
Prenatal Particulate Matter (PM) Exposure and Natriuretic Peptides in Newborns from Mexico City

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Environmental Monitoring
2.3. Cotinine Measurements
2.4. Natriuretic Peptide Concentrations in Newborns
2.5. Statistical Analyses
3. Results
3.1. Characteristics of the Study Participants, PM Levels and Natriuretic Peptide Concentrations
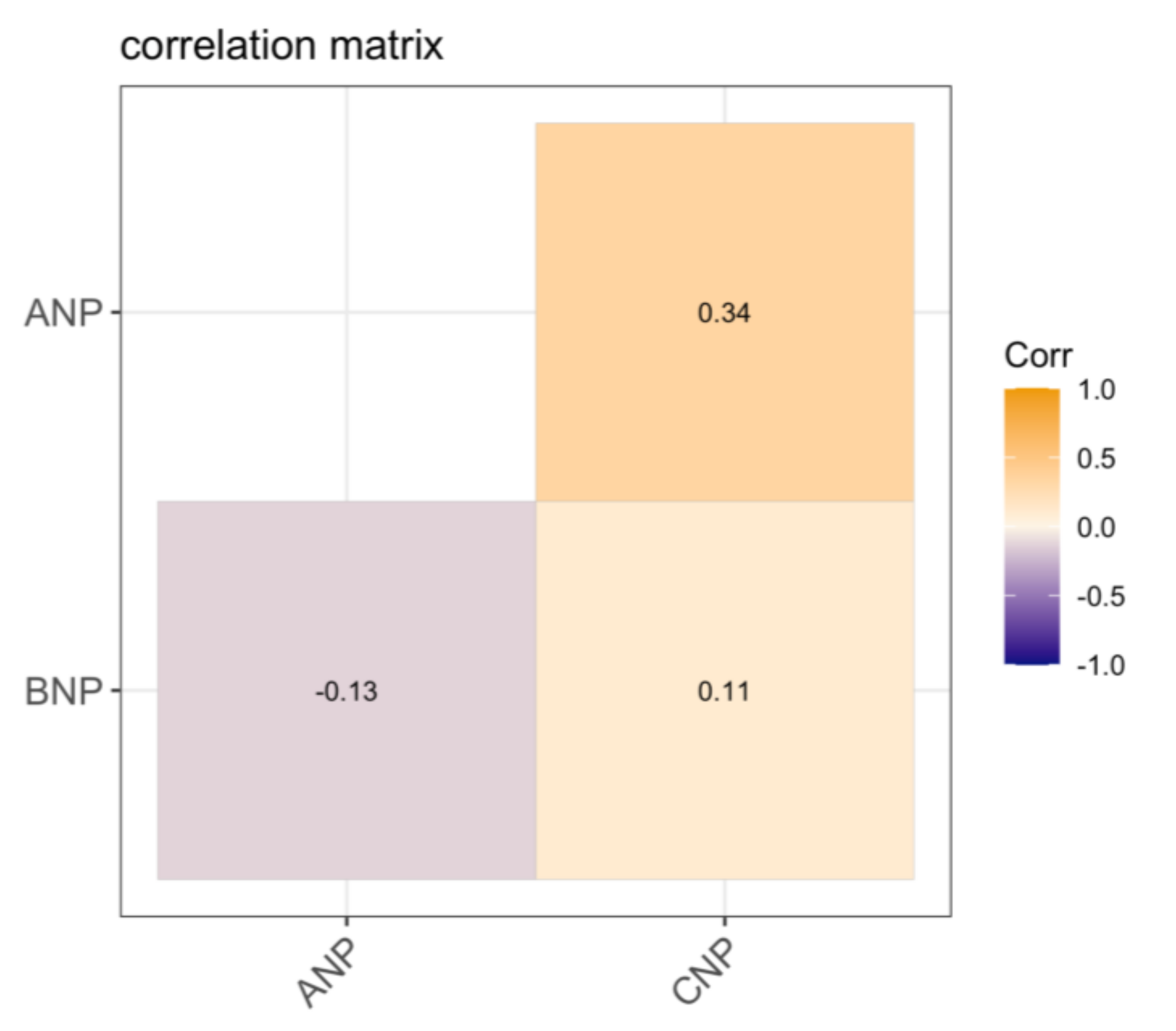
3.2. Correlations between Natriuretic Peptides, Characteristics of the Study Population and Particulate Matter Exposure
3.3. Multivariable Models for Associations between Natriuretic Peptides and PM2.5 or PM10 Exposure during Pregnancy
3.4. Linear Mixed Models to Assess Associations between Natriuretic Peptides and PM2.5 and PM10 Exposure during Pregnancy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goyal, N.; Karra, M.; Canning, D. Early-life exposure to ambient fine particulate air pollution and infant mortality: Pooled evidence from 43 low- and middle-income countries. Int. J. Epidemiol. 2019, 48, 1125–1141. [Google Scholar] [CrossRef] [PubMed]
- (INECC) INdEyCC: Valoración Económica de los Beneficios a la Salud de la Población Que se Alcanzarían por la Reducció de las PM2.5 Entres Zonas Metropolitanas Mexicanas. INECC; 2014. Available online: https://www.gob.mx/cms/uploads/attachment/file/195224/2014_CGSA_Beneficos_econ_micos_al_reducir_PM2.5.pdf (accessed on 19 December 2020).
- Trejo-Gonzalez, A.G.; Riojas-Rodriguez, H.; Texcalac-Sangrador, J.L.; Guerrero-Lopez, C.M.; Cervantes-Martinez, K.; Hurtado-Diaz, M.; de la Sierra-de la Vega, L.A.; Zuniga-Bello, P.E. Quantifying health impacts and economic costs of PM2.5 exposure in Mexican cities of the National Urban System. Int. J. Public Health 2019, 64, 561–572. [Google Scholar] [CrossRef]
- Liu, C.; Chen, R.; Sera, F.; Vicedo-Cabrera, A.M.; Guo, Y.; Tong, S.; Coelho, M.; Saldiva, P.H.N.; Lavigne, E.; Matus, P.; et al. Ambient Particulate Air Pollution and Daily Mortality in 652 Cities. N. Engl. J. Med. 2019, 381, 705–715. [Google Scholar] [CrossRef]
- Valavanidis, A.; Fiotakis, K.; Vlachogianni, T. Airborne particulate matter and human health: Toxicological assessment and importance of size and composition of particles for oxidative damage and carcinogenic mechanisms. J. Environ. Sci. Health C Environ. Carcinog. Ecotoxicol. Rev. 2008, 26, 339–362. [Google Scholar] [CrossRef]
