
IDTWO: A Protocol for a Randomised Controlled Trial of a Web-Based Mental Health Intervention for Australians with Intellectual Disability

 , ,
, , 
Abstract
:1. Introduction
2. Objectives and Hypotheses
3. Trial Design
4. Methods
4.1. Participants, Interventions, and Outcomes
4.1.1. Study Setting
4.1.2. Eligibility Criteria
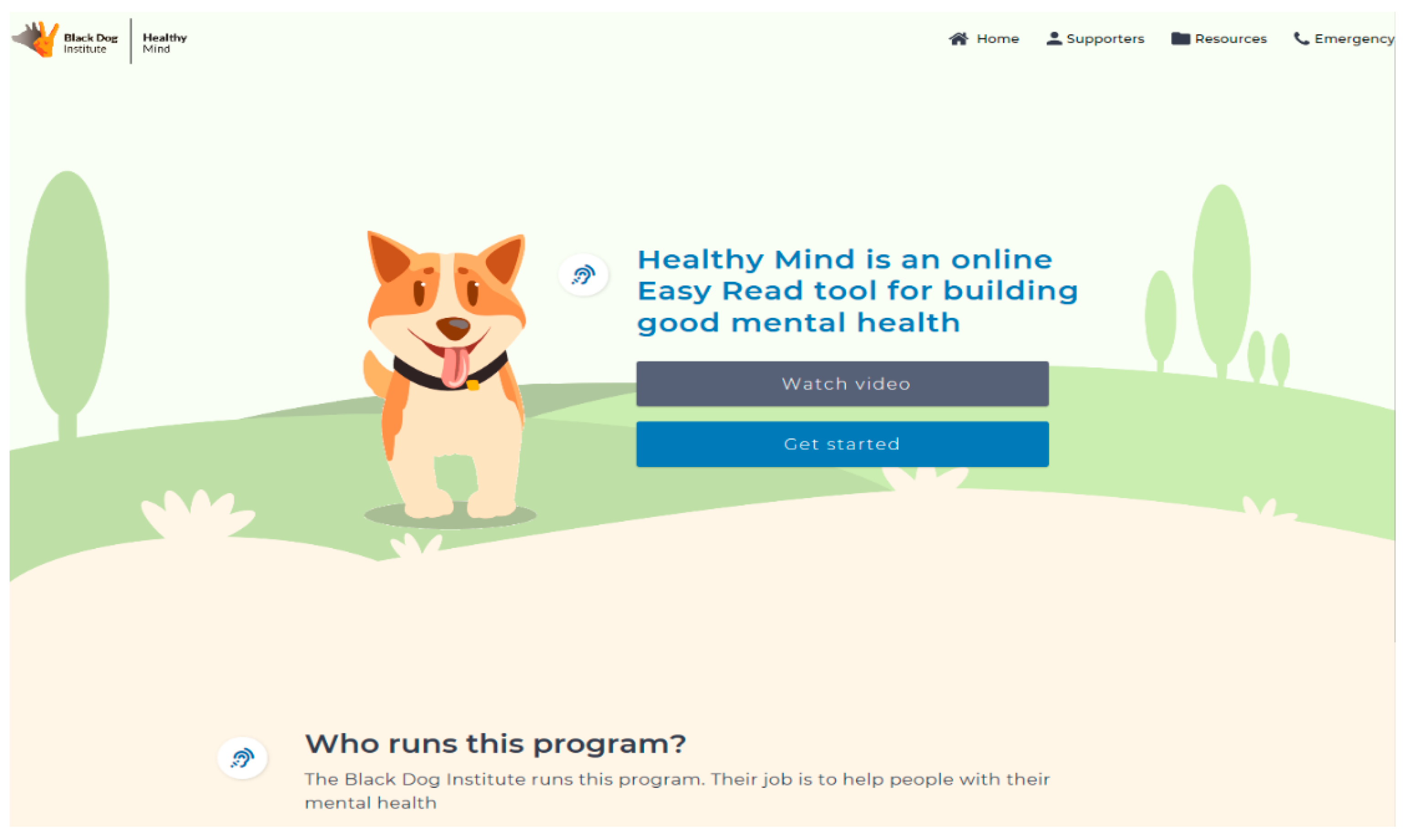
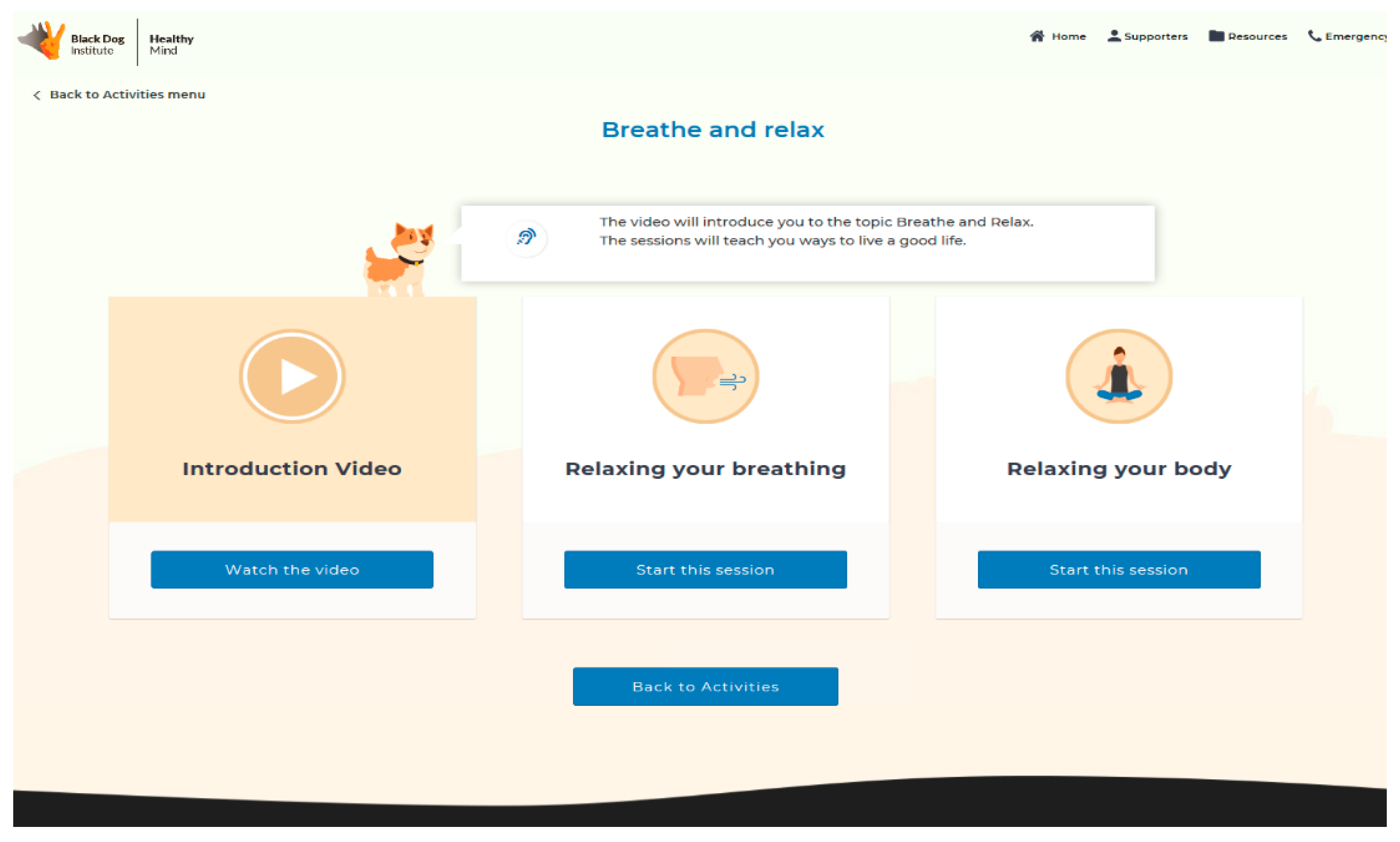
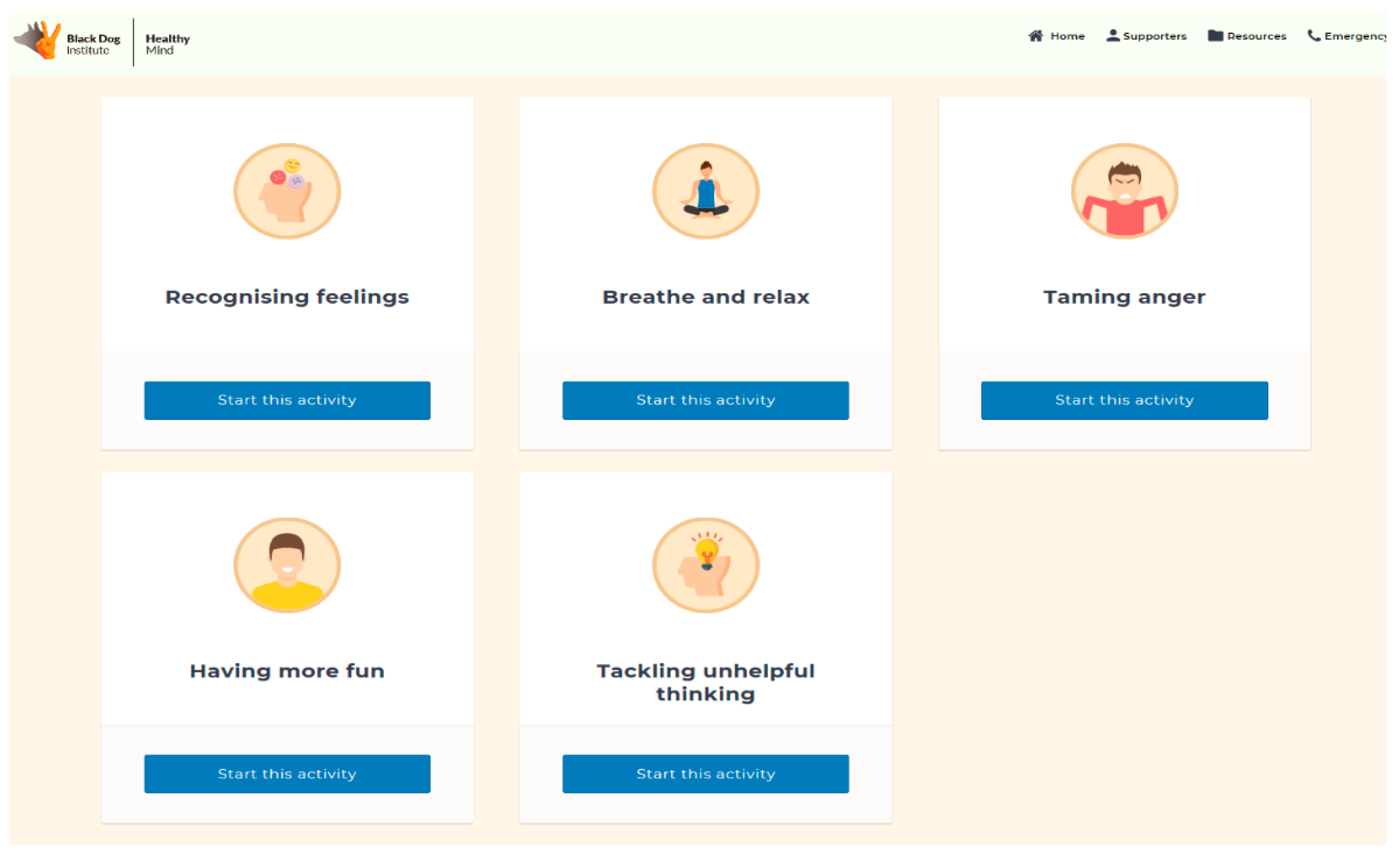
4.1.3. Interventions
4.1.4. Outcomes
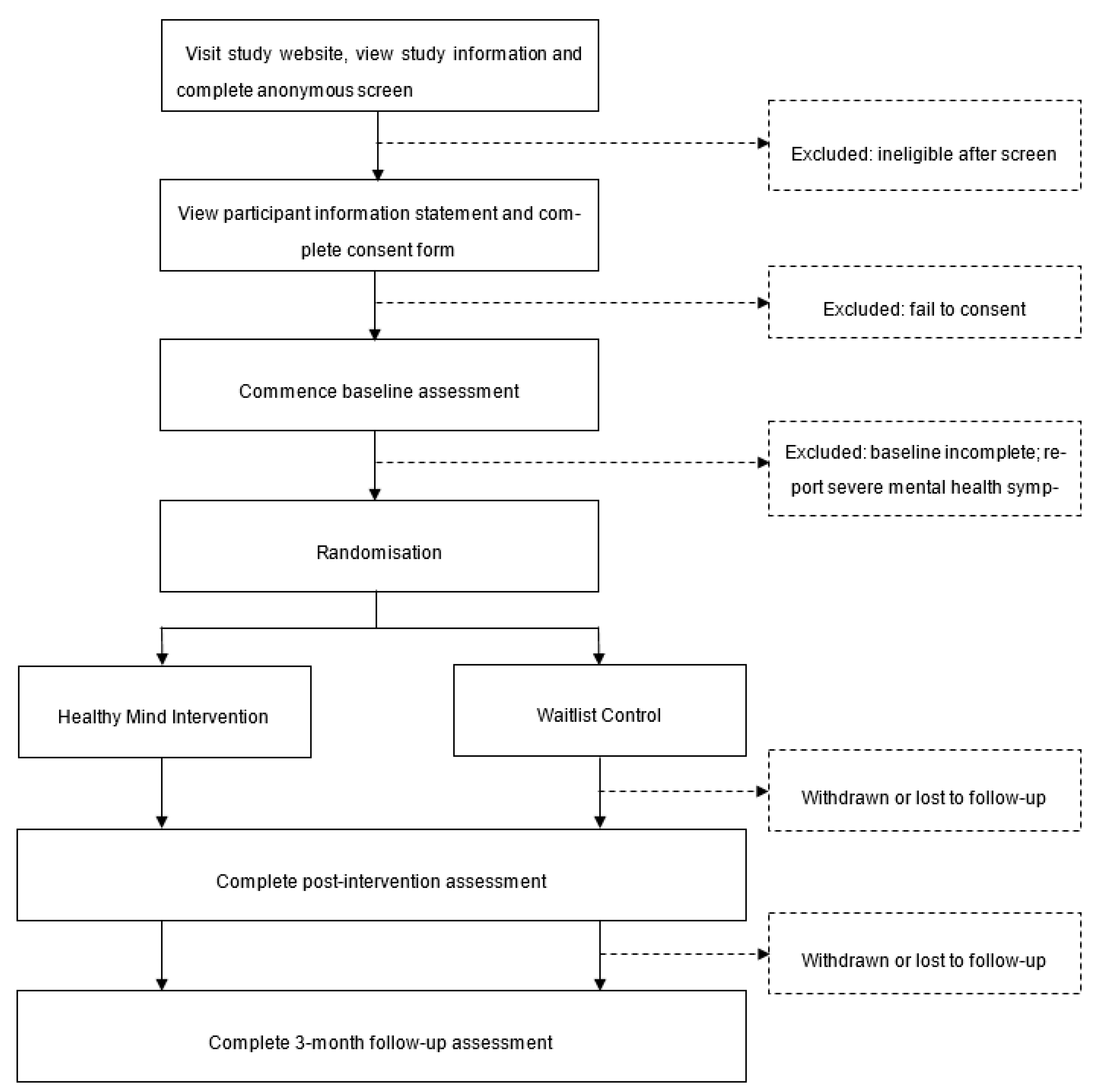
5. Participant Timeline
6. Sample Size
7. Recruitment
8. Assignment of Interventions
8.1. Allocation
8.2. Blinding
9. Data Collection, Management, and Analysis
9.1. Data Collection
9.2. Retention
9.3. Statistical Analysis
9.4. Monitoring
10. Ethics and Dissemination
10.1. Research Ethics Approval
10.2. Consent or Assent
10.3. Confidentiality
10.4. Ancillary and Post-Trial Care
11. Discussion
12. Limitations
13. Conclusions
- Trial registration: ACTRN126200001139
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Department of Developmental Disability Neuropsychiatry. Recommendations from the National Roundtable on the Mental Health of People with Intellectual Disability. Available online: https://www.3dn.unsw.edu.au/sites/default/files/documents/Communique_Full.pdf (accessed on 15 June 2019).
