
Effects of COVID-19 Lockdown on Physical Activity, Sedentary Behavior, and Satisfaction with Life in Qatar: A Preliminary Study

 ,
,  , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size
2.2. Survey Development, Promotion, and Distribution
2.3. Data Privacy/Security
2.4. International Physical Activity Questionnaire Short Form (IPAQ-SF)
2.5. Satisfaction with Life Questionnaire (SLQ)
2.6. Statistical Analyses
3. Results
3.1. Sample Description
3.2. International Physical Activity Questionnaire Short Form (IPAQ-SF)—Testing of Hypotheses 1 and 2
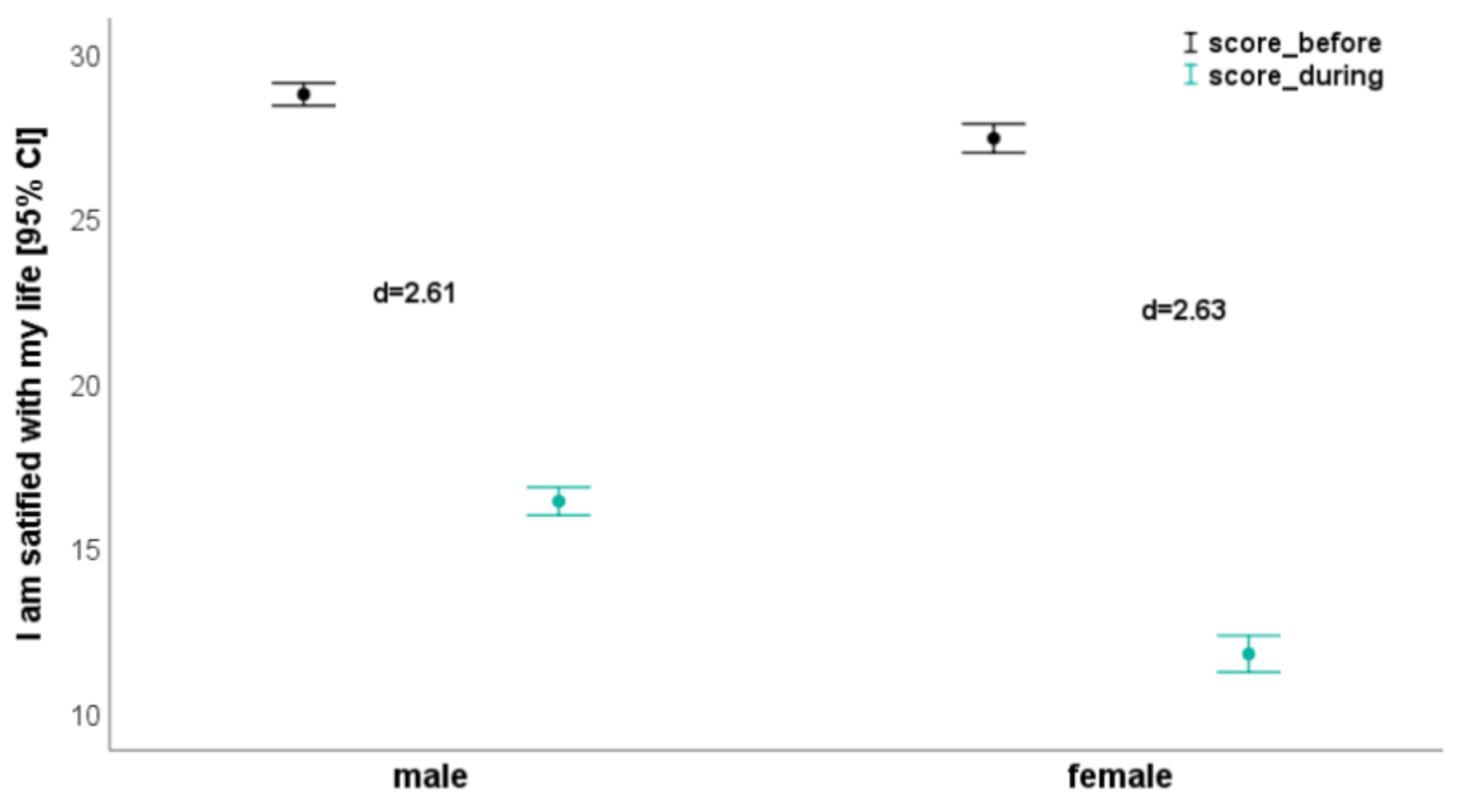
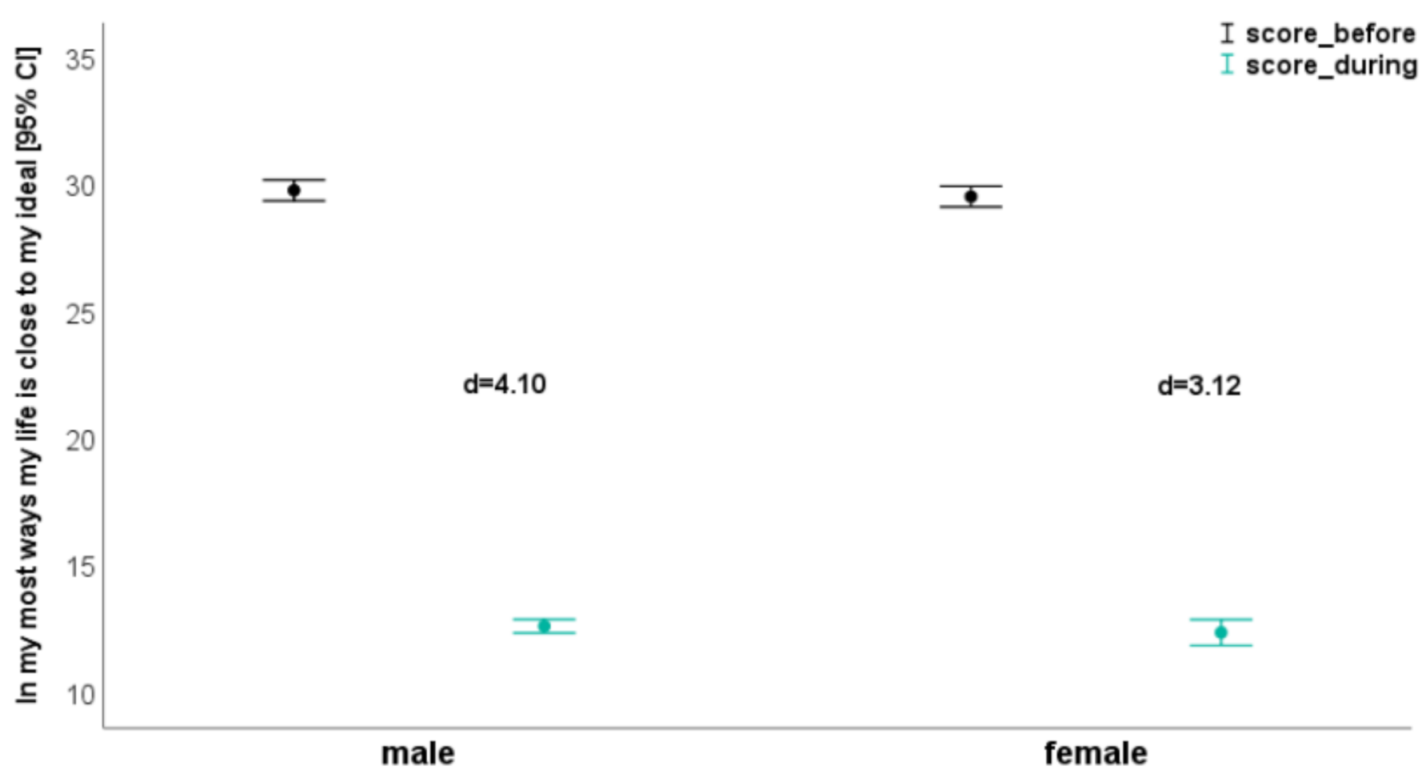
3.3. Satisfaction with Life Questionnaire (SLQ)—Testing of Hypothesis 3
4. Discussion
4.1. Impact of COVID 19 on Physical Activity
4.2. Impact COVID 19 on Life Satisfaction
4.3. Strengths, Limitations, and Perspective
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hossain, M.M.; Sultana, A.; Purohit, N. Mental health outcomes of quarantine and isolation for infection prevention: A systematic umbrella review of the global evidence. Epidemiol. Health 2020, 42, e2020038. [Google Scholar] [CrossRef]
- Ammar, A.; Chtourou, H.; Boukhris, O.; Trabelsi, K.; Masmoudi, L.; Brach, M.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. COVID-19 Home Confinement Negatively Impacts Social Participation and Life Satisfaction: A Worldwide Multicenter Study. Int. J. Environ. Res. Public Health 2020, 17, 6237. [Google Scholar] [CrossRef]
- Bloch, W.; Halle, M.; Steinacker, J.M. Sport in times of Corona. Ger. J. Sports Med. 2020, 71, 83–84. [Google Scholar] [CrossRef]
- Slimani, M.; Paravlic, A.; Mbarek, F.; Bragazzi, N.L.; Tod, D. The relationship between physical activity and quality of life during the confinement induced by COVID-19 Outbreak: A Pilot Study in Tunisia. Front. Psychol. 2020, 11, 1882. [Google Scholar] [CrossRef] [PubMed]
- Steinacker, J.M.; Bloch, W.; Halle, M.; Mayer, F.; Meyer, T.; Hirschmüller, A.; Roecker, K.; Wolfarth, B.; Nieß, A.; Reinsberger, C. Merkblatt: Gesundheitssituation für Sportler durch die aktuelle Coronavirus-Pandemie (SARS-CoV-2/COVID-19). Dtsch. Z. Sportmed. 2020, 71, 85–86. [Google Scholar] [CrossRef]
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Coronavirus disease (COVID-19): The need to maintain regular physical activity while taking precautions. J. Sport Health Sci. 2020, 9, 103–104. [Google Scholar] [CrossRef] [PubMed]
