
Effects of Plyometric and Balance Training on Neuromuscular Control of Recreational Athletes with Functional Ankle Instability: A Randomized Controlled Laboratory Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
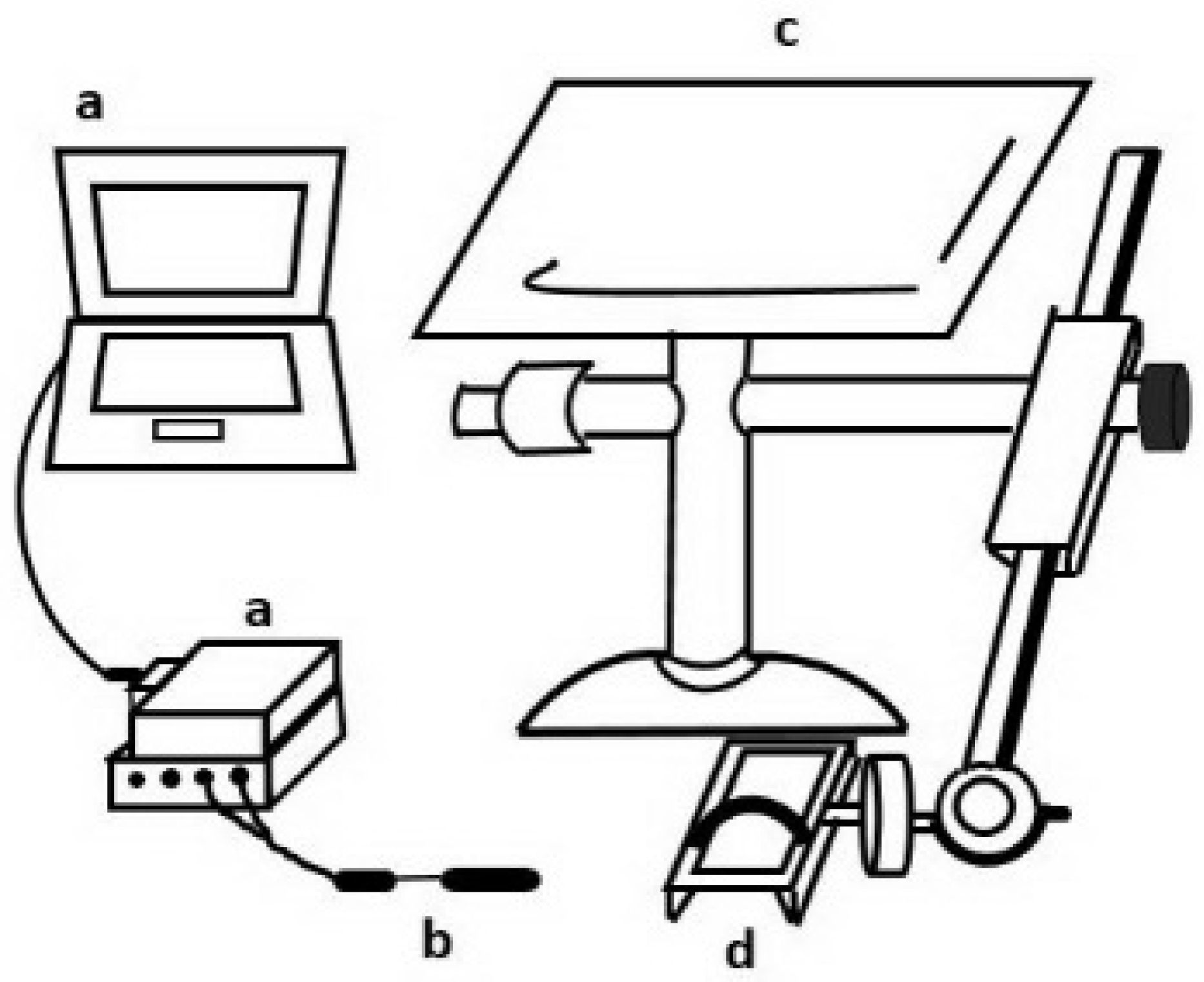
2.3. Experimental Procedure
2.4. Data Reduction
2.5. Training Programs
2.6. Statistical Analysis
3. Results
3.1. Demographics
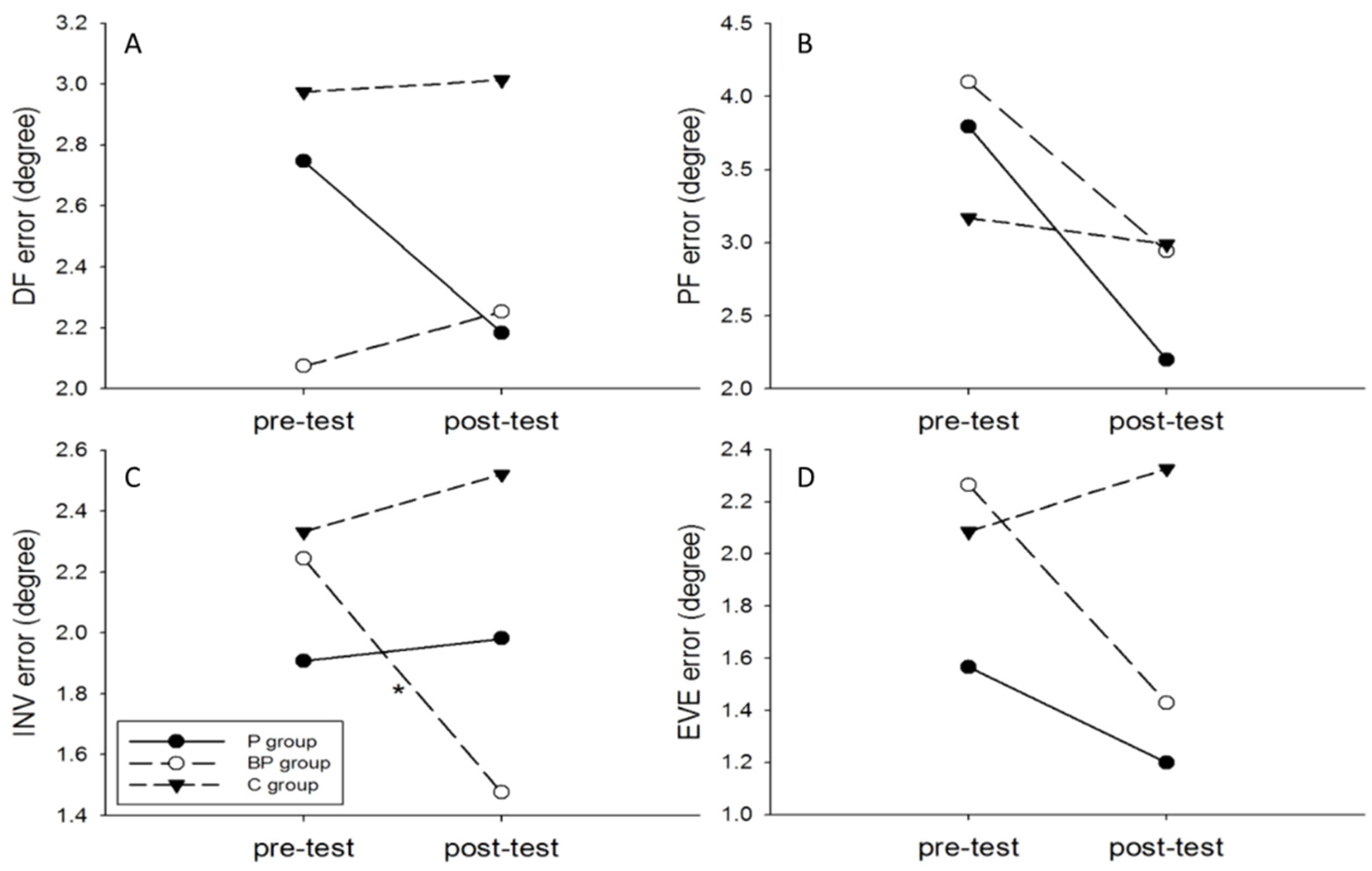
3.2. Joint Position Sense
3.3. Single-Leg Drop Landing
4. Discussion
4.1. Joint Position Sense
4.2. Muscle Activation Strategy (Activation Level)
4.3. Adjusting Time
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Donovan, L.; Hetzel, S.; Laufenberg, C.R.; McGuine, T.A. Prevalence and Impact of Chronic Ankle Instability in Adolescent Athletes. Orthop. J. Sports Med. 2020, 8. [Google Scholar] [CrossRef] [Green Version]
- Hertel, J. Sensorimotor Deficits with Ankle Sprains and Chronic Ankle Instability. Clin. Sports Med. 2008, 27, 353–370. [Google Scholar] [CrossRef]
- Hopkins, J.T.; Coglianese, M.; Glasgow, P.; Reese, S.; Seeley, M.K. Alterations in evertor/invertor muscle activation and center of pressure trajectory in participants with functional ankle instability. J. Electromyogr. Kinesiol. 2012, 22, 280–285. [Google Scholar] [CrossRef]
- Suda, E.Y.; Amorim, C.F.; de Sacco, I.C. Influence of ankle functional instability on the ankle electromyography during landing after volleyball blocking. J. Electromyogr. Kinesiol. 2009, 19, e84–e93. [Google Scholar] [CrossRef]
- Wright, C.J.; Arnold, B.L.; Ross, S.E. Altered Kinematics and Time to Stabilization During Drop-Jump Landings in Individuals With or Without Functional Ankle Instability. J. Athl. Train. 2016, 51, 5–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, J.; Rosen, A.B.; Brown, C.N. Functional performance deficits in adolescent athletes with a history of lateral ankle sprain(s). Phys. Ther. Sport 2018, 33, 125–132. [Google Scholar] [CrossRef]
- Houston, M.N.; Hoch, J.M.; Hoch, M.C. Patient-Reported Outcome Measures in Individuals With Chronic Ankle Instability: A Systematic Review. J. Athl. Train. 2015, 50, 1019–1033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, D.-J.; Kim, B.-J.; Kim, Y.-H.; Park, S.-Y. A three-week intervention emphasized diagonal eccentric contraction on balance and joint position sense and ankle strength in subjects with ankle instability: A randomized controlled trial. J. Back Musculoskelet. Rehabil. 2020, 34, 95–101. [Google Scholar] [CrossRef]