- Dadvand, P.; Figueras, F.; Basagana, X.; Beelen, R.; Martinez, D.; Cirach, M.; Schembari, A.; Hoek, G.; Brunekreef, B.; Nieuwenhuijsen, M.J. Ambient air pollution and preeclampsia: A spatiotemporal analysis. Environ. Health Perspect 2013, 121, 1365–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Dong, H.; Ren, M.; Liang, Q.; Shen, X.; Wang, Q.; Yu, L.; Lin, H.; Luo, Q.; Chen, W.; et al. Ambient air pollution exposure and gestational diabetes mellitus in Guangzhou, China: A prospective cohort study. Sci. Total Environ. 2020, 699, 134390. [Google Scholar] [CrossRef]
- Ha, S.; Sundaram, R.; Buck Louis, G.M.; Nobles, C.; Seeni, I.; Sherman, S.; Mendola, P. Ambient air pollution and the risk of pregnancy loss: A prospective cohort study. Fertil. Steril. 2018, 109, 148–153. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Xu, J.; Chen, D.; Sun, P.; Ma, X. The association between air pollution and preterm birth and low birth weight in Guangdong, China. BMC Public Health 2019, 19, 3. [Google Scholar] [CrossRef]
- Ghassabian, A.; Pierotti, L.; Basterrechea, M.; Chatzi, L.; Estarlich, M.; Fernandez-Somoano, A.; Fleisch, A.F.; Gold, D.R.; Julvez, J.; Karakosta, P.; et al. Association of Exposure to Ambient Air Pollution With Thyroid Function During Pregnancy. JAMA Netw Open 2019, 2, e1912902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Rossem, L.; Rifas-Shiman, S.L.; Melly, S.J.; Kloog, I.; Luttmann-Gibson, H.; Zanobetti, A.; Coull, B.A.; Schwartz, J.D.; Mittleman, M.A.; Oken, E.; et al. Prenatal air pollution exposure and newborn blood pressure. Environ Health Perspect 2015, 123, 353–359. [Google Scholar] [CrossRef] [Green Version]
- Madhloum, N.; Nawrot, T.S.; Gyselaers, W.; Roels, H.A.; Bijnens, E.; Vanpoucke, C.; Lefebvre, W.; Janssen, B.G.; Cox, B. Neonatal blood pressure in association with prenatal air pollution exposure, traffic, and land use indicators: An ENVIRONAGE birth cohort study. Environ. Int. 2019, 130, 104853. [Google Scholar] [CrossRef] [PubMed]
- Shahoud, J.S.; Sanvictores, T.; Aeddula, N.R. Physiology, Arterial Pressure Regulation; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Aflyatumova, G.N.; Nigmatullina, R.R.; Sadykova, D.I.; Chibireva, M.D.; Fugetto, F.; Serra, R. Endothelin-1, nitric oxide, serotonin and high blood pressure in male adolescents. Vasc. Health Risk Manag. 