- Lau, H.M.-C.; Lee, E.W.-C.; Wong, C.N.-C.; Ng, G.Y.-F.; Jones, A.Y.-M.; Hui, D.S.C. The Impact of Severe Acute Respiratory Syndrome on the Physical Profile and Quality of Life. Arch. Phys. Med. Rehabil. 2005, 86, 1134–1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arora, T.; Grey, I. Health behaviour changes during COVID-19 and the potential consequences: A mini-review. J. Health Psychol. 2020, 25, 1155–1163. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Bulzing, R.A.; Meyer, J.; Vancampfort, D.; Firth, J.; Stubbs, B.; Grabovac, I.; Willeit, P.; Tavares, V.D.; Calegaro, V.C.; et al. Associations of moderate to vigorous physical activity and sedentary behavior with depressive and anxiety symptoms in self-isolating people during the COVID-19 pandemic: A cross-sectional survey in Brazil. Psychiatry Res. 2020, 292, 113339. [Google Scholar] [CrossRef] [PubMed]
- Ingram, J.; Maciejewski, G.; Hand, C.J. Changes in Diet, Sleep, and Physical Activity Are Associated With Differences in Negative Mood During COVID-19 Lockdown. Front. Psychol. 2020, 2, 588604. [Google Scholar] [CrossRef]
- Ammar, A.; Mueller, P.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Brach, M.; Schmicker, M.; Bentlage, E.; et al. Psychological consequences of COVID-19 home confinement: The ECLB-COVID19 multicenter study. PLoS ONE 2020, 15, e0240204. [Google Scholar] [CrossRef] [PubMed]
- Lesser, I.A.; Nienhuis, C.P. The Impact of COVID-19 on Physical Activity Behavior and Well-Being of Canadians. Int. J. Environ. Res. Public Health 2020, 17, 3899. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Fuentes-García, J.P.; Martínez Patiño, M.J.; Villafaina, S.; Clemente-Suárez, V.J. The effect of COVID-19 confinement in behavioral, psychological, and training patterns of chess players. Front. Psychol. 2020, 11, 1812. [Google Scholar] [CrossRef] [PubMed]
- Altena, E.; Baglioni, C.; Espie, C.A.; Ellis, J.; Gavriloff, D.; Holzinger, B.; Schlarb, A.; Frase, L.; Susanna, J.; Riemann, D. Dealing with sleep problems during home confinement due to the COVID-19 outbreak: Practical recommendations from a task force of the European CBT-I Academy. J. Sleep Res. 2020, 4, e13052. [Google Scholar] [CrossRef]
