
The Influence of Air Pollutants and Meteorological Conditions on the Hospitalization for Respiratory Diseases in Shenzhen City, China

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
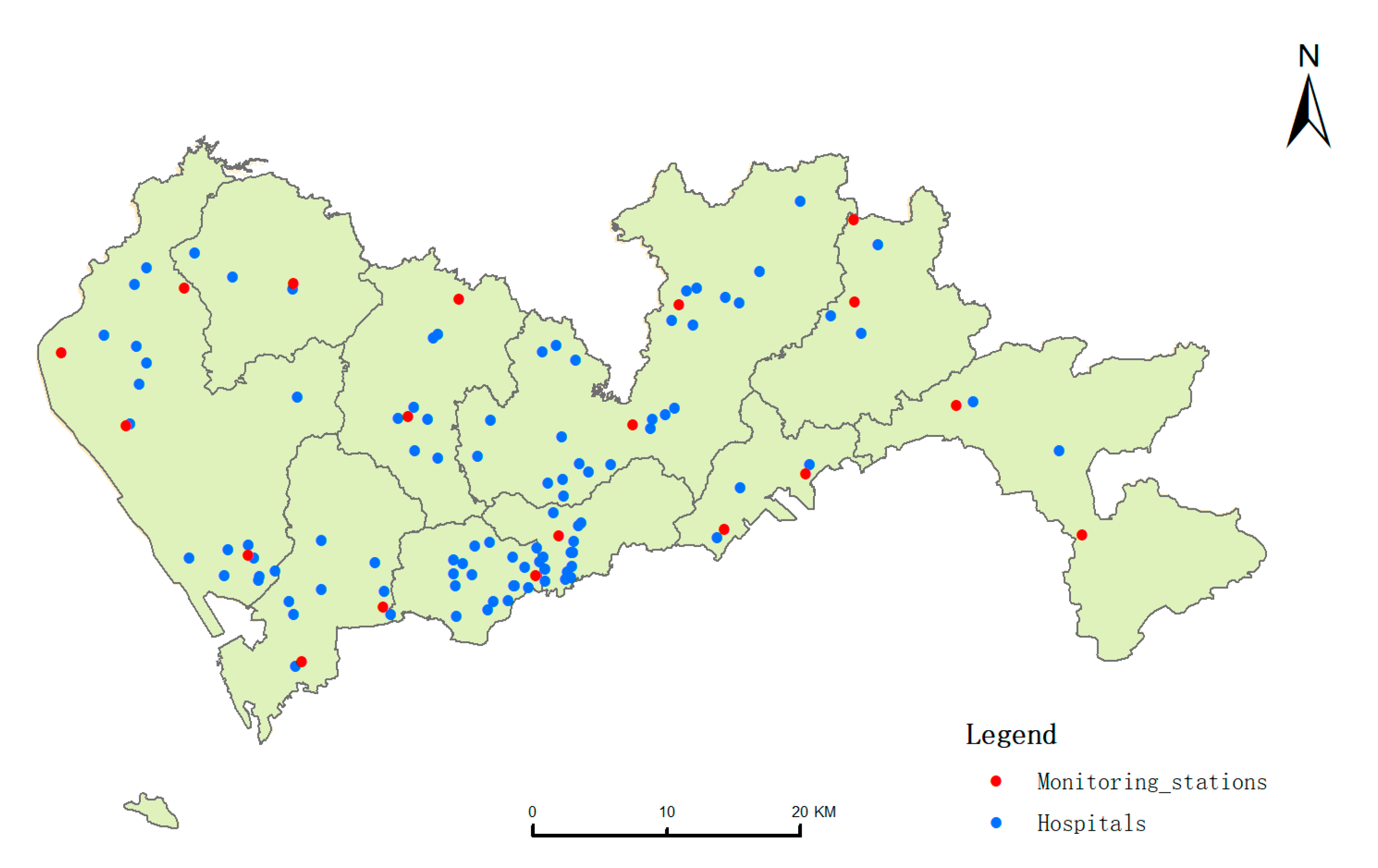
