
Stigmatization from Work-Related COVID-19 Exposure: A Systematic Review with Meta-Analysis

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Review Questions and Study Eligibility Criteria
2.2. Definition of Stigma Forms
2.3. Information Sources and Search
2.4. Study Selection and Data Collection
2.5. Rating of Methodological Study Quality (Risk of Bias)
2.6. Synthesis of Results and Meta-Analysis
3. Results
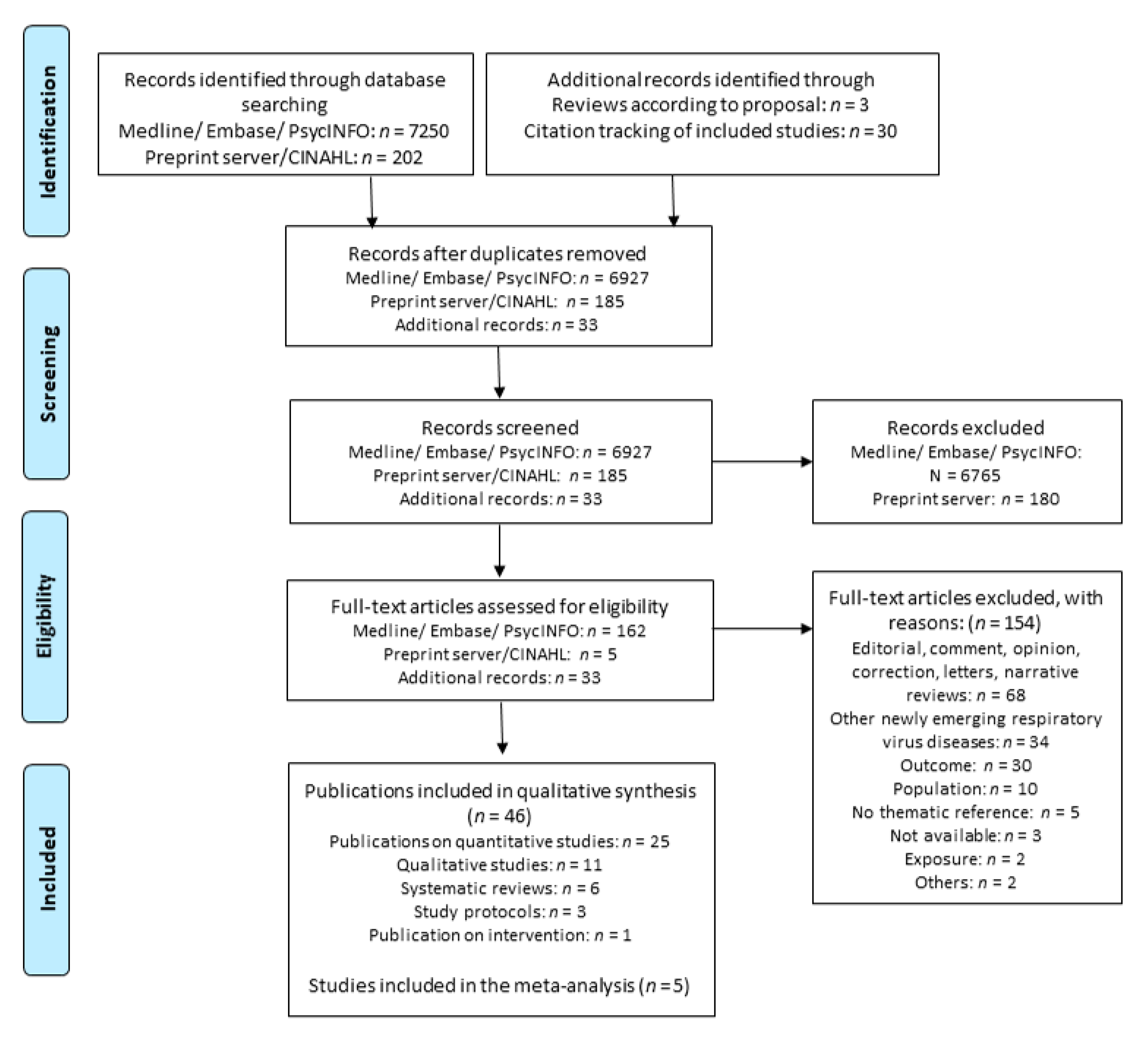
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Systematic Reviews
3.2.2. Quantitative Studies
3.2.3. Qualitative Studies
3.2.4. Intervention
3.2.5. Study Protocols
3.3. Prevalance of Stigmatization with Regard to Occupational Group
3.3.1. Quantitative Studies
3.3.2. Qualitative Studies
3.4. Stigmatization from Work-Related COVID-19 Exposure and Health
3.4.1. Descriptive Summary
3.4.2. Synthesis of Results
3.5. Measures to Prevent Work-Related Stigmatization from COVID-19
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Naeem, S.B.; Bhatti, R. The Covid-19 ’infodemic’: A new front for information professionals. Health Inf. Libr. J. 2020, 37, 233–239. [Google Scholar] [CrossRef] [PubMed]
- SPIEGEL. Menschen Werfen uns Offenbar vor, wir Hätten die Krankheit ins Dorf Gebracht. Available online: https://www.spiegel.de/psychologie/stigma-coronavirus-wie-covid-19-die-beziehung-zu-freunden-und-kollegen-veraendern-kann-a-d76839ad-d25b-4063-8f55-884bc86824cf (accessed on 7 September 2020).
- Heute, Z. Die Angst vor der Wut der Mitmenschen. Available online: https://www.zdf.de/nachrichten/panorama/corona-stigma-angst-wut-mitmenschen-100.html (accessed on 27 May 2020).