- Lazaroua, L.; Kofotolisa, N.; Mallioub, P.; Kellisa, E. Effects of two proprioceptive training programs on joint position sense, strength, activation and recurrent injuries after ankle sprains. Isokinet. Exerc. Sci. 2017, 25, 289–300. [Google Scholar] [CrossRef]
- Dias, A.; Pezarat-Correia, P.; Esteves, J.; Fernandes, O. The influence of a balance training program on the electromyographic latency of the ankle musculature in subjects with no history of ankle injury. Phys. Ther. Sport 2011, 12, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Eils, E.; Rosenbaum, D. A multi-station proprioceptive exercise program in patients with ankle instability. Med. Sci. Sports Exerc. 2001, 33, 1991–1998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez, M.; Sanchez-Sanchez, J.; Nakamura, F.Y.; Clemente, F.M.; Romero-Moraleda, B.; Ramirez-Campillo, R. Effects of Plyometric Jump Training in Female Soccer Player’s Physical Fitness: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 8911. [Google Scholar] [CrossRef]
- Ebben, W.P.; Simenz, C.; Jensen, R.L. Evaluation of Plyometric Intensity Using Electromyography. J. Strength Cond. Res. 2008, 22, 861–868. [Google Scholar] [CrossRef]
- Ellenbecker, T.S.; Sueyoshi, T.; Bailie, D.S. Muscular activation during plyometric exercises in 90° of glenohumeral joint abduction. Sports Health 2015, 7, 75–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alikhani, R.; Shahrjerdi, S.; Golpaigany, M.; Kazemi, M. The effect of a six-week plyometric training on dynamic balance and knee proprioception in female badminton players. J. Can. Chiropr. Assoc. 2019, 63, 144–153. [Google Scholar]
- Chimera, N.J.; Swanik, K.A.; Swanik, C.B.; Straub, S.J. Effects of Plyometric Training on Muscle-Activation Strategies and Performance in Female Athletes. J. Athl. Train. 2004, 39, 24–31. [Google Scholar] [PubMed]