2.1. The Information about Shenzhen City
2.2. Air Quality Data and Meteorological Data
2.3. Hospital Admission Data
2.4. Methods
3. Results
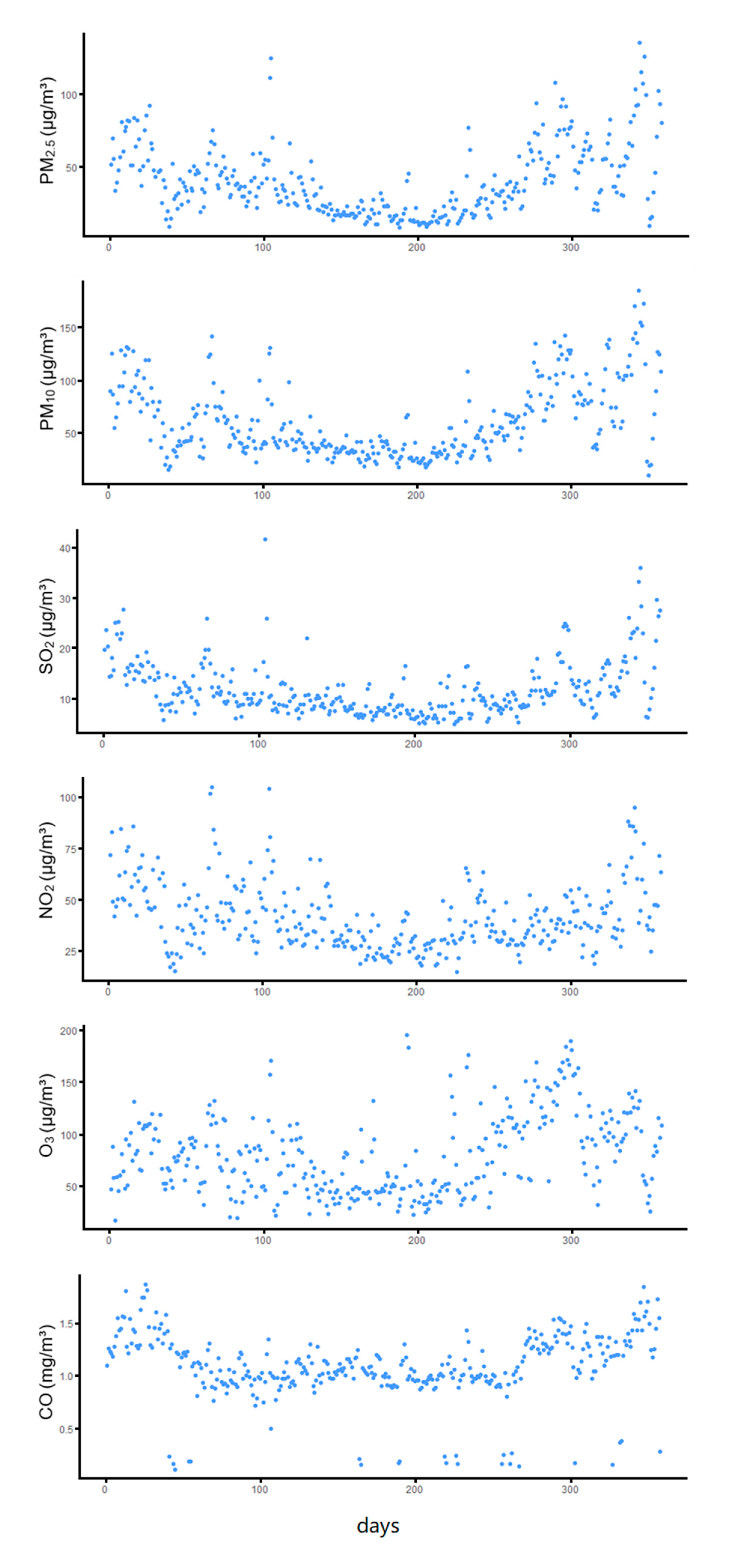
3.1. Descriptive Statistics