2018, 14, 213–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sofronova, S.I.; Borzykh, A.A.; Gaynullina, D.K.; Kuzmin, I.V.; Shvetsova, A.A.; Lukoshkova, E.V.; Tarasova, O.S. Endothelial nitric oxide weakens arterial contractile responses and reduces blood pressure during early postnatal development in rats. Nitric Oxide 2016, 55, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Rubattu, S.; Forte, M.; Marchitti, S.; Volpe, M. Molecular Implications of Natriuretic Peptides in the Protection from Hypertension and Target Organ Damage Development. Int. J. Mol. Sci. 2019, 20, 798. [Google Scholar] [CrossRef] [Green Version]
- Gupta, D.K.; Wang, T.J. Natriuretic Peptides and Cardiometabolic Health. Circ. J. 2015, 79, 1647–1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forte, M.; Madonna, M.; Schiavon, S.; Valenti, V.; Versaci, F.; Zoccai, G.B.; Frati, G.; Sciarretta, S. Cardiovascular Pleiotropic Effects of Natriuretic Peptides. Int. J. Mol. Sci. 2019, 20, 3874. [Google Scholar] [CrossRef] [Green Version]
- Wilson, M.O.; Barrell, G.K.; Prickett, T.C.R.; Espiner, E.A. Molecular forms of C-type natriuretic peptide in cerebrospinal fluid and plasma reflect differential processing in brain and pituitary tissues. Peptides 2018, 99, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, D.; Garcia-Rivas, G.; Laresgoiti-Servitje, E.; Yanez, J.; Torre-Amione, G.; Jerjes-Sanchez, C. B-type natriuretic peptide reference interval of newborns from healthy and pre-eclamptic women: A prospective, multicentre, cross-sectional study. BMJ Open 2018, 8, e022562. [Google Scholar] [CrossRef]
- Halse, K.G.; Lindegaard, M.L.; Goetze, J.P.; Damm, P.; Mathiesen, E.R.; Nielsen, L.B. Increased plasma pro-B-type natriuretic peptide in infants of women with type 1 diabetes. Clin. Chem. 2005, 51, 2296–2302. [Google Scholar] [CrossRef] [Green Version]
- Reid, R.A.; Prickett, T.C.; Pullar, B.E.; Darlow, B.A.; Gullam, J.E.; Espiner, E.A. C-type natriuretic peptide in complicated pregnancy: Increased secretion precedes adverse events. J. Clin. Endocrinol. Metab. 2014, 99, 1470–1478. [Google Scholar] [CrossRef] [Green Version]
- Bogacz, A.; Bartkowiak-Wieczorek, J.; Procyk, D.; Seremak-Mrozikiewicz, A.; Majchrzycki, M.; Dziekan, K.; Bienert, A.; Czerny, B. Analysis of the gene polymorphism of aldosterone synthase (CYP11B2) and atrial natriuretic peptide (ANP) in women with preeclampsia. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 197, 11–15. [Google Scholar] [CrossRef]
- Sordo, M.; Maciel-Ruiz, J.A.; Salazar, A.M.; Robles-Morales, R.; Veloz-Martinez, M.G.; Pacheco-Limon, J.H.; Nepomuceno-Hernandez, A.E.; Ayala-Yanez, R.; Gonsebatt, M.E.; Ostrosky-Wegman, P. Particulate matter-associated micronuclei frequencies in maternal and cord blood lymphocytes. Environ. Mol. Mutagen. 2019, 60, 421–427. [Google Scholar] [CrossRef]
