar] [CrossRef]
- Di Giuseppe, M.; Zilcha-Mano, S.; Prout, T.A.; Perry, J.C.; Orrù, G.; Conversano, C. Psychological Impact of Coronavirus Disease 2019 Among Italians During the First Week of Lockdown. Front. Psychiatry 2020, 11, 576597. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 Pandemic and Lockdown Measures Impact on Mental Health Among the General Population in Italy. Front. Psychiatry 2020, 11, 790. [Google Scholar] [CrossRef] [PubMed]
- Casagrande, M.; Favieri, F.; Tambelli, R.; Forte, G. The enemy who sealed the world: Effects quarantine due to the COVID-19 on sleep quality, anxiety, and psychological distress in the Italian population. Sleep Med. 2020, 75, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Amendola, S.; Spensieri, V.; Hengartner, M.P.; Cerutti, R. Mental health of Italian adults during COVID-19 pandemic. Br. J. Health Psychol. 2021, 26, 644–656. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, A.; Sampogna, G.; Giallonardo, V.; Del Vecchio, V.; Luciano, M.; Albert, U.; Carmassi, C.; Carrà, G.; Cirulli, F.; Dell’Osso, B.; et al. Effects of the lockdown on the mental health of the general population during the COVID-19 pandemic in Italy: Results from the COMET collaborative network. Eur. Psychiatry 2020, 63, e87. [Google Scholar] [CrossRef]
- Parola, A.; Rossi, A.; Tessitore, F.; Troisi, G.; Mannarini, S. Mental Health Through the COVID-19 Quarantine: A Growth Curve Analysis on Italian Young Adults. Front. Psychol. 2020, 11, 567484. [Google Scholar] [CrossRef]
- Unützer, J.; Kimmel, R.J.; Snowden, M. Psychiatry in the age of COVID-19. World Psychiatry 2020, 19, 130–131. [Google Scholar] [CrossRef]
- Seligman, M.E.P. Positive psychology, positive prevention, and positive therapy. In Handbook of Positive Psychology; Snyder, C.R., Lopez, S.J., Eds.; Oxford University Press: New York, NY, USA, 2002; pp. 3–9. [Google Scholar]
- Seligman, M.E.P. Positive psychology: Fundamental assumptions. Psychologist 2003, 16, 126–127. [Google Scholar]
- Seligman, M.E.P.; Csikszentmihalyi, M. Positive psychology: An introduction. Am. Psychol. 2000, 55, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. The explanatory and predictive scope of self-efficacy theory. J. Soc. Clin. Psychol. 1986, 4, 359–373. [Google Scholar] [CrossRef]
- Bandura, A. Human agency in social cognitive theory. Am. Psychol. 1989, 44, 1175–1184. [Google Scholar] [CrossRef]
- Bandura, A. Social cognitive theory of self-regulation. Organ. Behav. Hum. Decis. Process. 1991, 50, 248–287. [Google Scholar] [CrossRef]
- Bandura, A. Social cognitive theory: An agentic perspective. Annu. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Caprara, G.V.; Alessandri, G.; Caprara, M. The associations of positive orientation with health and psychosocial adaptation: A review of findings and perspectives. Asian J. Soc. Psychol. 2019, 22, 126–132. [Google Scholar] [CrossRef]
- Alessandri, G.; Vecchione, M.; Caprara, G.V. Assessment of regulatory emotional self-efficacy beliefs: A review of the status of the art and some suggestions to move the field forward. J. Psychoeduc. Assess. 2014, 33, 24–32. [Google Scholar] [CrossRef]
- Caprara, G.V.; Castellani, V.; Alessandri, G.; Mazzuca, F.; La Torre, M.; Barbaranelli, C.; Colaiaco, F.; Gerbino, M.; Pasquali, V.; D’Amelio, R.; et al. Being positive despite illness: The contribution of positivity to the quality of life of cancer patients. Psychol. Health 2016, 31, 524–534. [Google Scholar] [CrossRef]
