
Analysing the Impacts of Financial Support for Regional Suicide Prevention Programmes on Suicide Mortality Caused by Major Suicide Motives in Japan Using Statistical Government Data


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Statistical Analysis
3. Results
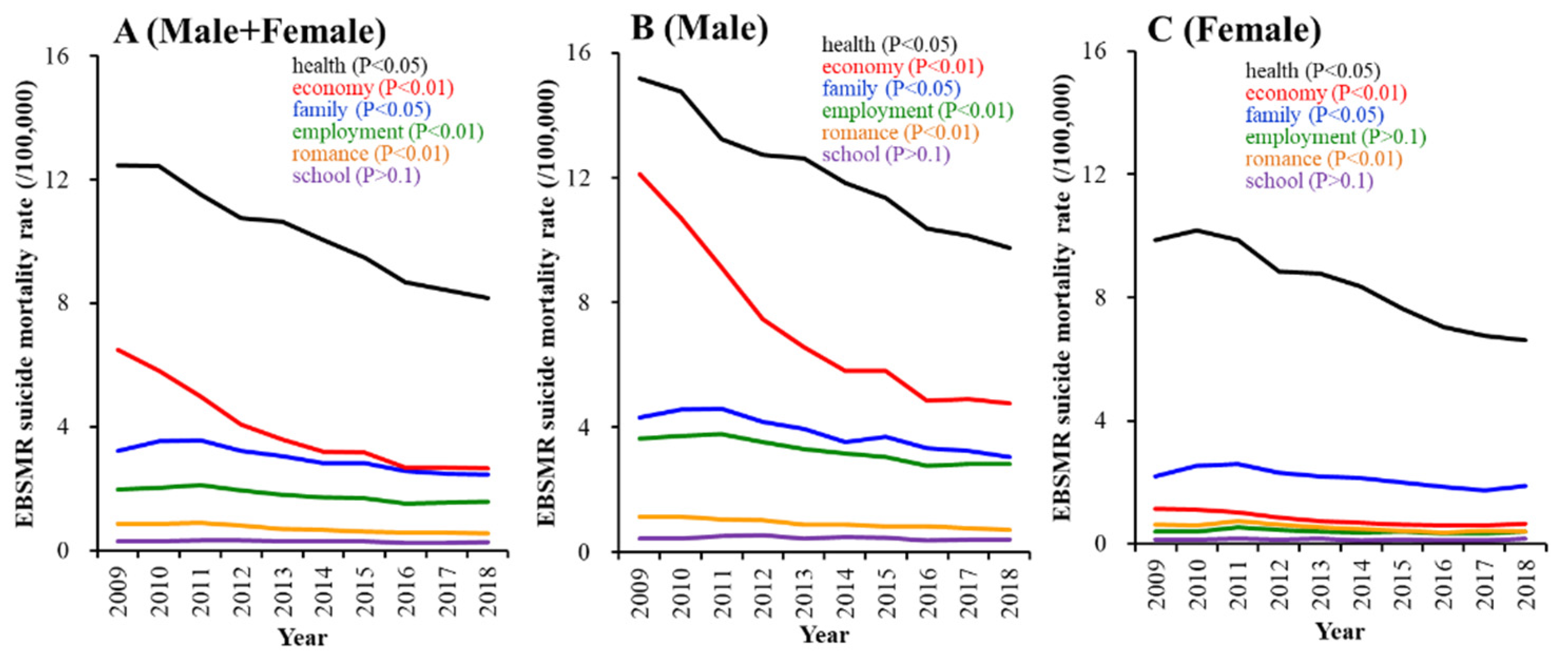
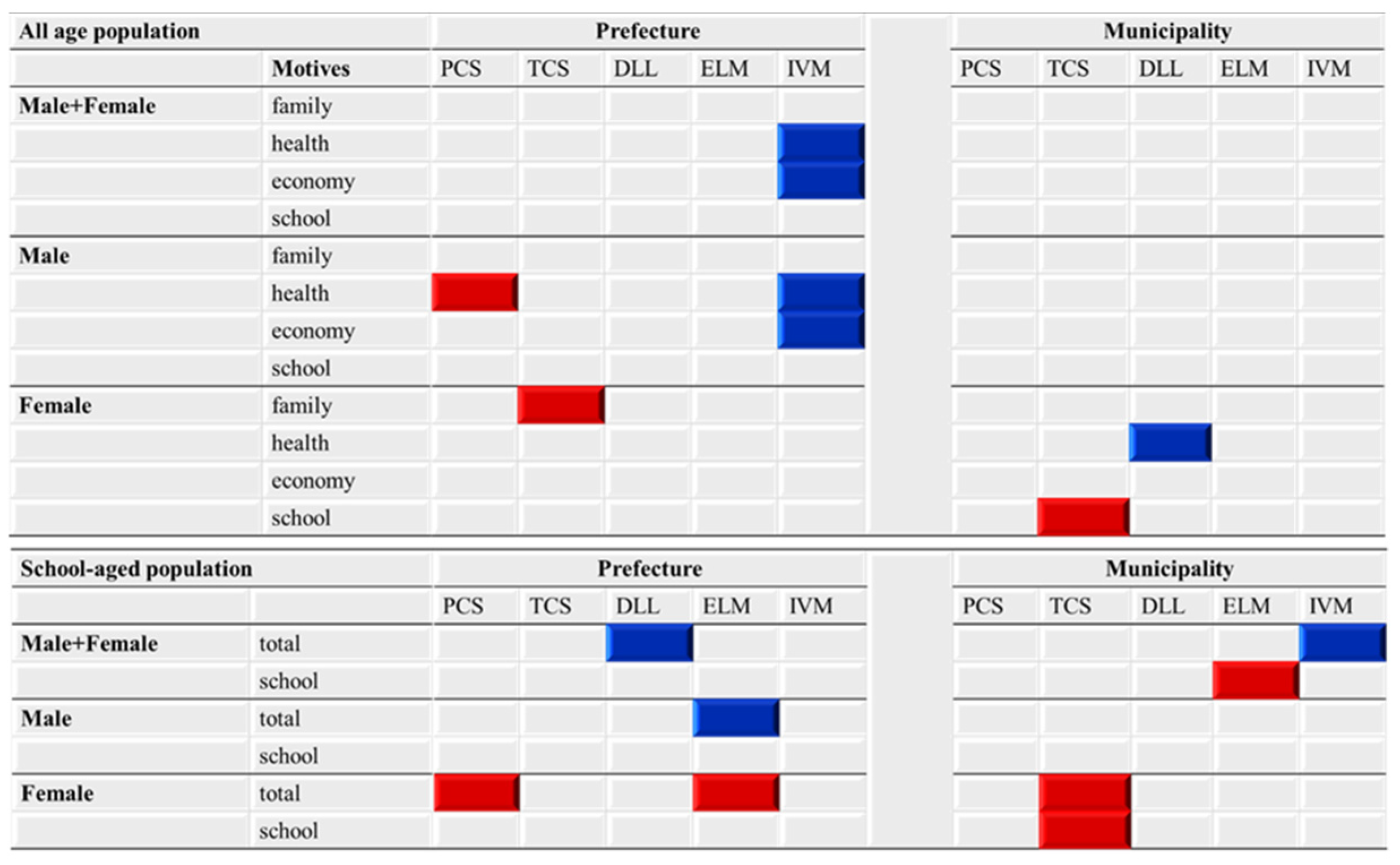
3.1. EBSMR Trends of Regional Suicide Mortality Associated with Six Suicide Motives between 2009 and 2018
3.2. Effects of Funding Amounts Provided to EFECBSC Sub-Divisions on EBSMR Trends of Suicide Mortalities Caused by Six Suicide Motives between 2009 and 2018
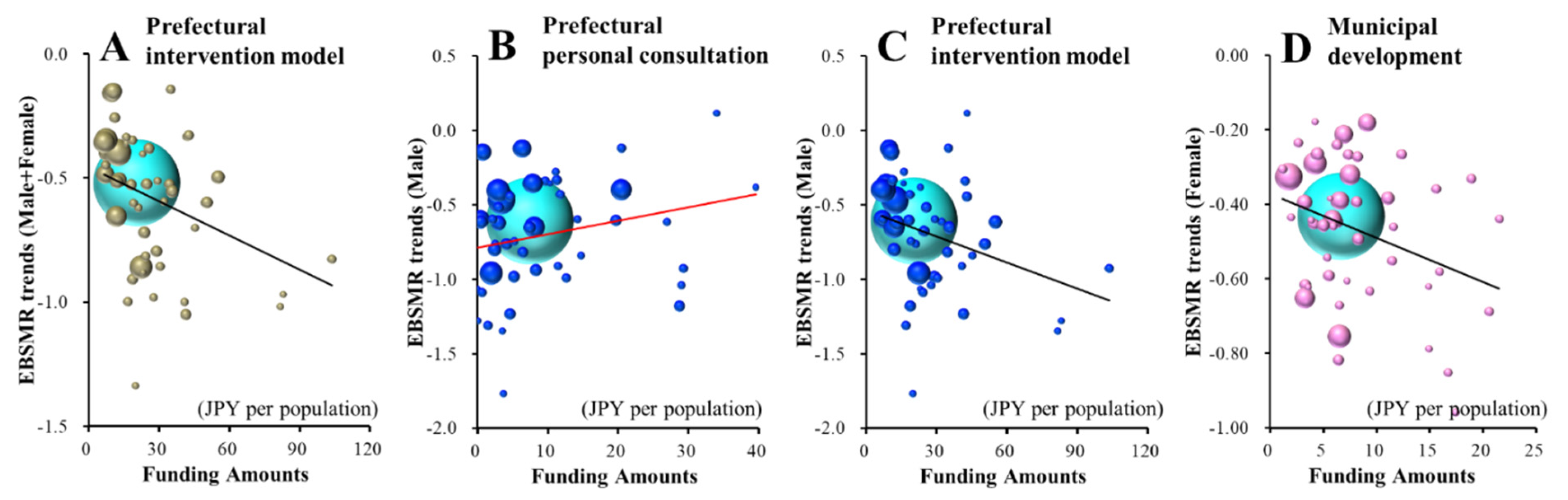