- HaP, R.B. Applied Mixed Models in Medicine, 3rd ed.; Wiley: Hoboken, NJ, USA, 2001. [Google Scholar]
- WHO’s global air-quality guidelines. Lancet 2006, 368, 1302. [CrossRef]
- Rouatbi, H.; Zigabe, S.; Gkiougki, E.; Vranken, L.; Van Linthout, C.; Seghaye, M.C. Biomarkers of neonatal stress assessment: A prospective study. Early Hum. Dev. 2019, 137, 104826. [Google Scholar] [CrossRef] [PubMed]
- Prickett, T.C.R.; Darlow, B.A.; Troughton, R.W.; Cameron, V.A.; Elliott, J.M.; Martin, J.; Horwood, L.J.; Espiner, E.A. New Insights into Cardiac and Vascular Natriuretic Peptides: Findings from Young Adults Born with Very Low Birth Weight. Clin. Chem. 2018, 64, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Kanbe, T.; Maeno, Y.; Fujino, H.; Kanda, H.; Hirose, A.; Okada, J.; Morikawa, T.; Iwata, S.; Iwata, O.; Matsuishi, T. Brain-type natriuretic peptide at birth reflects foetal maturation and antenatal stress. Acta Paediatr. 2009, 98, 1421–1425. [Google Scholar] [CrossRef]
- Nir, A.; Bar-Oz, B.; Perles, Z.; Brooks, R.; Korach, A.; Rein, A.J. N-terminal pro-B-type natriuretic peptide: Reference plasma levels from birth to adolescence. Elevated levels at birth and in infants and children with heart diseases. Acta Paediatr. 2004, 93, 603–607. [Google Scholar] [CrossRef]
- Mannarino, S.; Garofoli, F.; Mongini, E.; Cerbo, R.M.; Codazzi, A.C.; Tzialla, C.; Mazzucchelli, I.; Perotti, G.; Tinelli, C.; De Silvestri, A.; et al. BNP concentrations and cardiovascular adaptation in preterm and fullterm newborn infants. Early Hum. Dev. 2010, 86, 295–298. [Google Scholar] [CrossRef]
- Chu, C.; Gui, Y.H.; Ren, Y.Y. Evaluation of cardiac function in fetuses from pregnant women with abnormal blood glucose levels by brain natriuretic peptide in umbilical cord blood. Zhongguo Dang Dai Er Ke Za Zhi 2009, 11, 805–808. [Google Scholar] [PubMed]
- Wellenius, G.A.; Yeh, G.Y.; Coull, B.A.; Suh, H.H.; Phillips, R.S.; Mittleman, M.A. Effects of ambient air pollution on functional status in patients with chronic congestive heart failure: A repeated-measures study. Environ. Health 2007, 6, 26. [Google Scholar] [CrossRef] [Green Version]
