
Socio-Demographic Factors Influencing the Use of Assistive Technology among Children with Disabilities in Malawi

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Surveys
3. Study Variables
3.1. Dependent Variable
3.1.1. Use of Assistive Technology
3.1.2. Use of an Assistive Product for Personal Mobility
3.2. Independent Variables
3.3. Analysis
4. Results
4.1. Demographic Characteristics of Children by Type of Disability
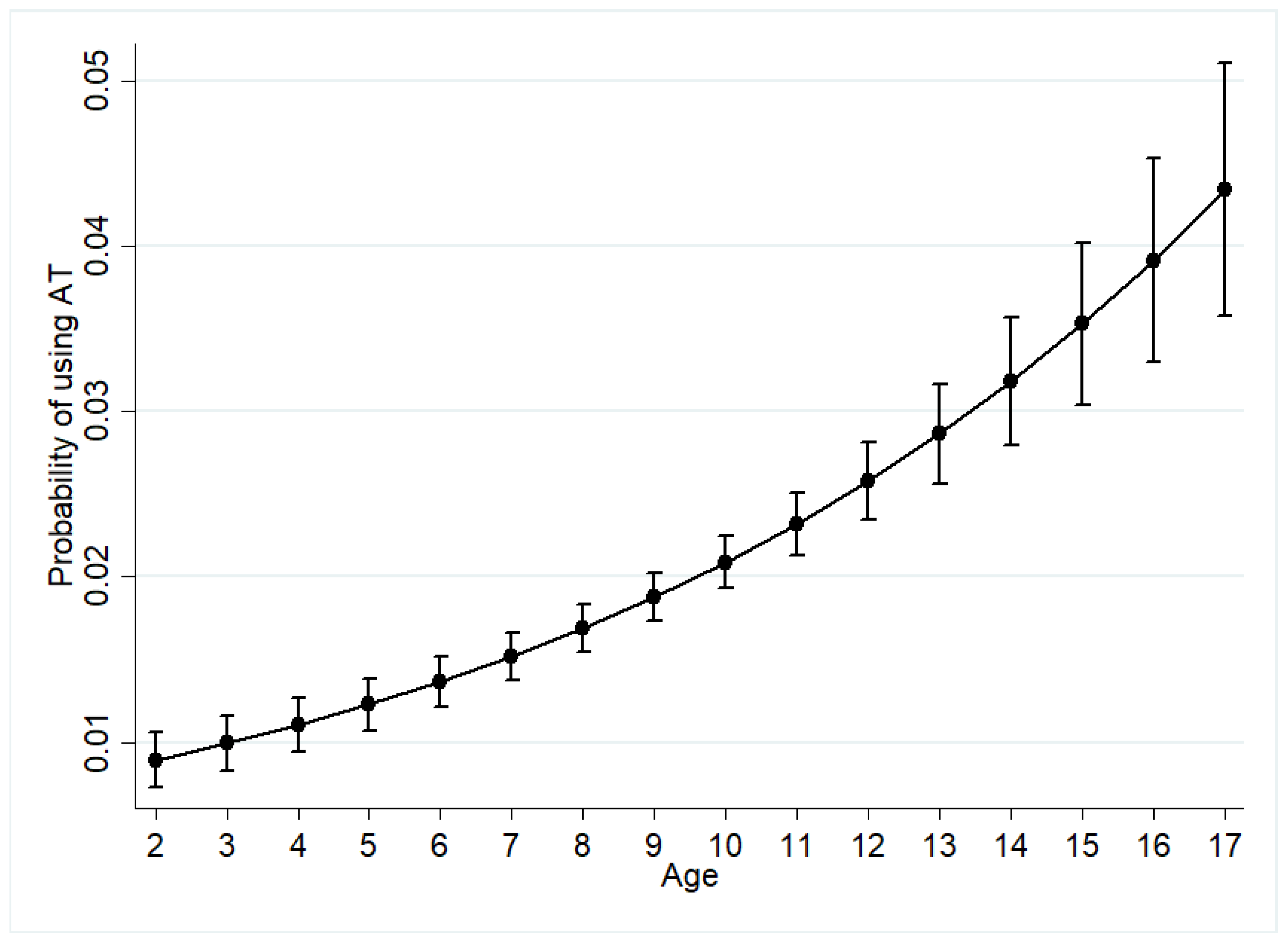
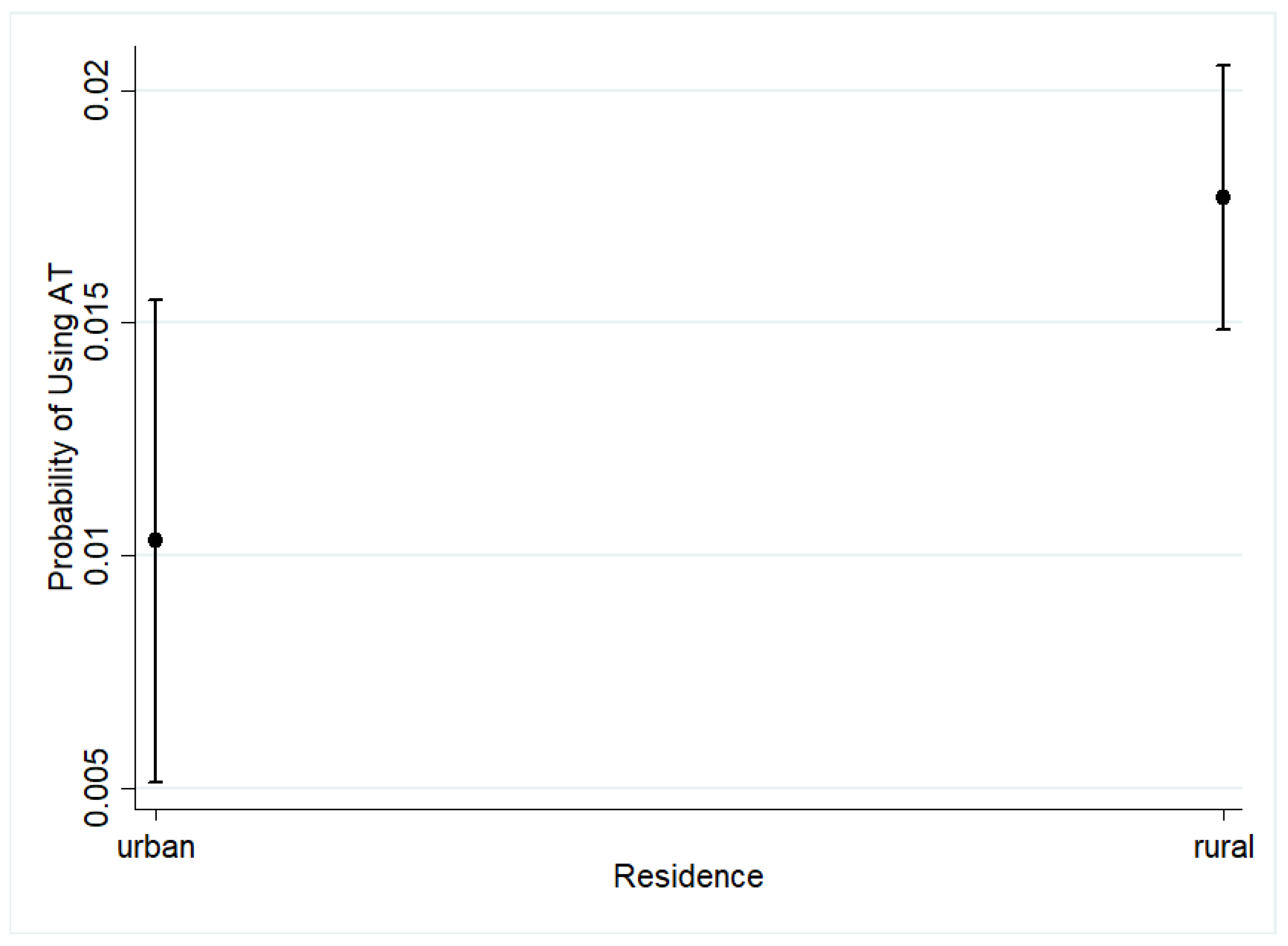
4.2. Logistic Regression Results
4.3. Use of AT for Personal Mobility as a Dependent Variable
4.4. Structure Equation Modeling Results
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eide, A.H.; Mannan, H.; Khogali, M.; Van Rooy, G.; Swartz, L.; Munthali, A.; Hem, K.-G.; MacLachlan, M.; Dyrstad, K. Perceived barriers for accessing health services among individuals with disability in four African countries. PLoS ONE 2015, 10, e0125915. [Google Scholar] [CrossRef]
- Parette, P.; Scherer, M. Assistive technology use and stigma. Educ. Train. Dev. Disabil. 2004, 1, 217–226. [Google Scholar]
- World Health Organization. Assistive Technology. Available online: https://www.who.int/news-room/fact-sheets/detail/assistive-technology (accessed on 25 August 2020).
