
The Influence of Burnout on Patient Safety Management Activities of Shift Nurses: The Mediating Effect of Compassion Satisfaction


Abstract
:1. Introduction
- -
- Investigating the differences in burnout, CS, and PSMA according to the general and job-related characteristics of nurses;
- -
- Investigating the correlation between burnout, CS, and PSMA of the nurses; and
- -
- Examining the effect of nurses’ burnout on PSMA and the mediating effect of CS between these two variables.
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Instruments
2.3.1. Patient Safety Management Activities
2.3.2. Burnout
2.3.3. Compassion Satisfaction
2.3.4. General and Job-Related Characteristics of Participants
2.4. Ethical Consideration
2.5. Data Collection Method
2.6. Data Analysis
3. Results
3.1. General Characteristics of Participants
3.2. Differences in Burnout, CS, and PSMA According to General and Job-Related Characteristics of Shift-Working Nurses
3.3. Participant’s Burnout, CS, and PSMA Level
3.4. CorrelationsamongBurnout, CS, and PSMA
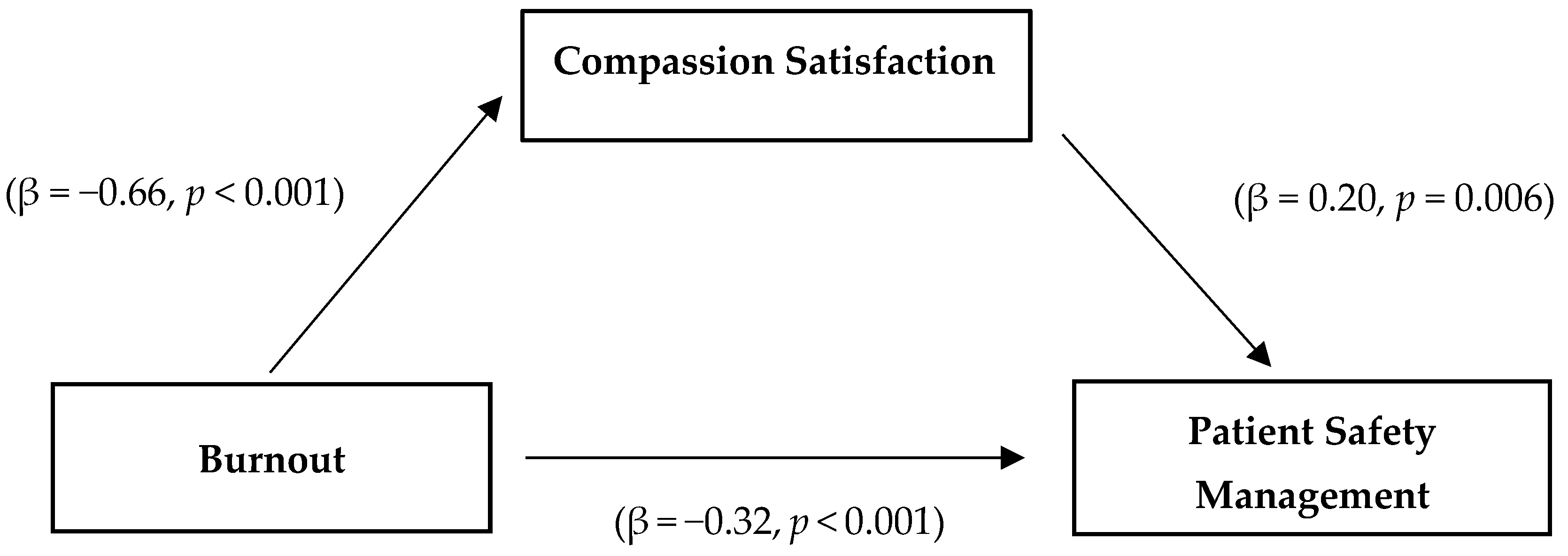
3.5. Mediating Effect of CS on the Relationship between Burnout and PSMA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Consultative Meeting Planning for the Global Patient Safety Challenge: Medication Safety, 19–20 April 2016, WHO Headquarters Geneva, Switzerland: Meeting Report; No. WHO/HIS/SDS/2016.20; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- KOPS. Annual Patient Safety Statistics for 2020. Available online: https://statistics.kops.or.kr/ (accessed on 1 August 2021).