- Ning, L.; Niu, J.; Bi, X.; Yang, C.; Liu, Z.; Wu, Q.; Ning, N.; Liang, L.; Liu, A.; Hao, Y.; et al. The impacts of knowledge, risk perception, emotion and information on citizens’ protective behaviors during the outbreak of COVID-19: A cross-sectional study in China. BMC Public Health 2020, 20, 1751. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Contry Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the international physical activity questionnaire short from (PAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitley, E.; Ball, J. Statistics Review 4: Sample Size Calculations. Crit. Care 2002, 6, 335–341. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Ma, Z.F. Impact of the COVID-19 Pandemic on Mental Health and Quality of Life among Local Residents in Liaoning Province, China: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 2381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Bortz, J. (Ed.) Basic principle of one-factorial analysis of variance. In Statistics for Social Scientists; Springer: Berlin/Heidelberg, Germany; New York, NY, USA, 1999; pp. 237–249. [Google Scholar]
- Hartmann, A.; Herzog, T.; Drinkmann, A. Psychotherapy of bulimia nervosa: What is effective? A meta-analysis. J. Psychosom. Res. 1992, 36, 159–167. [Google Scholar] [CrossRef]
- Cohen, J. The effect size. In Statistical Power Analysis for the Behavioural Sciences; Taylor & Francis: Abingdon, UK, 1988; pp. 77–83. [Google Scholar]
- Richardson, J.T.E. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Lancet Physical Activity Series Working, G. Effect of physical inactivity on major non- communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Tremblay, M.S.; Warburton, D.E.; Janssen, I.; Paterson, D.H.; Latimer, A.E.; Rhodes, R.E.; Kho, M.E.; Hicks, A.; LeBlanc, A.G.; Zehr, L.; et al. New Canadian physical activity guidelines. Appl. Physiol. Nutr. Metab. 2011, 36, 36–46. [Google Scholar] [CrossRef] [PubMed]
- King, A.C.; Powell, K.E.; Kraus, W.E. The US physical activity guidelines advisory committee report-introduction. Med. Sci. Sports Exerc. 2019, 51, 1203–1205. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Naming The Coronavirus Disease (COVID-19) and The Virus that Causes it; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Ammar, A.; Trabelsi, K.; Brach, M.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of home confinement on mental health and lifestyle behaviours during the COVID-19 outbreak: Insight from the ECLB-COVID19 multicenter study. Biol. Sport 2020, 38, 37–44. [Google Scholar]
- Giustino, V.; Parroco, A.M.; Gennaro, A.; Musumeci, G.; Palma, A.; Battaglia, G. Physical Activity Levels and Related Energy Expenditure during COVID-19 Quarantine among the Sicilian Active Population: A Cross-Sectional Online Survey Study. Sustainability 2020, 12, 4356. [Google Scholar] [CrossRef]