- Emiroglu, Y.; Kargin, R.; Kargin, F.; Akcakoyun, M.; Pala, S.; Mutlu, H.; Akcay, M.; Aung, S.M.; Baran, R.; Ozdemir, N. BNP levels in patients with long-term exposure to biomass fuel and its relation to right ventricular function. Pulm. Pharmacol. Ther. 2010, 23, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Caravedo, M.A.; Painschab, M.S.; Davila-Roman, V.G.; De Ferrari, A.; Gilman, R.H.; Vasquez-Villar, A.D.; Pollard, S.L.; Miranda, J.J.; Checkley, W.; Group, C.C.S. Lack of association between chronic exposure to biomass fuel smoke and markers of right ventricular pressure overload at high altitude. Am. Heart J. 2014, 168, 731–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Arifi, M.N.; Maayah, Z.H.; Alshamrani, A.A.; Korashy, H.M. Impact of cigarette smoke exposure on the expression of cardiac hypertrophic genes, cytochrome P450 enzymes, and oxidative stress markers in rats. J. Toxicol. Sci. 2012, 37, 1083–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cameron, V.A.; Ellmers, L.J. Minireview: Natriuretic peptides during development of the fetal heart and circulation. Endocrinology 2003, 144, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Houben, A.J.; van der Zander, K.; de Leeuw, P.W. Vascular and renal actions of brain natriuretic peptide in man: Physiology and pharmacology. Fundam. Clin. Pharmacol. 2005, 19, 411–419. [Google Scholar] [CrossRef]
- Volpe, M.; Carnovali, M.; Mastromarino, V. The natriuretic peptides system in the pathophysiology of heart failure: From molecular basis to treatment. Clin. Sci. 2016, 130, 57–77. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, R.; Ali, Y.; Hashizume, R.; Suzuki, N.; Ito, M. BNP as a Major Player in the Heart-Kidney Connection. Int. J. Mol. Sci. 2019, 20, 3581. [Google Scholar] [CrossRef] [Green Version]
- Stephenson, T.J.; Broughton Pipkin, F.; Hetmanski, D.; Yoxall, B. Atrial natriuretic peptide in the preterm newborn. Biol. Neonate 1994, 66, 22–32. [Google Scholar] [CrossRef]
- Vega, E.; Reyes, E.; Ruiz, H.; Garcia, J.; Sanchez, G.; Martinez-Villa, G.; Gonzalez, U.; Chow, J.C.; Watson, J.G. Analysis of PM2.5 and PM10 in the atmosphere of Mexico City during 2000-2002. J. Air Waste Manag. Assoc. 2004, 54, 786–798. [Google Scholar] [CrossRef] [Green Version]
- Capozzella, A.; Gioffre, P.A.; Chighine, A.; Sacco, C.; Casale, T.; Scala, B.; Palatiello, A.; Pimpinella, B.; Tomei, F.; Rosati, M.V. Occupational exposure to urban stressors and effects on atrial natriuretic peptide: Preliminary results. Ann. Ig. 2014, 26, 537–546. [Google Scholar]
- Chen, T.L.; Liao, J.W.; Chan, W.H.; Hsu, C.Y.; Yang, J.D.; Ueng, T.H. Induction of cardiac fibrosis and transforming growth factor-beta1 by motorcycle exhaust in rats. Inhal. Toxicol. 2013, 25, 525–535. [Google Scholar] [CrossRef] [PubMed]