- Link, B.G.; Phelan, J.C. Conceptualizing stigma. Annu. Rev. Sociol. 2001, 27, 363–385. [Google Scholar] [CrossRef]
- Pescosolido, B.A.; Martin, J.K. The stigma complex. Annu. Rev. Sociol. 2015, 41, 87–116. [Google Scholar] [CrossRef] [Green Version]
- Corrigan, P.W.; Larson, J.E.; Kuwabara, S.A. Social psychology of the stigma of mental illness: Public and self-stigma models. In Social Psychological Foundations of Clinical Psychology; The Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Pryor, J.B.; Reeder, G.D.; Monroe, A.E. The infection of bad company: Stigma by association. J. Personal. Soc. Psychol. 2012, 102, 224. [Google Scholar] [CrossRef] [Green Version]
- Berger, B.E.; Ferrans, C.E.; Lashley, F.R. Measuring stigma in people with HIV: Psychometric assessment of the HIV stigma scale. Res. Nurs. Health 2001, 24, 518–529. [Google Scholar] [CrossRef]
- Quinn, D.M.; Chaudoir, S.R. Living with a concealable stigmatized identity: The impact of anticipated stigma, centrality, salience, and cultural stigma on psychological distress and health. J. Personal. Soc. Psychol. 2009, 97, 634. [Google Scholar] [CrossRef] [Green Version]
- Corrigan, P.W.; Watson, A.C.; Barr, L. The self–stigma of mental illness: Implications for self–esteem and self–efficacy. J. Soc. Clin. Psychol. 2006, 25, 875–884. [Google Scholar] [CrossRef]
- van der Sanden, R.L.; Stutterheim, S.E.; Pryor, J.B.; Kok, G.; Bos, A.E. Coping with stigma by association and family burden among family members of people with mental illness. J. Nerv. Ment. Dis. 2014, 202, 710–717. [Google Scholar] [CrossRef] [Green Version]
- Einarsen, S.; Hoel, H.; Zapf, D.; Cooper, C. Bullying and Emotional Abuse in the Workplace; Taylor & Francis London & New York: London, UK; New York, NY, USA, 2002. [Google Scholar]
- Östman, M.; Kjellin, L. Stigma by association: Psychological factors in relatives of people with mental illness. Br. J. Psychiatry 2002, 181, 494–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mooney, S.J.; El-Sayed, A.M. Stigma and the etiology of depression among the obese: An agent-based exploration. Soc. Sci. Med. 2016, 148, 1–7. [Google Scholar] [CrossRef]
- Carpiniello, B.; Pinna, F. The reciprocal relationship between suicidality and stigma. Front. Psychiatry 2017, 8, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schomerus, G.; Angermeyer, M. Stigma and its impact on help-seeking for mental disorders: What do we know? Epidemiol. Psychiatr. Sci. 2008, 17, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Yebei, V.N.; Fortenberry, J.; Ayuku, D.O. Felt stigma among people living with HIV/AIDS in rural and urban Kenya. Afr. Health Sci. 2008, 8, 97–102. [Google Scholar] [PubMed]
- Deitch, E.A.; Barsky, A.; Butz, R.M.; Chan, S.; Brief, A.P.; Bradley, J.C. Subtle yet significant: The existence and impact of everyday racial discrimination in the workplace. Hum. Relat. 2003, 56, 1299–1324. [Google Scholar] [CrossRef]
- Weber, J.; Angerer, P.; Müller, A. Individual consequences of age stereotypes on older workers. Z. Für Gerontol. Und Geriatr. 2019, 52, 188–205. [Google Scholar] [CrossRef]
- von Kardorff, E. Zur Diskriminierung psychisch kranker Menschen. In Diskriminierung; Springer: Berlin/Heidelberg, Germany, 2010; pp. 279–305. [Google Scholar]
- Bartlett, J.E.; Bartlett, M.E. Workplace bullying: An integrative literature review. Adv. Dev. Hum. Resour. 2011, 13, 69–84. [Google Scholar] [CrossRef]
- Leymann, H. The content and development of mobbing at work. Eur. J. Work Organ. Psychol. 1996, 5, 165–184. [Google Scholar] [CrossRef]
- Zapf, D. Mobbing in Organisationen. Ein Überblick zum Stand der Forschung [Bullying at work. An overview of current research]. Z. Für Arb. Organ. 1999, 43, 1–25. [Google Scholar]
- Einarsen, S. The nature and causes of bullying at work. Int. J. Manpow. 1999, 20, 16–27. [Google Scholar] [CrossRef]
- Kisely, S.; Warren, N.; McMahon, L.; Dalais, C.; Henry, I.; Siskind, D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: Rapid review and meta-analysis. BMJ 2020, 369, m1642. [Google Scholar] [CrossRef]
- Serrano-Ripoll, M.J.; Meneses-Echavez, J.F.; Ricci-Cabello, I.; Fraile-Navarro, D.; Fiol-deRoque, M.A.; Pastor-Moreno, G.; Castro, A.; Ruiz-Perez, I.; Zamanillo Campos, R.; Goncalves-Bradley, D.C. Impact of viral epidemic outbreaks on mental health of healthcare workers: A rapid systematic review and meta-analysis. J. Affect. Disord. 2020, 277, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Paiano, M.; Jaques, A.E.; Nacamura, P.A.B.; Salci, M.A.; Radovanovic, C.A.T.; Carreira, L. Mental health of healthcare professionals in China during the new coronavirus pandemic: An integrative review. Rev. Bras. De Enferm. 2020, 73, e20200338. [Google Scholar] [CrossRef]