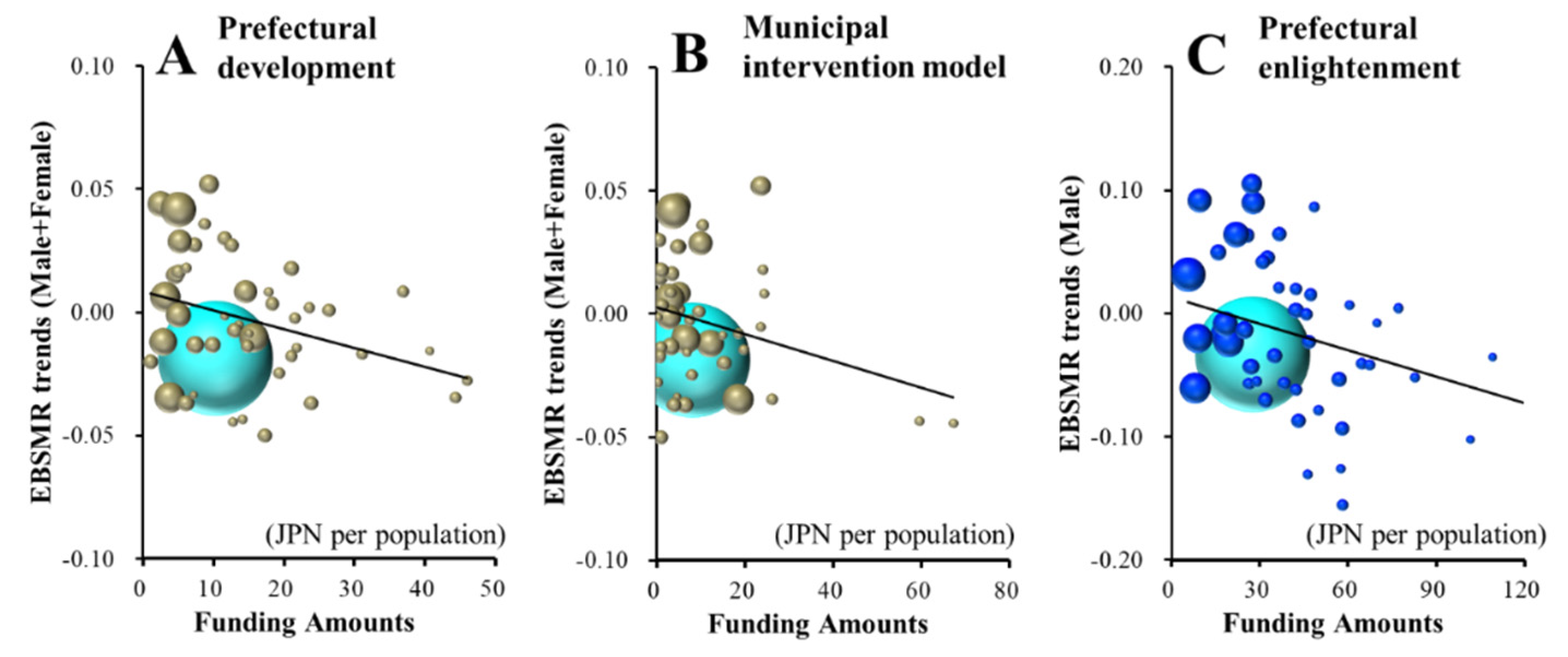
3.2.1. Effects of Amounts of Funding Provided to EFECBSC Sub-Divisions on EBSMR Trends of Suicide Mortalities Caused by Health-Related Motive between 2009 and 2018
3.2.2. Effects of Amounts of Funding Provided to EFECBSC Sub-Divisions on EBSMR Trends of Suicide Caused by Economy-Related Motives between 2009 and 2018
3.2.3. Effects of Amounts of Funding Provided to EFECBSC Sub-Divisions on EBSMR Trends of Suicide Caused by Family- and School-Related Motives between 2009 and 2018
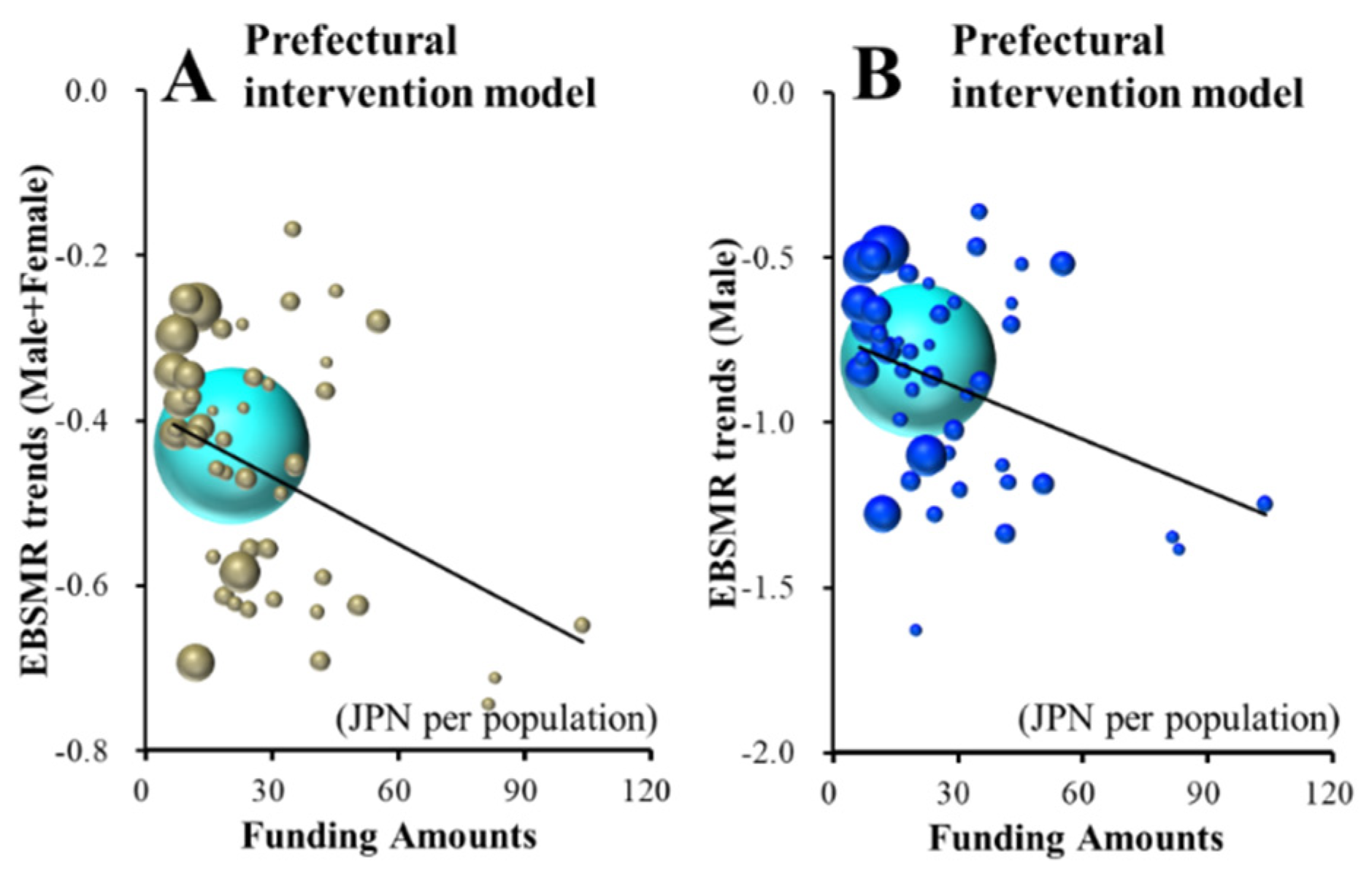
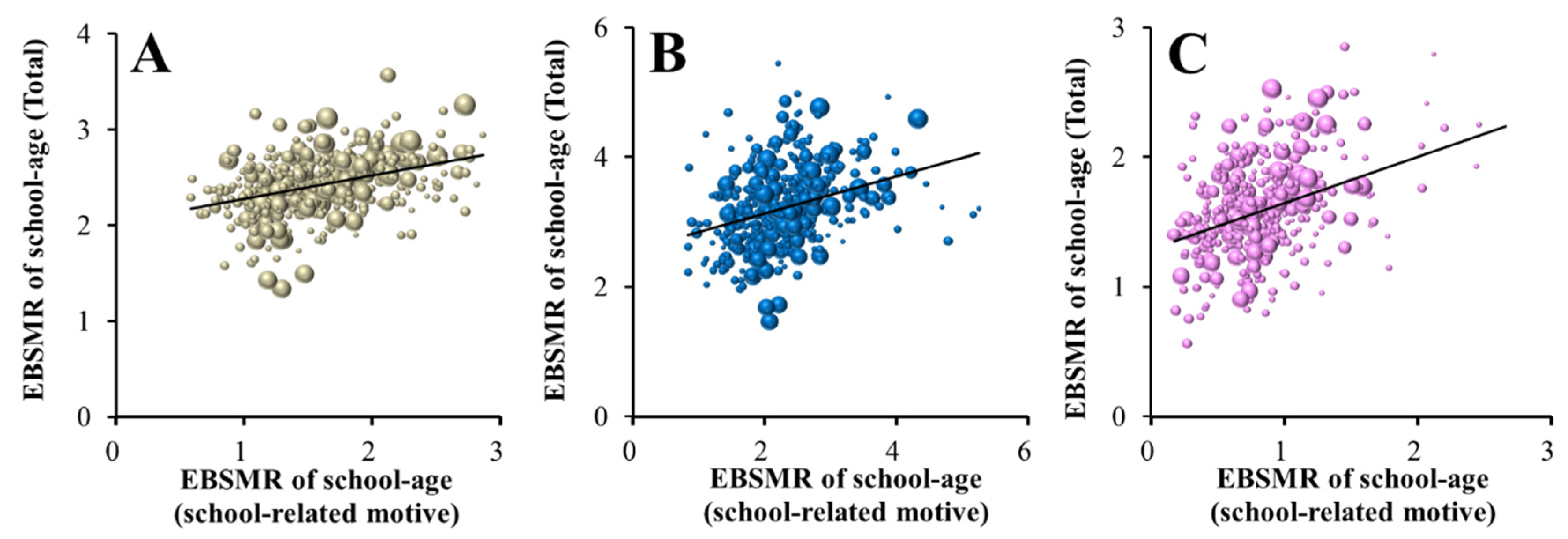