- Kryssie Kunert, M.S.N.; King, M.L.; Kolkhorst, F.W. Fatigue and sleep quality in nurses. J. Psychosoc. Nurs. Ment. Health Serv. 2007, 45, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Germain, A.; Moul, D.E.; Franzen, P.L.; Brar, L.K.; Fletcher, M.E.; Begley, A.; Houck, P.R.; Mazumdar, S.; Reynolds, C.F.; et al. Efficacy of brief behavioral treatment for chronic insomnia in older adults. Arch. Intern. Med. 2011, 171, 887–895. [Google Scholar] [CrossRef]
- Jung, Y.J.; Kang, S.W. Differences in sleep, fatigue, and neurocognitive function between shift nurses and non-shift nurses. Korean J. Adult Nurs. 2017, 29, 190–199. [Google Scholar] [CrossRef] [Green Version]
- Dall’Ora, C.; Ball, J.; Reinius, M.; Griffiths, P. Burnout in nursing: A theoretical review. Hum. Resour. Health 2020, 18, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.K.; Gandrakota, N.; Cimiotti, J.P.; Ghose, N.; Moore, M.; Ali, M.K. Prevalence of and factors associated with nurse burnout in the US. JAMA Netw. Open 2021, 4, e2036469. [Google Scholar] [CrossRef]
- Bagheri Hosseinabadi, M.; Ebrahimi, M.H.; Khanjani, N.; Biganeh, J.; Mohammadi, S.; Abdolahfard, M. The effects of amplitude and stability of circadian rhythm and occupational stress on burnout syndrome and job dissatisfaction among irregular shift working nurses. J. Clin. Nurs. 2019, 28, 1868–1878. [Google Scholar] [CrossRef]
- Hunsaker, S.; Chen, H.C.; Maughan, D.; Heaston, S. Factors that influence the development of compassion fatigue, burnout, and compassion satisfaction in emergency department nurses. J. Nurs. Scholarsh. 2015, 47, 186–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacPhee, M.; Dahinten, V.S.; Havaei, F. The Impact of heavy perceived nurse workloads on patient and nurse outcomes. Adm. Sci. 2017, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Garcia, C.D.L.; Abreu, L.C.D.; Ramos, J.L.S.; Castro, C.F.D.D.; Smiderle, F.R.N.; Santos, J.A.D.; Bezerra, I.M.P. Influence of burnout on patient safety: Systematic review and meta-analysis. Medicina 2019, 55, 553. [Google Scholar] [CrossRef] [Green Version]
- Stamm, B.H. The Concise ProQOL Manual. 2010. Available online: http://proqol.org (accessed on 6 July 2021).
- Burtson, P.L.; Stichler, J.F. Nursing work environment and nurse caring: Relationship among motivational factors. J. Adv. Nurs. 2010, 66, 1819–1831. [Google Scholar] [CrossRef]
- Lee, J.M.; Yom, Y.H. Effects of work stress, compassion fatigue, and compassion satisfaction on burnout in clinical nurses. J. Korean Acad. Nurs. Adm. 2013, 19, 689–697. [Google Scholar] [CrossRef]
- Jun, Y.J.; Sung, M.H. Effects of traumatic events, compassion fatigue, self-esteem, and compassion satisfaction on burnout of nurses in emergency department (ED). Korean J. Occup. Health Nurs. 2014, 23, 80–88. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.N.; Kim, J.A. Analysis of research on compassion satisfaction among nurses. J. Korea Acad.-Ind. Coop. Soc. 2016, 17, 599–609. Available online: https://www.dbpia.co.kr/Journal/articleDetail?nodeId=NODE07200229 (accessed on 1 May 2020).
