
Peer Support and Overdose Prevention Responses: A Systematic ‘State-of-the-Art’ Review

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy and Selection Criteria
2.3. Quality Assessment
2.4. Data Analysis
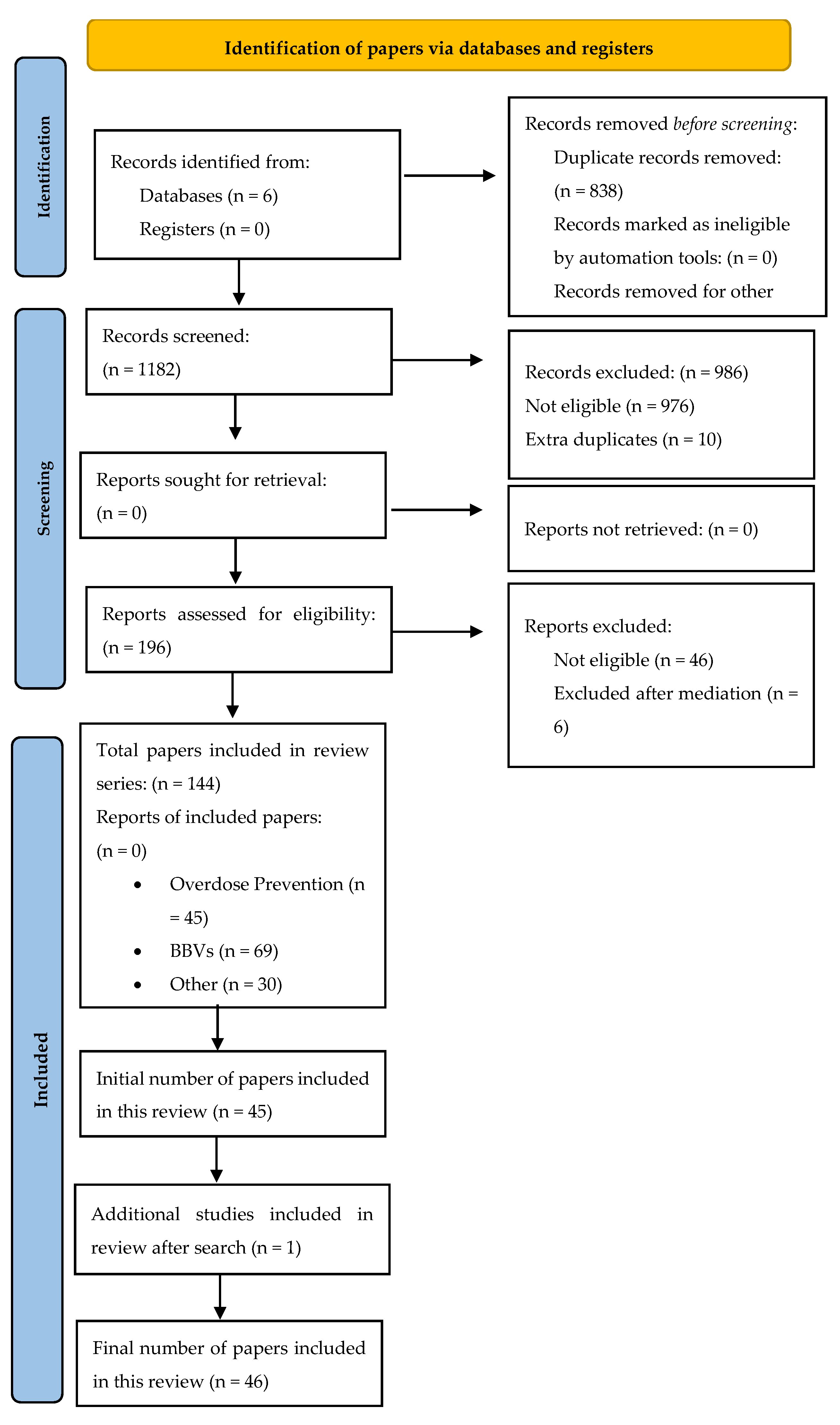
2.5. Identification of Relevant Papers
2.6. Characteristics of Included Papers
2.7. Overview of the Included Reviews: Primary Focus
3. Results
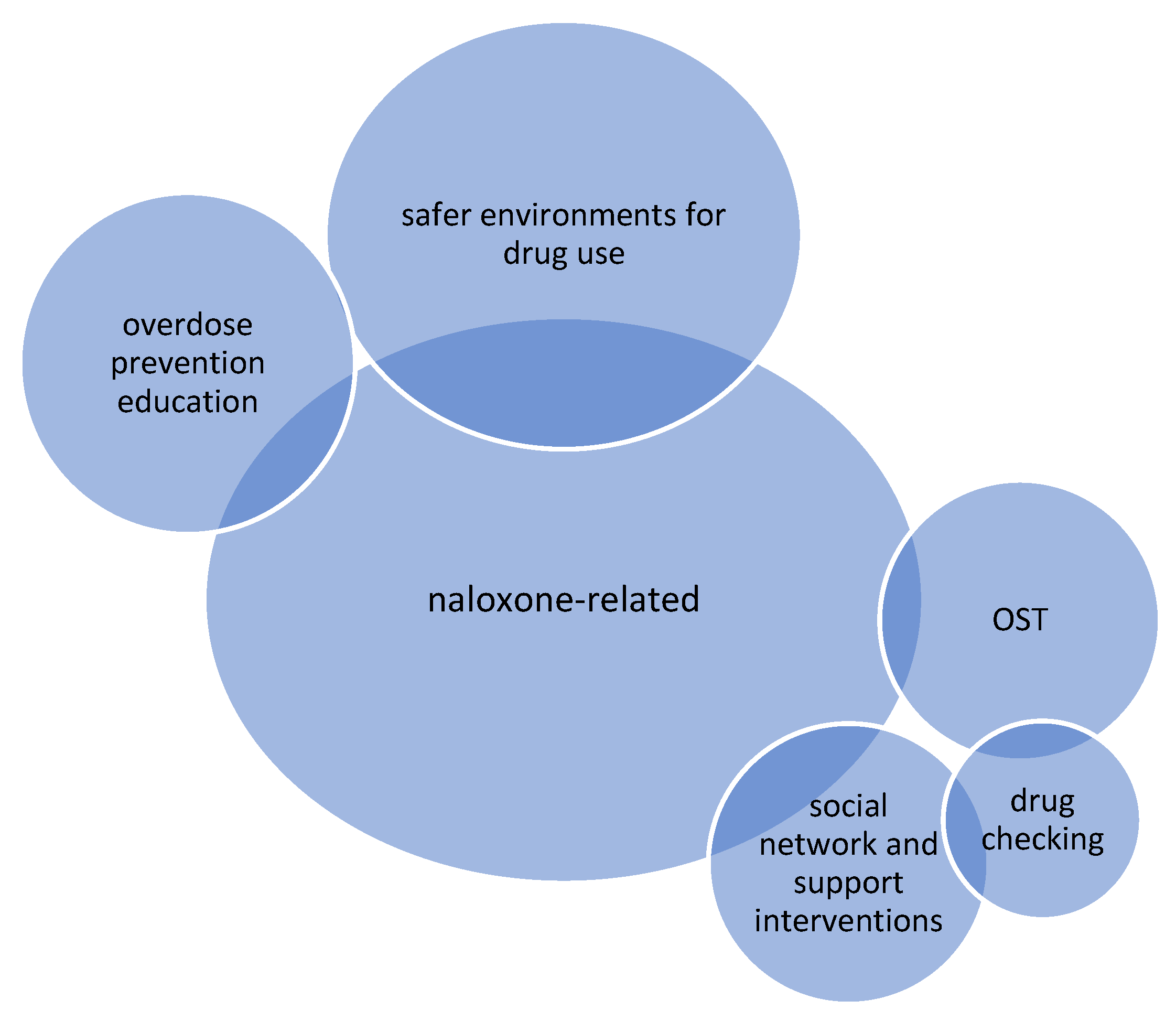
3.1. Naloxone-Related Interventions
3.1.1. PWUD Engaged and Committed to Peer-Involved Naloxone Interventions
3.1.2. Benefits for the Naloxone Administrator
3.1.3. Naloxone and Expanding Community Level Harm Reduction
3.1.4. Barriers to Naloxone Use
3.1.5. Implications of Naloxone Intervention
3.2. Safer Environments for Drug Use
3.2.1. The Role of Peers in the Social Dynamics of Safer Environments for Drug Use
3.2.2. A Trusted Environment Created by Peers
3.2.3. Benefits for Peer Workers in Safer Environments for Drug Use
3.2.4. Challenges for Peer Workers in Safer Environments for Drug Use
3.3. Overdose Prevention Education
3.4. Opioid Substitution Treatment (OST)
3.5. Drug Checking
3.6. Social Networks and Support Interventions
4. Discussion
4.1. Implications for Policy, Practice, and Research
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BBV | Blood Borne Virus |
| CPR | Cardiopulmonary resuscitation |
| DRDs | Drug-related deaths |
| ED | Emergency Department |
| HAT | Heroin Assisted Treatment |
| HCV | Hepatitis C Virus |
| HIV | Human Immunodeficiency Virus |
| NSP | Needle and Syringe Programmes |
| OEND | Overdose Education and Naloxone Distribution |
| OST | Opioid Substitution Treatment |
| OPS | Overdose Prevention Site |
| PRISMA | Preferred Reporting Items of Systematic Reviews and Meta-Analyses |
| PICOS Framework | Populations, interventions, comparators, outcomes and study designs framework for systematic review of literature |
| PWUD | People Who Use Drugs |
| SCS | Supervised Consumption Site |
| RCT | Randomized Controlled Trial |
| THN | Take-Home Naloxone |
| UK | United Kingdom |
| US | United States |
| VANDU | Vancouver Area Network of Drug Users |
References
- The European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). Eur. Drug Rep. 2017. Available online: https://www.emcdda.europa.eu/publications/edr/trends-developments/2021_en (accessed on 12 August 2021).