3.3. Effects of Amounts of Funding Provided to EFECBSC Sub-Divisions on EBSMR Trends of School-Aged Population between 2009 and 2018
3.3.1. Effects of Amounts of Funding Provided to EFECBSC Sub-Divisions on Male+Female and Male EBSMR Trends of School-Aged Population and Caused by School-Related Motive between 2009 and 2018
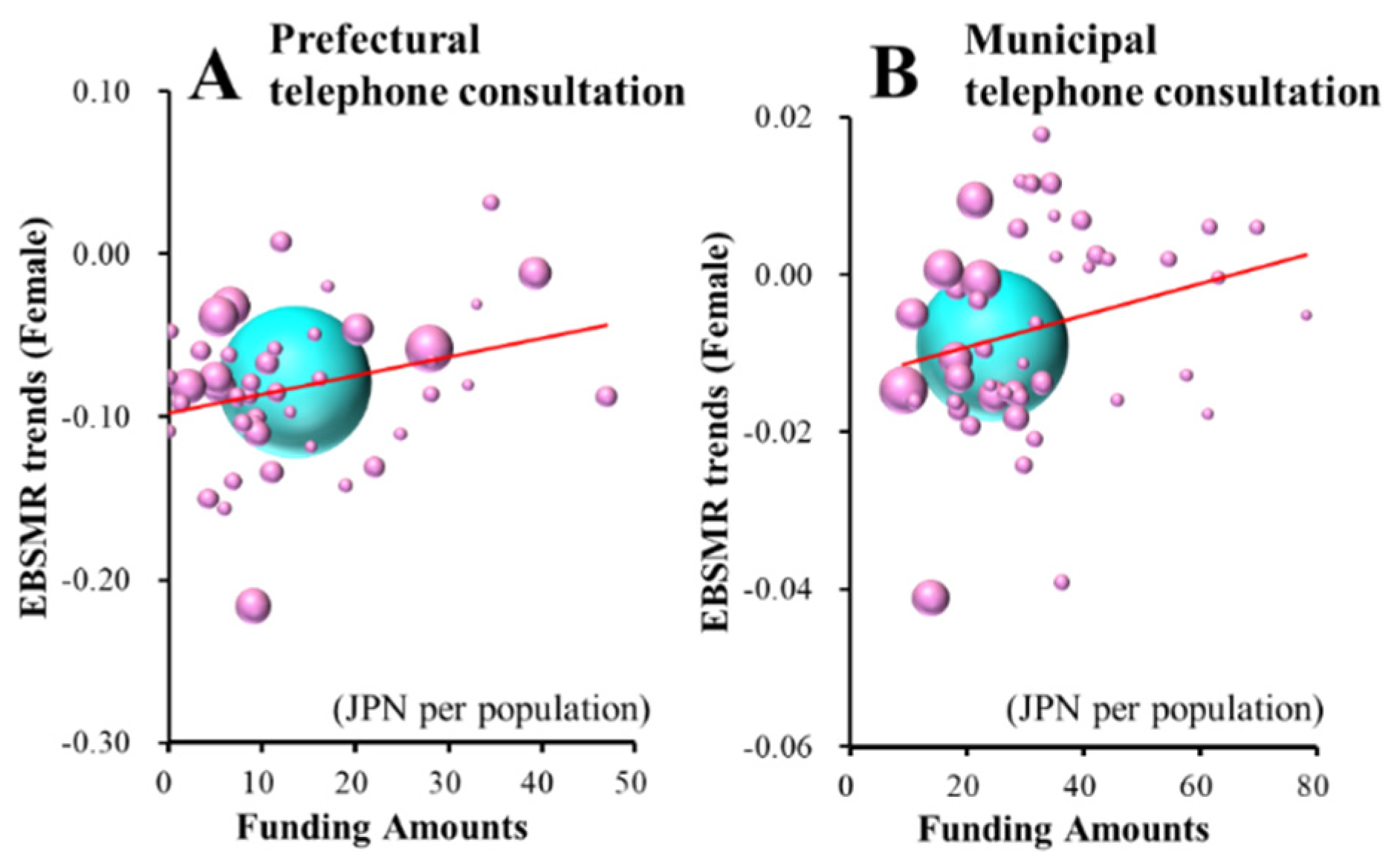
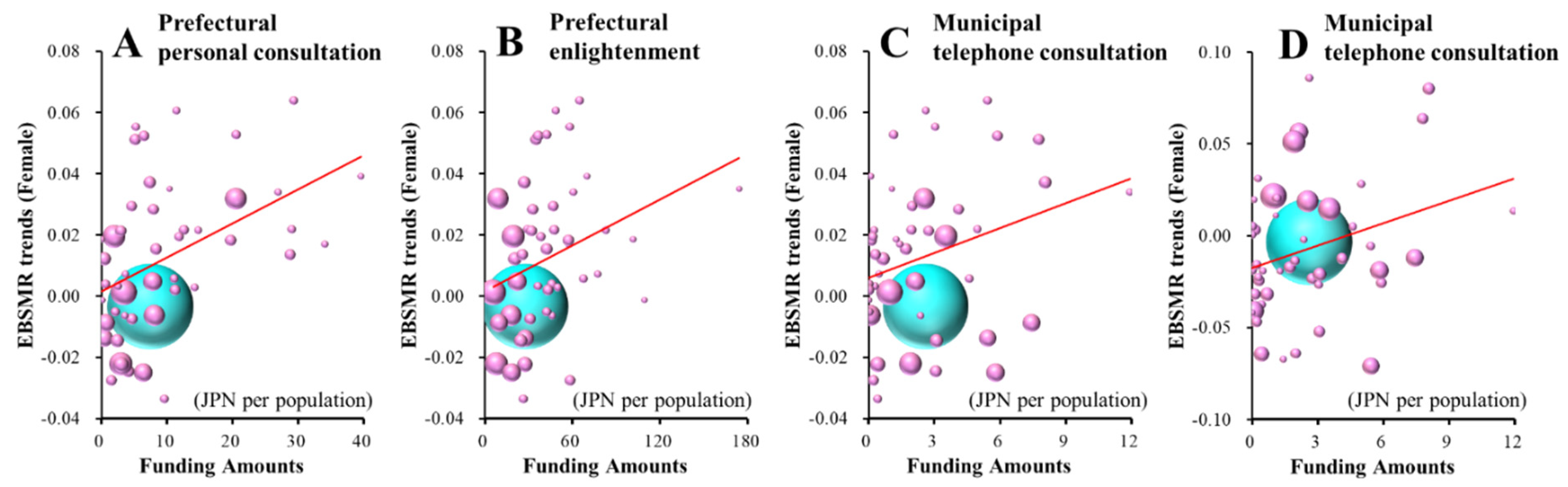
3.3.2. Effects of Amounts of Funding Provided to EFECBSC Sub-Divisions on Female EBSMR Trends of School-Aged Population and Caused by School-Related Motive between 2009 and 2018
4. Discussion
4.1. Effects of Amounts of Funding Provided to EFECBSC Sub-Divisions on Suicide Mortalities Caused by Suicide Motives between 2009 and 2018
4.2. Effects of Amounts of Funding Provided to EFECBSC Sub-Divisions on Suicide Mortalities of School-Aged Individuals between 2009 and 2018
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Preventing Suicide: A Resource for Filmmakers and Others Working on Stage and Screen. Available online: https://www.who.int/publications/i/item/preventing-suicide-a-resource-for-filmmakers-and-others-working-on-stage-and-screen (accessed on 18 November 2020).
- WHO. Preventing Suicide: A Global Imperative. Available online: https://www.who.int/publications/i/item/preventing-suicide-a-global-imperative (accessed on 18 November 2020).
- WHO. Suicide in the World. Available online: https://www.who.int/publications/i/item/suicide-in-the-world (accessed on 1 March 2021).
- WHO. Suicide Data. Available online: https://www.who.int/mental_health/prevention/suicide/countrydata/en/ (accessed on 1 December 2019).
- Kino, S.; Jang, S.N.; Gero, K.; Kato, S.; Kawachi, I. Age, period, cohort trends of suicide in japan and korea (1986–2015): A tale of two countries. Soc. Sci. Med. 2019, 235, 112385. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labor and Welfare. Basic Data on Suicide in the Region. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000140901.html (accessed on 17 March 2021).
