
Factors Influencing Care Pathways for Breast and Prostate Cancer in a Hospital Setting



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
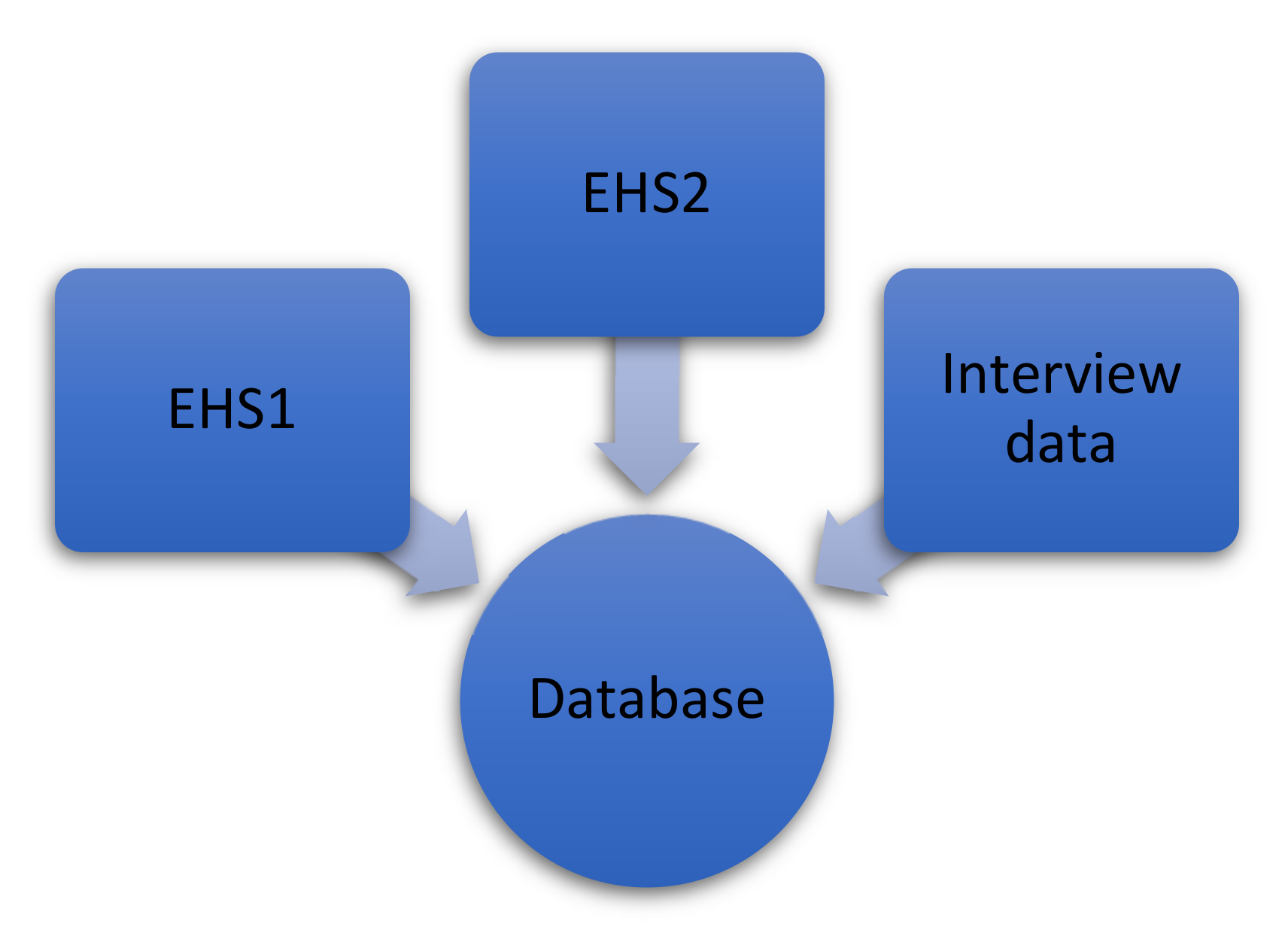
2.2. Data Sources
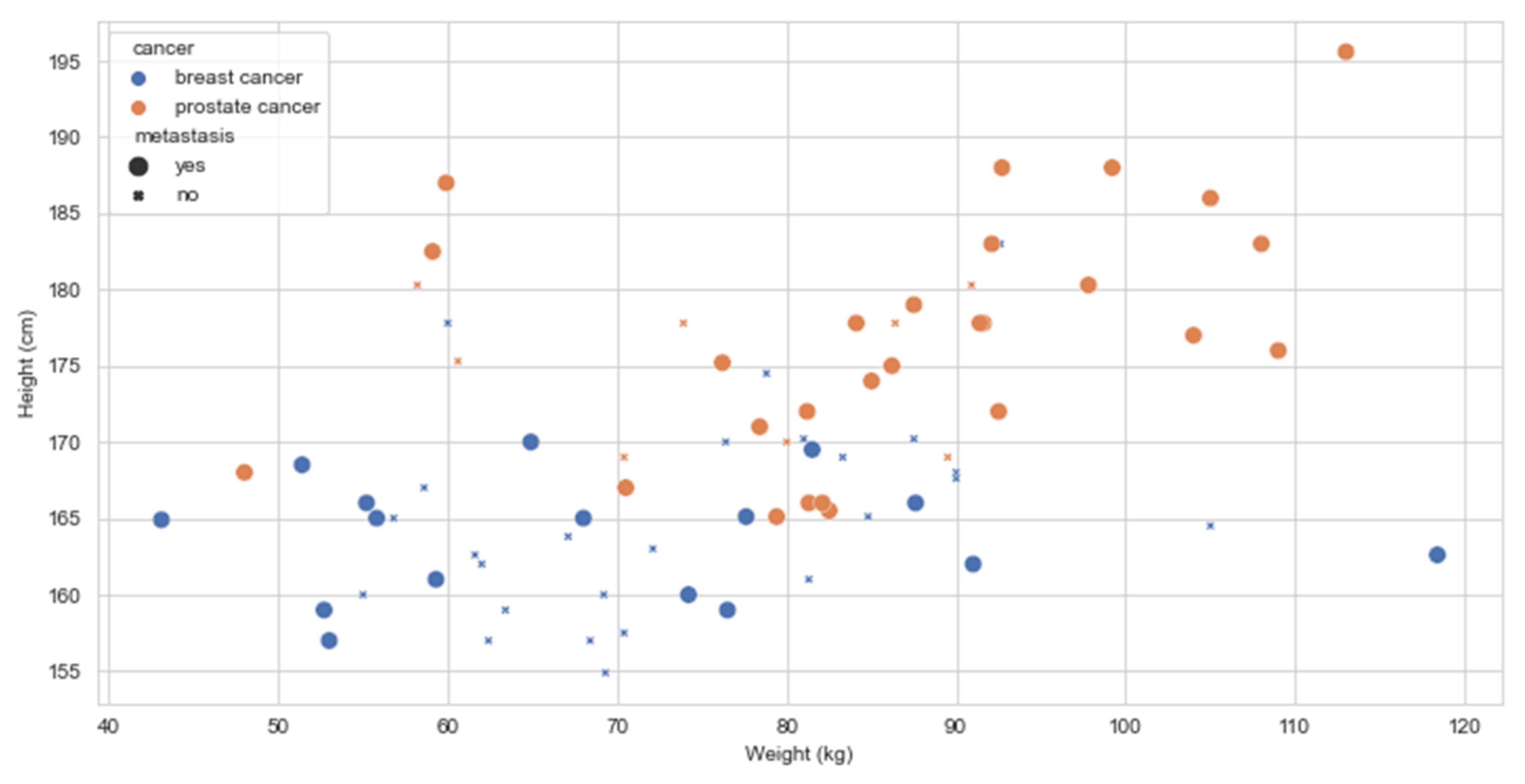
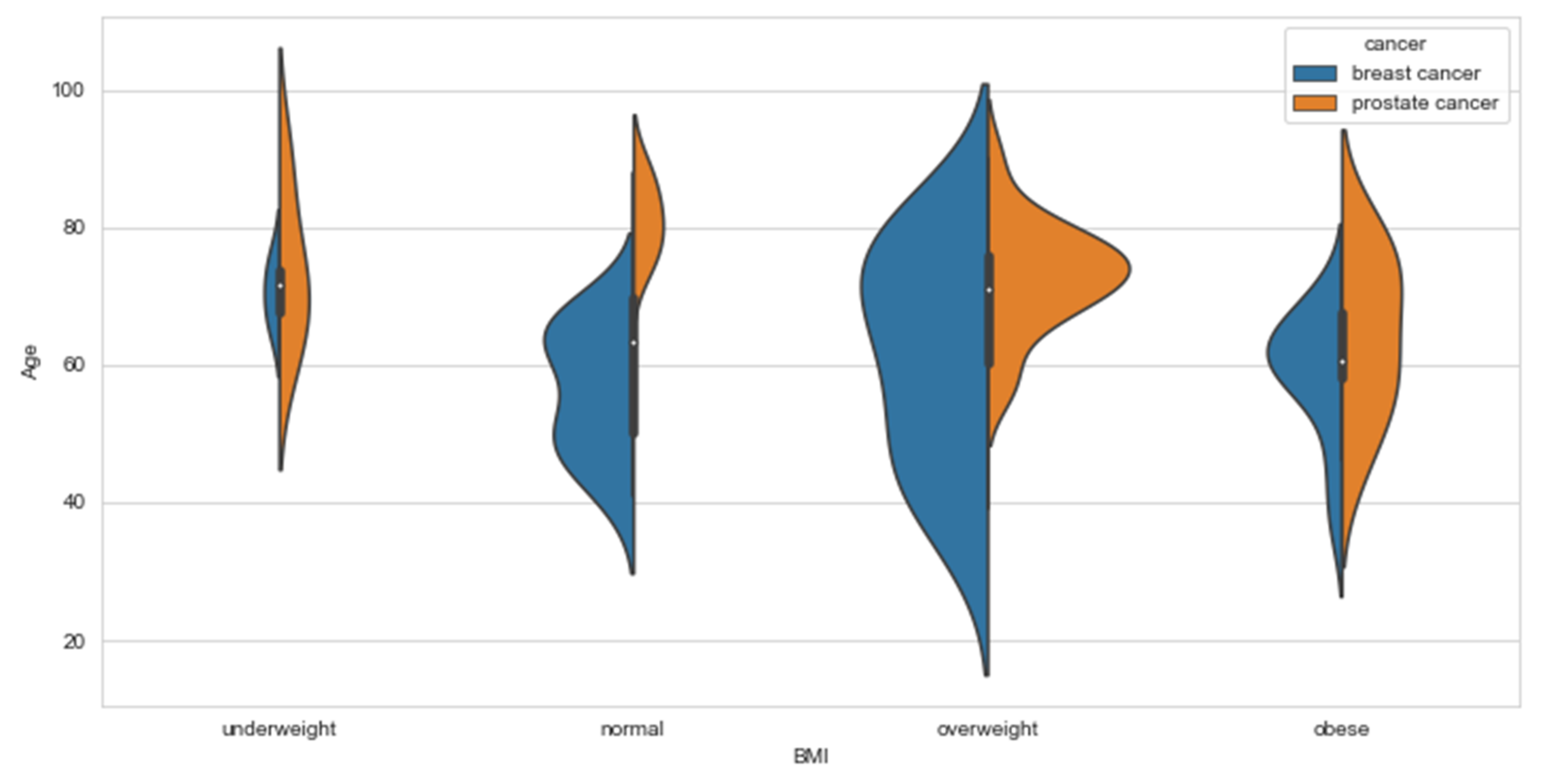
2.2.1. Demographic Data
2.2.2. Medical Data
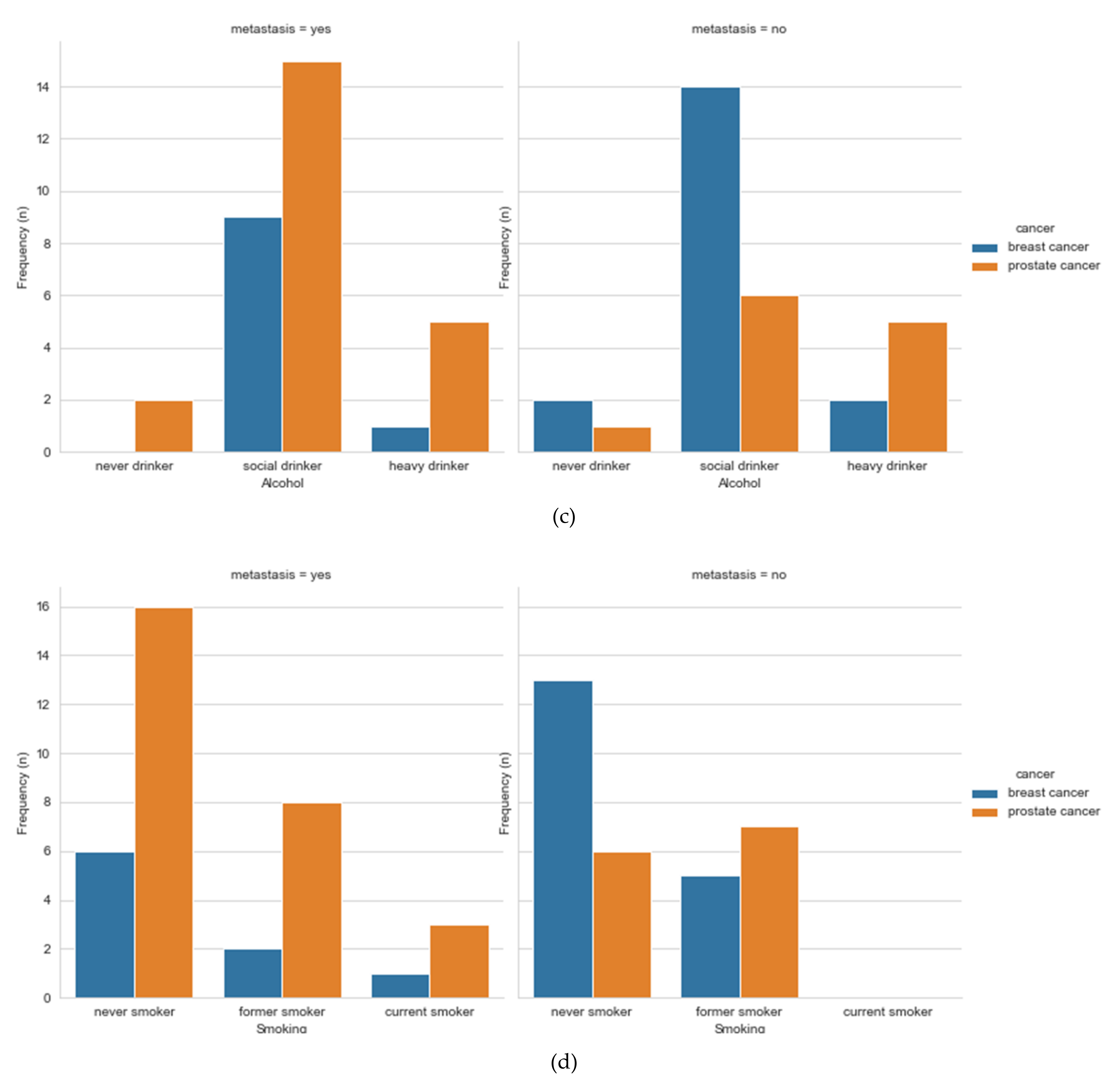
2.2.3. Lifestyle Data
2.3. Statistical Analysis
2.4. Ethics Statement
3. Results
3.1. Breast Cancer Study
3.1.1. Chemotherapy
3.1.2. Targeted Therapy