- Khasnabis, C.; Mirza, Z.; MacLachlan, M. Opening the GATE to inclusion for people with disabilities. Lancet 2015, 10010, 2229–2230. [Google Scholar] [CrossRef]
- Tebbutt, E.; Brodmann, R.; Borg, J.; MacLachlan, M.; Khasnabis, C.; Horvath, R. Assistive products and the sustainable development goals (SDGs). Glob. Health 2016, 12, 79. [Google Scholar] [CrossRef] [Green Version]
- Mji, G.; Edusei, A. An introduction to a special issue on the role of assistive technology in social inclusion of persons with disabilities in Africa: Outcome of the fifth African Network for Evidence-to-Action in Disability conference. Afr. J. Disabil. 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Osam, J.A.; Opoku, M.P.; Dogbe, J.A.; Nketsia, W.; Hammond, C. The use of assistive technologies among children with disabilities: The perception of parents of children with disabilities in Ghana. Disabil. Rehabil. Assist. Technol. 2019, 8, 1–8. [Google Scholar] [CrossRef]
- Ndiku Makewa, L.; Mutie, J. Assistive Technology for Managing Learners with Special Needs in Makueni County, Kenya. JRIIE 2018, 2. [Google Scholar]
- Abiatal, L.K.; Howard, G.R. Constructivist Assistive Technology in a Mathematics Classroom for the Deaf: Going Digital at a Rural Namibian Primary School. In Proceedings of the South African Institute of Computer Scientists and Information Technologists, Skukuza, South Africa, 17–18 September 2019; pp. 1–9. [Google Scholar]
- Borg, J.B.-B.; Khasnabis, C.; Mitra, G.; Myhill, W.; Raja, D. Assistive Technology for Children with Disabilities: Creating Opportunities for Education, Inclusion and Participation—A Discussion Pape; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Matter, R.A.; Eide, A.H. Access to assistive technology in two Southern African countries. Bmc Health Serv. Res. 2018, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Mwaijande, V.T. Access to Education and Assistive Devices for Children with Physical Disabilities in Tanzania; Oslo and Akershus University College: Oslo, Norway, 2014. [Google Scholar]
- Adebisi, R.O.; Liman, N.A.; Longpoe, P.K. Using Assistive Technology in Teaching Children with Learning Disabilities in the 21st Century. J. Educ. Pract. 2015, 6, 14–20. [Google Scholar]
- Eide, A.H.; Munthali, A. Living conditions among persons with disabilities in Malawi. Natl. Represent. Surv. 2017. [Google Scholar] [CrossRef]
- Loeb, M.; Eide, A.H. Living Conditions among People with Activity Limitations in Malawi. A National Representative Study; SINTEF Rapport; SINTEF: Trondheim, Norway, 2004. [Google Scholar]
- Visagie, S.; Eide, A.H.; Mannan, H.; Schneider, M.; Swartz, L.; Mji, G.; Munthali, A.; Khogali, M.; van Rooy, G.; Hem, K.-G. A description of assistive technology sources, services and outcomes of use in a number of African settings. Disabil. Rehabil. Assist. Technol. 2017, 12, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.M.; Ebuenyi, I.D.; Kafumba, J.; Jamali-Phiri, M.; MacLachlan, M.; Munthali, A. An overview of assistive technology products and services provided in Malawi. Disabil. Rehabil. Assist. Technol. 2020, 24, 1–5. [Google Scholar]