- Jang, Y.M.; Kim, S.Y. Coping strategies, compassion fatigue and compassion satisfaction among nurses in emergency room. J. Korean Clin. Nurs. Res. 2014, 20, 348–358. [Google Scholar] [CrossRef]
- Lee, S.S.; Choi, H.R. Convergence influences of nurses’ professional autonomy and empathy on patient safety culture. J. Converg. Inf. Technol. 2019, 17, 231–241. [Google Scholar] [CrossRef]
- Jang, H.M.; Park, J.Y.; Choi, Y.J.; Park, S.W.; Lim, H.N. Effect of general hospital nurses’ perception of patient safety culture and burnout on safety management activities. J. Korean Acad. Nurs. Adm. 2016, 22, 239–250. [Google Scholar] [CrossRef]
- Chu, M.S. The lived experience of newly employed nurses: A phenomenological study. Nurs. Sci. 2000, 12, 17–25. [Google Scholar]
- Lee, G.O. The Study on Nurse Manager Leadership and Patient Safety-Related Nursing Activities. Master’s Thesis, Kyung-Hee University, Seoul, Korea, 2009. [Google Scholar]
- Figley, C.R. (Ed.) Compassion Fatigue: Coping with Secondary Traumatic Stress in Those Who Treat the Traumatized; Brunner/Mazel Publishers: New York, NY, USA, 1995. [Google Scholar]
- Levine, D.M.; Stephan, D. Even You Can Learn Statistics and Analytics: An Easy to Understand Guide to Statistics and Analytics, 3rd ed.; Pearson FT Press: New Jersey, NJ, USA, 2014. [Google Scholar]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Abu-Bader, S.; Jones, T.V. Statistical mediation analysis using the sobel test and hayes SPSS process macro. Int. J. Quantit. Qualit. Res. Method 2021, 9, 42–61. [Google Scholar]
- Kim, M.K.; Lee, S.M. The causal relationships among staff nurses’ job stress factors, patient safety culture perception and patient safety management activities in a university hospital. J. Korean Acad. Nurs. Adm. 2019, 25, 340–352. [Google Scholar] [CrossRef]
- Bae, H.J.; Kim, J.E.; Bae, Y.H.; Kim, H.J. Factors associated with patient safety care activity among nurses in small-medium sized general hospitals. J. Korea Acad.-Ind. Coop. Soc. 2019, 20, 118–127. [Google Scholar] [CrossRef]
- Son, Y.L. The impact of perceived patient safety culture on safety care activities in general hospital nurse’s. J. Korea Acad.-Ind. Coop. Soc. 2016, 17, 509–517. [Google Scholar] [CrossRef] [Green Version]
- Korea Institute for Healthcare Accreditation. Korea 2020 Patient Safety Statistical Yearbook 2021. Available online: http://statistics.kops.or.kr (accessed on 28 May 2021).