3.2. The Relationship between the Concentration of Air Pollutants, Meteorological Factors, and Wind Direction
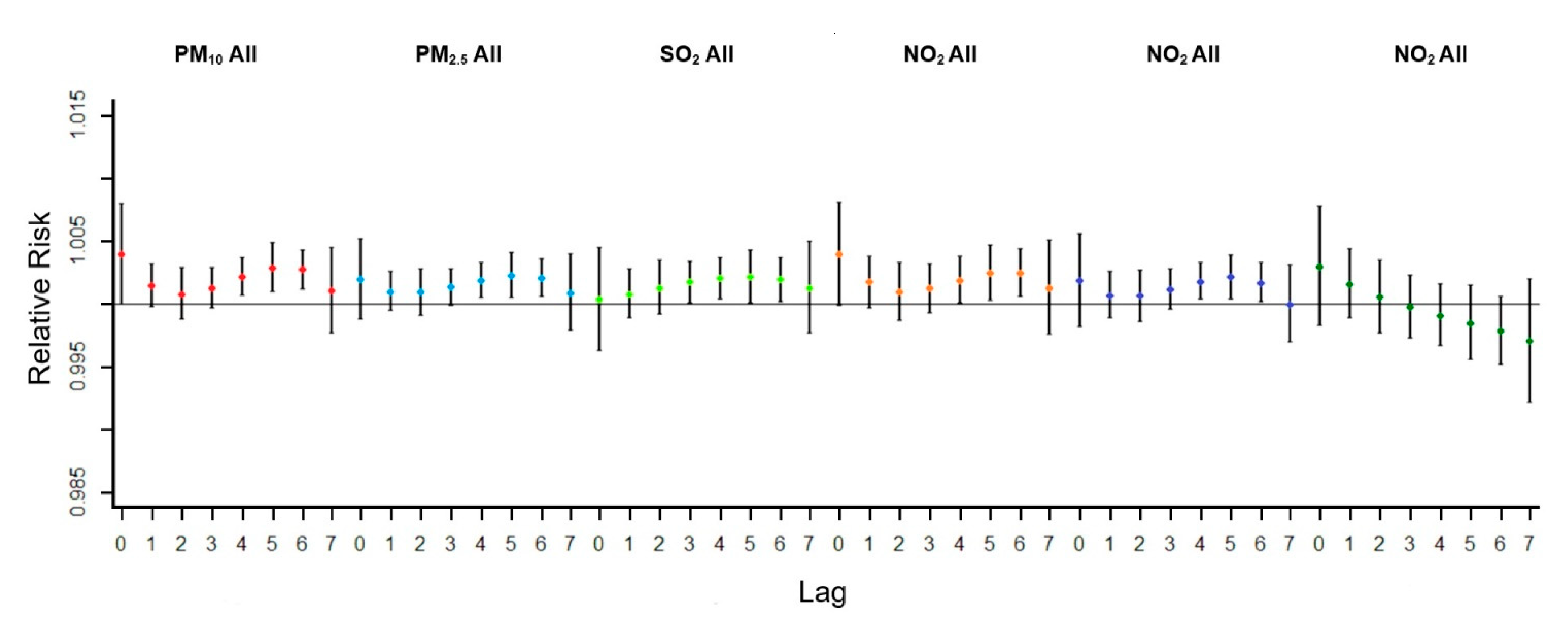
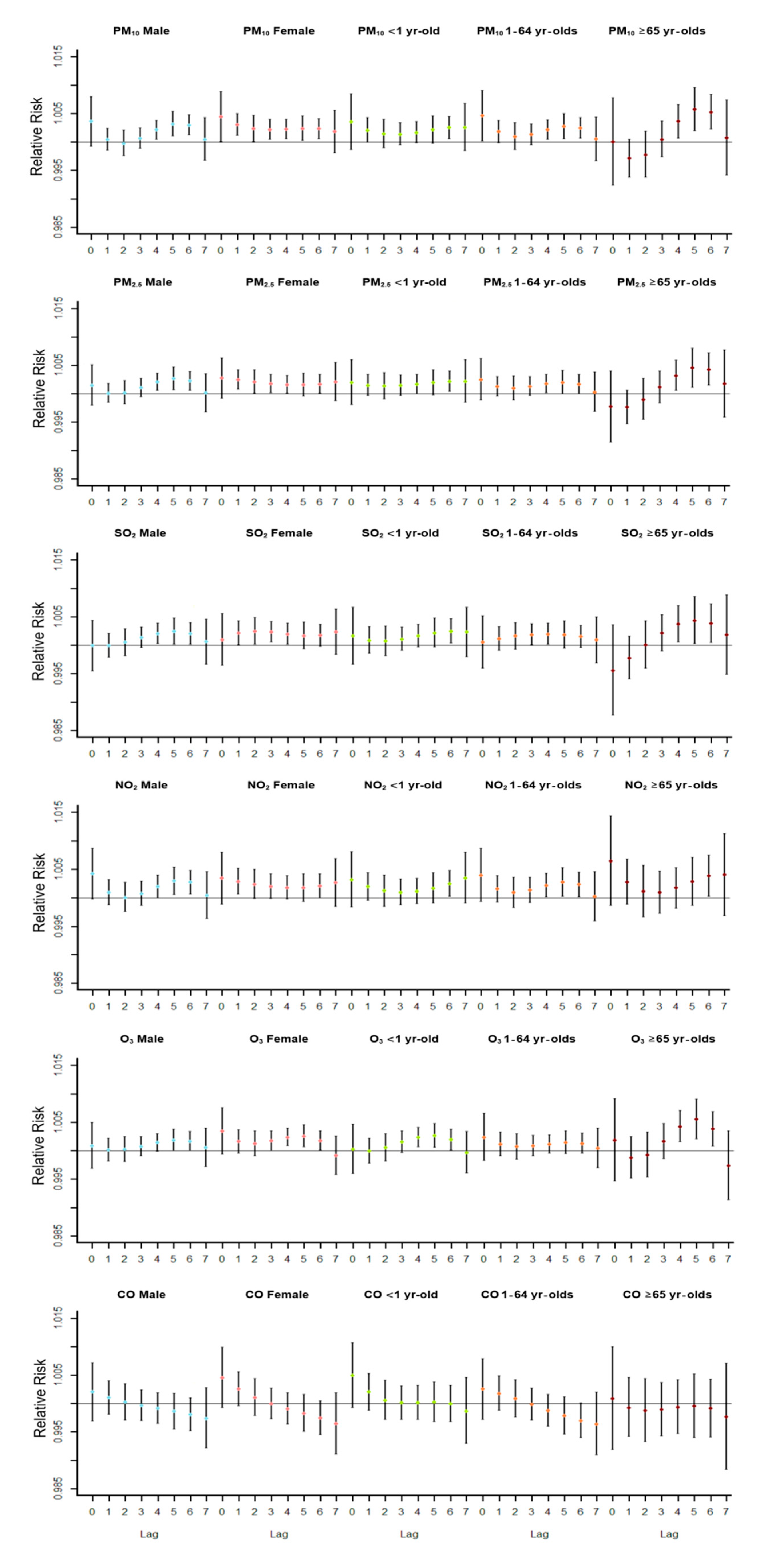
3.3. The Relationship between Six Air Pollutants and the Whole Number of Respiratory Inpatients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bp Statistical Review of World Energy June 2020. Available online: http://www.bp.com/statisticalreview (accessed on 19 February 2021).