- Bandura, A.; Caprara, G.V.; Barbaranelli, C.; Gerbino, M.; Pastorelli, C. Role of affective self-regulatory efficacy on diverse spheres of psychosocial functioning. Child Dev. 2003, 74, 769–782. [Google Scholar] [CrossRef]
- Caprara, G.V.; Fagnani, C.; Alessandri, G.; Steca, P.; Gigantesco, A.; Cavalli-Sforza, L.L.; Stazi, M.A. Human optimal functioning: The genetics of positive orientation towards self, life, and the future. Behav. Genet. 2009, 39, 277–284. [Google Scholar] [CrossRef]
- Alessandri, G.; Caprara, G.V.; Tisak, J. The unique contribution of positive orientation to optimal functioning: Further explorations. Eur. Psychol. 2012, 17, 44–54. [Google Scholar] [CrossRef]
- Caprara, G.V.; Alessandri, G.; Barbaranelli, C. Optimal Functioning: Contribution of Self-Efficacy Beliefs to Positive Orientation. Psychother. Psychosom. 2010, 79, 328–330. [Google Scholar] [CrossRef]
- Caprara, G.V.; Steca, P. The contribution of self-regulatory efficacy beliefs in managing affect and family relationships to positive thinking and hedonic balance. J. Soc. Clin. Psychol. 2006, 25, 601–625. [Google Scholar] [CrossRef]
- Caprara, G.V.; Steca, P.; Alessandri, G.; Abela, J.R.Z.; McWhinnie, C.M. Positive orientation: Explorations on what is common to life satisfaction, self-esteem, and optimism. Epidemiol. Psichiatr. Soc. 2010, 19, 63–71. [Google Scholar] [CrossRef]
- Caprara, G.V.; Alessandri, G.; Eisenberg, N.; Kupfer, A.; Steca, P.; Caprara, M.G.; Abela, J. The Positivity Scale. Psychol. Assess. 2012, 24, 701–712. [Google Scholar] [CrossRef]
- Baumeister, R.F. (Ed.) Self-Esteem: The Puzzle of Low Self-Regard; Plenum Press: New York, NY, USA, 1993. [Google Scholar]
- Greenberg, J.; Solomon, S.; Pyszczynski, T.; Rosenblatt, A.; Burling, J.; Lyon, D.; Simon, L.; Pinel, E. Why do people need self-esteem? Converging evidence that self-esteem serves an anxiety-buffering function. J. Personal. Soc. Psychol. 1992, 63, 913–922. [Google Scholar] [CrossRef]
- Kernis, M.H. Toward a Conceptualization of Optimal Self-Esteem. Psychol. Inq. 2003, 14, 1–26. [Google Scholar] [CrossRef]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: New Jersey, NJ, USA, 1985. [Google Scholar]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Scheier, M.F.; Carver, C.S. On the power of positive thinking: Benefits of being optimistic. Curr. Dir. Psychol. Sci. 1993, 2, 26–30. [Google Scholar] [CrossRef]
- Caprara, G.V.; Alessandri, G.; Colaiaco, F.; Zuffianò, A. Dispositional bases of self-serving positive evaluations. Personal. Individ. Differ. 2013, 55, 864–867. [Google Scholar] [CrossRef]
- Alessandri, G.; Vecchione, M.; Tisak, J.; Deiana, G.; Caria, S.; Caprara, G.V. The utility of positive orientation in predicting job performance and organisational citizenship behaviors. Appl. Psychol. 2012, 61, 669–698. [Google Scholar] [CrossRef]
- Barbaranelli, C.; Paciello, M.; Biagioli, V.; Fida, R.; Tramontano, C. Positivity and Behaviour: The Mediating Role of Self-Efficacy in Organisational and Educational Settings. J. Happiness Stud. 2018, 20, 707–727. [Google Scholar] [CrossRef]
- Livi, S.; Alessandri, G.; Caprara, G.V.; Pierro, A. Positivity within teamwork: Cross-level effects of positivity on performance. Personal. Individ. Differ. 2015, 85, 230–235. [Google Scholar] [CrossRef]