- Cabarkapa, S.; Nadjidai, S.E.; Murgier, J.; Ng, C.H. The psychological impact of COVID-19 and other viral epidemics on frontline healthcare workers and ways to address it: A rapid systematic review. Brain Behav. Immun. Health 2020, 8, 100144. [Google Scholar] [CrossRef]
- Muhidin, S.; Vizheh, M.; Moghadam, Z.B. Anticipating COVID-19-related stigma in survivors and health-care workers: Lessons from previous infectious diseases outbreaks—An integrative literature review. Psychiatry Clin. Neurosci. 2020. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, D.; Vaishnav, M.; Sathyanarayana Rao, T.S.; Raju, M.S.V.K.; Dalal, P.K.; Javed, A.; Saha, G.; Mishra, K.K.; Kumar, V.; Jagiwala, M.P. Impact of the COVID-19 pandemic on psychosocial health and well-being in South-Asian (World Psychiatric Association zone 16) countries: A systematic and advocacy review from the Indian Psychiatric Society. Indian J. Psychiatry 2020, 62, S343–S353. [Google Scholar] [CrossRef]
- Tng, X.J.J.; Chew, Q.H.; Sim, K. Psychological sequelae within different populations during the COVID-19 pandemic: A rapid review of extant evidence. Singap. Med. J. 2020. [Google Scholar] [CrossRef] [PubMed]
- De Brier, N.; Stroobants, S.; Vandekerckhove, P.; De Buck, E. Factors affecting mental health of health care workers during coronavirus disease outbreaks (SARS, MERS & COVID-19): A rapid systematic review. PLoS ONE 2020, 15, e0244052. [Google Scholar]
- Muller, R.A.E.; Stensland, R.S.Ø.; van de Velde, R.S. The mental health impact of the covid-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. Psychiatry Res. 2020, 293, 113441. [Google Scholar] [CrossRef]
- Sritharan, J.; Jegathesan, T.; Vimaleswaran, D.; Sritharan, A. Mental Health Concerns of Frontline Workers During the COVID-19 Pandemic: A Scoping Review. Glob. J. Health Sci. 2020, 12, 89–105. [Google Scholar] [CrossRef]
- Taylor, S.; Landry, C.A.; Rachor, G.S.; Paluszek, M.M.; Asmundson, G.J. Fear and avoidance of healthcare workers: An important, under-recognized form of stigmatization during the COVID-19 pandemic. J. Anxiety Disord. 2020, 75, 102289. [Google Scholar] [CrossRef] [PubMed]
- Dang, A.K.; Le, X.T.T.; Le, H.T.; Tran, B.X.; Do, T.T.T.; Phan, H.T.B.; Nguyen, T.T.; Pham, Q.T.; Ta, N.T.K.; Nguyen, Q.T. Evidence of COVID-19 impacts on occupations during the first Vietnamese national Lockdown. Ann. Glob. Health 2020, 86, 112. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, F.A.; Ahmad, B.; Ahmad, P.; Khalid, M.D.; Butt, D.Q.; Khan, S.Q. Concerns, perceived impact, and preparedness of oral healthcare workers in their working environment during COVID-19 pandemic. J. Occup. Health 2020, 62, e12168. [Google Scholar] [CrossRef] [PubMed]
- Mohindra, R.; Soni, R.K.; Suri, V.; Bhalla, A.; Singh, S.M. The experience of social and emotional distancing among health care providers in the context of COVID-19: A study from North India. J. Hum. Behav. Soc. Environ. 2020, 31, 173–183. [Google Scholar] [CrossRef]
- Chew, Q.H.; Chia, F.L.-A.; Ng, W.K.; Lee, W.C.I.; Tan, P.L.L.; Wong, C.S.; Puah, S.H.; Shelat, V.G.; Seah, E.-J.D.; Huey, C.W.T. Perceived Stress, Stigma, Traumatic Stress Levels and Coping Responses amongst Residents in Training across Multiple Specialties during COVID-19 Pandemic—A Longitudinal Study. Int. J. Environ. Res. Public Health 2020, 17, 6572. [Google Scholar] [CrossRef] [PubMed]
- Do Duy, C.; Nong, V.M.; Van, A.N.; Thu, T.D.; Do Thu, N.; Quang, T.N. COVID-19 related stigma and its association with mental health of health-care workers after quarantined in Vietnam. Psychiatry Clin. Neurosci. 2020, 74, 566–568. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Xu, S.; Wang, H.; Liu, Z.; Wu, J.; Li, G.; Miao, J.; Zhang, C.; Yang, Y.; Sun, W. COVID-19 in Wuhan: Sociodemographic characteristics and hospital support measures associated with the immediate psychological impact on healthcare workers. EClinicalMedicine 2020, 24, 100443. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement For Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Ijaz, S.; Verbeek, J.; Seidler, A.; Lindbohm, M.-L.; Ojajärvi, A.; Orsini, N.; Costa, G.; Neuvonen, K. Night-shift work and breast cancer—A systematic review and meta-analysis. Scand. J. Work Environ. Health 2013, 431–447. [Google Scholar] [CrossRef]
- Kuijer, P.P.F.; Verbeek, J.H.; Seidler, A.; Ellegast, R.; Hulshof, C.T.; Frings-Dresen, M.H.; Van der Molen, H.F. Work-relatedness of lumbosacral radiculopathy syndrome: Review and dose-response meta-analysis. Neurology 2018, 91, 558–564. [Google Scholar] [CrossRef]
- Romero Starke, K.; Kofahl, M.; Freiberg, A.; Schubert, M.; Groß, M.L.; Schmauder, S.; Hegewald, J.; Kämpf, D.; Stranzinger, J.; Nienhaus, A. Are Daycare Workers at a Higher Risk of Parvovirus B19 Infection? A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 1392. [Google Scholar] [CrossRef] [Green Version]