- Okada, M.; Hasegawa, T.; Kato, R.; Shiroyama, T. Analysing regional unemployment rates, gdp per capita and financial support for regional suicide prevention programme on suicide mortality in japan using governmental statistical data. BMJ Open 2020, 10, e037537. [Google Scholar] [CrossRef]
- Kato, R.; Okada, M. Can financial support reduce suicide mortality rates? Int. J. Environ. Res. Public Health 2019, 16, 4797. [Google Scholar] [CrossRef]
- Nakanishi, M.; Yamauchi, T.; Takeshima, T. National strategy for suicide prevention in japan: Impact of a national fund on progress of developing systems for suicide prevention and implementing initiatives among local authorities. Psychiatry Clin. Neurosci. 2015, 69, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labor and Welfare. National Plan for Prevention of Suicide. Available online: https://www.mhlw.go.jp/kokoro/nation/about.html (accessed on 18 November 2020).
- Ministry of Health, Labor and Welfare. Regional Suicide Countermeasures Emergency Enhancement Fund. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/kyoukakikin.html (accessed on 18 November 2020).
- Ministry of Health, Labor and Welfare. 2020 White Paper on Suicide Prevention. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/jisatsuhakusyo2020.html (accessed on 14 November 2020).
- Shiratori, Y.; Tachikawa, H.; Nemoto, K.; Endo, G.; Aiba, M.; Matsui, Y.; Asada, T. Network analysis for motives in suicide cases: A cross-sectional study. Psychiatry Clin. Neurosci. 2014, 68, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Konick, L.C.; Gutierrez, P.M. Testing a model of suicide ideation in college students. Suicide Life Threat. Behav. 2005, 35, 181–192. [Google Scholar] [CrossRef]
- Neufeld, E.; O’Rourke, N. Impulsivity and hopelessness as predictors of suicide-related ideation among older adults. Can. J. Psychiatry 2009, 54, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Troister, T.; Holden, R.R. A two-year prospective study of psychache and its relationship to suicidality among high-risk undergraduates. J. Clin. Psychol. 2012, 68, 1019–1027. [Google Scholar] [CrossRef]
- Beck, A.T. Thinking and depression: I. Idiosyncratic content and cognitive distortions. Arch. Gen. Psychiatry 1963, 9, 324–333. [Google Scholar] [CrossRef]
- Beck, A.T.; Brown, G.; Berchick, R.J.; Stewart, B.L.; Steer, R.A. Relationship between hopelessness and ultimate suicide: A replication with psychiatric outpatients. Am. J. Psychiatry 1990, 147, 190–195. [Google Scholar] [CrossRef]
- Tanaka, E.; Sakamoto, S.; Ono, Y.; Fujihara, S.; Kitamura, T. Hopelessness in a community population: Factorial structure and psychosocial correlates. J. Soc. Psychol. 1998, 138, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Wu, K.C.; Yousuf, S.; Yip, P.S. Suicide in Asia: Opportunities and challenges. Epidemiol. Rev. 2012, 34, 129–144. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labor and Welfare. 2019 White Paper on Suicide Prevention. Available online: https://www.mhlw.go.jp/wp/hakusyo/jisatsu/19/index.html (accessed on 14 November 2020).
- Ministry of Health, Labor and Welfare. Law Concerning the Promotion of Research and the Utilization of the Results to Contribute to the Comprehensive and Effective Implementation of Suicide Countermeasures. Available online: https://elaws.e-gov.go.jp/search/elawsSearch/elaws_search/lsg0500/detail?lawId=501AC1000000032_20190912_000000000000000&openerCode=1 (accessed on 12 November 2019).
- Statistics Bureau of the Ministry of Internal Affairs and Communications. Labor Force Survey. Available online: https://www.stat.go.jp/data/roudou/pref/index.html (accessed on 21 January 2020).
- Statistics Bureau of the Ministry of Internal Affairs and Communications. Population, Demographics and Number of Households Based on Basic Resident Register. Available online: http://www.soumu.go.jp/main_sosiki/jichi_gyousei/daityo/jinkou_jinkoudoutai-setaisuu.html (accessed on 18 November 2020).
- Kawaguchi, H.; Koike, S. Association between the density of physicians and suicide rates in japan: Nationwide ecological study using a spatial bayesian model. PLoS ONE 2016, 11, e0148288. [Google Scholar] [CrossRef]
- Shimizu, H. An introduction to the statistical free software had: Suggestions to improve teaching, learning and practice data analysis. J. Media Inf. Commun. 2016, 1, 59–73. [Google Scholar]
- Terada, M. Effect of individual differences in construal level on procrastination: Moderating role of intelligence theories. Psychology 2017, 8, 517–525. [Google Scholar] [CrossRef]
- Fukuyama, K.; Kato, R.; Murata, M.; Shiroyama, T.; Okada, M. Clozapine normalizes a glutamatergic transmission abnormality induced by an impaired nmda receptor in the thalamocortical pathway via the activation of a group iii metabotropic glutamate receptor. Biomolecules 2019, 9, 234. [Google Scholar] [CrossRef]
- Nakano, T.; Hasegawa, T.; Suzuki, D.; Motomura, E.; Okada, M. Amantadine combines astroglial system xc(-) activation with glutamate/nmda receptor inhibition. Biomolecules 2019, 9, 191. [Google Scholar] [CrossRef]
- Okada, M.; Fukuyama, K.; Nakano, T.; Ueda, Y. Pharmacological discrimination of effects of mk801 on thalamocortical, mesothalamic, and mesocortical transmissions. Biomolecules 2019, 9, 746. [Google Scholar] [CrossRef]
- Stack, S.J.S.; Behavior, L.T. Suicide: A 15-year review of the sociological literature part i: Cultural and economic factors. Suicide Life Threat. Behav. 2000, 30, 145–162. [Google Scholar]
- Ministry of Health, Labor and Welfare. Bugets for Suicide Prevention Programmes. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000133838.html (accessed on 12 November 2019).