- Miklovic, T.M.; Donovan, L.; Protzuk, O.A.; Kang, M.S.; Feger, M.A. Acute lateral ankle sprain to chronic ankle instability: A pathway of dysfunction. Physician Sportsmed. 2018, 46, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Herb, C.C.; Hertel, J. Current concepts on the pathophysiology and management of recurrent ankle sprains and chronic ankle instability. Curr. Phys. Med. Rehabil. Rep. 2014, 2, 25–34. [Google Scholar] [CrossRef] [Green Version]
- McCriskin, B.J.; Cameron, K.L.; Orr, J.D.; Waterman, B.R. Management and prevention of acute and chronic lateral ankle instability in athletic patient populations. World J. Orthop. 2015, 6, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Lundy-Ekman, L. Somatosensory System. In Neuroscience: Fundamentals for Rehabilitation; Elsevier Health Sciences: St. Louis, MO, USA, 2013; pp. 108–111. [Google Scholar]
- Chaouachi, A.; Othman, A.B.; Hammami, R.; Drinkwater, E.J.; Behm, D.G. The Combination of Plyometric and Balance Training Improves Sprint and Shuttle Run Performances More Often Than Plyometric-Only Training With Children. J. Strength Cond. Res. 2014, 28, 401–412. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Delahunt, E.; Bleakley, C.M.; Caulfield, B.; Docherty, C.L.; Fong, D.T.-P.; Fourchet, F.; Hertel, J.; Hiller, C.E.; Kaminski, T.W.; et al. Selection Criteria for Patients With Chronic Ankle Instability in Controlled Research: A Position Statement of the International Ankle Consortium. J. Athl. Train. 2014, 49, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Hiller, C.E.; Refshauge, K.M.; Bundy, A.C.; Herbert, R.D.; Kilbreath, S.L. The Cumberland Ankle Instability Tool: A Report of Validity and Reliability Testing. Arch. Phys. Med. Rehabil. 2006, 87, 1235–1241. [Google Scholar] [CrossRef]
- Coughlan, G.; Caulfield, B. A 4-Week Neuromuscular Training Program and Gait Patterns at the Ankle Joint. J. Athl. Train. 2007, 42, 51–59. [Google Scholar] [PubMed]
- Sekir, U.; Yildiz, Y.; Hazneci, B.; Ors, F.; Saka, T.; Aydin, T. Reliability of a functional test battery evaluating functionality, proprioception, and strength in recreational athletes with functional ankle instability. Eur. J. Phys. Rehabil. Med. 2008, 44, 407–415. [Google Scholar] [PubMed]
- Perotto, A.; Thomas, C.C. Anatomical Guide for The Electromyographer: The Limbs and Trunk; Charles, C., Ed.; Thomas Publisher Ltd.: Springfield, IL, USA, 2005. [Google Scholar]