- Callus, E.; Bassola, B.; Fiolo, V.; Bertoldo, E.G.; Pagliuca, S.; Lusignani, M. Stress Reduction Techniques for Health Care Providers Dealing With Severe Coronavirus Infections (SARS, MERS, and COVID-19): A Rapid Review. Front. Psychol. 2020, 11, 3325. [Google Scholar] [CrossRef] [PubMed]
- Joo, J.Y.; Liu, M.F. Nurses’ barriers to caring for patients with COVID-19: A qualitative systematic review. Int. Nurs. Rev. 2021. [Google Scholar] [CrossRef]
- Rahman, M.; Ahmed, R.; Moitra, M.; Damschroder, L.; Brownson, R.; Chorpita, B.; Idele, P.; Gohar, F.; Huang, K.Y.; Saxena, S. Mental Distress and Human Rights Violations During COVID-19: A Rapid Review of the Evidence Informing Rights, Mental Health Needs, and Public Policy Around Vulnerable Populations. Front. Psychiatry 2020, 11, 603875. [Google Scholar] [CrossRef]
- Blake, H.; Bermingham, F.; Johnson, G.; Tabner, A. Mitigating the psychological impact of covid-19 on healthcare workers: A digital learning package. Int. J. Environ. Res. Public Health 2020, 17, 2997. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.S.; Bhattacharyya, R.; Bhattacharyya, S.; Gupta, S.; Das, S.; Banerjee, B.B. Attitude, practice, behavior, and mental health impact of COVID-19 on doctors. Indian J. Psychiatry 2020, 62, 257. [Google Scholar]
- Juan, Y.; Yuanyuan, C.; Qiuxiang, Y.; Cong, L.; Xiaofeng, L.; Yundong, Z.; Jing, C.; Peifeng, Q.; Yan, L.; Xiaojiao, X.; et al. Psychological distress surveillance and related impact analysis of hospital staff during the COVID-19 epidemic in Chongqing, China. Compr. Psychiatry 2020, 103, 152198. [Google Scholar] [CrossRef] [PubMed]
- Kackin, O.; Ciydem, E.; Aci, O.S.; Kutlu, F.Y. Experiences and psychosocial problems of nurses caring for patients diagnosed with COVID-19 in Turkey: A qualitative study. Int. J. Soc. Psychiatry 2020, 20764020942788. [Google Scholar] [CrossRef]
- Kalateh Sadati, A.; Zarei, L.; Shahabi, S.; Heydari, S.T.; Taheri, V.; Jiriaei, R.; Ebrahimzade, N.; Lankarani, K.B. Nursing experiences of COVID-19 outbreak in Iran: A qualitative study. Nurs. Open 2021, 8, 72–79. [Google Scholar] [CrossRef]
- Abdel Wahed, W.Y.; Hefzy, E.M.; Ahmed, M.I.; Hamed, N.S. Assessment of Knowledge, Attitudes, and Perception of Health Care Workers Regarding COVID-19, A Cross-Sectional Study from Egypt. J. Community Health 2020. [Google Scholar] [CrossRef]
- Chew, Q.H.; Wei, K.C.; Vasoo, S.; Sim, K. Psychological and Coping Responses of Health Care Workers Toward Emerging Infectious Disease Outbreaks: A Rapid Review and Practical Implications for the COVID-19 Pandemic. J. Clin. Psychiatry 2020, 81. [Google Scholar] [CrossRef]
- Fawaz, M.; Samaha, A. The psychosocial effects of being quarantined following exposure to COVID-19: A qualitative study of Lebanese health care workers. Int. J. Soc. Psychiatry 2020, 66, 560–565. [Google Scholar] [CrossRef]
- Dye, T.D.; Alcantara, L.; Siddiqi, S.; Barbosu, M.; Sharma, S.; Panko, T.; Pressman, E. Risk of COVID-19-related bullying, harassment and stigma among healthcare workers: An analytical cross-sectional global study. BMJ Open 2020, 10, e046620. [Google Scholar] [CrossRef]
- Elhadi, M.; Msherghi, A.; Elgzairi, M.; Alhashimi, A.; Bouhuwaish, A.; Biala, M.; Abuelmeda, S.; Khel, S.; Khaled, A.; Alsoufi, A. Burnout Syndrome Among Hospital Healthcare Workers During the COVID-19 Pandemic and Civil War: A Cross-Sectional Study. Front. Psychiatry 2020, 11, 1426. [Google Scholar] [CrossRef]
- Elhadi, M.; Msherghi, A.; Elgzairi, M.; Alhashimi, A.; Bouhuwaish, A.; Biala, M.; Abuelmeda, S.; Khel, S.; Khaled, A.; Alsoufi, A.; et al. Psychological status of healthcare workers during the civil war and COVID-19 pandemic: A cross-sectional study. J. Psychosom. Res. 2020, 137, 110221. [Google Scholar] [CrossRef]
- Greene, T.; Harju-Seppänen, J.; Adeniji, M.; Steel, C.; Grey, N.; Brewin, C.R.; Bloomfield, M.A.; Billings, J. Predictors of PTSD, depression and anxiety in UK frontline health and social care workers during COVID-19. Eur. J. Psychotraumatol. 2020, 12, 1882781. [Google Scholar] [CrossRef] [PubMed]
- Khanal, P.; Devkota, N.; Dahal, M.; Paudel, K.; Joshi, D. Mental health impacts among health workers during COVID-19 in a low resource setting: A cross-sectional survey from Nepal. Glob. Health 2020, 16, 89. [Google Scholar] [CrossRef] [PubMed]
- Khanal, P.; Devkota, N.; Dahal, M.; Paudel, K.; Mishra, S.R.; Joshi, D. Corona virus fear among health workers during the early phase of pandemic response in Nepal: A web-based cross-sectional study. bioRxiv 2020. [Google Scholar] [CrossRef]