- Emerson, E.; Hatton, C. Mental health of children and adolescents with intellectual disabilities in Britain. Br. J. Psychiatry 2007, 191, 493–499. [Google Scholar] [CrossRef] [PubMed]
- White, P.; Chant, D.; Edwards, N.; Townsend, C.; Waghorn, G. Prevalence of Intellectual Disability and Comorbid Mental Illness in an Australian Community Sample. Aust. N. Z. J. Psychiatry 2005, 39, 395–400. [Google Scholar] [CrossRef]
- Evans, E.; Howlett, S.; Kremser, T.; Simpson, J.; Kayess, R.; Trollor, J. Service development for intellectual disability mental health: A human rights approach. J. Intellect. Disabil. Res. 2012, 56, 1098–1109. [Google Scholar] [CrossRef]
- Weiss, J.A.; Lunsky, Y.; Gracey, C.; Canrinus, M.; Morris, S. Emergency Psychiatric Services for Individuals with Intellectual Disabilities: Caregivers’ Perspectives. J. Appl. Res. Intellect. Disabil. 2009, 22, 354–362. [Google Scholar] [CrossRef]
- Donner, B.; Mutter, R.; Scior, K. Mainstream In-Patient Mental Health Care for People with Intellectual Disabilities: Service User, Carer and Provider Experiences. J. Appl. Res. Intellect. Disabil. 2010, 23, 214–225. [Google Scholar] [CrossRef]
- Chaplin, R. Mental health services for people with intellectual disabilities. Curr. Opin. Psychiatry 2011, 24, 372–376. [Google Scholar] [CrossRef] [PubMed]