- Greer, A.; Ritter, A. The legal regulation of drugs and role of government: Perspectives from people who use drugs. Drug Alcohol Depend. 2019, 206, 107737. [Google Scholar] [CrossRef]
- Imtiaz, S.; Shield, K.D.; Fischer, B.; Elton-Marshall, T.; Sornpaisarn, B.; Probst, C.; Rehm, J. Recent changes in trends of opioid overdose deaths in North America. Subst. Abus. Treat. Prev. Policy 2020, 15, 1–9. [Google Scholar] [CrossRef]
- Rehm, J.; Probst, C. Decreases of life expectancy despite decreases in non-communicable disease mortality: The role of substance use and socioeconomic status. Eur. Addict. Res. 2018, 24, 53–59. [Google Scholar] [CrossRef]
- Henry, B. Stopping the Harm: Decriminalization of People Who Use Drugs in BC; Office of the Provincial Health Officer: Victoria, BC, Canada, 2019. Available online: https://www2.gov.bc.ca/assets/gov/health/about-bc-s-health-care-system/office-of-the-provincial-health-officer/reports-publications/special-reports/stopping-the-harm-report.pdf (accessed on 9 July 2021).
- The European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). Drug-Related Deaths and Mortality in Europe. Update from the EMCDDA Expert Network. 2021. Available online: https://www.emcdda.europa.eu/publications/technical-reports/drug-related-deaths-and-mortality-europe_en (accessed on 23 August 2021).
- Irvine, M.A.; Kuo, M.; Buxton, J.A.; Balshaw, R.; Otterstatter, M.; Macdougall, L.; Gilbert, M. Modelling the combined impact of interventions in averting deaths during a synthetic-opioid overdose epidemic. Addiction 2019, 114, 1602–1613. [Google Scholar] [CrossRef]
- Richert, T. Wasted, overdosed, or beyond saving—To act or not to act? Heroin users’ views, assessments, and responses to witnessed overdoses in Malmö, Sweden. Int. J. Drug. Pol. 2015, 26, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Baptiste-Roberts, K.; Hossain, M. Socioeconomic Disparities and Self-reported Substance Abuse-related Problems. Addict. Health 2018, 10, 112–122. [Google Scholar] [CrossRef]
- Krawczyk, N.; Feder, K.A.; Saloner, B.; Crum, R.M.; Kealhofer, M.; Mojtabai, R. The association of psychiatric comorbidity with treatment completion among clients admitted to substance use treatment programs in a U.S. national sample. Drug Alcohol Depend. 2017, 175, 157–163. [Google Scholar] [CrossRef] [PubMed]
- DeBeck, K.; Cheng, T.; Montaner, J.S.; Beyrer, C.; Elliott, R.; Sherman, S.; Baral, S. HIV and the criminalisation of drug use among people who inject drugs: A systematic review. Lancet HIV 2017, 4, e357–e374. [Google Scholar] [CrossRef]
- Harm reduction: An approach to reducing risky health behaviours in adolescents. Paediatr. Child Health 2008, 13, 53–56. [CrossRef] [Green Version]
- United Nations Office on Drugs and Crime (UNODC). Reducing the Harm of Drug Use and Dependence. 2007. Available online: https://www.unodc.org/docs/treatment/Reducing_the_Adverse_Health_and_Social_Consequences_of_Abuse.pdf (accessed on 12 July 2021).
- International Harm Reduction Association. What is Harm Reduction? 2021. Available online: https://www.hri.global/what-is-harm-reduction (accessed on 9 July 2021).
- Holloway, K.; Hills, R.; May, T. Fatal and non-fatal overdose among opiate users in South Wales: A qualitative study of peer responses. Int. J. Drug Pol. 2018, 56, 56–63. [Google Scholar] [CrossRef]
- Marshall, Z.; Dechman, M.K.; Minichiello, A.; Alcock, L.; Harris, G.E. Peering into the literature: A systematic review of the roles of people who inject drugs in harm reduction initiatives. Drug Alcohol Depend. 2015, 151, 1–14. [Google Scholar] [CrossRef]
- Boucher, L.M.; Marshall, Z.; Martin, A.; Larose-Hébert, K.; Flynn, J.V.; LaLonde, C.; Pineau, D.; Bigelow, J.; Rose, T.; Chase, R.; et al. Expanding conceptualizations of harm reduction: Results from a qualitative community-based participatory research study with people who inject drugs. Harm Reduct. J. 2017, 14, 18. [Google Scholar] [CrossRef] [PubMed]
- Foreman-Mackey, A.; Bayoumi, A.M.; Miskovic, M.; Kolla, G.; Strike, C. ‘It’s our safe sanctuary’: Experiences of using an unsanctioned overdose prevention site in Toronto, Ontario. Int. J. Drug Policy 2019, 73, 135–140. [Google Scholar] [CrossRef]
- Friedman, S.R.; Pouget, E.R.; Sandoval, M.; Jones, Y.; Nikolopoulos, G.K.; Mateu-Gelabert, P. Measuring Altruistic and Solidaristic Orientations Toward Others Among People Who Inject Drugs. J. Addict. Dis. 2015, 34, 248–254. [Google Scholar] [CrossRef] [Green Version]