- Teng, C.I.; Dai, Y.T.; Lotus Shyu, Y.I.; Wong, M.K.; Chu, T.L.; Tsai, Y.H. Professional commitment, patient safety, and patient-perceived care quality. J. Nurs. Scholarsh. 2009, 41, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J. Patient Safety Culture and Management Activities Perceived by Hospital Nurses. Master’s Thesis, Eulji University, Daejeon, Korea, 2011. [Google Scholar]
- Scott, L.D.; Rogers, A.E.; Hwang, W.T.; Zhang, Y. Effects of critical care nurses’ work hours on vigilance and patients’ safety. Am. J. Crit. Care 2006, 15, 30–37. [Google Scholar] [CrossRef]
- Han, M.Y.; Lee, M.S.; Bae, J.Y.; Kim, Y.S. Effects of nursing practice environment, compassion fatigue and compassion satisfaction on burnout in clinical nurses. J. Korean Acad. Nurs. Adm. 2015, 21, 193–202. [Google Scholar] [CrossRef]
- Duarte, J.; Pinto-Gouveia, J.; Cruz, B. Relationships between nurses’ empathy, self-compassion and dimensions of professional quality of life: A cross-sectional study. Int. J. Nurs. Stud. 2016, 60, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells-English, D.; Giese, J.; Price, J. Compassion fatigue and satisfaction: Influence on turnover among oncology nurses at an urban cancer center. Clin. J. Oncol. Nurs. 2019, 23, 487–493. [Google Scholar] [CrossRef]
- Jakimowicz, S.; Perry, L.; Lewis, J. Compassion satisfaction and fatigue: A cross-sectional survey of Australian intensive care nurses. Aust. Crit. Care 2018, 31, 396–405. [Google Scholar] [CrossRef]
- Yun, J.I.; Son, H.M. Mediating effects of burnout between time pressure and safety care activities of nurses. J. Korean Acad. Nurs. Adm. 2019, 25, 248–257. [Google Scholar] [CrossRef]
- Hong, K.J.; Cho, S.H. Comparison of nursing workforce supply and employment in south Korea and other OECD countries. Perspect. Nurs. Sci. 2017, 14, 55–63. [Google Scholar] [CrossRef] [Green Version]
- Jung, M.R.; Jeong, E. Effect of professional quality of life and vitality on work-life balance of clinical nurses. J. Korean Soc. Wellness 2019, 14, 11–20. [Google Scholar] [CrossRef]
- Day, H. The meaning of compassion. Br. J. Nurs. 2015, 24, 342–343. [Google Scholar] [CrossRef]