- Whittle, E.L.; Fisher, K.R.; Reppermund, S.; Lenroot, R.; Trollor, J. Barriers and Enablers to Accessing Mental Health Services for People With Intellectual Disability: A Scoping Review. J. Ment. Health Res. Intellect. Disabil. 2018, 11, 69–102. [Google Scholar] [CrossRef]
- Willner, P. Readiness for Cognitive Therapy in People with Intellectual Disabilities. J. Appl. Res. Intellect. Disabil. 2006, 19, 5–16. [Google Scholar] [CrossRef]
- Willner, P.; Hatton, C. CBT for People with Intellectual Disabilities. J. Appl. Res. Intellect. Disabil. 2006, 19, 1–3. [Google Scholar] [CrossRef]
- Mesa, S.; Tsakanikos, E. Attitudes and self-efficacy towards adults with mild intellectual disability among staff in acute psychiatric wards: An empirical investigation. Adv. Ment. Health Intellect. Disabil. 2014, 8, 79–90. [Google Scholar] [CrossRef]
- Weise, J.; Fisher, K.R.; Whittle, E.; Trollor, J.N. What Can the Experiences of People With an Intellectual Disability Tell Us About the Desirable Attributes of a Mental Health Professional? J. Ment. Health Res. Intellect. Disabil. 2018, 11, 183–202. [Google Scholar] [CrossRef]