- Harris, M.; Rhodes, T. Methadone diversion as a protective strategy: The harm reduction potential of ‘generous constraints’. Int. J. Drug Policy 2013, 24, e43–e50. [Google Scholar] [CrossRef]
- Bardwell, G.; Kerr, T.; Boyd, J.; McNeil, R. Characterizing peer roles in an overdose crisis: Preferences for peer workers in overdose response programs in emergency shelters. Drug Alcohol Depend. 2018, 190, 6–8. [Google Scholar] [CrossRef] [PubMed]
- Greer, A.; Buxton, J.A.; Pauly, B.; Bungay, V. Organizational support for frontline harm reduction and systems navigation work among workers with living and lived experience: Qualitative findings from British Columbia, Canada. Harm Reduct. J. 2021, 18, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Pauly, B.; Wallace, B.; Pagan, F.; Phillips, J.; Wilson, M.; Hobbs, H.; Connolly, J. Impact of overdose prevention sites during a public health emergency in Victoria, Canada. PLoS ONE 2020, 15, e0229208. [Google Scholar] [CrossRef]
- Mamdani, Z.; McKenzie, S.; Pauly, B.; Cameron, F.; Conway-Brown, J.; Edwards, D.; Howell, A.; Scott, T.; Seguin, R.; Woodrow, P.; et al. “Running myself ragged”: Stressors faced by peer workers in overdose response settings. Harm Reduct. J. 2021, 18, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Winstanley, E.L. The Bell Tolls for Thee & Thine: Compassion Fatigue & the Overdose Epidemic. Int. J. Drug Policy 2020, 85, 102796. [Google Scholar] [CrossRef] [PubMed]
- Wagner, K.D.; Davidson, P.J.; Iverson, E.; Washburn, R.; Burke, E.; Kral, A.H.; McNeeley, M.; Bloom, J.J.; Lankenau, S.E. “I felt like a superhero”: The experience of responding to drug overdose among individuals trained in overdose prevention. Int. J. Drug Policy 2013, 25, 157–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holloway, K.R.; Bennett, T.H.; Hills, R. Non-fatal overdose among opiate users in Wales: A national survey. J. Subst. Use 2016, 21, 471–477. [Google Scholar] [CrossRef]
- Parkin, S.; Coomber, R. Public injecting drug use and the social production of harmful practice in high-rise tower blocks (London, UK): A Lefebvrian analysis. Health Place 2011, 17, 717–726. [Google Scholar] [CrossRef]
- Parkin, S. Habitus and Drug Using Environments: Health, Place and Lived-Experience; Routledge: Oxfordshire, UK, 2013; ISBN 978–1–4094–6493–8. [Google Scholar]
- Bennett, T.; Holloway, K. The impact of take-home naloxone distribution and training on opiate overdose knowledge and response: An evaluation of the THN Project in Wales. Drugs: Educ. Prev. Policy 2012, 19, 320–328. [Google Scholar] [CrossRef]
- Rome, A.; Boyle, K. Reducing Drug Users’ Risk of Overdose. The Scottish Government. 2008. Available online: https://lx.iriss.org.uk/sites/default/files/resources/reducing%20drug%20user.pdf (accessed on 15 June 2021).
- Kennedy, M.C.; Boyd, J.; Mayer, S.; Collins, A.; Kerr, T.; McNeil, R. Peer worker involvement in low-threshold supervised consumption facilities in the context of an overdose epidemic in Vancouver, Canada. Soc. Sci. Med. 2019, 225, 60–68. [Google Scholar] [CrossRef]
- Marshall, C.; Perreault, M.; Archambault, L.; Milton, D. Experiences of peer-trainers in a take-home naloxone program: Results from a qualitative study. Int. J. Drug Policy 2017, 41, 19–28. [Google Scholar] [CrossRef]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef] [PubMed]
- Miler, J.A.; Carver, H.; Foster, R.; Parkes, T. Provision of peer support at the intersection of homelessness and problem substance use services: A systematic ‘state of the art’ review. BMC Public Health 2020, 20, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Snilstveit, B.; Oliver, S.; Vojtkova, M. Narrative approaches to systematic review and synthesis of evidence for international development policy and practice. J. Dev. Eff. 2012, 4, 409–429. [Google Scholar] [CrossRef]
- Ray, L.A.; Bujarski, S.; Grodin, E.; Hartwell, E.; Green, R.; Venegas, A.; Lim, A.C.; Gillis, A.; Miotto, K. State-of-the-art behavioral and pharmacological treatments for alcohol use disorder. Am. J. Drug Alcohol Abus. 2018, 45, 124–140. [Google Scholar] [CrossRef] [PubMed]
- Brand, P.; Li, S.; White, M. Young People’s Statistics from the National Drug Treatment Monitoring System (NDTMS): 1 April 2016 to 31 March 2017. Public Health England. 2017. Available online: https://www.basw.co.uk/system/files/resources/basw_64456-7.pdf (accessed on 7 June 2021).