- Monterrosa-Castro, A.; Redondo-Mendoza, V.; Mercado-Lara, M. Psychosocial factors associated with symptoms of generalized anxiety disorder in general practitioners during the COVID-19 pandemic. J. Investig. Med. Off. Publ. Am. Fed. Clin. Res. 2020. [Google Scholar] [CrossRef]
- Ramaci, T.; Barattucci, M.; Ledda, C.; Rapisarda, V. Social Stigma during COVID-19 and its impact on HCWs outcomes. Sustainability 2020, 12, 3834. [Google Scholar] [CrossRef]
- Sharma, M.; Creutzfeldt, C.J.; Lewis, A.; Patel, P.V.; Hartog, C.; Jannotta, G.E.; Blissitt, P.; Kross, E.K.; Kassebaum, N.; Greer, D.M.; et al. Healthcare professionals’ perceptions of critical care resource availability and factors associated with mental well-being during COVID-19: Results from a US survey. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020. [Google Scholar] [CrossRef]
- Tan, W.; Hao, F.; McIntyre, R.S.; Jiang, L.; Jiang, X.; Zhang, L.; Zhao, X.; Zou, Y.; Hu, Y.; Luo, X. Is returning to work during the COVID-19 pandemic stressful? A study on immediate mental health status and psychoneuroimmunity prevention measures of Chinese workforce. Brain Behav. Immun. 2020, 87, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Uvais, N.A.; Aziz, F.; Hafeeq, B. COVID-19-Related Stigma and Perceived Stress among Dialysis Staff; Springer: New York City, NY, USA, 2020. [Google Scholar]
- Uvais, N.A.; Shihabudheen, P.; Hafi, N.A.B. Perceived Stress and Stigma Among Doctors Working in COVID-19-Designated Hospitals in India. Prim. Care Companion CNS Disord. 2020, 22. [Google Scholar] [CrossRef]
- Yadav, K.; Laskar, A.R.; Rasania, S. A study on stigma and apprehensions related to COVID-19 among healthcare professionals in Delhi. Int. J. Community Med. Public Health 2020, 7, 4547. [Google Scholar] [CrossRef]
- Said, R.M.; El-Shafei, D.A. Occupational stress, job satisfaction, and intent to leave: Nurses working on front lines during COVID-19 pandemic in Zagazig City, Egypt. Environ. Sci. Pollut. Res. 2021, 28, 8791–8801. [Google Scholar] [CrossRef]
- Zandifar, A.; Badrfam, R.; Khonsari, N.M.; Mohammadi, M.R.; Asayesh, H.; Qorbani, M. Prevalence and associated factors of posttraumatic stress symptoms and stigma among health care workers in contact with COVID-19 patients. Iran. J. Psychiatry 2020, 15, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Gao, H.; Zou, Y.; Lin, F. Changes in psychological wellbeing, attitude, and information-seeking behavior among people at the epicenter of the COVID-19 pandemic: A panel survey of residents in Hubei province, China. Epidemiol. Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- Abedi, V.; Olulana, O.; Avula, V.; Chaudhary, D.; Khan, A.; Shahjouei, S.; Li, J.; Zand, R. Racial, Economic, and Health Inequality and COVID-19 Infection in the United States. J. Racial Ethn. Health Disparities 2020. [Google Scholar] [CrossRef]
- McMahon, S.A.; Ho, L.S.; Brown, H.; Miller, L.; Ansumana, R.; Kennedy, C.E. Healthcare providers on the frontlines: A qualitative investigation of the social and emotional impact of delivering health services during Sierra Leone’s Ebola epidemic. Health Policy Plan. 2016, 31, 1232–1239. [Google Scholar] [CrossRef] [Green Version]
- See, L.-C.; Shen, Y.-M.; Chen, C.-L.; Huang, T.-M.; Huang, Y.-H.; Huang, H.-C.; Lin, S.-R. Professional attitude of health care workers toward serving HIV/AIDS patients and drug users: Questionnaire design and evaluation of reliability and validity. AIDS Care 2011, 23, 1448–1455. [Google Scholar] [CrossRef]
- Reazee, N.; Mardani-Hamooleh, M.; Seraji, M. Nurses’ perception of ethical challenges in caring for patients with COVID-19: A qualitative analysis. J. Med. Ethics Hist. Med. 2020, 13, 23. [Google Scholar]
- Rizvi Jafree, S.; ul Momina, A.; Naqi, S.A. Significant other family members and their experiences of COVID-19 in Pakistan: A qualitative study with implications for social policy. Stigma Health 2020. [Google Scholar] [CrossRef]
- Feroz, A.S.; Pradhan, N.A.; Ahmed, Z.H.; Shah, M.M.; Asad, N.; Saleem, S.; Siddiqi, S. The Perceptions and Experiences of Health-Care Providers During COVID-19 Pandemic in Karachi, Pakistan: An Exploratory Qualitative Study. Pak. An Explor. Qual. Study (6/22/2020) 2020. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3634827 (accessed on 15 April 2021).
- Crowe, S.; Howard, A.F.; Vanderspank-Wright, B.; Gillis, P.; McLeod, F.; Penner, C.; Haljan, G. The effect of COVID-19 pandemic on the mental health of Canadian critical care nurses providing patient care during the early phase pandemic: A mixed method study. Intensive Crit. Care Nurs. 2020, 63, 102999. [Google Scholar] [CrossRef]
- Hien, W.; von Schwarzkopf, H. Corona-Gefährdung im Erleben von Pflegekräften–Eine Explorative Studiemit Hinweisen auf Erweiterte Gesundheitsschutzkonzepte; Berufsgenossenschaft für Gesundheitsdienst und Wohlfahrtspflege: Bremen, Germany; p. 2020.