- Costa, S.; Ferreira, J.; Silveira, C.; Costa, C.; Lopes, D.; Relvas, H.; Borrego, C.; Roebeling, P.; Miranda, A.I.; Teixeira, J.P. Integrating health on air quality assessment—Review report on health risks of two major European outdoor air pollutants: PM and NO2. J. Toxicol. Environ. Health Part B 2014, 17, 307–340. [Google Scholar] [CrossRef]
- Beckerman, B.S.; Jerrett, M.; Finkelstein, M.; Kanaroglou, P.; Brook, J.R.; Arain, M.A.; Sears, M.R.; Stieb, D.; Balmes, J.; Chapman, K. The association between chronic exposure to traffic-related air pollution and ischemic heart disease. J. Toxicol. Environ. Health Part A 2012, 75, 402–411. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.S.; Chiu, H.F.; Liou, S.H.; Yang, C.Y. Short-term effects of fine particulate air pollution on hospital admissions for respiratory diseases: A case-crossover study in a tropical city. J. Toxicol. Environ. Health Part A 2014, 77, 1091–1101. [Google Scholar] [CrossRef] [PubMed]
- Tsangari, H.; Paschalidou, A.K.; Kassomenos, A.P.; Vardoulakis, S.; Heaviside, C.; Georgiou, K.E.; Yamasaki, E.N. Extreme weather and air pollution effects on cardiovascular and respiratory hospital admissions in Cyprus. Sci. Total Environ. 2016, 542, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Xia, X.L.; Zhang, A.; Liang, S.; Qi, Q.W.; Jiang, L.L.; Ye, Y.J. The Association between Air Pollution and Population Health Risk for Respiratory Infection: A Case Study of Shenzhen, China. Int. J. Environ. Res. Public Health 2017, 14, 950. [Google Scholar] [CrossRef] [Green Version]
- GBD. 2016 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar]
- Chen, R.; Huang, W.; Wong, C.M.; Wang, Z.; Thach, T.Q.; Chen, B.; Kan, H.; CAPES Collaborative Group. Short-term exposure to sulfur dioxide and daily mortality in 17 Chinese cities: The China air pollution and health effects study (CAPES). Environ. Res. 2012, 118, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Sunyer, J.; Ballester, F.; Tertre, A.L.; Atkinson, R.; Ayres, J.G.; Forastiere, F.; Forsberg, B.; Vonk, J.M.; Bisanti, L.; Tenías, J.M.; et al. The association of daily sulfur dioxide air pollution levels with hospital admissions for cardiovascular diseases in Europe (The Aphea-II study). Europ. Heart J. 2003, 24, 752–760. [Google Scholar] [CrossRef]
- Wang, X.Y.; Hu, W.; Tong, S. Long-term exposure to gaseous air pollutants and cardio-respiratory mortality in Brisbane, Austral. Geospatial Health 2009, 3, 257–263. [Google Scholar] [CrossRef] [Green Version]
- Chang, G.; Pan, X.; Xie, X.; Gao, Y. Time-series analysis on the relationship between air pollution and daily mortality in Beijing. Wei Sheng Yan Jiu J. Hygiene Res. 2003, 32, 565–568. [Google Scholar]
- Guo, Y.; Jia, Y.; Pan, X.; Liu, L.; Wichmann, H.E. The association between fine particulate air pollution and hospital emergency room visits for cardiovascular diseases in Beijing, China. Sci. Total Environ. 2009, 407, 4826–4830. [Google Scholar] [CrossRef]