- Moyes, A.J.; Hobbs, A.J. C-type Natriuretic Peptide: A Multifaceted Paracrine Regulator in the Heart and Vasculature. Int. J. Mol. Sci. 2019, 20, 2281. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | Total (n = 110) | Included (n = 51) | Excluded (n = 59) | p-Value |
|---|---|---|---|---|
| Maternal characteristics | ||||
| Age (years) | 27.00 (23.75–31.25) | 25.00 (23.00–30.00) | 29.00 (25.00–32.00) | 0.06 |
| Ocupation | ||||
| Yes | 52 (47.27) | 19 (37.26) | 33(55.93) | <0.001 |
| No | 50 (45.46) | 32 (62.75) | 18 (30.51) | |
| Smoking before pregnancy | ||||
| Yes | 19 (17.3) | 11 (21.57) | 8 (1.36) | 0.579 |
| No | 84 (76.36) | 40 (78.43) | 44 (74.6) | |
| Newborn characteristics | ||||
| Weight (g) | 3120 (2880–3450) | 3200 (3000–3460) | 3050 (2700–3450) | 0.19 |
| Height (cm) | 50.0 (49.00–51.50) | 50.00 (49.00–51.00) | 50.00 (49.00–52.00) | 0.86 |
| Sex | ||||
| Girls | 53 (48.18) | 23 (45.10) | 30 (50.85) | 0.71 |
| Boys | 54 (49.09) | 27 (52.94) | 27 (45.76) | |
| Capurro | 39.00 (38.00–40.00) | 39.00 (39.00–40.00) | 39.00 (38.00–40.00) | 0.062 |
| PM2.5 exposure (μg/m3) | ||||
| First trimester | 22.47 (18.79–25.49) | 20.15 (16.42–24.53) | 23.63 (19.86–27.50) | <0.001 |
| Second trimester | 23.32 (18.73–26.65) | 22.55 (17.36–24.90) | 24.13 (20.49–26.88) | 0.018 |
| Third trimester | 24.65 (18.39–27.74) | 24.85 (18.41–29.33) | 24.63 (18.47–26.55) | 0.40 |
| Whole Pregnancy | 22.63 (21.07–24.71) | 22.16 (20.37–22.74) | 24.43 (22.00–25.64) | <0.001 |
| PM10 exposure (μg/m3) | ||||
| First trimester | 39.26 (33.06–50.63) | 35.00 (29.35–47.14) | 45.85 (34.89–54.73) | <0.001 |
| Second trimester | 44.77 (34.14–49.41) | 42.44 (33.19–48.69) | 46.66 (34.55–54.30) | 0.19 |
| Third trimester | 44.73 (32.97–56.88) | 47.35 (32.22–57.11) | 42.25 (35.04–55.22) | 0.93 |
| Whole pregnancy | 42.58 (39.44–47.66) | 41.63 (38.44–43.10) | 46.63 (40.21–48.79) | 0.002 |
| ANP (pg/mL) | BNP (pg/mL) | CNP (pg/mL) | |
|---|---|---|---|
| N | 48 | 51 | 51 |
| Mean (Min–Max) | 67.78 (1.54–258.7) | 98.09 (39.23–279.60) | 1475 (5.76–7344.73) |
| Median and IQR | 66.71 (46.92–80.23) | 98.23 (73.64–112.30) | 1129.11 (944.10–1452.02) |
| Variables | ANP (pg/mL) | BNP (pg/mL) | CNP (pg/mL) | |||
|---|---|---|---|---|---|---|
| r | P | r | P | r | P | |
| Maternal characteristics | ||||||
| Age (years) | 0.04 | 0.81 | −0.03 | 0.85 | −0.05 | 0.72 |