- Kim, H.J.; Yom, Y.H. Structural equation modeling on burnout in clinical nurses based on CS-CF Model. J. Korean Acad. Nurs. 2014, 44, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Freudenberger, H.J. Staff burn-out. J. Soc. Issues 1974, 30, 159–165. [Google Scholar] [CrossRef]
- Leiter, M.P. Burnout as a developmental process: Consideration of models. In Professional Burnout: Recent Developments in Theory and Research; CRC Press: New York, NY, USA, 2018; pp. 237–250. Available online: https://www.taylorfrancis.com/chapters/edit/10.1201/9780203741825-18/burnout-developmental-process-consideration-models-michael-leiter (accessed on 16 July 2020).
- Lee, S.Y. Understanding and management of burnout. J. Korean Neuropsychiatr. Assoc. 2020, 59, 105–114. [Google Scholar] [CrossRef]
- Zhang, Y.Y.; Zhang, C.; Han, X.R.; Li, W.; Wang, Y.L. Determinants of compassion satisfaction, compassion fatigue and burn out in nursing: A correlative meta-analysis. Medicine 2018, 97, e11086. [Google Scholar] [CrossRef]
- Hinderer, K.A.; VonRueden, K.T.; Friedmann, E.; McQuillan, K.A.; Gilmore, R.; Kramer, B.; Murray, M. Burnout, compassion fatigue, compassion satisfaction, and secondary traumatic stress in trauma nurses. J. Trauma Nurs. 2014, 21, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Laschinger, H.K.S.; Leiter, M.P. The impact of nursing work environments on patient safety outcomes: The mediating role of burnout engagement. J. Nurs. Adm. 2006, 36, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, Y.; Miyoshi, T.; Hagiya, H.; Kosaki, Y.; Otsuka, F. Burnout of healthcare workers amid the covid-19 pandemic: A Japanese cross-sectional survey. Int. J. Environ. Res. Public Health 2021, 18, 2434. [Google Scholar] [CrossRef]
- Ruiz-Fernández, M.D.; Ramos-Pichardo, J.D.; Ibáñez-Masero, O.; Cabrera-Troya, J.; Carmona-Rega, M.I.; Ortega-Galán, Á.M. Compassion fatigue, burnout, compassion satisfaction and perceived stress in healthcare professionals during the COVID-19 health crisis in Spain. J. Clin. Nurs. 2020, 29, 4321–4330. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Categories | n (%) | Burnout | CS | PSMA | |||
|---|---|---|---|---|---|---|---|---|
| M ± SD | t/F (p) Tukey | M ± SD | t/F (p) Tukey | M ± SD | t/F (p) Tukey | |||
| Age (year) | <25 | 85 (28.2) | 2.94 ± 0.56 | 0.61 (0.545) | 2.91 ± 0.67 | 1.30 (0.274) | 4.02 ± 0.56 | 0.12 (0.885) |
| 25–<30 | 120 (39.9) | 3.02 ± 0.50 | 2.93 ± 0.67 | 3.98 ± 0.59 | ||||
| ≥30 | 96 (31.9) | 3.00 ± 0.49 | 3.05 ± 0.66 | 4.00 ± 0.49 | ||||