- Bhatt, N.; Bhatt, B.; Gurung, S.; Dahal, S.; Jaishi, A.R.; Neupane, B.; Budhathoki, S.S. Perceptions and experiences of the public regarding the COVID-19 pandemic in Nepal: A qualitative study using phenomenological analysis. BMJ Open 2020, 10, e043312. [Google Scholar] [CrossRef]
- Lee, N.; Lee, H.-J. South Korean Nurses’ Experiences with Patient Care at a COVID-19-Designated Hospital: Growth after the Frontline Battle against an Infectious Disease Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 9015. [Google Scholar] [CrossRef]
- Zolnikov, T.R.; Furio, F. Stigma on first responders during COVID-19. Stigma Health 2020, 5, 375–379. [Google Scholar] [CrossRef]
- Jesus, T.S.; Kamalakannan, S.; Bhattacharjya, S.; Bogdanova, Y.; Arango-Lasprilla, J.; Bentley, J.; Gibson, B.E.; Papadimitriou, C. People with disabilities and other forms of vulnerability to the COVID-19 pandemic: Study protocol for a scoping review and thematic analysis. Arch. Rehabil. Res. Clin. Transl. 2020, 2, 100079. [Google Scholar] [CrossRef] [PubMed]
- Nochaiwong, S.; Ruengorn, C.; Awiphan, R.; Ruanta, Y.; Boonchieng, W.; Nanta, S.; Kowatcharakul, W.; Pumpaisalchai, W.; Kanjanarat, P.; Mongkhon, P.; et al. Mental health circumstances among health care workers and general public under the pandemic situation of COVID-19 (HOME-COVID-19). Medicine 2020, 99, e20751. [Google Scholar] [CrossRef] [PubMed]
- Mongkhon, P.; Ruengorn, C.; Awiphan, R.; Thavorn, K.; Hutton, B.; Wongpakaran, N.; Wongpakaran, T.; Nochaiwong, S. Exposure to COVID-19-Related Information and its Association With Mental Health Problems in Thailand: Nationwide, Cross-sectional Survey Study. J. Med. Internet Res. 2021, 23, e25363. [Google Scholar] [CrossRef] [PubMed]
- Ruengorn, C.; Awiphan, R.; Wongpakaran, N.; Wongpakaran, T.; Nochaiwong, S.; Outcomes, H.; Health Outcomes and Mental Health Care Evaluation Survey Research Group. Association of job loss, income loss, and financial burden with adverse mental health outcomes during coronavirus disease 2019 pandemic in Thailand: A nationwide cross-sectional study. Depress. Anxiety 2021, 38, 648–660. [Google Scholar] [CrossRef]
- Sulaiman, A.H.; Ahmad Sabki, Z.; Jaafa, M.J.; Francis, B.; Razali, K.A.; Juares Rizal, A.; Mokhtar, N.H.; Juhari, J.A.; Zainal, S.; Ng, C.G. Development of a Remote Psychological First Aid Protocol for Healthcare Workers Following the COVID-19 Pandemic in a University Teaching Hospital, Malaysia. Healthcare 2020, 8, 228. [Google Scholar] [CrossRef] [PubMed]
- Newheiser, A.-K.; Barreto, M. Hidden costs of hiding stigma: Ironic interpersonal consequences of concealing a stigmatized identity in social interactions. J. Exp. Soc. Psychol. 2014, 52, 58–70. [Google Scholar] [CrossRef] [Green Version]
- Bos, A.E.; Kanner, D.; Muris, P.; Janssen, B.; Mayer, B. Mental illness stigma and disclosure: Consequences of coming out of the closet. Issues Ment. Health Nurs. 2009, 30, 509–513. [Google Scholar] [CrossRef]
- Topkaya, N. Gender, Self-Stigma, and Public Stigma in Predicting Attitudes toward Psychological Help-Seeking. Educ. Sci. Theory Pract. 2014, 14, 480–487. [Google Scholar] [CrossRef]
- Kulesza, M.; Raguram, R.; Rao, D. Perceived mental health related stigma, gender, and depressive symptom severity in a psychiatric facility in South India. Asian J. Psychiatry 2014, 9, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, K.M.; Christensen, H.; Jorm, A.F. Predictors of depression stigma. BMC Psychiatry 2008, 8, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreiner, G.E.; Ashforth, B.E.; Sluss, D.M. Identity dynamics in occupational dirty work: Integrating social identity and system justification perspectives. Organ. Sci. 2006, 17, 619–636. [Google Scholar] [CrossRef]
- Mejia, C.; Pittman, R.; Beltramo, J.M.; Horan, K.; Grinley, A.; Shoss, M.K. Stigma & dirty work: In-group and out-group perceptions of essential service workers during COVID-19. Int. J. Hosp. Manag. 2021, 93, 102772. [Google Scholar]
- Hennein, R.; Mew, E.J.; Lowe, S.R. Socio-ecological predictors of mental health outcomes among healthcare workers during the COVID-19 pandemic in the United States. PLoS ONE 2021, 16, e0246602. [Google Scholar] [CrossRef]
- Heijnders, M.; Van Der Meij, S. The fight against stigma: An overview of stigma-reduction strategies and interventions. Psychol. Health Med. 2006, 11, 353–363. [Google Scholar] [CrossRef]
- International Labour Organization. Managing Work-Related Psychosocial Risks during the COVID-19 Pandemic; ILO: Geneva, Switzerland, 2020. [Google Scholar]
- Krendl, A.C.; Pescosolido, B.A. Countries and cultural differences in the stigma of mental illness: The east–west divide. J. Cross-Cult. Psychol. 2020, 51, 149–167. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Category | Inclusion | Exclusion |
|---|---|---|
| Population | General working population (all sexes) | Children and youth, unemployed persons or persons in non-paid employment, pensioners, and persons over 70 years |
| Exposure | SARS-CoV-2 (A) | Other infectious diseases such as HIV and tuberculosis 1 |
| Outcomes | All stigmatization forms (including bullying) in association with work (A); measures that prevent work-related stigmatization (C) | - |
| Category | Inclusion | Exclusion |
|---|---|---|
| Population | General working population (all sexes) | Children and youth, unemployed persons or persons in non-paid employment, pensioners, and persons above 70 years |
| Exposure | Work-related stigmatization (all forms) due to COVID-19 | - |
| Outcomes | Physical and mental health, stigma-reducing strategies | - |
| Stigma Forms | Description | Examples from Included Studies |
|---|---|---|