3.1.3. Surgery
3.1.4. Endocrine Therapy
3.1.5. Radiotherapy
3.1.6. Bisphosphonate
3.2. Prostate Cancer Study
3.2.1. Endocrine Therapy
3.2.2. Chemotherapy
3.2.3. Radiotherapy
3.2.4. Bisphosphonate
3.2.5. Radium Ra 223 Dichloride
3.2.6. Surgery
3.3. Breast and Prostate Analysis
3.3.1. Chemotherapy
3.3.2. Radiotherapy
3.3.3. Endocrine Therapy
3.3.4. Surgery
3.3.5. Bisphosphonate
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | No. of Patients |
|---|---|
| Total number of patients selected to participate in the study | 117 |
| Patients contacted | 109 |
| Patients participated | 83 |
| Breast cancer patients | 41 |
| Prostate cancer patients | 42 |
| Patients who did not want to participate | 18 |
| Patients who withdrew | 1 |
| Patients who forgot about the interview appointment | 1 |
| Patients who rescheduled the interview beyond the study period | 1 |
| Patients who did not feel well to participate | 4 |
| Patients who did not participate because of the length of the interview | 4 |
| Patients who did not participate and did not give any explanation | 7 |
| Patients who were told about the study but were not interviewed because the number of participants was reached | 8 |
| Patients who were selected but not contacted | 8 |
Pre diagnosis
|
| Diagnosis Breast clinic appointment
|
Treatment
|
Follow-up
|
References
- International Agency for Research on Cancer, WHO. Cancer Tomorrow. Available online: https://gco.iarc.fr/tomorrow/en/dataviz/bars?mode=population (accessed on 14 April 2021).