- Caprara, G.V.; Eisenberg, N.; Alessandri, G. Positivity: The dispositional basis of happiness. J. Happiness Stud. 2017, 18, 353–371. [Google Scholar] [CrossRef]
- Castellani, V.; Perinelli, E.; Gerbino, M.; Caprara, G.V. Positive orientation and interpersonal styles. Personal. Individ. Differ. 2016, 98, 229–234. [Google Scholar] [CrossRef]
- Luengo Kanacri, B.P.; Eisenberg, N.; Thartori, E.; Pastorelli, C.; Uribe Tirado, L.M.; Gerbino, M.; Caprara, G.V. Longitudinal relations among positivity, perceived positive school climate, and prosocial behavior in Colombian adolescents. Child Dev. 2017, 88, 1100–1114. [Google Scholar] [CrossRef]
- Caprara, M.; Di Giunta, L.; Caprara, G.V. Association of positivity with health problems in old age: Preliminary findings from Spanish middle class seniors. J. Happiness Stud. 2017, 18, 1339–1358. [Google Scholar] [CrossRef]
- Clark, D.A.; Beck, A.T. Scientific Foundations of Cognitive Theory and Therapy of Depression; Wiley: New York, NY, USA, 1999. [Google Scholar]
- Zuffianò, A.; López-Pérez, B.; Cirimele, F.; Kvapilová, J.; Caprara, G.V. The Positivity Scale: Concurrent and Factorial Validity Across Late Childhood and Early Adolescence. Front. Psychol. 2019, 10, 831. [Google Scholar] [CrossRef] [PubMed]
- Fagnani, C.; Medda, E.; Stazi, M.A.; Caprara, G.V.; Alessandri, G. Investigation of age and gender effects on positive orientation in Italian twins. Int. J. Psychol. 2014, 49, 453–461. [Google Scholar] [CrossRef]
- Alessandri, G.; Caprara, G.V.; De Pascalis, V. Relations among EEG-alpha asymmetry and positivity personality trait. Brain Cogn. 2015, 97, 10–21. [Google Scholar] [CrossRef] [PubMed]
- Milioni, M.; Alessandri, G.; Eisenberg, N.; Caprara, G.V. The role of positivity as predictor of ego-resiliency from adolescence to young adulthood. Personal. Individ. Differ. 2016, 101, 306–311. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control; Freeman: New York, NY, USA, 1997. [Google Scholar]
- Bakioğlu, F.; Korkmaz, O.; Ercan, H. Fear of COVID-19 and Positivity: Mediating Role of Intolerance of Uncertainty, Depression, Anxiety, and Stress. Int. J. Ment. Health Addict. 2020, 28, 1–14. [Google Scholar] [CrossRef]
- Yildirim, M.; Güler, A. Positivity explains how COVID-19 perceived risk increases death distress and reduces happiness. Personal. Individ. Differ. 2021, 168, 110347. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.J. Handbook of Emotion Regulation, 2nd ed.; Guilford Press: New York, NY, USA, 2014. [Google Scholar]
- Werner, K.; Gross, J.J. Emotion regulation and psychopathology: A conceptual framework. In Emotion Regulation and Psychopathology: A Transdiagnostic Approach to Etiology and Treatment; Kring, A.M., Sloan, D.M., Eds.; Guilford Press: New York, NY, USA, 2010; pp. 13–37. [Google Scholar]
- Caprara, G.V.; Di Giunta, L.; Eisenberg, N.; Gerbino, M.; Pastorelli, C.; Tramontano, C. Assessing regulatory emotional self-efficacy in three countries. Psychol. Assess. 2008, 20, 227–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caprara, G.V.; Gerbino, M. Autoefficacia Emotiva Percepita: La capacità di regolare l’affettività negativa e di esprimere quella positiva. In La Valutazione Dell’autoefficacia; Caprara, G.V., Ed.; Edizioni Erickson: Trento, Italy, 2001; pp. 35–50. [Google Scholar]