- Boyatzis, R.E. Transforming Qualitative Information: Thematic Analysis and Code Development; SAGE Publications Ltd.: Thousand Oaks, CA, USA; Case Western Reserve University: Cleveland, OH, USA, 1998; ISBN 9780761909613. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. ResPsychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Bennett, A.S.; Bell, A.; Tomedi, L.; Hulsey, E.G.; Kral, A.H. Characteristics of an Overdose Prevention, Response, and Naloxone Distribution Program in Pittsburgh and Allegheny County, Pennsylvania. J. Hered. 2011, 88, 1020–1030. [Google Scholar] [CrossRef] [Green Version]
- Waye, K.M.; Goyer, J.; Dettor, D.; Mahoney, L.; Samuels, E.A.; Yedinak, J.; Marshall, B.D. Implementing peer recovery services for overdose prevention in Rhode Island: An examination of two outreach-based approaches. Addict. Behav. 2018, 89, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Piper, T.M.; Stancliff, S.; Rudenstine, S.; Sherman, S.; Nandi, V.; Clear, A.; Galea, S. Evaluation of a Naloxone Distribution and Administration Program in New York City. Subst. Use Misuse 2008, 43, 858–870. [Google Scholar] [CrossRef] [PubMed]
- Wagner, K.D.; Valente, T.W.; Casanova, M.; Partovi, S.M.; Mendenhall, B.M.; Hundley, J.H.; Gonzalez, M.; Unger, J. Evaluation of an overdose prevention and response training programme for injection drug users in the Skid Row area of Los Angeles, CA. Int. J. Drug Policy 2010, 21, 186–193. [Google Scholar] [CrossRef] [Green Version]
- Welch, A.E.; Jeffers, A.; Allen, B.; Paone, D.; Kunins, H.V. Relay: A Peer-Delivered Emergency Department-Based Response to Nonfatal Opioid Overdose. Am. J. Public Health 2019, 109, 1392–1395. [Google Scholar] [CrossRef]
- Winhusen, T.; Wilder, C.; Lyons, M.S.; Theobald, J.; Kropp, F.; Lewis, D. Evaluation of a personally-tailored opioid overdose prevention education and naloxone distribution intervention to promote harm reduction and treatment readiness in individuals actively using illicit opioids. Drug Alcohol Depend. 2020, 216, 108265. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, M.; Hashimi, S.; Tsai, K.; Lampkin, H.; Jozaghi, E. Back to the core: A network approach to bolster harm reduction among persons who inject drugs. Int. J. Drug Policy 2018, 51, 95–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elkhalifa, S.; Jozaghi, E.; Marsh, S.; Thomson, E.; Gregg, D.; Buxton, J.; Jolly, A. Social network support and harm reduction activities in a peer researcher-led pilot study, British Columbia, Canada. Harm Reduct. J. 2020, 17, 1–11. [Google Scholar] [CrossRef]
- Galea, S.; Worthington, N.; Piper, T.M.; Nandi, V.V.; Curtis, M.; Rosenthal, D.M. Provision of naloxone to injection drug users as an overdose prevention strategy: Early evidence from a pilot study in New York City. Addict. Behav. 2006, 31, 907–912. [Google Scholar] [CrossRef]
- Gaston, R.L.; Best, D.; Manning, V.; Day, E. Can we prevent drug related deaths by training opioid users to recognise and manage overdoses? Harm Reduct. J. 2009, 6, 26. [Google Scholar] [CrossRef] [Green Version]
- Krawczyk, N.; Buresh, M.; Gordon, M.S.; Blue, T.R.; Fingerhood, M.I.; Agus, D. Expanding low-threshold buprenorphine to justice-involved individuals through mobile treatment: Addressing a critical care gap. J. Subst. Abus. Treat. 2019, 103, 1–8. [Google Scholar] [CrossRef]
- Mitra, S.; Rachlis, B.; Krysowaty, B.; Marshall, Z.; Olsen, C.; Rourke, S.; Kerr, T. Potential use of supervised injection services among people who inject drugs in a remote and mid-size Canadian setting. BMC Public Health 2019, 19, 284. [Google Scholar] [CrossRef] [PubMed]
- Hanson, B.L.; Porter, R.R.; Zöld, A.L.; Terhorst-Miller, H. Preventing opioid overdose with peer-administered naloxone: Findings from a rural state. Harm Reduct. J. 2020, 17, 1–9. [Google Scholar] [CrossRef]
- Kerr, T.; Small, W.; Peeace, W.; Douglas, D.; Pierre, A.; Wood, E. Harm reduction by a “user-run” organization: A case study of the Vancouver Area Network of Drug Users (VANDU). Int. J. Drug Policy 2006, 17, 61–69. [Google Scholar] [CrossRef]
- Kolla, G.; Strike, C. ‘It’s too much, I’m getting really tired of it’: Overdose response and structural vulnerabilities among harm reduction workers in community settings. Int. J. Drug Policy 2019, 74, 127–135. [Google Scholar] [CrossRef] [PubMed]
- McAuley, A.; Munro, A.; Taylor, A. “Once I’d done it once it was like writing your name”: Lived experience of take-home naloxone administration by people who inject drugs. Int. J. Drug Policy 2018, 58, 46–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNeil, R.; Small, W.C.; Lampkin, H.; Shannon, K.; Kerr, T. “People Knew They Could Come Here to Get Help”: An Ethnographic Study of Assisted Injection Practices at a Peer-Run ‘Unsanctioned’ Supervised Drug Consumption Room in a Canadian Setting. AIDS Behav. 2014, 18, 473–485. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, K.; Durante, S.E.; Pellatt, K.; Richardson, C.G.; Mathias, S.; Buxton, J.A. Naloxone and the Inner City Youth Experience (NICYE): A community-based participatory research study examining young people’s perceptions of the BC take home naloxone program. Harm Reduct. J. 2017, 14, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owczarzak, J.; Weicker, N.; Urquhart, G.; Morris, M.; Park, J.N.; Sherman, S.G. “We know the streets:” race, place, and the politics of harm reduction. Health Place 2020, 64, 102376. [Google Scholar] [CrossRef]