- Rambotti, S. Is there a relationship between welfare-state policies and suicide rates? Evidence from the U.S. States, 2000–2015. Soc. Sci. Med. 2020, 246, 112778. [Google Scholar] [CrossRef] [PubMed]
- Mattei, G.; Pistoresi, B.; De Vogli, R. Impact of the economic crises on suicide in italy: The moderating role of active labor market programs. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 201–208. [Google Scholar] [CrossRef]
- Mattei, G.; Pistoresi, B. Unemployment and suicide in italy: Evidence of a long-run association mitigated by public unemployment spending. Eur. J. Health Econ. HEPAC Health Econ. Prev. Care 2019, 20, 569–577. [Google Scholar] [CrossRef]
- Cylus, J.; Glymour, M.M.; Avendano, M. Do generous unemployment benefit programs reduce suicide rates? A state fixed-effect analysis covering 1968–2008. Am. J. Epidemiol. 2014, 180, 45–52. [Google Scholar] [CrossRef]
- Ross, J.M.; Yakovlev, P.A.; Carson, F. Does state spending on mental health lower suicide rates? 2012, 41, 408–417. J. Soc.-Econ. 2012, 41, 408–417. [Google Scholar] [CrossRef]
- Doki, S.; Kaneko, H.; Oi, Y.; Usami, K.; Sasahara, S.; Matsuzaki, I. Risk factors for suicidal ideation among telephone crisis hotline callers in japan. Crisis 2016, 37, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Ohtaki, Y.; Oi, Y.; Doki, S.; Kaneko, H.; Usami, K.; Sasahara, S.; Matsuzaki, I. Characteristics of telephone crisis hotline callers with suicidal ideation in japan. Suicide Life Threat. Behav. 2017, 47, 54–66. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, S.L.; Uddin, R.; Brady, M.; Batchelor, S.; Ross, V.; Spence, S.H.; Watling, D.; Kolves, K. Systematic review: The state of research into youth helplines. J. Am. Acad. Child Adolesc. Psychiatry 2020. [Google Scholar] [CrossRef] [PubMed]
- Gould, M.S.; Kalafat, J.; Harrismunfakh, J.L.; Kleinman, M. An evaluation of crisis hotline outcomes. Part 2: Suicidal callers. Suicide Life Threat. Behav. 2007, 37, 338–352. [Google Scholar] [CrossRef]
- Lapierre, S.; Erlangsen, A.; Waern, M.; De Leo, D.; Oyama, H.; Scocco, P.; Gallo, J.; Szanto, K.; Conwell, Y.; Draper, B.; et al. A systematic review of elderly suicide prevention programs. Crisis 2011, 32, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Oyama, H.; Goto, M.; Fujita, M.; Shibuya, H.; Sakashita, T. Preventing elderly suicide through primary care by community-based screening for depression in rural japan. Crisis 2006, 27, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Oyama, H.; Koida, J.; Sakashita, T.; Kudo, K. Community-based prevention for suicide in elderly by depression screening and follow-up. Community Ment. Health J. 2004, 40, 249–263. [Google Scholar] [CrossRef]
- Oyama, H.; Sakashita, T.; Ono, Y.; Goto, M.; Fujita, M.; Koida, J. Effect of community-based intervention using depression screening on elderly suicide risk: A meta-analysis of the evidence from japan. Community Ment. Health J. 2008, 44, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Oyama, H.; Watanabe, N.; Ono, Y.; Sakashita, T.; Takenoshita, Y.; Taguchi, M.; Takizawa, T.; Miura, R.; Kumagai, K. Community-based suicide prevention through group activity for the elderly successfully reduced the high suicide rate for females. Psychiatry Clin. Neurosci. 2005, 59, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Drapeau, A.; Boyer, R.; Lesage, A. The influence of social anchorage on the gender difference in the use of mental health services. J. Behav. Health Serv. Res. 2009, 36, 372–384. [Google Scholar] [CrossRef] [PubMed]
- Du, L.; Shi, H.Y.; Qian, Y.; Jin, X.H.; Li, Y.; Yu, H.R.; Liu, X.M.; Fu, X.L.; Chen, H.L. Association between social support and suicidal ideation in patients with cancer: A systematic review and meta-analysis. Eur. J. Cancer Care 2020, 30, e13382. [Google Scholar]
- Kyung, Y.; Choi, M.H.; Jeon, Y.J.; Lee, J.S.; Lee, J.H.; Jo, S.H.; Kim, S.H. Association of atopic dermatitis with suicide risk among 788,411 adolescents: A korean cross-sectional study. Ann. Allergy Asthma Immunol. 2020, 125, 55–64. [Google Scholar] [CrossRef]
- Vazquez-Ortiz, M.; Angier, E.; Blumchen, K.; Comberiati, P.; Duca, B.; DunnGalvin, A.; Gore, C.; Hox, V.; Jensen, B.; Pite, H.; et al. Understanding the challenges faced by adolescents and young adults with allergic conditions: A systematic review. Allergy 2020, 75, 1850–1880. [Google Scholar] [CrossRef]
- Karimi, L.; Hoppe, D.; Burdick, C.; Buultjens, M.; Wijeratne, T.; Crewther, S.G. Recent evidence regarding the association between migraine and suicidal behaviors: A systematic review. Front. Neurol. 2020, 11, 490. [Google Scholar] [CrossRef]
- Natale, P.; Palmer, S.C.; Ruospo, M.; Saglimbene, V.M.; Rabindranath, K.S.; Strippoli, G.F. Psychosocial interventions for preventing and treating depression in dialysis patients. Cochrane Database Syst. Rev. 2019, 12, CD004542. [Google Scholar] [CrossRef]
- Ingram, S.; Ringle, J.L.; Hallstrom, K.; Schill, D.E.; Gohr, V.M.; Thompson, R.W. Coping with crisis across the lifespan: The role of a telephone hotline. J. Child. Fam. Stud. 2008, 17, 663–674. [Google Scholar] [CrossRef]
- Fukkink, R.G.; Bruns, S.; Ligtvoet, R. Voices of children from around the globe; an international analysis of children’s issues at child helplines. Child. Soc. 2016, 30, 510–519. [Google Scholar] [CrossRef]
- Mishara, B.L.; Chagnon, F.; Daigle, M.; Balan, B.; Raymond, S.; Marcoux, I.; Bardon, C.; Campbell, J.K.; Berman, A. Comparing models of helper behavior to actual practice in telephone crisis intervention: A silent monitoring study of calls to the U.S. 1-800-suicide network. Suicide Life Threat. Behav. 2007, 37, 291–307. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Education, Culture, Sports, Science and Technology. 2017 White Paper on Education, Culture, Sports, Science and Technology. Available online: https://warp.ndl.go.jp/info:ndljp/pid/11509864/www.mext.go.jp/b_menu/hakusho/html/hpab201701/1417254.htm (accessed on 31 January 2021).