- Chen, G.; Song, G.; Jiang, L.; Zhang, Y.; Zhao, N.; Chen, B.; Kan, H. Short-term effects of ambient gaseous pollutants and particulate matter on daily mortality in Shanghai, China. J. Occupat. Health 2008, 50, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Venners, S.A.; Wang, B.; Xu, Z.; Schlatter, Y.; Wang, L.; Xu, X. Particulate matter, sulfur dioxide, and daily mortality in Chongqing, China. Environ. Health Perspect. 2003, 111, 562–567. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Ma, M.; Xiao, C.; Zhang, C.; Chen, J.; Lin, H.; Du, Y.; Liu, M. Association of air pollution and mortality of acute lower respiratory tract infections in Shenyang, China: A time series analysis study. Iran. J. Public Health 2018, 47, 1261. [Google Scholar] [PubMed]
- Galon-Negru, A.G.; Olariu, R.I.; Arsene, C. Size-resolved measurements of PM2. 5 water-soluble elements in Iasi, north-eastern Romania: Seasonality, source apportionment and potential implications for human health. Sci. Total Environ. 2019, 695, 133839. [Google Scholar] [CrossRef] [PubMed]
- Baysal, A.; Saygin, H.; Ustabasi, G.S. Interaction of PM2.5 airborne particulates with ZnO and TiO2 nanoparticles and their effect on bacteria. Environ. Monit. Assess. 2018, 190, 34. [Google Scholar] [CrossRef]
- Phung, D.; Hien, T.T.; Linh, H.N.; Luong, L.M.; Morawska, L.; Chu, C.; Binh, N.D.; Thai, P.K. Air pollution and risk of respiratory and cardiovascular hospitalizations in the most populous city in Vietnam. Sci. Total Environ. 2016, 557, 322–330. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.J.; Zhang, X.; Zhang, L.W.; Wang, X.M. Changing trends in meteorological elements and reference evapotranspiration in a mega city: A case study in Shenzhen city, China. Adv. Meteorol. 2015, 2015, 324502. [Google Scholar] [CrossRef]
- Eccles, R.; Wilkinson, J.E. Exposure to cold and acute upper respiratory tract infection. Rhinology 2015, 53, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Mu, Z.; Chen, P.L.; Geng, F.H.; Ren, L.; Gu, W.C.; Ma, J.Y.; Peng, L.; Li, Q.Y. Synergistic effects of temperature and humidity on the symptoms of COPD patients. Int. J. Biometeorol. 2017, 61, 1919–1925. [Google Scholar] [CrossRef]
- Chen, G.; Zhang, Y.; Zhang, W.; Li, S.; Williams, G.; Marks, G.B.; Jalaludin, B.; Abramson, M.J.; Luo, F.; Yang, D.; et al. Attributable risks of emergency hospital visits due to air pollutants in China: A multi-city study. Environ. Pollut. 2017, 228, 43–49. [Google Scholar] [CrossRef]
- Zhao, Y.; Wang, S.; Lang, L.; Huang, C.; Ma, W.; Lin, H. Ambient fine and coarse particulate matter pollution and respiratory morbidity in Dongguan, China. Environ. Pollut. 2017, 222, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Luong, L.T.M.; Dang, T.N.; Thanh, H.N.T.; Phung, D.; Tran, L.K.; Van, D.D.; Thai, P.K. Particulate air pollution in Ho Chi Minh city and risk of hospital admission for acute lower respiratory infection (ALRI) among young children. Environ. Pollut. 2020, 257, 113424. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Wang, T.; Zhou, F.; Liu, Y.; Zhao, W.; Wang, X.; Chen, H.; Cui, Y. Ambient air pollution and daily hospital admissions for respiratory disease in children in Guiyang, China. Front. Pediatr. 2019, 7, 400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Morisaki, H.; Wei, Y.; Li, Z.; Yang, L.; Zhou, Q.; Zhang, X.; Xing, W.; Hu, M.; Shima, M.; et al. Characteristics of air pollutants inside and outside a primary school classroom in Beijing and respiratory health impact on children. Environ. Pollut. 2019, 255, 113147. [Google Scholar] [CrossRef] [PubMed]
