
Comparison of Interface Pressures and Subjective Comfort of Pressure-Relieving Overlays on the Operating Table for Healthy Volunteers


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample and Setting
2.3. Measures
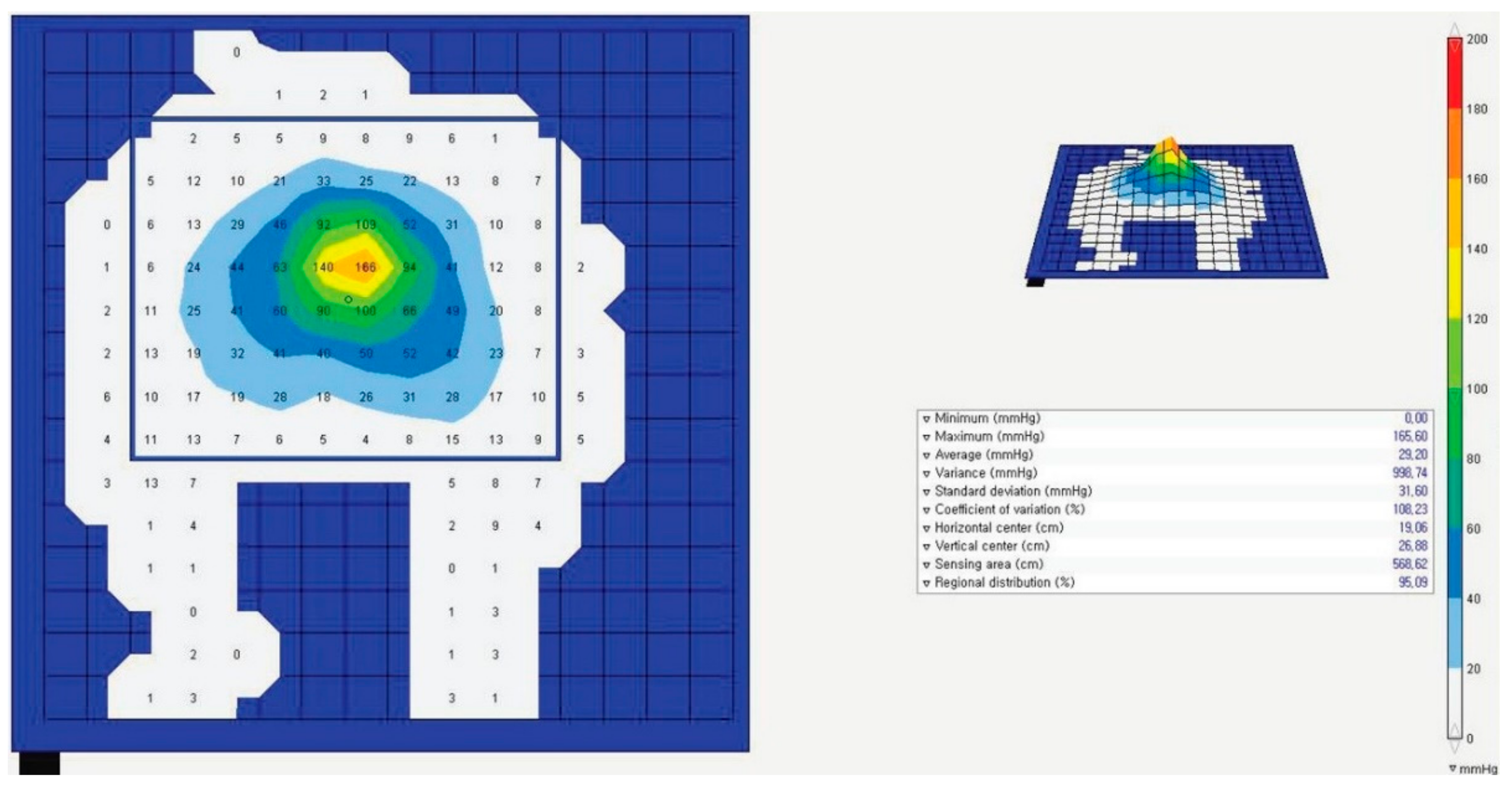
2.3.1. Interface Pressure
2.3.2. Subjective Comfort
2.4. Data Collection and Analysis
2.5. Ethical Approval
3. Results
3.1. General Characteristics of Participants
3.2. Comparison of the Average Interface Pressure on the Sacrum and Both Heels
3.3. Comparison of Subjective Comfort
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- European Pressure Ulcer Advisory Panel; National Pressure Injury Advisory Panel; Pan Pacific Pressure Injury Alliance. Prevention and treatment of pressure ulcers/injuries: Clinical practice guideline. In The International Guideline; Haesler, E., Ed.; EPUAP/NPIAP/PPPIA: Prague, Czech Republic, 2019. [Google Scholar]
- Lyder, C.H.; Wang, Y.; Metersky, M.; Curry, M.; Kliman, R.; Verzier, N.R.; Hunt, D.R. Hospital-Acquired Pressure Ulcers: Results from the National Medicare Patient Safety Monitoring System Study. J. Am. Geriatr. Soc. 2012, 60, 1603–1608. [Google Scholar] [CrossRef]
- Chaboyer, W.; Bucknall, T.; Webster, J.; McInnes, E.; Gillespie, B.M.; Banks, M.; Whitty, J.A.; Thalib, L.; Roberts, S.; Tallott, M.; et al. The effect of a patient centred care bundle intervention on pressure ulcer incidence (INTACT): A cluster randomised trial. Int. J. Nurs. Stud. 2016, 64, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Spruce, L. Back to Basics: Preventing Perioperative Pressure Injuries. AORN J. 2017, 105, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-L.; Chen, X.-Y.; Wu, J. The incidence of pressure ulcers in surgical patients of the last 5 years: A systematic review. Wounds 2012, 24, 234–241. [Google Scholar]
- Meehan, A.J.; Beinlich, N.R.; Hammonds, T.L. A Nurse-Initiated Perioperative Pressure Injury Risk Assessment and Prevention Protocol. AORN J. 2016, 104, 554–565. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.-L.; Lee, W.-R.; Yeh, C.-C.; Shih, C.-C.; Chen, T.-L.; Liao, C.-C. Adverse Outcomes after Major Surgery in Patients with Pressure Ulcer: A Nationwide Population-Based Retrospective Cohort Study. PLoS ONE 2015, 10, e0127731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oomens, C.W.J.; Bader, D.L.; Loerakker, S.; Baaijens, F. Pressure Induced Deep Tissue Injury Explained. Ann. Biomed. Eng. 2014, 43, 297–305. [Google Scholar] [CrossRef]
- Yoshimura, M.; Ohura, N.; Santamaria, N.; Watanabe, Y.; Akizuki, T.; Gefen, A. High body mass index is a strong predictor of intraoperative acquired pressure injury in spinal surgery patients when prophylactic film dressings are applied: A retrospective analysis prior to the BOSS Trial. Int. Wound J. 2020, 17, 660–669. [Google Scholar] [CrossRef]