- Ebuenyi, I.D.; Smith, E.M.; Kafumba, J.; Jamili, M.Z.; Munthali, A.; MacLachlan, M. Implementation of the Assistive Product List (APL) in Malawi through development of appropriate policy and systems: An Action Research Protocol. BMJ Open 2020, 10, e040281. [Google Scholar] [CrossRef] [PubMed]
- Jamali-Phiri, M.; Kafumba, J.A.; MacLachlan, M.; Smith, E.M.; Ebuenyi, I.D.; Eide, A.H.; Munthali, A. Addressing data deficiencies in assistive technology by using statistical matching methodology: A case study from Malawi. Disabil. Rehabil. Assist. Technol. 2020, 9, 1–15. [Google Scholar] [CrossRef]
- NSONM, I. Malawi Demographic and Health Survey 2015–2016; National Statistical Office: Rockville, MD, USA, 2017. [Google Scholar]
- D’Orazio, M. Statistical Matching and Imputation of Survey Data with the Package StatMatch for the R Environment. R Package Vignette. 2011. Available online: Http://www.Cros-Portal.Eu/Sites/Default/Files//Stat._Matching__Statmatch.Pdf (accessed on 25 August 2020).
- Moriarity, C.; Scheuren, F. Statistical matching: A paradigm for assessing the uncertainty in the procedure. J. Off. Stat. 2001, 17, 407. [Google Scholar]
- Donatiello, G.; D‘Orazio, M.; Frattarola, D.; Rizzi, A.; Scanu, M.; Spaziani, M. Statistical matching of income and consumption expenditures. Int. J. Econ. Sci. 2014, 3, 50. [Google Scholar]
- D’Orazio, M. Statistical Matching and Imputation of Survey Data with StatMatch; Italian National Institute of Statistics: Rome, Italy, 2016. [Google Scholar]
- D’Orazio, M.; Di Zio, M.; Scanu, M. Old and new approaches in statistical matching when samples are drawn with complex survey designs. In Proceedings of the 45th Riunione Scientifica della Societa’Italiana di Statistica, Padova, Italy, 15–18 June 2010; pp. 16–18. [Google Scholar]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression; Wiley: New York, NY, USA, 2000. [Google Scholar]
- Mitchell, M.N. Interpreting and Visualizing Regression Models Using Stata; Stata Press: College Station, TX, USA, 2012; Volume 5. [Google Scholar]
- Kaye, H.S.; Yeager, P.; Reed, M. Disparities in usage of assistive technology among people with disabilities. Assist. Technol. 2008, 20, 194–203. [Google Scholar] [CrossRef]
- Zimmer, Z.; Chappell, N.L. Mobility restriction and the use of devices among seniors. J. Aging Health 1994, 6, 185–208. [Google Scholar] [CrossRef]
- Yeung, K.-T.; Lin, C.-H.; Teng, Y.-L.; Chen, F.-F.; Lou, S.-Z.; Chen, C.-L. Use of and self-perceived need for assistive devices in individuals with disabilities in Taiwan. PLoS ONE 2016, 11, e0152707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matter, R.; Harniss, M.; Oderud, T.; Borg, J.; Eide, A.H. Assistive technology in resource-limited environments: A scoping review. Disabil. Rehabil. Assist. Technol. 2017, 12, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Lersilp, S.; Putthinoi, S.; Lersilp, T. Facilitators and barriers of assistive technology and learning environment for children with special needs. Occup. Ther. Int. 2018, 2018, 3705946. [Google Scholar] [CrossRef] [PubMed]