- Delahunt, E.; Monaghan, K.; Caulfield, B. Altered Neuromuscular Control and Ankle Joint Kinematics during Walking in Subjects with Functional Instability of the Ankle Joint. Am. J. Sports Med. 2006, 34, 1970–1976. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.-Y.; Chen, W.-L.; Lin, C.-F.; Lee, H.-J. Lower Extremity Biomechanics in Athletes With Ankle Instability After a 6-Week Integrated Training Program. J. Athl. Train. 2014, 49, 163–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect size estimates: Current use, calculations, and interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.K. Alternatives to P value: Confidence interval and effect size. Korean J. Anesthesiol. 2016, 69, 555–562. [Google Scholar] [CrossRef] [Green Version]
- Jain, T.K.; Wauneka, C.N.; Liu, W. The effect of balance training on ankle proprioception in patients with functional ankle instability. J. Foot Ankle Res. 2014, 7 (Suppl. 1), A37. [Google Scholar] [CrossRef] [Green Version]
- Swanik, K.A.; Lephart, S.M.; Swanik, C.B.; Lephart, S.P.; Stone, D.A.; Fu, F.H. The effects of shoulder plyometric training on proprioception and selected muscle performance characteristics. J. Shoulder Elb. Surg. 2002, 11, 579–586. [Google Scholar] [CrossRef] [Green Version]
- Yokoyama, S.; Matsusaka, N.; Gamada, K.; Ozaki, M.; Shindo, H. Position-Specific Deficit of Joint Position Sense in Ankles with Chronic Functional Instability. J. Sports Sci. Med. 2008, 7, 480–485. [Google Scholar]
- Mckinlay, B.J.; Wallace, P.; Dotan, R.; Long, D.; Tokuno, C.; Gabriel, D.A.; Falk, B. Effects of Plyometric and Resistance Training on Muscle Strength, Explosiveness, and Neuromuscular Function in Young Adolescent Soccer Players. J. Strength Cond. Res. 2018, 32, 3039–3050. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-K.; Lien, Y.-H.; Lin, K.-H.; Shih, T.T.; Wang, T.-G.; Wang, H.-K. Relationships between three potentiation effects of plyometric training and performance. Scand. J. Med. Sci. Sports 2010, 20, e80–e86. [Google Scholar] [CrossRef]
- Blackburn, J.T.; Hirth, C.J.; Guskiewicz, K.M. Exercise Sandals Increase Lower Extremity Electromyographic Activity During Functional Activities. J. Athl. Train. 2003, 38, 198–203. [Google Scholar]