- National Cancer Registry Ireland. Cancer Factsheet. Available online: https://www.ncri.ie/factsheets (accessed on 14 April 2021).
- Fioretti, F.; Tavani, A.; Bosetti, C.; La Vecchia, C.; Negri, E.; Barbone, F.; Talamini, R.; Franceschi, S. Risk factors for breast cancer in nulliparous women. Br. J. Cancer 1999, 79, 1923–1928. [Google Scholar] [CrossRef] [PubMed]
- Centre for Disease Control and Prevention. National Health Interview Survey, Glossary, General Concepts. Available online: https://www.cdc.gov/nchs/nhis/tobacco/tobacco_glossary.htm (accessed on 14 April 2021).
- National Institute on Alcohol Abuse and Alcoholism. Drinking Levels Defined. Available online: https://www.niaaa.nih.gov/alcohol-health/overview-alcohol-consumption/moderate-binge-drinking (accessed on 14 April 2021).
- Bakker, M.F.; De Lange, S.V.; Pijnappel, R.M.; Mann, R.M.; Peeters, P.H.; Monninkhof, E.M.; Emaus, M.J.; Loo, C.E.; Bisschops, R.H.; Lobbes, M.B.; et al. Supplemental MRI Screening for Women with Extremely Dense Breast Tissue. N. Engl. J. Med. 2019, 381, 2091–2102. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Bella, F.; Godos, J.; Sciacca, S.; Del Rio, D.; Ray, S.; Galvano, F.; Giovannucci, E.L. Possible role of diet in cancer: Systematic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr. Rev. 2017, 75, 405–419. [Google Scholar] [CrossRef] [PubMed]
- Mourouti, N.; Kontogianni, M.; Papavagelis, C.; Panagiotakos, D.B. Diet and breast cancer: A systematic review. Int. J. Food Sci. Nutr. 2014, 66, 1–42. [Google Scholar] [CrossRef] [PubMed]
- Chajès, V.; Romieu, I. Nutrition and breast cancer. Maturitas 2014, 77, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Dandamudi, A.; Tommie, J.; Nommsen-Rivers, L.; Couch, S. Dietary Patterns and Breast Cancer Risk: A Systematic Review. Anticancer Res. 2018, 38, 3209–3222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeinomar, N.; kConFab Investigators; Knight, J.A.; Genkinger, J.M.; Phillips, K.-A.; Daly, M.B.; Milne, R.L.; Dite, G.S.; Kehm, R.D.; Liao, Y. Alcohol consumption, cigarette smoking, and familial breast cancer risk: Findings from the Prospective Family Study Cohort (ProF-SC). Breast Cancer Res. 2019, 21, 128. [Google Scholar] [CrossRef] [PubMed]
- Macacu, A.; Autier, P.; Boniol, M.; Boyle, P. Active and passive smoking and risk of breast cancer: A meta-analysis. Breast Cancer Res. Treat. 2015, 154, 213–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzal, F.; Bjelic-Radisic, V.; Knauer, M.; Steger, G.; Hubalek, M.; Balic, M.; Singer, C.; Bartsch, R.; Schrenk, P.; Soelkner, L.; et al. Impact of Breast Surgery in Primary Metastasized Breast Cancer. Ann. Surg. 2019, 269, 1163–1169. [Google Scholar] [CrossRef] [PubMed]
- Rashaan, Z.; Bastiaannet, E.; Portielje, J.; van de Water, W.; van der Velde, S.; Ernst, M.; van de Velde, C.; Liefers, G. Surgery in metastatic breast cancer: Patients with a favorable profile seem to have the most benefit from surgery. Eur. J. Surg. Oncol. 2012, 38, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Incorvati, J.A.; Shah, S.; Mu, Y.; Lu, J. Targeted therapy for HER2 positive breast cancer. J. Hematol. Oncol. 2013, 6, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Comprehensive Cancer Network. Practice Guidelines in Oncology: Breast Cancer. Available online: https://www.nccn.org/store/login/login.aspx?ReturnURL=https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on 6 September 2019).