| Newborn characteristics | ||||||
| Weight (g) | −0.16 | 0.28 | 0.19 | 0.17 | 0.08 | 0.58 |
| Height (cm) | −0.11 | 0.45 | 0.23 | 0.11 | 0.12 | 0.40 |
| Capurro | −0.14 | 0.33 | −5.1 × 10–4 | 0.99 | −0.14 | 0.33 |
| PM2.5 exposure (μg/m3) | ||||||
| First trimester | 0.10 | 0.48 | 0.11 | 0.44 | −0.08 | 0.58 |
| Second trimester | 0.30 | 0.04 | −0.25 | 0.08 | −0.01 | 0.94 |
| Third trimester | −0.32 | 0.03 | 0.11 | 0.43 | 0.07 | 0.61 |
| Whole pregnancy | −0.04 | 0.80 | −1.7 × 10−3 | 0.99 | −0.03 | 0.86 |
| PM10 exposure (μg/m3) | ||||||
| First trimester | 0.17 | 0.24 | 0.12 | 0.41 | −0.06 | 0.68 |
| Second trimester | 0.26 | 0.07 | −0.27 | 0.05 | 0.07 | 0.62 |
| Third trimester | −0.39 | 0.01 | 0.11 | 0.46 | 0.03 | 0.84 |
| Whole pregnancy | −0.004 | 0.98 | −0.13 | 0.35 | 0.09 | 0.55 |
| PM2.5 First Trimester | PM2.5 Second Trimester | PM2.5 Third Trimester | PM2.5 Whole Pregnancy | |
|---|---|---|---|---|
| BNP (pg/mL) | β (95% Cl) | β (95% Cl) | β (95% Cl) | β (95% Cl) |
| Model 1 | 1.05 (−1.17, 3.26) | −2.59 (−4.82, −0.36) | 0.66 (−0.95, 2.28) | −0.06 (−5.89, 5.77) |
| Model 2 | 0.97 (−1.29, 3.23) | −2.76 (−5.02, −0.50) | 0.603 (−1.05, 2.25) | −1.05 (−7.61, 5.52) |
| Model 3 | 0.70 (−1.51, 2.90) | −2.65 (−4.83, −0.47) | 0.53 (−1.06, 2.12) | −1.94 (−8.31, 4.42) |
| Model 4 | 0.58 (−1.62, 2.77) | −2.47 (−4.67, −0.27) | 0.63 (−0.95, 2.21) | −1.23 (−7.65, 5.18) |
| CNP (pg/mL) | ||||
| Model 1 | 5.65 (−69.2, 80.50) | 2.27 (−76.65, 81.20) | −1.47 (−55.86, 52.93) | 11.16 (−184.03, 206.34) |
| Model 2 | −3.27 (−77.96, 71.42) | −7.07 (−85.77, 71.63) | −8.22 (−62.5, 46.03) | −69.83 (−284.14, 144.54) |
| Model 3 | −3.02 (−79.12, 73.09) | −7.21 (−86.90, 72.48) | −8.16 (−63.09, 46.76) | −70.04 (−288.69, 148.60) |
| Model 4 | −2.03 (−79.21, 75.16) | −9.30 (−90.71, 72.12) | −8.99 (−64.70, 46.72) | −78.40 (−302.49, 145.69) |
| ANP (pg/mL) | ||||
| Model 1 | 0.19 (−2.33, 2.70) | 2.14 (−0.44, 4.72) | −1.32 (−3.02, 0.39) | −1.43 (−8.08, 5.22) |
| Model 2 | 0.30 (−2.26, 2.87) | 2.27 (−0.33, 4.88) | −1.27 (−3.03, 0.49) | −0.64 (−8.40, 7.08) |
| Model 3 | 0.45 (−2.08, 2.99) | 2.13 (−0.47, 4.72) | −1.20 (−2.94, 0.54) | −0.25 (−7.88, 7.39) |
| Model 4 | 0.47 (−2.14, 3.07) | 2.15 (−0.49, 4.78) | −1.22 (−3.0, 0.55) | −0.25 (−8.01, 7.52) |
| PM10 First Trimester | PM10 Second Trimester | PM10 Third Trimester | PM10 Whole Pregnancy | |
|---|---|---|---|---|
| BNP (pg/mL) | β (95% Cl) | β (95% Cl) | β (95% Cl) | β (95% Cl) |
| Model 1 | 0.23 (−0.74, 1.21) | −1.32 (−2.46,−0.17) | 0.30 (−0.52, 1.11) | −0.48 (−3.06, 2.09) |