| Public stigma | Endorsement of stereotypes, prejudices and discrimination against a group, that holds a specific characteristic. In surveys, the public is asked. | Stereotypes: e.g., “Healthcare workers who work in hospitals are likely to have COVID-19” [35]. Discrimination: e.g., “Healthcare workers should have some restrictions on their freedom [35]. Social exclusion as a component of discrimination: e.g., “I do not want to be around someone who works in a healthcare setting [35]. |
| Associative stigma | Endorsement of stereotypes, prejudices and discrimination against a group which is transferred to relatives. In surveys, the public or affected persons are asked. | Discrimination: e.g., “Relatives being alienated because employment related to COVID-19” [36]. Social exclusion as a component of discrimination: e.g., “People would avoid my family members because of my job” [37]. Aggressive behavior/bullying as a component of discrimination: e.g., “Have verbally abused (…) or physically assaulted (…) my family members” [38]. |
| Self-stigma (internalized) | Internalization, i.e., perception and transfer of stereotypes and devaluations to the own person. In surveys, affected persons are asked. | e.g., “Felt guilty about possibly exposing family, community and peers to infection” [38]; “feeling inferior to others due to occupation” [39]. |
| Self-stigma (perceived) | Belief that “most people” will devalue and discriminate the stigmatized. In surveys, affected persons are asked. | Stereotypes: e.g., “People do not trust me and worry that I might infect them” [38]. Discrimination: e.g., „People feel uncomfortable when I am around” [40] Social exclusion as a component of discrimination: e.g., “Family members and friends have avoided contact with me because of my work?” [41]. Aggressive behavior/bullying as a component of discrimination: e.g., “People have verbally abused me or physically assaulted me” [38]. |
| Self-stigma (anticipated) | Expectation of experiencing prejudice and discrimination due to a specific characteristic. In surveys, (potentially) affected persons are asked. | Fear, perceived consequences: “People would avoid me because of my job” [37]. |
| First Author Risk of Bias | Region Study Design Comments | Population | Stigmatization Form Assessment | Time of COVID-19 Pandemic |
|---|---|---|---|---|
| Chatterjee et al. [50] High risk | India CS Convenience sample | Physicians | Self-stigma (perceived) 1-item | Not specified |
| Chaudhary et al. [37] High risk | Pakistan CS # invited n. r. | Clinical oral HCWs Non-clinical oral HCWs from 10 different dental hospitals | Self-stigma (anticipated) Associative stigma 4-items | Not specified |
| Chen et al. [72] High risk | China Longitudinal # invited n. r. | Government/public institution/institutions/state-owned, enterprises, private enterprise staff or individual business | Self-stigma (perceived) 1-item | Baseline: rapid increase in COVID-19 cases and related deaths; follow-up: authorities relaxed lowdown |
| Chew et al. [39] High risk | Singapore Longitudinal Response: 49.2% | Medical residents in training (medical and surgical) | Self-stigma (anticipated) Self-stigma (internalized) 12 items (Healthcare Workers Stigma scale, HWSS) | Not specified |
| Dang et al. [36] High risk | Vietnam CS Convenience sample | HCWs, professional educators, white collar workers, students, others | Self-stigma (perceived) Self-stigma (anticipated) Associative stigma 4-items | Data collection one week after social distancing and lockdown was ordered by government |
| Do Duy et al. [40] High risk | Vietnam CS # invited n. r. | Clinicians, nurses, others | Self-stigma (perceived) Self-stigma (anticipated) Self-stigma (internalized) 12 items (adaption of Berger’s HIV Stigma Scale) | Lockdown of workplace because of COVID-19 outbreak-> all employees required to quarantine for 23 days. Data collection after quarantine |
| Dye et al. [57] High risk | Worldwide CS Convenience sample | n.r. | Self-stigma (anticipated) Associative stigma 1 item | Not specified |
| Elhadi et al. [59] High risk | Libya CS Convenience sample | HCWs (doctors and nurses) from 15 hospitals working during the outbreak period | Self-stigma (perceived) 1 item | Not specified (but during civil war) |
| Elhadi et al. [58] High risk | Libya CS Response: 88.7% | HCWs working in either surgery, internal medicine, intensive care, or emergency departments | Self-stigma (perceived) 1 item | Not specified (but during civil war) |
| Greene et al. [60] High risk | UK CS Convenience sample | Frontline health and social care workers working in a variety of healthcare roles in UK hospitals, nursing or care homes, and community settings | Self-stigma (perceived) 1 item | During COVID-19 pandemic (post-peak phase of the initial COVID-19 wave in the UK) |
| Juan et al. [51] High risk | China CS Response: 91.2% | hospital staff from five national COVID-19 designated hospitals (working in isolation ward, general ward) | Self-stigma (perceived) 1 item | Study period corresponds with the highest point of the COVID-19 epidemic in China |
| Khanal et al. [61,62] High risk | Nepal CS # invited n. r. | Nurses, doctors, paramedics, laboratory staff, pharmacists, public health professional currently working in COVID-19 management | Self-stigma (perceived) 1 item | During lockdown |
| Mohindra et al. [38] High risk | India CS Convenience sample | Doctors, nurses, hospital attendants, sanitation attendants, others working at the hospital | Self-stigma (perceived) Self-stigma (internalized) 19 items (adapted from Ebola epidemic questionnaire [74]) | During lockdown |
| Monterossa-Castro et al. [63] High risk | Colombia CS # invited n. r. | General Practitioners | Self-stigma (perceived) (questions not described) | Responses to “the 24–30 March period, when the country was in a health emergency, in the initial phase of containment” |