- Jukic, I.; Calleja-González, J.; Cos, F.; Cuzzolin, F.; Olmo, J.; Terrados, N.; Njaradi, N.; Sassi, R.; Requena, B.; Milanovic, L.; et al. Strategies and Solutions for Team Sports Athletes in Isolation due to COVID-19. Sports 2020, 8, 56. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.A.; Pranata, R. Sports activities during any pandemic lockdown. Ir. J. Med. Sci. 2020, 1–5. [Google Scholar] [CrossRef]
- Yeo, T.J. Sport and exercise during and beyond the COVID-19 pandemic. Eur. J. Prev. Cardiol. 2020, 27, 1239–1241. [Google Scholar] [CrossRef]
- Myer, G.D.; Faigenbaum, A.D.; Cherny, C.E.; Heidt, R.S.; Hewett, T.E. Did the NFL Lockout expose the Achilles heel of competitive sports? J. Orthop. Sports Phys. Ther. 2011, 41, 702–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pillay, L.; van Rensburg, D.C.; van Rensburg, A.J.; Ramagole, D.A.; Holtzhausen, L.; Dijkstra, H.P.; Cronje, T. Nowhere to hide: The significant impact of coronavirus disease 2019 (COVID-19) measures on elite and semi-elite South African athletes. J. Sci. Med. Sport 2020, 23, 670–679. [Google Scholar] [CrossRef]
- Alajmi, J.; Jeremijenko, A.M.; Abraham, J.C.; Alishaq, M.; Concepcion, E.G.; Butt, A.A.; Abou-Samra, A.B. COVID-19 infection among healthcare workers in a national healthcare system: The Qatar experience. Int. J. Infect. Dis. 2020, 100, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Al Kuwari, H.M.; Rahim, H.F.A.; Abu-Raddad, L.J.; Abou-Samra, A.B.; Al Kanaani, Z.; Al Khal, A.; Butt, A.A. Epidemiological investigation of the first 5685 cases of SARS-CoV-2 infection in Qatar, 28 February–18 April 2020. BMJ Open 2020, 10, e040428. [Google Scholar] [CrossRef] [PubMed]
- Pancani, L.; Marinucci, M.; Aureli, N.; Riva, P. Forced social isolation and mental health: A study on 1006 Italians under COVID-19 quarantine. PsyArXiv 2020, Preprint. [Google Scholar]
- Lima, C.K.; de Medeiros Carvalho, P.M.; Lima, I.D.; de Oliveira Nunes, J.V.; Saraiva, J.S.; de Souza, R.I.; da Silva, C.G.; Neto, M.L. The emotional impact of Coronavirus 2019-nCoV (new Coronavirus disease). Psychiatry Res. 2020, 287, 112915. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.X.; Tower, N. Unprecedented disruptions of lives and work—A survey of the health, distress and life satisfaction of working adults in China one month into the COVID-19 outbreak. Psychiatry Res. 2020, 288, 112958. [Google Scholar] [CrossRef] [PubMed]