- Laudner, K.G.; Koschnitzky, M.M. Ankle Muscle Activation When Using the Both Sides Utilized (BOSU) Balance Trainer. J. Strength Cond. Res. 2010, 24, 218–222. [Google Scholar] [CrossRef]
- Neamatallah, Z.; Herrington, L.; Jones, R. An investigation into the role of gluteal muscle strength and EMG activity in controlling HIP and knee motion during landing tasks. Phys. Ther. Sport 2020, 43, 230–235. [Google Scholar] [CrossRef]
- Simpson, J.D.; Stewart, E.M.; Turner, A.J.; Macias, D.M.; Wilson, S.J.; Chander, H.; Knight, A.C. Neuromuscular control in individuals with chronic ankle instability: A comparison of unexpected and expected ankle inversion perturbations during a single leg drop-landing. Hum. Mov. Sci. 2019, 64, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Wikstrom, E.A.; Tillman, M.D.; Chmielewski, T.L.; Cauraugh, J.H.; Borsa, P.A. Dynamic Postural Stability Deficits in Subjects with Self-Reported Ankle Instability. Med. Sci. Sports Exerc. 2007, 39, 397–402. [Google Scholar] [CrossRef]
- Son, S.J.; Kim, H.; Seeley, M.K.; Hopkins, J.T. Altered Walking Neuromechanics in Patients With Chronic Ankle Instability. J. Athl. Train. 2019, 54, 684–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bavdek, R.; Zdolšek, A.; Strojnik, V.; Dolenec, A. Peroneal muscle activity during different types of walking. J. Foot Ankle Res. 2018, 11, 50. [Google Scholar] [CrossRef]
- Mineta, S.; Inami, T.; Mariano, R.; Hirose, N. High lateral plantar pressure is related to an increased tibialis anterior/fibularis longus activity ratio in patients with recurrent lateral ankle sprain. Open Access J. Sports Med. 2017, 8, 123–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brand, A.; Bradley, M.T. The precision of effect size estimation from published psychological research: Surveying confidence intervals. Psychol. Rep. 2016, 118, 154–170. [Google Scholar] [CrossRef]
- Gutierrez, G.M.; Knight, C.A.; Swanik, C.B.; Royer, T.; Manal, K.; Caulfield, B.; Kaminski, T.W. Examining Neuromuscular Control During Landings on a Supinating Platform in Persons With and Without Ankle Instability. Am. J. Sports Med. 2012, 40, 193–201. [Google Scholar] [CrossRef]