| Ramaci et al. [64] High risk | Italy CS Convenience sample | Nurses and doctors | Self-stigma (perceived) Self-stigma (anticipated) Questionnaire adapted from HIV/AIDS/drug users questionnaire [75] | During national lockdown |
| Said et al. [70] High risk | Egypt CS (controlled) Convenience sample | Nurses from triage hospital and from a hospital with no triage or isolation | Self-stigma (perceived) Self-stigma (internalized) 2 items (from US National Centre for Posttraumatic Stress Disorder 2020 and “MERS-CoV staff questionnaire”) | Not specified |
| Sharma et al. [65] High risk | USA CS Convenience sample | HCWs caring for COVID-19 patients (intensive care unit): physicians, nurses, respiratory therapists, advanced practice providers | Self-stigma (perceived) Not reported | Not specified |
| Tan et al. [66] High risk | China CS Response: 50.9% | Members of the workforce who returned to work: workers, and technical staff, executives, sales and marketing, management and others> | Self-stigma (perceived) 1 item | Returning to work after lockdown and quarantine in Chongqing, during the peak of the COVID-19 epidemic when strict infection control was in place |
| Taylor et al. [35] High risk | Canada, USA CS # invited n. r. | Non-HCWs | Public stigma 8 items | Not specified |
| Uvais et al. [67,68] High risk | India CS Convenience sample | Physicians working in hospitals | Self-stigma (perceived) Self-stigma (anticipated) 13 items (Perceived Stigma Scale) | Not specified |
| Yadav et al. [69] High risk | India CS Response: 36.6% | HCWs | Self-stigma (perceived) Associative stigma Adapted Stigma assessment and reduction of impact (SARI) Stigma scale | Not specified |
| Zandifar et al. [71] High risk | Iran CS Response: 92% | HCWs engaged in the field of diagnostic and treatment of COVID-19 patients working in 9 general hospitals (physicians, nurses, technicians) | Self-stigma (perceived) 22-items (adopted from the HIV Stigma Scale) | Not specified |
| Zhu et al. [41] High risk | China CS Response: 77.1% | HCWs from hospital directly providing services to confirmed or suspected COVID-19 patients (physicians, nurses, technicians) | Self-stigma (perceived) 1 item | COVID-19 outbreak (2 weeks after the authority in Wuhan suspended all public transport) |
| Study | Region | Population | Stigmatization Form Assessment | Time of COVID-19 Pandemic |
|---|---|---|---|---|
| Bhatt et al. [81] | Nepal | Teachers, students, security personnel, head of household, leaders, health workers, homemaker, others | Self-stigma (perceived) Associative stigma Interviews and focus group discussions | Not specified |
| Crowe et al. [79] | Canada | Critical Care Registered Nurses (CCRN) providing direct patient care in the intensive care and high acuity units in an academic teaching hospital | Self-stigma (perceived) Interviews | During the initial phase of the COVID-19 pandemic |
| Dye et al. [57] | Worldwide | Not reported | Self-stigma (perceived) Associative stigma Open-ended question | Not specified |
| Fawaz et al. [56] | Lebanon | Nurses and physicians working at various COVID-19 units | Self-stigma (perceived) Semi-structured interviews | Being quarantined following occupational COVID-19 exposure |
| Feroz et al. [78] | Pakistan | Key informants KIIs (senior management and hospital leadership, directly or indirectly involved with the management of COVID-19 patients) | Self-stigma (anticipated) Semi-structured interviews and a purposive sampling approach | Not specified |
| Hien et al. [80] | Germany | Nurses in clinics and retirement homes | Self-stigma (perceived) Associative stigma Interviews | Not specified |
| Kackin et al. [52] | Turkey | Nurses caring for COVID-19 patients | Self-stigma (perceived) Associative stigma Semi-structured interviews | Not specified |
| Kalateh-Sadati et al. [53] | Iran | Nurses working in hospitals specified for COVID-19 treatment | Self-stigma (perceived) Interviews | Not specified |
| Lee et al. [82] | South Korea | COVID-19-designated hospital nurses providing direct care for patients | Self-stigma (perceived) Associative stigma In-depth interviews | Not specified |
| Reazee et al. [76] | Iran | Nurses working fulltime in COVID-19 wards | Self-stigma (perceived) Associative stigma Interviews | Not specified |
| Rizvi Jafree et al. [77] | Pakistan | Not reported | Self-stigma (perceived) Semi-structured interviews | COVID-19-affected families admitted at three government-allocated hospitals |
| Zolnikov et al. [83] | Canada, Ireland, Kenya, USA | First responders/HCWs: nurses, physicians, firefighters, paramedics, police officers, nurse technicians, behavioural therapists, orthodontists, dialysis technicians, technicians in medical surgery, data specialists, emergency medical technicians | Self-stigma (internalized) Semi-structured interviews | Not specified |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schubert, M.; Ludwig, J.; Freiberg, A.; Hahne, T.M.; Romero Starke, K.; Girbig, M.; Faller, G.; Apfelbacher, C.; von dem Knesebeck, O.; Seidler, A. Stigmatization from Work-Related COVID-19 Exposure: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 6183. https://doi.org/10.3390/ijerph18126183
Schubert M, Ludwig J, Freiberg A, Hahne TM, Romero Starke K, Girbig M, Faller G, Apfelbacher C, von dem Knesebeck O, Seidler A. Stigmatization from Work-Related COVID-19 Exposure: A Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(12):6183. https://doi.org/10.3390/ijerph18126183
Chicago/Turabian StyleSchubert, Melanie, Julia Ludwig, Alice Freiberg, Taurai Monalisa Hahne, Karla Romero Starke, Maria Girbig, Gudrun Faller, Christian Apfelbacher, Olaf von dem Knesebeck, and Andreas Seidler. 2021. "Stigmatization from Work-Related COVID-19 Exposure: A Systematic Review with Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 12: 6183. https://doi.org/10.3390/ijerph18126183