- Copley, J.; Ziviani, J. Barriers to the use of assistive technology for children with multiple disabilities. Occup. Ther. Int. 2004, 11, 229–243. [Google Scholar] [CrossRef] [PubMed]
- MacLachlan, M.; Scherer, M.J. Systems thinking for assistive technology: A commentary on the GREAT summit. Disabil. Rehabil. Assist. Technol. 2018, 13, 492–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacLachlan, M.; Banes, D.; Bell, D.; Borg, J.; Donnelly, B.; Fembek, M.; Ghosh, R.; Gowran, R.J.; Hannay, E.; Hiscock, D. Assistive technology policy: A position paper from the first global research, innovation, and education on assistive technology (GREAT) summit. Disabil. Rehabil. Assist. Technol. 2018, 13, 454–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Dependent Variable | Data Source |
|---|---|
| Ever used an assistive technology | 2017 LCS |
| Use of mobility devices (wheelchairs, crutches, walking sticks, white cane, standing frame) (Note on mobility products or devices, the 2017 LCS did not differentiate the products by low cost, improvised aids, and manufactured aids.) | 2017 LCS |
| Independent Variable | |
| Disability or functional limitation | 2015-16 MDHS |
| Age | 2015-16 MDHS |
| Sex | 2015-16 MDHS |
| Place of residence | 2015-16 MDHS |
| Region | 2015-16 MDHS |
| Level of education | 2015-16 MDHS |
| Household income (wealth status) | 2015-16MDHS |
| Sex of the household head | 2015-16 MDHS |
| Background Characteristics 1 | Delay in Sitting Standing or Walking | Seeing Difficulty | Hearing Difficulty | Walking Difficulty | Has Fits or Lose Consciousness | Learning Difficulty | Speech Different from Normal | Mentally Backward or Slow 2 | Number |
|---|---|---|---|---|---|---|---|---|---|
| Age group | |||||||||
| 2–4 | 4.2 | 2.0 | 2.9 | 2.0 | 4.0 | 4.7 | 6.2 | 5.7 | 10,974 |
| 5–9 | 4.2 | 2.8 | 6.4 | 2.6 | 3.6 | 4.7 | 4.7 | 7.7 | 19,904 |
| Sex | |||||||||
| Male | 4.5 | 2.5 | 5.2 | 2.5 | 3.8 | 4.9 | 5.6 | 7.4 | 15,280 |
| Female | 4.0 | 2.5 | 5.1 | 2.3 | 3.6 | 4.5 | 4.6 | 6.5 | 15,598 |
| Place of residence | |||||||||
| Urban | 3.2 | 2.9 | 3.6 | 1.8 | 2.1 | 4.3 | 4.6 | 5.3 | 4722 |
| Rural | 4.4 | 2.5 | 5.4 | 2.5 | 4.0 | 4.8 | 5.2 | 7.2 | 26,156 |
| Region | |||||||||
| Northern | 3.3 | 2.3 | 4.0 | 1.8 | 3.0 | 3.5 | 4.5 | 3.6 | 6133 |
| Central | 4.4 | 2.8 | 5.3 | 2.2 | 5.1 | 4.8 | 4.4 | 7.3 | 10,134 |
| Southern | 4.5 | 2.4 | 5.6 | 2.7 | 3.1 | 5.1 | 5.9 | 8.1 | 14,611 |
| Level of Education | |||||||||
| No education | 4.5 | 2.2 | 3.7 | 2.4 | 4.2 | 5.0 | 6.4 | 6.2 | 14,679 |
| Primary | 4.1 | 2.8 | 6.5 | 2.4 | 3.2 | 4.4 | 4.3 | 7.6 | 16,188 |