- Caprara, G.V.; Steca, P. Affective and social self-regulatory efficacy beliefs as determinants of positive thinking and happiness. Eur. Psychol. 2005, 10, 275–286. [Google Scholar] [CrossRef]
- Caprara, G.V.; Steca, P. Self-efficacy beliefs as determinants of prosocial behavior conducive to life satisfaction across ages. J. Soc. Clin. Psychol. 2005, 24, 191–217. [Google Scholar] [CrossRef]
- Alessandri, G.; Caprara, G.V.; Eisenberg, N.; Steca, P. Reciprocal relations among self-efficacy beliefs and prosociality across time. J. Personal. 2009, 77, 1229–1259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caprara, G.V.; Alessandri, G.; Barbaranelli, C.; Vecchione, M. The longitudinal relations between self-esteem and affective self-regulatory efficacy. J. Res. Personal. 2013, 47, 859–870. [Google Scholar] [CrossRef]
- McAdams, D.P. What do we know when we know a person? J. Personal. 1995, 36, 365–396. [Google Scholar] [CrossRef] [Green Version]
- Fiorenzato, E.; Zabberoni, S.; Costa, A.; Cona, G. Cognitive and mental health changes and their vulnerability factors related to COVID-19 lockdown in Italy. PLoS ONE 2021, 16, e0246204. [Google Scholar] [CrossRef] [PubMed]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: Immediate psychological responses and associated factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef] [PubMed]
- Medda, E.; Toccaceli, V.; Gigantesco, A.; Picardi, A.; Fagnani, C.; Stazi, M.A. The COVID-19 pandemic in Italy: Depressive symptoms immediately before and after the first lockdown. J. Affect. Disord. 2021, 298, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moghanibashi-Mansourieh, A. Assessing the anxiety level of Iranian general population during COVID-19. Asian J. Psychiatry 2020, 51, 102076. [Google Scholar] [CrossRef]
- Fricker, R.D. Sampling methods for web and e-mail surveys. In The SAGE Handbook of Online Research Methods; Fielding, N., Blank, G., Lee, R.M., Eds.; SAGE: Thousand Oaks, CA, USA, 2008; pp. 195–216. [Google Scholar]
- Heikamp, T.; Alessandri, G.; Laguna, M.; Petrovic, V.; Caprara, M.G.; Trommsdorff, G. Cross-cultural validation of the positivity-scale in five European countries. Personal. Individ. Differ. 2014, 71, 140–145. [Google Scholar] [CrossRef] [Green Version]
- Borsa, J.C.; Damásio, B.F.; Souza, D.S.D.; Koller, S.H.; Caprara, G.V. Psychometric properties of the positivity scale-Brazilian version. Psicol. Reflexão Crítica 2015, 28, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Macías, A.B. Validación psicométrica preliminar de la escala de positividad en dos muestras de agentes educativos Mexicanos. Cuad. Hispanoam. Psicol. 2015, 15, 75–85. [Google Scholar] [CrossRef] [Green Version]
- Tian, L.; Zhang, D.; Huebner, E.S. Psychometric properties of the positivity scale among Chinese adults and early adolescents. Front. Psychol. 2018, 9, 197. [Google Scholar] [CrossRef] [Green Version]
- McDonald, R.P. Test Theory: A Unified Treatment; Lawrence Erlbaum: Mahwah, NJ, USA, 1999. [Google Scholar]
- Gunzenhauser, C.; Heikamp, T.; Gerbino, M.; Alessandri, G.; von Suchodoletz, A.; Di Giunta, L.; Caprara, G.V.; Trommsdorff, G. Self-efficacy in regulating positive and negative emotions: A validation study in Germany. Eur. J. Psychol. Assess. 2013, 29, 197–204. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, T.E.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Julian, L.J. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS-A). Arthritis Care Res. 2011, 63, S467–S472. [Google Scholar] [CrossRef] [Green Version]