- De Noronha, M.; Refshauge, K.M.; Crosbie, J.; Kilbreath, S.L. Relationship Between Functional Ankle Instability and Postural Control. J. Orthop. Sports Phys. Ther. 2008, 38, 782–789. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject Characteristics | Control Group | Isolated Plyometric Training Group | Integrated Balance + Plyometric Training Group | p-Value |
|---|---|---|---|---|
| CAIT score at baseline | 19.90 ± 3.41 | 19.05 ± 2.88 | 17.56 ± 4.47 | 0.952 |
| Total unstable ankle (bilateral:unilateral) | 10 (2:8) | 10 (3:7) | 10 (3:7) | - |
| Number of ankle sprains (in 6 months) | 1.70 ± 1.252 | 1.60 ± 0.97 | 1.50 ± 1.08 | 0.922 |
| Number of ankle sprains (in 2 years) | 4.50 ± 2.78 | 4.00 ± 2.54 | 3.50 ± 2.10 | 0.668 |
| Muscle | P Group | BP Group | C Group | Interaction Effect F Value | Interaction Effect p Value | Between- Group Effect Size, Cohen d (P-C Group) | Between- Group Effect Size, Cohen d (BP-C Group) | Between- Group Effect Size, Cohen d (P-BP Group) | 95% CI (Effect Size P-C Group) | 95% CI (Effect Size BP-C Group) | 95% CI (Effect Size P-BP Group) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Training | Post-Training | Pre-Training | Post-Training | Pre-Training | Post-Training | |||||||||
| TA | 34.49 ± 10.98 | 41.89 ± 13.98 # | 38.46 ± 8.61 | 44.15 ± 16.50 * | 36.88 ± 10.13 | 33.46 ± 12.45 | 4.469 | 0.014 | 0.637 | 0.731 | −0.148 | −0.261, 1.535 | −0.174, 1.636 | −0.730, 1.026 |
| PL | 64.24 ± 15.09 | 68.37 ± 26.36 | 70.50 ± 12.84 | 74.22 ± 16.05 | 59.62 ± 12.57 | 61.86 ± 14.05 | 0.091 | 0.913 | 0.308 | 0.820 | −0.268 | −0.574, 1.190 | −0.093, 1.733 | −0.612, 1.148 |
| GL | 41.33 ± 19.11 | 73.43 ± 21.80 *,# | 47.21 ± 19.66 | 78.88 ± 28.14 *,# | 48.39 ± 16.92 | 46.56 ± 15.60 | 21.434 | <0.001 | 1.418 | 1.421 | −0.217 | 0.202, 2.094 | 0.440, 2.402 | −0.662, 1.096 |
| GM | 58.19 ± 24.97 | 74.88 ± 15.04 *,# | 56.01 ± 30.07 | 69.69 ± 18.34 # | 61.21 ± 14.26 | 61.94 ± 11.77 | 4.543 | 0.013 | 0.958 | 0.503 | 0.310 | 0.033, 1.883 | −0.387, 1.393 | −0.572, 1.192 |
| SOL | 32.36 ± 10.06 | 66.66 ±16.49 *,# | 36.23 ± 12.80 | 68.21 ± 17.14 *,# | 37.81 ± 8.29 | 40.03 ± 14.50 | 27.025 | <0.001 | 1.715 | 1.775 | −0.092 | 0.690, 2.740 | 0.740, 2.810 | −0.785, 0.970 |