- Agudelo-Castañeda, D.M.; Calesso, T.E.; Alves, L.; Fernández-Niño, J.A.; Rodríguez-Villamizar, L.A. Monthly-Term Associations Between Air Pollutants and Respiratory Morbidity in South Brazil 2013–2016: A Multi-City, Time-Series Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3787. [Google Scholar] [CrossRef] [Green Version]
- Pascal, M.; Falq, G.; Wagner, V.; Chatignoux, E.; Corso, M.; Blanchard, M.; Host, S.; Pascal, L.; Larrieu, S. Short-term impacts of particulate matter (PM10, PM10–2.5, PM2. 5) on mortality in nine French cities. Atmosph. Environ. 2014, 95, 175–184. [Google Scholar] [CrossRef]
- Chen, S.; Guo, L.; Wang, Z.; Mao, W.; Ge, Y.; Ying, X.; Fang, J.; Long, Q.; Liu, Q.; Xiang, H.; et al. Current situation and progress toward the 2030 health-related Sustainable Development Goals in China: A systematic analysis. PLoS Med. 2019, 16, e1002975. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Wang, X.; Lv, C.; Li, W.; Ma, D.; Zhang, Q.; Dong, L. The effect of air pollution on hospitalization of individuals with respiratory and cardiovascular diseases in Jinan, China. Medicine 2019, 98, e15634. [Google Scholar] [CrossRef]
- Shamsipour, M.; Hassanvand, M.S.; Gohari, K.; Yunesian, M.; Fotouhi, A.; Naddafi, K.; Sheidaei, A.; Faridi, S.; Akhlaghi, A.A.; Rabiei, K.; et al. National and sub-national exposure to ambient fine particulate matter (PM2. 5) and its attributable burden of disease in Iran from 1990 to 2016. Environ. Pollut. 2019, 255, 113173. [Google Scholar] [CrossRef]
- Huang, H.C.; Tantoh, D.M.; Hsu, S.Y.; Nfor, O.N.; Lin, C.F.; Lung, C.C.; Ho, C.C.; Chen, C.Y.; Liaw, Y.P. Association between coarse particulate matter (PM10-2.5) and nasopharyngeal carcinoma among Taiwanese men. J. Investig. Med. 2020, 68, 419–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maesano, C.N.; Morel, G.; Matynia, A.; Ratsombath, N.; Bonnety, J.; Legros, G.; Da, C.P.; Prud’homme, J.; Annesi-Maesano, I. Impacts on human mortality due to reductions in PM10 concentrations through different traffic scenarios in Paris, France. Sci. Total Environ. 2020, 698, 134257. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frequency Distribution | Minimum Value | Maximum Value | Average Value (Standard Deviation) | |||
|---|---|---|---|---|---|---|
| Items | 25 | 50 | 75 | |||
| air pollutants | ||||||
| PM2.5(μg/m3) | 21.28 | 34.46 | 53.98 | 8.26 | 135.81 | 40.22(24.48) |
| PM10(μg/m3) | 35.05 | 49.41 | 79.75 | 10.25 | 184.78 | 61.31(34.75) |
| SO2(μg/m3) | 8.10 | 10.46 | 14.18 | 5.03 | 41.63 | 11.84(5.48) |
| NO2(μg/m3) | 29.55 | 37.54 | 48.84 | 14.83 | 104.81 | 41.29(16.45) |
| O3(μg/m3) | 48.25 | 74.27 | 107.77 | 17.32 | 195.18 | 80.49(38.53) |
| CO(mg/m3) | 0.96 | 1.08 | 1.28 | 0.11 | 1.86 | 1.09(0.32) |