- Vyas, O.H.; Kaklamani, V.G. Evaluating the Role of Extended Aromatase Inhibitor Therapy in Early Hormone-Positive Breast Cancer. Curr. Breast Cancer Rep. 2017, 9, 183–187. [Google Scholar] [CrossRef]
- Møller, H.; Roswall, N.; Van Hemelrijck, M.; Larsen, S.B.; Cuzick, J.; Holmberg, L.; Overvad, K.; Tjonneland, A. Prostate cancer incidence, clinical stage and survival in relation to obesity: A prospective cohort study in Denmark. Int. J. Cancer 2015, 136, 1940–1947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassett, J.K.; Severi, G.; Baglietto, L.; MacInnis, R.; Hoang, H.N.; Hopper, J.L.; English, D.; Giles, G. Weight change and prostate cancer incidence and mortality. Int. J. Cancer 2012, 131, 1711–1719. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.; Tilling, K.; Turner, E.L.; Martin, R.; Lennon, R.; Lane, J.A.; Donovan, J.L.; Hamdy, F.C.; Neal, D.E.; Bosch, J.L.H.R.; et al. Systematic review and meta-analysis of the associations between body mass index, prostate cancer, advanced prostate cancer, and prostate-specific antigen. Cancer Causes Control 2020, 31, 431–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, F.F.; Leitzmann, M.F.; Hillreiner, A.; Sedlmeier, A.; Prokopidi-Danisch, M.E.; Burger, M.; Jochem, C. Sedentary Behavior and Prostate Cancer: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Cancer Prev. Res. 2019, 12, 675–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zuccolo, L.; Harris, R.; Gunnell, D.; Oliver, S.; Lane, J.A.; Davis, M.; Donovan, J.; Neal, D.; Hamdy, F.; Beynon, R.; et al. Height and Prostate Cancer Risk: A Large Nested Case-Control Study (ProtecT) and Meta-analysis. Cancer Epidemiol. Biomark. Prev. 2008, 17, 2325–2336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez-Cornago, A.; Appleby, P.N.; Pischon, T.; Tsilidis, K.K.; Tjønneland, A.; Olsen, A.; Overvad, K.; Kaaks, R.; Kühn, T.; Boeing, H.; et al. Tall height and obesity are associated with an increased risk of aggressive prostate cancer: Results from the EPIC cohort study. BMC Med. 2017, 15, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.M.; PRACTICAL Consortium; Gaunt, T.; Lewis, S.; Holly, J.; Donovan, J.L.; Hamdy, F.C.; Kemp, J.; Eeles, R.; Easton, D. The effects of height and BMI on prostate cancer incidence and mortality: A Mendelian randomization study in 20,848 cases and 20,214 controls from the PRACTICAL consortium. Cancer Causes Control 2015, 26, 1603–1616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khankari, N.K.; Shu, X.-O.; Wen, W.; Kraft, P.; Lindström, S.; Peters, U.; Schildkraut, J.; Schumacher, F.; Bofetta, P.; Risch, A.; et al. Association between Adult Height and Risk of Colorectal, Lung, and Prostate Cancer: Results from Meta-analyses of Prospective Studies and Mendelian Randomization Analyses. PLoS Med. 2016, 13, e1002118. [Google Scholar] [CrossRef] [PubMed] [Green Version]






| Characteristics | Breast Cancer | Prostate Cancer |
|---|---|---|
| Sex | ||
| Male | 0 (0%) | 42 (100%) |