| Total | 4.2 | 2.5 | 5.2 | 2.4 | 3.7 | 4.7 | 5.1 | 6.9 | 30,878 |
| Background Characteristics | Seeing Difficulty | Hearing Difficulty | Communication Difficulty | Difficulty Remembering/ Concentrating | Walking Difficulty | Washing/Dressing Difficulty | Number of Children |
|---|---|---|---|---|---|---|---|
| Age group | |||||||
| 10–14 | 2.2 | 4.6 | 2.0 | 5.1 | 1.2 | 1.8 | 19,116 |
| 15–17 | 2.8 | 4.6 | 2.1 | 6.3 | 1.3 | 1.2 | 7610 |
| Total | 2.4 | 4.6 | 2.1 | 5.4 | 1.2 | 1.7 | 26,726 |
| Sex | |||||||
| Male | 2.1 | 4.4 | 2.3 | 5.4 | 1.2 | 1.9 | 13,712 |
| Female | 2.6 | 4.7 | 1.8 | 5.5 | 1.3 | 1.4 | 13,014 |
| Total | 2.4 | 4.6 | 2.1 | 5.4 | 1.2 | 1.7 | 26,726 |
| Place of residence | |||||||
| Urban | 3.3 | 3.9 | 1.7 | 5.1 | 1.0 | 1.1 | 423 |
| Rural | 2.2 | 4.7 | 2.1 | 5.5 | 1.3 | 1.8 | 22,303 |
| Total | 2.4 | 4.6 | 2.1 | 5.4 | 1.2 | 1.7 | 26,726 |
| Region | |||||||
| Northern | 2.2 | 4.0 | 1.5 | 3.1 | 1.3 | 1.6 | 5371 |
| Central | 2.4 | 4.4 | 2.0 | 6.2 | 1.3 | 1.4 | 8670 |
| Southern | 2.4 | 5.0 | 2.4 | 5.9 | 1.2 | 1.8 | 12,685 |
| Total | 2.4 | 4.6 | 2.1 | 5.4 | 1.2 | 1.7 | 26,726 |
| Level of Education | |||||||
| No education, Preschool | 2.2 | 4.4 | 12.5 | 13.1 | 8.5 | 13.5 | 458 |
| Primary | 2.2 | 4.7 | 1.9 | 5.4 | 1.1 | 1.5 | 24,312 |
| Secondary/higher | 4.2 | 3.4 | 1.2 | 4.8 | 0.8 | 0.4 | 1956 |
| Total | 2.4 | 4.6 | 2.1 | 5.4 | 1.2 | 1.7 | 26,726 |
| Wealth status | |||||||
| poorest | 2.0 | 4.8 | 2.6 | 5.4 | 1.5 | 1.8 | 4582 |
| poorer | 2.1 | 5.3 | 2.6 | 5.8 | 1.5 | 2.3 | 4699 |
| middle | 2.2 | 4.5 | 1.7 | 6.0 | 1.3 | 1.7 | 5369 |
| richer | 2.5 | 4.5 | 2.1 | 5.4 | 1.2 | 1.6 | 5993 |
| richest | 2.9 | 4.0 | 1.6 | 4.7 | 0.9 | 1.0 | 6083 |
| Total | 2.4 | 4.6 | 2.1 | 5.4 | 1.2 | 1.7 | 26,726 |
| Sex of household head | |||||||
| Male | 2.3 | 4.5 | 1.9 | 5.4 | 1.1 | 1.5 | 18,080 |
| Female | 2.6 | 4.8 | 2.5 | 5.6 | 1.5 | 2.0 | 8646 |
| Total | 2.4 | 4.6 | 2.1 | 5.4 | 1.2 | 1.7 | 26,726 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jamali-Phiri, M.; Ebuenyi, I.D.; Smith, E.M.; Kafumba, J.A.; MacLachlan, M.; Munthali, A. Socio-Demographic Factors Influencing the Use of Assistive Technology among Children with Disabilities in Malawi. Int. J. Environ. Res. Public Health 2021, 18, 3062. https://doi.org/10.3390/ijerph18063062
Jamali-Phiri M, Ebuenyi ID, Smith EM, Kafumba JA, MacLachlan M, Munthali A. Socio-Demographic Factors Influencing the Use of Assistive Technology among Children with Disabilities in Malawi. International Journal of Environmental Research and Public Health. 2021; 18(6):3062. https://doi.org/10.3390/ijerph18063062
Chicago/Turabian StyleJamali-Phiri, Monica, Ikenna D. Ebuenyi, Emma M. Smith, Juba Alyce Kafumba, Malcolm MacLachlan, and Alister Munthali. 2021. "Socio-Demographic Factors Influencing the Use of Assistive Technology among Children with Disabilities in Malawi" International Journal of Environmental Research and Public Health 18, no. 6: 3062. https://doi.org/10.3390/ijerph18063062