| Gender | Male | 18 (6.0) | 2.80 ± 0.64 | −1.61 (0.109) | 3.02 ± 0.72 | 0.37 (0.713) | 4.21 ± 0.63 | 1.71 (0.089) |
| Female | 283 (94.0) | 3.00 ± 0.51 | 2.96 ± 0.65 | 3.98 ± 0.54 | ||||
| Marital status | Single | 238 (79.1) | 3.00 ± 0.53 | 0.80 (0.425) | 2.92 ± 0.65 | −2.38 (0.018) | 3.99 ± 0.57 | −0.32 (0.753) |
| Married | 63 (20.9) | 2.94 ± 0.47 | 3.13 ± 0.65 | 4.02 ± 0.48 | ||||
| Religion | No | 182 (60.5) | 3.04 ± 0.52 | 2.00 (0.047) | 2.87 ± 0.65 | −3.08 (0.002) | 3.96 ± 0.55 | −1.63 (0.104) |
| Yes | 119 (39.5) | 2.92 ± 0.50 | 3.10 ± 0.65 | 4.06 ± 0.54 | ||||
| Education | Diploma a | 123 (40.9) | 3.05 ± 0.48 | 3.14 (0.045) c < a | 2.87 ± 0.63 | 3.39 (0.035) a < c | 3.94 ± 0.56 | 0.89 (0.413) |
| Bachelor b | 174 (57.8) | 2.96 ± 0.53 | 3.00 ± 0.67 | 4.03 ± 0.54 | ||||
| ≥Masters c | 4 (1.3) | 2.50 ± 0.14 | 3.60 ± 0.50 | 4.13 ± 0.30 | ||||
| Regular exercise | No | 129 (42.9) | 3.13 ± 0.53 | 3.41 (0.001) | 2.88 ± 0.65 | −1.97 (0.050) | 3.91 ± 0.51 | −2.36 (0.019) |
| Yes | 172 (57.1) | 2.91 ± 0.48 | 3.03 ± 0.65 | 4.06 ± 0.57 | ||||
| Subjective health status * | Good a | 80 (26.6) | 2.77 ± 0.45 | 10.96 (<0.001) a < b,c | 3.12 ± 0.71 | 3.61 (0.028) n/a | 4.12 ± 0.57 | 2.73 (0.067) |
| Moderate b | 192 (63.8) | 3.06 ± 0.53 | 2.89 ± 0.60 | 3.95 ± 0.53 | ||||
| Poor c | 29 (9.6) | 3.14 ± 0.44 | 3.01 ± 0.76 | 3.95 ± 0.55 | ||||
| Clinical Experience (year) | <2 | 116 (38.5) | 2.95 ± 0.56 | 0.59 (0.555) | 2.87 ± 0.62 | 1.93 (0.171) | 4.04 ± 0.56 | 0.52 (0.593) |
| 2~<5 | 79 (26.2) | 3.02 ± 0.49 | 3.02 ± 0.70 | 3.96 ± 0.58 | ||||
| ≥5 | 106 (35.2) | 3.01 ± 0.49 | 3.02 ± 0.66 | 3.98 ± 0.51 | ||||
| Position | Staff nurse | 288 (95.7) | 2.99 ± 0.51 | 0.69 (0.490) | 2.95 ± 0.64 | −2.05 (0.042) | 4.00 ± 0.54 | 0.21 (0.832) |
| Charge nurse | 13 (4.3) | 2.89 ± 0.71 | 3.32 ± 0.83 | 3.97 ± 0.65 | ||||
| Working unit * | Medical ward a | 91 (30.2) | 3.15 ± 0.52 | 3.13 (0.009) d < a | 2.86 ± 0.69 | 0.91 (0.472) | 3.96 ± 0.61 | 1.47 (0.210) |
| Surgical ward b | 80 (26.6) | 2.98 ± 0.57 | 2.95 ± 0.74 | 3.98 ± 0.57 | ||||
| ICU c | 33 (11.0) | 2.94 ± 0.44 | 3.00 ± 0.56 | 4.24 ± 0.46 | ||||
| ED d | 33 (11.0) | 2.79 ± 0.51 | 3.10 ± 0.65 | 3.98 ± 0.47 | ||||
| Ped ward/DR | 37 (12.3) | 2.94 ± 0.44 | 3.06 ± 0.51 | 4.00 ± 0.48 | ||||
| etc. | 27 (9.0) | 2.88 ± 0.42 | 2.99 ± 0.66 | 3.93 ± 0.50 | ||||