- Vereenooghe, L.; Gega, L.; Langdon, P.E. Intellectual disability and computers in therapy: Views of service users and clinical psychologists. Cyberpsychol. J. Psychosoc. Res. Cyberspace 2017, 11, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Dew, A.; Dowse, L.; Athanassiou, U.; Trollor, J. Current Representation of People with Intellectual Disability in Australian Mental Health Policy: The Need for Inclusive Policy Development. J. Policy Pract. Intellect. Disabil. 2018, 15, 136–144. [Google Scholar] [CrossRef]
- Mason, J.; Crowson, K.; Katsikitis, M.; Moodie, M. Australia’s National Disability Insurance Scheme: A collaboration opportunity for academia and industry. Tizard Learn. Disabil. Rev. 2018, 23, 139–146. [Google Scholar] [CrossRef]
- Einfeld, S.L.; Piccinin, A.M.; MacKinnon, A.; Hofer, S.M.; Taffe, J.; Gray, K.M.; Bontempo, D.E.; Hoffman, L.R.; Parmenter, T.; Tonge, B.J. Psychopathology in Young People With Intellectual Disability. JAMA 2006, 296, 1981–1989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinberg, L. Cognitive and affective development in adolescence. Trends Cogn. Sci. 2005, 9, 69–74. [Google Scholar] [CrossRef]
- Kilford, E.J.; Garrett, E.; Blakemore, S.-J. The development of social cognition in adolescence: An integrated perspective. Neurosci. Biobehav. Rev. 2016, 70, 106–120. [Google Scholar] [CrossRef]