- Palamar, J.J.; Acosta, P.; Sutherland, R.; Shedlin, M.G.; Barratt, M.J. Adulterants and altruism: A qualitative investigation of “drug checkers” in North America. Int. J. Drug Policy 2019, 74, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Parkin, S.; Neale, J.; Brown, C.; Campbell, A.N.; Castillo, F.; Jones, J.D.; Strang, J.; Comer, S.D. Opioid overdose reversals using naloxone in New York City by people who use opioids: Implications for public health and overdose harm reduction approaches from a qualitative study. Int. J. Drug Policy 2020, 79, 102751. [Google Scholar] [CrossRef]
- Pauly, B.B.; Mamdani, Z.; Mesley, L.; McKenzie, S.; Cameron, F.; Edwards, D.; Howell, A.; Knott, M.; Scott, T.; Seguin, R.; et al. It’s an emotional roller coaster… But sometimes it’s fucking awesome”: Meaning and motivation of work for peers in overdose response environments in British Columbia. Int. J. Drug Pol. 2021, 88, 103015. [Google Scholar] [CrossRef]
- Small, W.; Wood, E.; Tobin, D.; Rikley, J.; Lapushinsky, D.; Kerr, T. The Injection Support Team: A Peer-Driven Program to Address Unsafe Injecting in a Canadian Setting. Subst Use Misuse 2012, 47, 491–501. [Google Scholar] [CrossRef]
- Van Schipstal, I.; Mishra, S.; Berning, M.; Murray, H. Harm Reduction from Below. Contemp. Drug Probl. 2016, 43, 199–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartlett, N.; Xin, D.; Zhang, H.; Huang, B. A qualitative evaluation of a peer-implemented overdose response pilot project in Gejiu, China. Int. J. Drug Policy 2011, 22, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Boyd, S.; Murray, D.; MacPherson, D. Telling our stories: Heroin-assisted treatment and SNAP activism in the Downtown Eastside of Vancouver. Harm. Reduct. J. 2017, 14, 27:1–27:14. [Google Scholar] [CrossRef] [Green Version]
- Farrugia, A.; Neale, J.; Dwyer, R.; Fomiatti, R.; Fraser, S.; Strang, J.; Dietze, P. Conflict and communication: Managing the multiple affordances of take-home naloxone administration events in Australia. Addict. Res. Theory 2020, 28, 29–37. [Google Scholar] [CrossRef]
- Bardwell, G.; Boyd, J.; Kerr, T.; McNeil, R. Negotiating space & drug use in emergency shelters with peer witness injection programs within the context of an overdose crisis: A qualitative study. Health Place 2018, 53, 86–93. [Google Scholar] [CrossRef]
- Dechman, M.K. Peer helpers’ struggles to care for “others” who inject drugs. Int. J. Drug Policy 2015, 26, 492–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faulkner-Gurstein, R. The social logic of naloxone: Peer administration, harm reduction, and the transformation of social policy. Soc. Sci. Med. 2017, 180, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Glick, J.L.; Christensen, T.; Park, J.N.; McKenzie, M.; Green, T.C.; Sherman, S.G. Stakeholder perspectives on implementing fentanyl drug checking: Results from a multi-site study. Drug Alcohol Depend. 2019, 194, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Green, T.C.; Bowman, S.E.; Ray, M.; McKenzie, M.; Lord, S.E.; Rich, J.D. Development of an incarceration-specific overdose prevention video: Staying Alive on the Outside. Health Educ. J. 2015, 74, 627–637. [Google Scholar] [CrossRef]
- Bergamo, S.; Parisi, G.; Jarre, P. Harm reduction in Italy: The experience of an unsanctioned supervised injection facility run by drug users. Drugs Alcohol Today 2018, 19, 59–71. [Google Scholar] [CrossRef]
- Leece, P.; Khorasheh, T.; Paul, N.; Keller-Olaman, S.; Massarella, S.; Caldwell, J.; Parkinson, M.; Strike, C.; Taha, S.; Penney, G.; et al. ‘Communities are attempting to tackle the crisis’: A scoping review on community plans to prevent and reduce opioid-related harms. BMJ Open 2019, 9, e028583. [Google Scholar] [CrossRef]
- Olding, M.; Ivsins, A.; Mayer, S.; Betsos, A.; Boyd, J.; Sutherland, C.; Culbertson, C.; Kerr, T.; McNeil, R. A Low-Barrier and Comprehensive Community-Based Harm-Reduction Site in Vancouver, Canada. Am. J. Public Health 2020, 110, 833–835. [Google Scholar] [CrossRef]
- Kerr, T.; Mitra, S.; Kennedy, M.C.; McNeil, R. Supervised injection facilities in Canada: Past, present, and future. Harm Reduct. J. 2017, 14, 1–9. [Google Scholar] [CrossRef]
- McAuley, A.; Aucott, L.; Matheson, C. Exploring the life-saving potential of naloxone: A systematic review and descriptive meta-analysis of take home naloxone (THN) programmes for opioid users. Int. J. Drug Policy 2015, 26, 1183–1188. [Google Scholar] [CrossRef]