| Female | 41 (100%) | 0 (0%) |
| Age (years) | ||
| Median (range) | 61 (33–83) | 74 (46–90) |
| Median on diagnosis (range) | 58 (33–81) | 66 (38–86) |
| Education | ||
| No education | 0 (0%) | 2 (4.8%) |
| Primary school | 0 (0%) | 5 (11.9%) |
| Secondary school | 12 (29.3%) | 4 (9.5%) |
| Professional certificate | 1 (2.4%) | 6 (14.3%) |
| Bachelor’s degree | 20 (48.8%) | 9 (21.4%) |
| Master’s degree | 8 (19.5%) | 1 (2.4%) |
| PhD | 0 (0%) | 4 (9.5%) |
| No information | 0 (0%) | 11 (26.2%) |
| Work | ||
| Full time employment | 18 (43.9%) | 6 (14.3%) |
| Part time employment | 1 (2.4%) | 2 (4.8%) |
| Unemployed | 2 (4.9%) | 2 (4.8%) |
| Retired | 19 (46.3%) | 25 (59.5%) |
| No information | 1 (2.4%) | 7 (16.7%) |
| Marital status | ||
| Single | 5 (12.2%) | 3 (7.1%) |
| Married | 24 (58.5%) | 34 (81.0%) |
| Partnership | 2 (4.9%) | 0 (0%) |
| Widowed | 6 (14.6%) | 5 (11.9%) |
| Divorced | 1 (2.4%) | 0 (0%) |
| Unmarried | 3 (7.3%) | 0 (0%) |
| Provinces | ||
| Connacht | 0 (0%) | 2 (4.8%) |
| Leinster | 40 (97.6%) | 37 (88.1%) |
| Munster | 1 (2.4%) | 1 (2.4%) |
| Ulster | 0 (0%) | 2 (4.8%) |
| Religion | ||
| Not religious | 7 (17.1%) | 2 (4.8%) |
| Religious | 25 (61.0%) | 30 (71.4%) |
| Not disclosed | 9 (22.0%) | 10 (23.8%) |
| Insurance | ||
| Private insurance | 24 (58.5%) | 37 (88.1%) |
| Self-pay | 17 (41.5%) | 5 (11.9%) |
| Chemotherapy (38/46) | Radiotherapy (28/46) | Targeted Therapy (25/46) | Endocrine Therapy (26/46) | Surgery (32/46) | BISPHOSPHONATE (11/46) | Immunotherapy (1/46) | |
|---|---|---|---|---|---|---|---|
| Age group | 0.079 | 0.506 | 0.837 | 0.527 | 0.638 | 0.708 | 0.876 |
| Hearing | 0.029 | 0.423 | 0.359 | 0.380 | 0.508 | 0.575 | 0.881 |
| Vision | 0.363 | 0.734 | 0.596 | 0.596 | 0.075 | 0.267 | 0.371 |
| Allergies | 0.496 | 0.801 | 0.773 | 0.191 | 0.497 | 0.435 | 0.458 |
| BMI groups | 0.509 | 0.044 | 0.972 | 0.474 | 0.411 | 0.531 | 0.282 |
| Tumor stage group | 0.830 | 0.834 | 0.498 | 0.588 | 0.169 | 0.146 | .a |
| Cancer grade | 0.200 | 0.528 | 0.169 | 0.212 | 0.134 | 0.058 | .a |
| Cancer stage | 0.628 | 0.404 | 0.272 | 0.279 | 0.058 | 0.022 | 0.414 |
| Diet | 0.522 | 0.919 | 0.221 | 0.132 | 0.016 | 0.051 | 0.067 |
| Alcohol | 0.131 | 0.276 | 0.374 | 0.096 | 0.654 | 0.147 | 0.026 |
| Smoking | 0.244 | 0.170 | 0.038 | 0.918 | 0.095 | 0.710 | 0.182 |
| Exercise | 0.639 | 0.934 | 0.704 | 0.635 | 0.029 | 0.087 | 0.208 |
| Age at data collection | 0.039 | 0.752 | 0.612 | 0.723 | 0.867 | 0.887 | 0.706 |
| Age at diagnosis | 0.047 | 0.735 | 0.635 | 0.807 | 0.877 | 0.787 | 0.851 |
| Years diagnosed with cancer | 0.333 | 0.394 | 0.769 | 0.016 | 0.076 | 0.310 | 0.316 |
| Height (cm) | 0.632 | 0.089 | 0.154 | 0.649 | 0.693 | 0.511 | 0.546 |
| Weight (kg) | 0.739 | 0.042 | 0.675 | 0.471 | 0.346 | 0.797 | 0.243 |
| BMI | 0.783 | 0.007 | 0.974 | 0.492 | 0.527 | 0.787 | 0.163 |
| Tumor size (mm) | 0.706 | 0.784 | 0.503 | 0.800 | 0.331 | 0.174 | .a |
| Progesterone receptor score | 0.438 | 0.862 | 0.886 | 0.016 | 0.365 | 0.279 | 0.295 |