- Joseph, J.; McLaughlin, D.; Darian, V.; Hayes, L.; Siddiqui, A. Alternating Pressure Overlay for Prevention of Intraoperative Pressure Injury. J. Wound Ostomy Cont. Nurs. 2019, 46, 13–17. [Google Scholar] [CrossRef]
- Neo, T.G.; Koo, S.H.; Chew, S.T.H.; Png, G.K.; Lacuesta, M.J.; Wu, M.Y.L.; Tay, R.Y.C.; Singh, P.A.; Chandran, R. A randomized controlled trial to compare the interface pressures of alternating pressure overlay with gel pad versus gel pad alone during prolonged surgery. J. Tissue Viability 2021, 6. [Google Scholar] [CrossRef]
- Pham, B.; Teague, L.; Mahoney, J.; Goodman, L.; Paulden, M.; Poss, J.; Li, J.; Sikich, N.J.; Lourenco, R.; Ieraci, L.; et al. Support surfaces for intraoperative prevention of pressure ulcers in patients undergoing surgery: A cost-effectiveness analysis. Surgery 2011, 150, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.J. Strategies for improving the review and assessment of national health insurance reimbursement claims. Health Welfare Policy Forum 2019, 272, 26–38. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Saghaleini, S.H.; Dehghan, K.; Shadvar, K.; Sanaie, S.; Mahmoodpoor, A.; Ostadi, Z. Pressure ulcer and nutrition. Indian J. Crit. Care Med. 2018, 22, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.Y.; Chen, H.L.; Xu, X.J. Pressure-redistribution surfaces for prevention of surgery-related pressure ulcers: A me-ta-analysis. Ostomy Wound Manag. 2013, 59, 36–48. [Google Scholar]
- Mervis, J.S.; Phillips, T.J. Pressure ulcers: Pathophysiology, epidemiology, risk factors, and presentation. J. Am. Acad. Dermatol. 2019, 81, 881–890. [Google Scholar] [CrossRef]
- Reddy, M.; Gill, S.S.; Rochon, P.A. Preventing Pressure Ulcers: A Systematic Review. JAMA 2006, 296, 974–984. [Google Scholar] [CrossRef]
- Keller, B.; Overbeeke, J.; Van Der Werken, C. Interface pressure measurement during surgery: A comparison of four operating table surfaces. J. Wound Care 2006, 15, 5–9. [Google Scholar] [CrossRef]
- Bulfone, G.; Marzoli, I.; Quattrin, R.; Fabbro, C.; Palese, A. A Longitudinal Study of the Incidence of Pressure Sores and the Associated Risks and Strategies Adopted in Italian Operating Theatres. J. Perioper. Pract. 2012, 22, 50–56. [Google Scholar] [CrossRef]
- Walton-Geer, P.S. Prevention of Pressure Ulcers in the Surgical Patient. AORN J. 2009, 89, 538–552. [Google Scholar] [CrossRef]
- Thorne, S.; Sauvé, K.; Yacoub, C.; Guitard, P. Evaluating the pressure-reducing capabilities of the gel pad in supine. Am. J. Occup. Ther. 2009, 63, 744–750. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.O.; Shin, Y.S. A survey of nursing practice guidelines for prevention of pressure injury in the operating room. J. Korea Acad.-Ind. Coop. Soc. 2018, 19, 635–644, In Korean. [Google Scholar] [CrossRef]