- McNeil, R.; Small, W. ‘Safer environment interventions’: A qualitative synthesis of the experiences and perceptions of people who inject drugs. Soc. Sci. Med. 2014, 106, 151–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, T.M.; Kolla, G.; van der Meulen, E.; Dodd, Z. Critical studies of harm reduction: Overdose response in uncertain political times. Int. J. Drug Policy 2019, 76, 102615. [Google Scholar] [CrossRef]
- Small, D.; Palepu, A.; Tyndall, M.W. The establishment of North America’s first state sanctioned supervised injection facility: A case study in culture change. Int. J. Drug Policy 2006, 17, 73–82. [Google Scholar] [CrossRef]
- Wallace, B.; Van Roode, T.; Pagan, F.; Phillips, P.; Wagner, H.; Calder, S.; Aasen, J.; Pauly, B.; Hore, D. What is needed for implementing drug checking services in the context of the overdose crisis? A qualitative study to explore perspectives of potential service users. Harm Reduct. J. 2020, 17, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Caulkins, J.P.; Pardo, B.; Kilmer, B. Supervised consumption sites: A nuanced assessment of the causal evidence. Addiction 2019, 114, 2109–2115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livingston, J.D. Supervised consumption sites and crime: Scrutinizing the methodological weaknesses and aberrant results of a government report in Alberta, Canada. Harm. Reduct. J. 2021, 18, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Ashford, R.D.; Curtis, B.; Brown, A.M. Peer-delivered harm reduction and recovery support services: Initial evaluation from a hybrid recovery community drop-in center and syringe exchange program. Harm Reduct. J. 2018, 15, 52. [Google Scholar] [CrossRef] [Green Version]
- Olding, M.; Boyd, J.; Kerr, T.; McNeil, R. And we just have to keep going: Task shifting and the production of burnout among overdose response workers with lived experience. Soc. Sci. Med. 2021, 270, 113631. [Google Scholar] [CrossRef] [PubMed]
- Mamdani, Z.; Mckenzie, S.; Cameron, F.; Knott, M.; Conway-brown, J.; Scott, T. Using Intervention Mapping to Develop ‘ROSE’: An Intervention to Support Peer Workers in Overdose Response Settings. 2021. Available online: https://assets.researchsquare.com/files/rs-406184/v2/58e10d83-c0c9-428a-9a67-3e69d30a04c0.pdf?c=1631888305 (accessed on 17 July 2021).
- Greer, A.; Bungay, V.; Pauly, B.; Buxton, J. ‘Peer’ work as precarious: A qualitative study of work conditions and experiences of people who use drugs engaged in harm reduction work. Int. J. Drug Pol. 2020, 85, 102922. [Google Scholar] [CrossRef] [PubMed]
- Schneider, K.E.; Park, J.N.; Allen, S.T.; Weir, B.W.; Sherman, S.G. Knowledge of ‘Good Samaritan’ laws and beliefs about arrests among persons who inject drugs a year after policy change in Baltimore, Maryland. Public Health Rep. 2020, 135, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Souleymanov, R.; Kuzmanović, D.; Marshall, Z.; Scheim, A.I.; Mikiki, M.; Worthington, C.; Millson, M.P. The ethics of community-based research with people who use drugs: Results of a scoping review. BMC Med. Ethics 2016, 17, 25. [Google Scholar] [CrossRef] [Green Version]
- Salazar, Z.R.; Vincent, L.; Figgatt, M.C.; Gilbert, M.K.; Dasgupta, N. Research led by people who use drugs: Centering the expertise of lived experience. Subst. Abus. Treat. Prev. Policy 2021, 16, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Papamihali, K.; Yoon, M.; Graham, B.; Karamouzian, M.; Slaunwhite, A.K.; Tsang, V.; Young, S.; Buxton, J.A. Convenience and comfort: Reasons reported for using drugs alone among clients of harm reduction sites in British Columbia, Canada. Harm Reduct. J. 2020, 17, 1–11. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion | Exclusion |
|---|---|
| Populations | |
|
|
| Interventions | |
|
|
| Comparators | |
|
|
| Outcomes | |
|
|
| Study design | |
|
|
| Operator | Definition |
|---|---|
| PsychINFO | |
| TI (peer support OR peer intervention OR peers OR peer mentor) OR AB (peer support OR peer intervention OR peers OR peer mentor) OR KW (peer support OR peer intervention OR peers OR peer mentor) |
| SU (peer support OR peer intervention OR peers OR peer mentoring OR lived experience) |
| 1 OR 2 |
| TI (substance use or substance abuse or substance misuse or drug use or drug abuse or drug misuse or dependence or addiction or alcohol use or alcohol misuse or alcohol abuse or alcoholism or smoking) OR AB (substance use or substance abuse or substance misuse or drug use or drug abuse or drug misuse or dependence or addiction or alcohol use or alcohol misuse or alcohol abuse or alcoholism or smoking) OR KW (substance use or substance abuse or substance misuse or drug use or drug abuse or drug misuse or dependence or addiction or alcohol use or alcohol misuse or alcohol abuse or alcoholism or smoking) |