| Estrogen receptor score | 0.266 | 0.830 | 0.747 | 0.000 | 0.456 | 0.740 | 0.197 |
| HER2 score | 0.690 | 0.708 | 0.000 | 0.715 | 0.312 | 0.229 | 0.154 |
| Days between diagnosis and starting of treatment | 0.542 | 1.000 | 0.860 | 0.002 | 0.189 | 0.374 | 0.090 |
| Chemotherapy 1 cycles | 0.953 | 0.049 | 0.012 | 0.044 | 0.007 | 0.012 | 0.114 |
| Chemotherapy 2 cycles | 0.843 | 0.171 | 0.103 | 0.340 | 0.005 | 0.028 | 0.048 |
| Chemotherapy 3 cycles | .a | 0.881 | 0.319 | 0.811 | 0.319 | 0.319 | .a |
| Targeted therapy cycles | 0.662 | 0.951 | .a | 0.653 | 0.343 | 0.847 | .a |
| Bisphosphonate cycles | 0.813 | 0.170 | 0.260 | 0.184 | 0.238 | 0.045 | .a |
| Tumor size post neoadjuvant chemotherapy (mm) | 0.353 | 0.353 | 0.715 | 0.172 | 0.353 | 0.353 | .a |
| Radiotherapy sessions first site | 0.139 | 0.812 | 0.575 | 0.330 | 0.355 | 0.084 | 0.317 |
| Radiotherapy site one Grey units | 0.622 | 0.579 | 0.227 | 0.471 | 0.234 | 0.084 | 0.317 |
| Radiotherapy sessions 2nd site | 0.376 | 0.274 | 0.741 | 0.804 | 1.000 | 0.510 | 0.302 |
| Radiotherapy site two Grey units | 0.189 | 0.829 | 0.683 | 0.288 | 0.392 | 0.780 | 0.307 |
| Oncotype score | .a | 0.737 | .a | 0.764 | 0.380 | .a | .a |
| Chemotherapy (17/42) | Radiotherapy (24/42) | Surgery (7/42) | Bisphosphonate (33/42) | Xofigo (8/42) | |
|---|---|---|---|---|---|
| Age | 0.002 | 0.088 | 0.332 | 0.198 | 0.577 |
| Age at diagnosis | 0.053 | 0.380 | 0.855 | 0.165 | 0.543 |
| Years with cancer | 0.000 | 0.003 | 0.015 | 0.501 | 0.633 |
| Height (cm) | 0.005 | 0.010 | 0.427 | 0.482 | 0.878 |
| Weight (kg) | 0.000 | 0.007 | 0.559 | 0.310 | 0.444 |
| BMI | 0.095 | 0.371 | 0.725 | 0.274 | 0.457 |
| Initial PSA | 0.840 | 0.097 | 0.820 | 0.002 | 0.185 |
| Diagnosis to treatment days | 0.040 | 0.523 | 0.000 | 0.592 | 0.397 |
| Age group | 0.067 | 0.923 | 1.000 | 0.281 | 0.741 |
| BMI groups | 0.017 | 0.362 | 0.430 | 0.482 | 0.455 |
| Gleason score | 0.490 | 0.215 | 0.347 | 0.495 | 0.207 |
| Diet | 0.810 | 0.281 | 0.434 | 0.483 | 0.057 |
| Drinking | 0.222 | 0.920 | 0.976 | 0.613 | 0.926 |
| Smoking | 0.693 | 0.901 | 0.458 | 0.350 | 0.653 |
| Exercise | 0.562 | 0.811 | 0.020 | 0.679 | 0.141 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bardhi, O.; Garcia-Zapirain, B.; Nuño-Solinis, R. Factors Influencing Care Pathways for Breast and Prostate Cancer in a Hospital Setting. Int. J. Environ. Res. Public Health 2021, 18, 7913. https://doi.org/10.3390/ijerph18157913
Bardhi O, Garcia-Zapirain B, Nuño-Solinis R. Factors Influencing Care Pathways for Breast and Prostate Cancer in a Hospital Setting. International Journal of Environmental Research and Public Health. 2021; 18(15):7913. https://doi.org/10.3390/ijerph18157913
Chicago/Turabian StyleBardhi, Ornela, Begonya Garcia-Zapirain, and Roberto Nuño-Solinis. 2021. "Factors Influencing Care Pathways for Breast and Prostate Cancer in a Hospital Setting" International Journal of Environmental Research and Public Health 18, no. 15: 7913. https://doi.org/10.3390/ijerph18157913