| meteorological conditions | ||||||
| temperature(°C) | 20.00 | 25.00 | 28.00 | 9.00 | 31.00 | 23.85(5.02) |
| humidity(%) | 68.00 | 78.00 | 87.00 | 24.00 | 100.00 | 75.62(14.69) |
| The average daily number of hospital admission for respiratory diseases | 275.00 | 310.00 | 340.00 | 82.00 | 417.00 | 307.92(52.49) |
| male | 168.00 | 188.00 | 209.00 | 46.00 | 274.00 | 188.42(33.49) |
| female | 107.00 | 121.00 | 134.00 | 30.00 | 177.00 | 119.50(21.86) |
| <1 year | 59.50 | 79.00 | 93.00 | 20.00 | 125.00 | 76.58(20.66) |
| 1–64 years old | 183.50 | 204.00 | 227.00 | 47.00 | 310.00 | 203.32(38.55) |
| ≥65 years old | 23.00 | 27.00 | 33.00 | 8.00 | 56.00 | 28.01(7.35) |
| SO2 | NO2 | CO | O3 | PM10 | PM2.5 | AQI | Air Temperature | Humidity | East Wind | South Wind | West Wind | North Wind | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SO2 | 1.000 | ||||||||||||
| NO2 | 0.745 ** | 1.000 | |||||||||||
| CO | 0.510 ** | 0.459 ** | 1.000 | ||||||||||
| O3 | 0.583 ** | 0.317 ** | 0.359 ** | 1.000 | |||||||||
| PM10 | 0.831 ** | 0.641 ** | 0.531 ** | 0.728 ** | 1.000 | ||||||||
| PM2.5 | 0.815 ** | 0.667 ** | 0.576 ** | 0.684 ** | 0.947 ** | 1.000 | |||||||
| AQI | 0.824 ** | 0.767 ** | 0.593 ** | 0.677 ** | 0.904 ** | 0.929 ** | 1.000 | ||||||
| air temperature | −0.506 ** | −0.447 ** | −0.410 ** | −0.173 ** | −0.433 ** | −0.543 ** | −0.437 ** | 1.000 | |||||
| humidity | −0.630 ** | −0.206 ** | −0.321 ** | −0.662 ** | −0.667 ** | −0.558 ** | −0.499 ** | 0.265 ** | 1.000 | ||||
| East wind | −0.214 ** | −0.274 ** | −0.059 | −0.043 | −0.098 | −0.097 | −0.135 * | −0.012 | 0.003 | 1.000 | |||
| south wind | −0.259 ** | −0.236 ** | −0.114 * | −0.145 ** | −0.158 ** | −0.180 ** | −0.206 ** | 0.157 ** | 0.123 * | 0.404 ** | 1.000 | ||
| west wind | −0.100 | −0.128 * | −0.021 | −0.057 | −0.043 | −0.055 | −0.079 | 0.142 ** | 0.030 | −0.037 | 0.460 ** | 1.000 | |
| North wind | 0.016 | −0.112 * | 0.065 | 0.049 | 0.034 | 0.036 | 0.013 | −0.108 * | −0.121 * | 0.567 ** | 0.022 | 0.091 | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, S.; Sun, C.; Liu, C.; Jiang, L.; Xie, Y.; Yan, S.; Jiang, Z.; Qi, Q.; Zhang, A. The Influence of Air Pollutants and Meteorological Conditions on the Hospitalization for Respiratory Diseases in Shenzhen City, China. Int. J. Environ. Res. Public Health 2021, 18, 5120. https://doi.org/10.3390/ijerph18105120
Liang S, Sun C, Liu C, Jiang L, Xie Y, Yan S, Jiang Z, Qi Q, Zhang A. The Influence of Air Pollutants and Meteorological Conditions on the Hospitalization for Respiratory Diseases in Shenzhen City, China. International Journal of Environmental Research and Public Health. 2021; 18(10):5120. https://doi.org/10.3390/ijerph18105120
Chicago/Turabian StyleLiang, Shi, Chong Sun, Chanfang Liu, Lili Jiang, Yingjia Xie, Shaohong Yan, Zhenyu Jiang, Qingwen Qi, and An Zhang. 2021. "The Influence of Air Pollutants and Meteorological Conditions on the Hospitalization for Respiratory Diseases in Shenzhen City, China" International Journal of Environmental Research and Public Health 18, no. 10: 5120. https://doi.org/10.3390/ijerph18105120