| Muscle | P Group | BP Group | C Group | Interaction Effect F Value | Interaction Effect p Value | Between- Group Effect Size, Cohen d (P-C Group) | Between- Group Effect Size, Cohen d (BP-C Group) | Between- Group Effect Size, Cohen d (P-BP Group) | 95% CI (Effect Size P-C Group) | 95% CI (Effect Size BP-C Group) | 95% CI (Effect Size P-BP Group) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Training | Post-Training | Pre-Training | Post-Training | Pre-Training | Post-Training | |||||||||
| TA | 102.88 ± 20.93 | 119.29 ± 38.33 # | 94.51 ± 15.23 | 102.63 ± 35.58 | 97.32 ± 10.96 | 99.13 ± 23.80 | 1.418 | 0.248 | 0.632 | 0.116 | 0.451 | −0.266, 1.530 | −0.761, 0.993 | −0.437, 1.339 |
| PL | 102.67 ± 25.88 | 114.61 ± 25.98 | 95.21 ± 20.21 | 100.96 ± 18.58 | 98.35 ± 18.77 | 94.90 ± 23.28 | 1.999 | 0.142 | 0.799 | 0.288 | 0.604 | −0.112, 1.710 | −0.593, 1.169 | −0.292, 1.500 |
| GL | 87.26 ± 19.09 | 85.43 ± 21.58 | 86.04 ± 16.46 | 82.44 ± 21.70 | 92.63 ± 16.89 | 89.74 ± 17.40 | 0.034 | 0.967 | −0.220 | −0.371 | 0.138 | −0.659, 1.099 | −0.513, 1.255 | −0.740, 1.016 |
| GM | 89.22 ± 14.51 | 92.39 ± 20.33 | 85.45 ± 18.75 | 88.26 ± 17.54 | 91.87 ± 12.80 | 86.17 ± 17.16 | 1.264 | 0.288 | 0.331 | 0.121 | 0.218 | −0.552, 1.214 | −0.756, 0.998 | −0.661, 1.097 |
| SOL | 73.75 ± 24.24 | 77.80 ± 21.33 | 71.54 ± 17.61 | 75.68 ± 26.79 | 78.07 ± 17.43 | 79.01 ± 12.34 | 0.130 | 0.878 | −0.069 | −0.160 | 0.088 | −0.808, 0.946 | −0.718, 1.038 | −0.789, 0.965 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, P.-Y.; Jankaew, A.; Lin, C.-F. Effects of Plyometric and Balance Training on Neuromuscular Control of Recreational Athletes with Functional Ankle Instability: A Randomized Controlled Laboratory Study. Int. J. Environ. Res. Public Health 2021, 18, 5269. https://doi.org/10.3390/ijerph18105269
Huang P-Y, Jankaew A, Lin C-F. Effects of Plyometric and Balance Training on Neuromuscular Control of Recreational Athletes with Functional Ankle Instability: A Randomized Controlled Laboratory Study. International Journal of Environmental Research and Public Health. 2021; 18(10):5269. https://doi.org/10.3390/ijerph18105269
Chicago/Turabian StyleHuang, Pi-Yin, Amornthep Jankaew, and Cheng-Feng Lin. 2021. "Effects of Plyometric and Balance Training on Neuromuscular Control of Recreational Athletes with Functional Ankle Instability: A Randomized Controlled Laboratory Study" International Journal of Environmental Research and Public Health 18, no. 10: 5269. https://doi.org/10.3390/ijerph18105269