- Lima, C.K.; de Medeiros Carvalho, P.M.; Lima, I.D.; de Oliveira Nunes, J.V.; Saraiva, J.S.; de Souza, R.I.; da Silva, C.G.; Neto, M.L. Effects of COVID-19 home confinement on eating behaviour and physical activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Zahra, D.; Sadatmahalleh, S.J.; Samaneh, Y.; Mahnaz, B.K.; Anoshiravan, K. Influential Factors on Quality of Life in Married Iranian Women during the Covid-19 Pandemic in 2020: A Path Analysis 2020. Available online: https://assets.researchsquare.com/files/rs-27439/v1/605f054d-948c-4f39-99ee-d967d1fb95da.pdf (accessed on 11 August 2020).
- Guhl, E.; Althouse, A.; Sharbaugh, M.; Pusateri, A.M.; Paasche-Orlow, M.; Magnani, J.W. Association of income and health-related quality of life in atrial fibrillation. Open Heart 2019, 6, e000974. [Google Scholar] [CrossRef] [Green Version]
- Mak, W.W.S.; Law, R.W.; Woo, J.; Cheung, F.M.; Lee, D. Social support and psychological adjustment to SARS: The mediating role of self-care self-efficacy. Psychol. Health 2009, 24, 161–174. [Google Scholar] [CrossRef] [PubMed]
- Qi, M.; Li, P.; Moyle, W.; Weeks, B.; Jones, C. Physical Activity, Health-Related Quality of Life, and Stress among the Chinese Adult Population during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6494. [Google Scholar] [CrossRef] [PubMed]
- Tsang, C.D. An exploratory study of the impact of stress on quality of life among front-line nursing staff working in respiratory fever admission wards (RFAWs) and general medical wards (GMWs). J. Appl. Phys. Lett. 2008, 92, 191105. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 1144) | Male (n = 588) | Female (n = 556) | p | ηp2 | |
|---|---|---|---|---|---|
| Age (yr) | 33.1 ± 11.1 (18.0–67.0) | 35.9 ± 11.4 (18.0–67.0) | 30.0 ± 9.90 (18.0–65.0) | <0.001 | 0.07 |
| Height (m) | 1.70 ± 0.10 (1.40–1.98) | 1.78 ± 0.10 (1.55–1.98) | 1.62 ± 0.10 (1.40–1.81) | <0.001 | 0.53 |
| Mass (kg) | 76.1 ± 16.4 (28.0–142) | 85.4 ± 13.1 (50.0–142) | 66.2 ± 13.4 (28.0–140) | <0.001 | 0.34 |
| BMI (kg/m2) | 26.1 ± 4.44 (11.7–49.1) | 27.0 ± 4.15 (16.4–49.1) | 25.1 ± 4.54 (11.7–44.7) | <0.001 | 0.04 |
| Variables | Categories | Male n (%) | Female n (%) | Total n | Chi2 (p) |
|---|---|---|---|---|---|
| Age (yr) | 18–35 | 308 (43) | 409 (57) | 717 | 55.7 <0.001 |
| 36–55 | 255 (65) | 138 (35) | 393 | ||
| >55 | 25 (74) | 9 (26) | 34 | ||
| BMI (kg/m2) | <18.5 | 5 (33) | 10 (67) | 15 | 43.6 <0.001 |
| 18.5–24.9 | 206 (41) | 297 (59) | 503 | ||
| 25–29.9 | 259 (60) | 175 (40) | 434 | ||
| 30 or greater | 118 (62) | 74 (38) | 192 | ||
| Athlete | Yes | 96 (28) | 250 (72) | 346 | 111.1 <0.001 |