- Duetzmann, S.; Forsey, L.M.; Senft, C.; Seifert, V.; Ratliff, J.; Park, J. Sacral Peak Pressure in Healthy Volunteers and Patients with Spinal Cord Injury. Nurs. Res. 2015, 64, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Romanelli, M.; Clark, M.; Gefen, A.; Ciprandi, G. Science and Practice of Pressure Ulcer Management, 2nd ed.; Springer: London, UK, 2018; pp. 1–249. [Google Scholar]
- Park, K.H.; Park, J. The Efficacy of a Viscoelastic Foam Overlay on Prevention of Pressure Injury in Acutely Ill Patients. J. Wound Ostomy Cont. Nurs. 2017, 44, 440–444. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Category | n (%) or Mean ± SD |
|---|---|---|
| Gender | Male | 2 (6.5) |
| Female | 29 (93.5) | |
| Age (years) | 38.42 ± 9.64 | |
| Height (cm) | 161.06 ± 5.92 | |
| Weight (kg) | 57.32 ± 11.58 | |
| Body mass index | 22.01 ± 3.85 | |
| Underweight | 4 (12.9) | |
| Normal | 20 (64.5) | |
| Overweight | 3 (9.7) |
| Variables | Standard Mattress (n = 30) | PU 1 Foam (n = 30) | Gel Pad (n = 30) | EC 2 Foam (n = 30) | F | p | Post-Hoc |
|---|---|---|---|---|---|---|---|
| Mean ± SD | |||||||
| Sacrum | 56.10 ± 23.03 a | 31.55 ± 13.60 b | 57.42 ± 35.61 c | 47.03 ± 32.29 | 5.82 | 0.001 | a,c > b |
| Both heels | 84.68 ± 36.47 a | 41.39 ± 13.29 b | 63.58 ± 32.31 c | 48.10 ± 27.01 d | 13.97 | <0.001 | a > b,c,d; c > b |
| Variable | Standard Mattress (n = 30) | PU 1 Foam (n = 30) | Gel Pad (n = 30) | EC 2 Foam (n = 30) | F | p | Post-Hoc |
|---|---|---|---|---|---|---|---|
| Mean ± SD | |||||||
| Subjective comfort ratings | 5.38 ± 1.76 a | 7.00 ± 2.09 b | 5.91 ± 1.74 c | 6.57 ± 2.01 d | 13.46 | <0.001 | a < b,d; d > c |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, M.J.; Ko, S. Comparison of Interface Pressures and Subjective Comfort of Pressure-Relieving Overlays on the Operating Table for Healthy Volunteers. Int. J. Environ. Res. Public Health 2021, 18, 2640. https://doi.org/10.3390/ijerph18052640
Han MJ, Ko S. Comparison of Interface Pressures and Subjective Comfort of Pressure-Relieving Overlays on the Operating Table for Healthy Volunteers. International Journal of Environmental Research and Public Health. 2021; 18(5):2640. https://doi.org/10.3390/ijerph18052640
Chicago/Turabian StyleHan, Min Jung, and Sangjin Ko. 2021. "Comparison of Interface Pressures and Subjective Comfort of Pressure-Relieving Overlays on the Operating Table for Healthy Volunteers" International Journal of Environmental Research and Public Health 18, no. 5: 2640. https://doi.org/10.3390/ijerph18052640