| Number of night duties (Monthly) | ≤ 6 | 102 (22.9) | 2.96 ± 0.60 | 0.44 (0.727) | 2.97 ± 0.73 | 0.66 (0.580) | 3.96 ± 0.59 | 0.48 (0.700) |
| 7~8 | 140 (49.8) | 3.00 ± 0.52 | 2.923 ± 0.67 | 4.04 ± 0.53 | ||||
| ≥ 9 | 49 (16.3) | 3.01 ± 0.50 | 3.07 ± 0.72 | 3.96 ± 0.52 | ||||
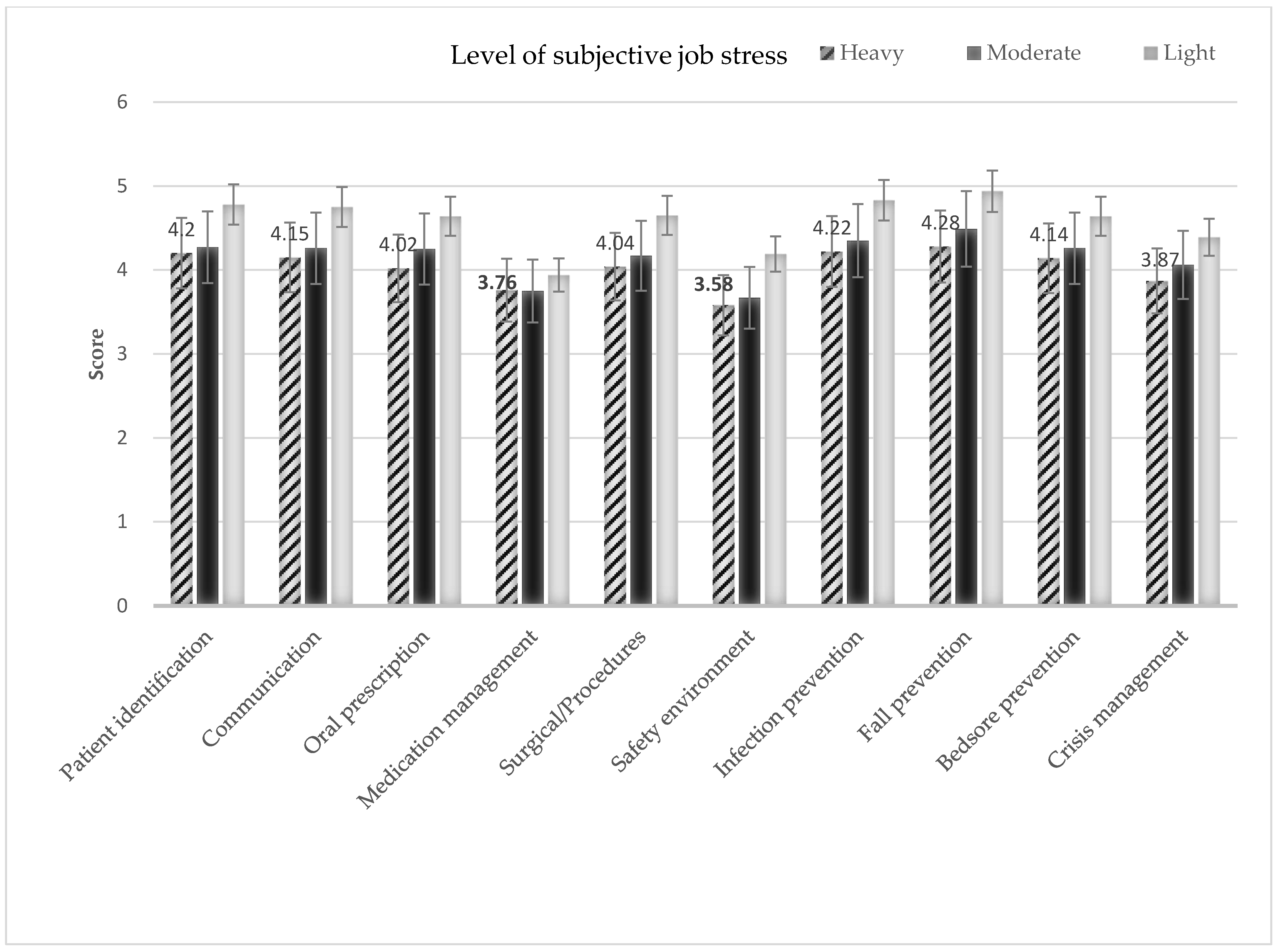
| Subjective job stress * | Heavy a | 198 (65.8) | 3.13 ± 0.51 | 28.67 (<0.001) c < b< a | 2.88 ± 0.68 | 5.13 (0.006) n/a | 3.94 ± 0.55 | 6.01 (0.003) a,b < c |
| Moderate b | 91 (30.2) | 2.77 ± 0.37 | 3.10 ± 0.60 | 4.06 ± 0.55 | ||||
| Light c | 12 (4.0) | 2.36 ± 0.54 | 3.27 ± 0.36 | 4,45 ± 0.32 | ||||
| Variables (Item Range) | M ± SD | Range |
|---|---|---|
| Min−Max | ||
| Burnout (10−50) | 29.89 ± 5.16 | 12–49 |
| CS (10−50) | 29.61 ± 6.55 | 11–50 |
| PSMA (46−230) | 183.92 ± 25.22 | 108–230 |
| Variables | Burnout r (p) | CS r (p) | PSMA r (p) |
|---|---|---|---|
| Burnout | 1 | ||
| CS | −0.66 (<0.001) | 1 | |
| PSMA | −0.32 (<0.001) | 0.32 (<0.001) | 1 |
| Variables | B (SE) | β | t (p) | R2 (Adj.R2) | F (p) |
|---|---|---|---|---|---|
| Step 1. Burnout → CS | −0.84 (0.055) | −0.66 | −15.16 (<0.001) | 0.43 (0.43) | 229.66 (<0.001) |
| Step 2. Burnout → PSMA | −0.34 (0.058) | −0.32 | −5.74 (<0.001) | 0.10 (0.10) | 32.94 (<0.001) |
| Step 3. Burnout, CS → PSMA | |||||
| Burnout → PSMA | −0.20 (0.077) | −0.18 | −2.55 (0.011) | 0.11 (0.12) | 20.64 (<0.001) |
| CS → PSMA+ | 0.17 (0.060) | 0.20 | 2.76 (0.006) | ||
| Sobel test: Z = −3.21, p = 0.001 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryu, I.S.; Shim, J. The Influence of Burnout on Patient Safety Management Activities of Shift Nurses: The Mediating Effect of Compassion Satisfaction. Int. J. Environ. Res. Public Health 2021, 18, 12210. https://doi.org/10.3390/ijerph182212210
Ryu IS, Shim J. The Influence of Burnout on Patient Safety Management Activities of Shift Nurses: The Mediating Effect of Compassion Satisfaction. International Journal of Environmental Research and Public Health. 2021; 18(22):12210. https://doi.org/10.3390/ijerph182212210
Chicago/Turabian StyleRyu, I Seul, and JaeLan Shim. 2021. "The Influence of Burnout on Patient Safety Management Activities of Shift Nurses: The Mediating Effect of Compassion Satisfaction" International Journal of Environmental Research and Public Health 18, no. 22: 12210. https://doi.org/10.3390/ijerph182212210