| No | 492 (62) | 306 (38) | 798 | ||
| Smoker | Yes | 270 (100) | 0 (0) | 270 | 334.2 <0.001 |
| No | 318 (36) | 556 (64) | 874 | ||
| Health status | None of the above | 452 (52) | 426 (68) | 878 | 93.8 <0.001 |
| Anxiety or depression | 117 (74) | 41 (26) | 158 | ||
| Diabetes | 0 (0) | 19 (100) | 19 | ||
| Cardiovascular disease and pulmonary disease | 0 (0) | 32 (100) | 32 | ||
| Motor problem | 19 (33) | 38 (67) | 57 |
| Male (n = 588) | Female (n = 556) | Variance Analysis/Effects p (ηp2) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Before | During | d | Before | During | d | Gender | Time | Gender × Time | |
| Vigorous physical activities | |||||||||
| Days/week (d) | 2.09 ± 0.81 | 1.43 ± 0.56 | 0.96 | 2.44 ± 1.00 | 1.46 ± 0.82 | 1.08 | <0.001 (0.03) | <0.001 (0.35) | <0.001 (0.02) |
| Minutes/week (min) | 39.7 ± 11.3 | 28.0 ± 10.5 | 1.07 | 25.7 ± 12.1 | 19.7 ± 8.48 | 0.58 | <0.001 (0.34) | <0.001 (0.27) | <0.001 (0.04) |
| MET-minutes/week | 663 ± 320 | 323 ± 187 | 1.34 | 520 ± 372 | 238 ± 205 | 0.98 | <0.001 (0.07) | <0.001 (0.39) | 0.012 (0.01) |
| Moderate physical activities | |||||||||
| Days/week (d) | 2.42 ± 0.66 | 1.56 ± 0.54 | 0.99 | 2.16 ± 0.82 | 1.46 ± 0.63 | 0.97 | <0.001 (0.03) | <0.001 (0.41) | 0.003 (0.01) |
| Minutes/week (min) | 40.4 ± 11.2 | 24.2 ± 9.05 | 1.60 | 35.3 ± 14.3 | 21.0 ± 9.51 | 1.20 | <0.001 (0.06) | <0.001 (0.50) | 0.035 (0.00) |
| MET-minutes/week | 394 ± 166 | 152 ± 79.7 | 1.97 | 315 ± 188 | 130 ± 96.3 | 1.30 | <0.001 (0.06) | <0.001 (0.54) | <0.001 (0.02) |
| Walking | |||||||||
| Days/walk for at least 10 min (d) | 4.28 ± 1.47 | 2.74 ± 0.74 | 1.39 | 3.06 ± 1.09 | 2.07 ± 0.92 | 0.99 | <0.001 (0.24) | <0.001 (0.45) | <0.001 (0.04) |
| Minutes per/walking days (min) | 37.0 ± 12.5 | 23.0 ± 8.59 | 1.33 | 43.5 ± 17.2 | 20.6 ± 8.73 | 1.77 | <0.001 (0.01) | <0.001 (0.57) | <0.001 (0.07) |
| MET-minutes/week | 528 ± 271 | 215 ± 120 | 1.60 | 449 ± 261 | 141 ± 87.0 | 1.77 | <0.001 (0.06) | <0.001 (0.58) | 0.767 (0.00) |
| Sitting | |||||||||
| Hours per weekday (h) | 3.64 ± 1.42 | 6.51 ± 1.22 | 2.17 | 3.49 ± 1.53 | 6.12 ± 1.41 | 1.79 | <0.001 (0.02) | <0.001 (0.67) | 0.040 (0.00) |
| All Physical Activity | |||||||||
| Days/week (d) | 2.93 ± 0.57 | 1.91 ± 0.37 | 2.17 | 2.55 ± 0.61 | 1.67 ± 0.53 | 1.54 | <0.001 (0.13) | <0.001 (0.66) | 0.001 (0.01) |
| Minutes/week (min) | 117 ± 21.4 | 75.1 ± 16.9 | 2.19 | 105 ± 31.3 | 61.2 ± 16.0 | 1.85 | <0.001 (0.14) | <0.001 (0.67) | 0.468 (0.00) |