- Pedrabissi, L.; Santinello, M. Verifica della Validità dello STAI Forma Y di Spielberger. Giunti Organ. Spec. 1989, 191–192, 11–14. [Google Scholar]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Radloff, L.S.; Teri, L. Use of the Center for Epidemiological Studies-Depression Scale with older adults. Clin. Gerontol. 1986, 5, 119–136. [Google Scholar] [CrossRef]
- Balsamo, M.; Saggino, A. Depression assessment questionnaires in the Italian context: A critical analysis. Psicoter. Cogn. Comport. 2007, 13, 167–199. [Google Scholar]
- Weissman, M.M.; Sholomskas, D.; Pottenger, M.; Prushoff, B.A.; Locke, B.Z. Assessing depressive symptoms in five psychiatric populations: A validation study. Am. J. Epidemiol. 1977, 106, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Orme, J.G.; Reis, J.; Herz, E.J. Factorial and discriminant validity of the Center for Epidemiological Studies Depression (CES-D) Scale. J. Clin. Psychol. 1986, 42, 28–33. [Google Scholar] [CrossRef]
- Bandura, A. Guide to the construction of self-efficacy scales. In Self-Efficacy Beliefs of Adolescents; Pajares, F., Urdan, T., Eds.; Information Age Publishing: Greenwich, CT, USA, 2006; pp. 1–43. [Google Scholar]
- Cattell, R.B.; Vogelmann, S. A comprehensive trial of the screeand KG criteria for determining the number of factors. Multivar. Behav. Res. 1977, 12, 289–325. [Google Scholar] [CrossRef] [PubMed]
- Hattie, J. Methodology review: Assessing unidimensionality of tests and items. Appl. Psychol. Meas. 1985, 9, 139–164. [Google Scholar] [CrossRef]
- Hauser, R.M.; Warren, J.R. Socioeconomic Indexes for Occupations: A review, Update, and Critique. Sociol. Methodol. 1997, 27, 177–289. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. (Eds.) Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modelling; Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudek, R. Alternative ways of assessing model fit. In Testing Structural Equation Models; Bollen, K.A., Long, J.S., Eds.; Sage: Newbury Park, CA, USA, 1993. [Google Scholar]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Tucker, L.R.; Lewis, C. A reliability coefficient for maximum likelihood factor analysis. Psychometrika 1973, 38, 1–10. [Google Scholar] [CrossRef]
- Byrne, B. Structural Equation Modeling with EQS and EQS/Windows; Sage Publications: London, UK, 1994. [Google Scholar]
- Scott-Lennox, J.A.; Scott-Lennox, R.D. Sex-race differences in social support and depression in older low-income adults. In Structural Equation Modeling: Concepts, Issues, and Applications; Hoyle, R.H., Ed.; SAGE: Thousand Oaks, CA, USA, 1995; pp. 199–216. [Google Scholar]
- Bollen, K.A. Structural Equations with Latent Variables. In Wiley Series in Probability and Mathematical Statistics; John Wiley & Sons, Inc: New York, NY, USA, 1989. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation and Conditional Process Analysis; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Fredrickson, B.L. What good are positive emotions? Rev. Gen. Psychol. 1998, 2, 300–319. [Google Scholar] [CrossRef]
- Fredrickson, B.L. The role of positive emotions in positive psychology: The broaden-and-build theory of positive emotions. Am. Psychol. 2001, 56, 218–226. [Google Scholar] [CrossRef]