| Model 2 | 0.20 (−0.79, 1.19) | −1.43 (−2.60, −0.27) | 0.27 (−0.57, 1.10) | −0.94 (−3.76, 1.88) |
| Model 3 | 0.06 (−0.91, 1.03) | −1.41 (−2.53, −0.29) | 0.20 (−0.60, 1.01) | −1.59 (−4.34, 1.16) |
| Model 4 | 0.03 (−0.93, 0.99) | −1.30 (−2.44, −0.17) | 0.24 (−0.56, 1.04) | −1.29 (−4.07, 1.50) |
| CNP (pg/mL) | ||||
| Model 1 | 12.15 (−20.4, 44.65) | 8.11 (−32.29, 48.52) | −3.51 (−30.95, 23.93) | 28.93 (−56.94, 114.80) |
| Model 2 | 9.0 (−23.41, 41.42) | 2.48 (−38.12, 43.07) | −6.68 (−33.97, 20.60) | 3.12 (−89.6, 95.9) |
| Model 3 | 9.33 (−23.8, 42.43) | 2.45 (−38.62, 43.52) | −6.65 (−34.33, 21.03) | 3.91 (−91.9, 99.72) |
| Model 4 | 9.57 (−23.9, 43.04) | 1.29 (−40.93, 43.51) | −6.99 (−35.03, 21.04) | 1.16 (−97.3, 96.4) |
| ANP (pg/mL) | ||||
| Model 1 | 0.52 (−0.63, 1.70) | 0.93 (−0.39, 2.24) | −0.96 (−1.80, −0.12) | −0.96 (−3.96, 2.03) |
| Model 2 | 0.56 (−0.60, 1.73) | 1.01 (−0.33, 2.35) | −0.95 (−1.81, −0.08) | −0.73 (−4.07, 2.62) |
| Model 3 | 0.65 (−0.49, 1.80) | 0.96 (−0.36, 2.28) | −0.90 (−1.76, −0.04) | −0.35 (−3.70, 2.99) |
| Model 4 | 0.67 (−0.51, 1.84) | 0.98 (−0.37, 2.34) | −0.90 (−1.80, −0.03) | −0.36 (−3.80, 3.05) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Rodríguez, A.; Maciel-Ruiz, J.A.; Salazar, A.M.; Sordo, M.; Ostrosky-Wegman, P.; Limón-Pacheco, J.H.; Nepomuceno-Hernández, A.E.; Ayala-Yáñez, R.; Gonsebatt, M.E.; Osorio-Yáñez, C. Prenatal Particulate Matter (PM) Exposure and Natriuretic Peptides in Newborns from Mexico City. Int. J. Environ. Res. Public Health 2021, 18, 6546. https://doi.org/10.3390/ijerph18126546
Muñoz-Rodríguez A, Maciel-Ruiz JA, Salazar AM, Sordo M, Ostrosky-Wegman P, Limón-Pacheco JH, Nepomuceno-Hernández AE, Ayala-Yáñez R, Gonsebatt ME, Osorio-Yáñez C. Prenatal Particulate Matter (PM) Exposure and Natriuretic Peptides in Newborns from Mexico City. International Journal of Environmental Research and Public Health. 2021; 18(12):6546. https://doi.org/10.3390/ijerph18126546
Chicago/Turabian StyleMuñoz-Rodríguez, Abigail, Jorge Alfonso Maciel-Ruiz, Ana María Salazar, Monserrat Sordo, Patricia Ostrosky-Wegman, Jorge H. Limón-Pacheco, Andrés Eduardo Nepomuceno-Hernández, Rodrigo Ayala-Yáñez, María Eugenia Gonsebatt, and Citlalli Osorio-Yáñez. 2021. "Prenatal Particulate Matter (PM) Exposure and Natriuretic Peptides in Newborns from Mexico City" International Journal of Environmental Research and Public Health 18, no. 12: 6546. https://doi.org/10.3390/ijerph18126546