| MET-minutes/week | 1584 ± 447 | 689 ± 249 | 2.57 | 1283 ± 582 | 509 ± 271 | 1.82 | <0.001 (0.14) | <0.001 (0.69) | <0.001 (0.01) |
| Male (n = 588) | Female (n = 556) | Variance Analysis/Effects p (ηp2) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Before | During | d | Before | During | d | Sex | Time | Sex × Time | |
| In most ways my life is close to my ideal | |||||||||
| Score Q1 | 29.8 ± 5.06 | 12.6 ± 3.34 | 4.10 | 29.5 ± 4.85 | 12.4 ± 6.11 | 3.12 | 0.230 (0.00) | <0.001 (0.86) | 0.989 (0.00) |
| The conditions of my life are excellent. | |||||||||
| Score Q2 | 33.1 ± 2.63 | 12.2 ± 2.64 | 7.93 | 30.3 ± 4.15 | 13.2 ± 6.92 | 3.09 | <0.001 (0.02) | <0.001 (0.91) | <0.001 (0.09) |
| I am satisfied with my life | |||||||||
| Score Q3 | 28.8 ± 4.26 | 16.4 ± 5.25 | 2.61 | 27.5 ± 5.26 | 11.8 ± 6.67 | 2.63 | <0.001 (0.14) | <0.001 (0.76) | <0.001 (0.04) |
| So far I have gotten the important things I want in life. | |||||||||
| Score Q4 | 30.5 ± 4.02 | 13.0 ± 2.78 | 5.15 | 28.6 ± 2.86 | 15.2 ± 4.03 | 3.89 | 0.241 (0.00) | <0.001 (0.90) | <0.001 (0.14) |
| If I could live my life over, I would change almost nothing. | |||||||||
| Score Q5 | 31.8 ± 3.56 | 15.0 ± 4.52 | 4.94 | 31.1 ± 4.73 | 10.9 ± 5.54 | 3.93 | <0.001 (0.12) | <0.001 (0.89) | <0.001 (0.06) |
| Total score | |||||||||
| 30.8 ± 2.00 | 13.8 ± 1.77 | 9.02 | 29.4 ± 1.85 | 12.7 ± 2.54 | 7.61 | <0.001 (0.17) | <0.001 (0.97) | 0.117 (0.00) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hermassi, S.; Sellami, M.; Salman, A.; Al-Mohannadi, A.S.; Bouhafs, E.G.; Hayes, L.D.; Schwesig, R. Effects of COVID-19 Lockdown on Physical Activity, Sedentary Behavior, and Satisfaction with Life in Qatar: A Preliminary Study. Int. J. Environ. Res. Public Health 2021, 18, 3093. https://doi.org/10.3390/ijerph18063093
Hermassi S, Sellami M, Salman A, Al-Mohannadi AS, Bouhafs EG, Hayes LD, Schwesig R. Effects of COVID-19 Lockdown on Physical Activity, Sedentary Behavior, and Satisfaction with Life in Qatar: A Preliminary Study. International Journal of Environmental Research and Public Health. 2021; 18(6):3093. https://doi.org/10.3390/ijerph18063093
Chicago/Turabian StyleHermassi, Souhail, Maha Sellami, Ahmad Salman, Abdulla S. Al-Mohannadi, El Ghali Bouhafs, Lawrence D. Hayes, and René Schwesig. 2021. "Effects of COVID-19 Lockdown on Physical Activity, Sedentary Behavior, and Satisfaction with Life in Qatar: A Preliminary Study" International Journal of Environmental Research and Public Health 18, no. 6: 3093. https://doi.org/10.3390/ijerph18063093