| SU substance use or substance abuse or substance misuse or drug use or drug abuse or drug misuse or dependence or addiction or alcohol use or alcohol misuse or alcohol abuse or alcoholism or smoking |
| 4 OR 5 |
| TI harm reduction OR AB harm reduction OR KW harm reduction |
| SU harm reduction |
| 7 OR 8 |
| 3 AND 6 AND 9 |
| English language |
| 2000–2020 |
| Removal of duplicates followed by PRISMA guidelines of article sifting: title sift, abstract sift, full-text sift, review reference lists, and articles citing. |
| Interventions | Description of Intervention | Number of Papers | Papers |
|---|---|---|---|
| Naloxone-related interventions | Naloxone is a medication that can reverse the effects of opioids to save lives during an overdose. Interventions include training in recognising signs of overdose and safely administering naloxone, take-home naloxone (THN) programmes which provide naloxone to be used when witnessing an overdose, and peer programmes where people who inject drugs are trained to use it to help their peers. | 23 | [15,17,33,44,46,47,48,49,52,53,56,58,59,61,62,64,68,70,72,76,77,80,82] |
| Safer environments for drug use | Creating environments which offer safety or supervision during drug consumption to reduce risk of overdose, such as safe consumption sites. Spaces can be staffed with paid employees, volunteers, or peers trained in the use of naloxone. | 13 | [23,32,35,50,55,60,66,71,76,79,81,82,83] |
| Overdose prevention education interventions | Provision of training to bystanders regarding how to intervene during a witnessed opioid overdose. This includes brief interventions, education, and training related to overdose management and intervention. | 7 | [47,53,57,58,66,75,77] |
| Opioid substitution treatment (OST) | Treatment to reduce drug dependence and injecting frequency by offering people who are opioid dependent an alternative, prescribed medicine, typically methadone or buprenorphine. | 4 | [17,54,69,78] |
| Drug checking | Drug checking services enable individuals to have their drugs chemically analysed, providing information on the content of the samples as well as advice, and, in some cases, counselling or brief interventions. | 4 | [63,74,78,84] |
| Social network and support interventions | Relational interventions across different contexts which focus on the provision of social support and connection to PWUD by peers. | 3 | [51,57,67] |
| Intervention Type | Theme | Subthemes |
|---|---|---|
| Naloxone-related | PWUD * engaged and committed to peer-involved interventions | Naloxone administration Naloxone education and training |
| Benefits for the administrator | Empowerment Reduction in risk | |
| Naloxone and expanding community level harm reduction | Reach in the community Integration in the community | |
| Barriers to naloxone use | Micro barriers Macro barriers | |
| Implications of naloxone intervention | Unpleasant effects of withdrawal Pleasure from illicit drug use | |
| Safer environments for drug use | The role of peers in the social dynamics of safer environments for drug use | Connectivity Mitigation of barriers and risk Constraints |
| A trusted environment created by peers | Safety Comfort Trust | |
| Benefits for peer workers in safer environments for drug use | ||
| Challenges for peer workers in safer environments for drug use | Individual challenges Organizational and macro challenges | |
| Overdose prevention education | Peers providing actionable knowledge and skills | |
| Impact of overdose prevention education on behaviour | ||
| Limitations of peer inclusion in overdose prevention education | ||
| Opioid substitution treatment (OST) | Low-barrier community reintegration | |
| Peers as Experts | ||
| Challenges associated with OST | ||
| Drug checking | Hesitancy to engage with technology | |
| Social checking | ||
| Social networks and support interventions | Reciprocity |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mercer, F.; Miler, J.A.; Pauly, B.; Carver, H.; Hnízdilová, K.; Foster, R.; Parkes, T. Peer Support and Overdose Prevention Responses: A Systematic ‘State-of-the-Art’ Review. Int. J. Environ. Res. Public Health 2021, 18, 12073. https://doi.org/10.3390/ijerph182212073
Mercer F, Miler JA, Pauly B, Carver H, Hnízdilová K, Foster R, Parkes T. Peer Support and Overdose Prevention Responses: A Systematic ‘State-of-the-Art’ Review. International Journal of Environmental Research and Public Health. 2021; 18(22):12073. https://doi.org/10.3390/ijerph182212073
Chicago/Turabian StyleMercer, Fiona, Joanna Astrid Miler, Bernie Pauly, Hannah Carver, Kristina Hnízdilová, Rebecca Foster, and Tessa Parkes. 2021. "Peer Support and Overdose Prevention Responses: A Systematic ‘State-of-the-Art’ Review" International Journal of Environmental Research and Public Health 18, no. 22: 12073. https://doi.org/10.3390/ijerph182212073