- Fredrickson, B.L.; Branigan, C. Positive emotions broaden the scope of attention and thought-action repertories. Cogn. Emot. 2005, 19, 313–332. [Google Scholar] [CrossRef]
- Caprara, G.V.; Caprara, G.; Steca, P. Personality’s correlates of adult development and aging. Eur. Psychol. 2003, 8, 131–147. [Google Scholar] [CrossRef]
- Kuzman, M.R.; Curkovic, M.; Wasserman, D. Principles of mental health care during the COVID-19 pandemic. Eur. Psychiatry 2020, 63, e45. [Google Scholar] [CrossRef] [PubMed]
- McDaid, D. Viewpoint: Investing in strategies to support mental health recovery from the COVID-19 pandemic. Eur. Psychiatry 2021, 64, e32. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total Sample | Early Adulthood | Middle Adulthood | Late Adulthood | ||||
|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | |
| Positivity | 3.72 | 0.67 | 3.64 | 0.71 | 3.78 | 0.62 | 3.79 | 0.61 |
| SE_NEG | 2.94 | 0.70 | 2.89 | 0.68 | 2.99 | 0.75 | 2.97 | 0.68 |
| SE_POS | 3.71 | 0.83 | 3.67 | 0.87 | 3.78 | 0.80 | 3.68 | 0.77 |
| State anxiety | 2.07 | 0.57 | 2.15 | 0.61 | 1.99 | 0.53 | 1.98 | 0.49 |
| Depressive symptoms | 1.72 | 0.58 | 1.85 | 0.60 | 1.61 | 0.53 | 1.58 | 0.51 |
| SE_COVID-19 | 4.07 | 0.61 | 3.99 | 0.61 | 4.11 | 0.61 | 4.24 | 0.55 |
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| 1. Positivity | — | |||||
| 2. SE_NEG | 0.41 *** | — | ||||
| 3. SE_POS | 0.46 *** | 0.36 *** | — | |||
| 4. State Anxiety | −0.52 *** | −0.40 *** | −0.042 *** | — | ||
| 5. Depressive symptoms | −0.52 *** | −0.38 *** | −0.36 *** | 0.70 *** | — | |
| 6. SE_COVID-19 | 0.17 *** | 0.18 *** | 0.27 *** | −0.15 *** | −0.13 *** | — |
| Positivity | SE_NEG | SE_POS | State Anxiety | Depressive Symptoms | SE_COVID-19 | |
|---|---|---|---|---|---|---|
| Gender | −0.02; −0.06; −0.05 | −0.13 ***; −0.11 *; −0.13 * | 0.07 *; 0.03; −0.03 | 0.16 ***; 0.16 ***; 0.10 * | 0.14 ***; 0.14 **; 0.22 *** | 0.05; 0.12 *; 0.06 |
| SES | 0.09 *; 0.10 *; 0.12 * | 0.01; 0.03; −0.05 | −0.03; 0.07; 0.11 * | 0.02; −0.04; −0.04 | −0.02; −0.02; −0.05 | 0.01; 0.03; −0.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thartori, E.; Pastorelli, C.; Cirimele, F.; Remondi, C.; Gerbino, M.; Basili, E.; Favini, A.; Lunetti, C.; Fiasconaro, I.; Caprara, G.V. Exploring the Protective Function of Positivity and Regulatory Emotional Self-Efficacy in Time of Pandemic COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 13171. https://doi.org/10.3390/ijerph182413171
Thartori E, Pastorelli C, Cirimele F, Remondi C, Gerbino M, Basili E, Favini A, Lunetti C, Fiasconaro I, Caprara GV. Exploring the Protective Function of Positivity and Regulatory Emotional Self-Efficacy in Time of Pandemic COVID-19. International Journal of Environmental Research and Public Health. 2021; 18(24):13171. https://doi.org/10.3390/ijerph182413171
Chicago/Turabian StyleThartori, Eriona, Concetta Pastorelli, Flavia Cirimele, Chiara Remondi, Maria Gerbino, Emanuele Basili, Ainzara Favini, Carolina Lunetti, Irene Fiasconaro, and Gian Vittorio Caprara. 2021. "Exploring the Protective Function of Positivity and Regulatory Emotional Self-Efficacy in Time of Pandemic COVID-19" International Journal of Environmental Research and Public Health 18, no. 24: 13171. https://doi.org/10.3390/ijerph182413171