- Ministry of Education, Culture, Sports, Science and Technology. School Basic Survey. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00400001&kikan=00400&tstat=000001011528&cycle=0&tclass1=000001148386&tclass2=000001148404&tclass3=000001148405&tclass4=000001148409&tclass5val=0 (accessed on 31 January 2021).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Motives for Suicide | Male | Female |
| Total | 69.8 ± 3.0 (79.1–59.6) | 30.2 ± 3.0 (40.4–20.9) |
| Health | 58.9 ± 5.2 (78.2–40.5) | 41.1 ± 5.2 (59.5–21.8) |
| Economy | 89.0 ± 7.1 (100.0–60.0) | 11.0 ± 7.1 (40.0–0.0) |
| Family | 64.4 ± 8.0 (92.9–37.5) | 35.7 ± 8.0 (62.5–7.1) |
| Employment | 89.0 ± 7.1 (100.0–57.1) | 11.0 ± 7.1 (42.9–0.0) |
| Romance | 65.4 ± 17.2 (100.0–0.0) | 34.6 ± 17.2 (100.0–0.0) |
| School | 75.0 ± 25.2 (100.0–0.0) | 25.1 ± 25.2 (100.0–0.0) |
| Male+Female | Adjusted R2 | F | p | Factor | β | p | VIF | |
|---|---|---|---|---|---|---|---|---|
| health | 0.087 | 5.405 | 0.025 | Prefectural | Intervention model | −0.327 | 0.05 | 1.000 |
| economy | 0.104 | 6.316 | 0.016 | Prefectural | Intervention model | −0.351 | 0.016 | 1.000 |
| Male | Adjusted R2 | F | p | Factor | β | p | VIF | |
| health | 0.150 | 5.066 | 0.010 | Prefectural | Intervention model | −0.364 | 0.05 | 1.024 |
| Prefectural | Personal consultation | +0.297 | 0.05 | 1.024 | ||||
| economy | 0.108 | 6.551 | 0.014 | Prefectural | Intervention model | −0.356 | 0.05 | 1.100 |
| Female | Adjusted R2 | F | p | Factor | β | p | VIF | |
| family | 0.066 | 4.228 | 0.046 | Prefectural | Telephone consultation | +0.293 | 0.05 | 1.000 |
| health | 0.086 | 5.431 | 0.025 | Municipal | Development leaders/listeners | −0.326 | 0.05 | 1.000 |
| school | 0.063 | 4117 | 0.048 | Municipal | Telephone consultation | +0.290 | 0.05 | 1.000 |
| Male+Female | Adjusted R2 | F | p | Factor | β | p | VIF | |
|---|---|---|---|---|---|---|---|---|
| Total | 0.167 | 5.625 | 0.001 | Prefectural | Development leaders/listeners | −0.344 | 0.05 | 1.00 |
| Municipal | Intervention model | −0.301 | 0.05 | 1.00 | ||||
| Male | Adjusted R2 | F | p | Factor | β | p | VIF | |
| Total | 0.109 | 6.600 | 0.014 | Prefectural | Enlightenment | −0.358 | 0.05 | 1.009 |
| Female | Adjusted R2 | F | p | Factor | β | p | VIF | |
| Total | 0.306 | 5.766 | 0.004 | Prefectural | Personal consultation | +0.375 | 0.01 | 1.031 |
| Prefectural | Enlightenment | +0.304 | 0.01 | 1.045 | ||||
| Municipal | Telephone consultation | +0.321 | 0.05 | 1.059 | ||||
| School-related motives | 0.071 | 4.517 | 0.039 | Municipal | Telephone consultation | +0.302 | 0.05 | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakano, T.; Hasegawa, T.; Okada, M. Analysing the Impacts of Financial Support for Regional Suicide Prevention Programmes on Suicide Mortality Caused by Major Suicide Motives in Japan Using Statistical Government Data. Int. J. Environ. Res. Public Health 2021, 18, 3414. https://doi.org/10.3390/ijerph18073414
Nakano T, Hasegawa T, Okada M. Analysing the Impacts of Financial Support for Regional Suicide Prevention Programmes on Suicide Mortality Caused by Major Suicide Motives in Japan Using Statistical Government Data. International Journal of Environmental Research and Public Health. 2021; 18(7):3414. https://doi.org/10.3390/ijerph18073414
Chicago/Turabian StyleNakano, Tomosuke, Toshiki Hasegawa, and Motohiro Okada. 2021. "Analysing the Impacts of Financial Support for Regional Suicide Prevention Programmes on Suicide Mortality Caused by Major Suicide Motives in Japan Using Statistical Government Data" International Journal of Environmental Research and Public Health 18, no. 7: 3414. https://doi.org/10.3390/ijerph18073414