- Calabro, F.J.; Murty, V.P.; Jalbrzikowski, M.; Tervo-Clemmens, B.; Luna, B. Development of Hippocampal–Prefrontal Cortex Interactions through Adolescence. Cereb. Cortex 2019, 30, 1548–1558. [Google Scholar] [CrossRef]
- Salomon, C.; Trollor, J. Young people with an intellectual disability experience poorer physical and mental health during transition to adulthood. Evid. Based Nurs. 2017, 21, 20. [Google Scholar] [CrossRef]
- Forte, M.; Jahoda, A.; Dagnan, D. An anxious time? Exploring the nature of worries experienced by young people with a mild to moderate intellectual disability as they make the transition to adulthood. Br. J. Clin. Psychol. 2011, 50, 398–411. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, J.E.; Joussemet, M. The Benefits of Supporting the Autonomy of Individuals with Mild Intellectual Disabilities: An Experimental Study. J. Appl. Res. Intellect. Disabil. 2016, 30, 830–846. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, K.; Ouellette-Kuntz, H.; Blinkhorn, A.; Démoré, A. Out of School and Into Distress: Families of Young Adults with Intellectual and Developmental Disabilities in Transition. J. Appl. Res. Intellect. Disabil. 2016, 30, 774–781. [Google Scholar] [CrossRef]
- Hronis, A.; Roberts, L.; Kneebone, I.I. A review of cognitive impairments in children with intellectual disabilities: Implications for cognitive behaviour therapy. Br. J. Clin. Psychol. 2017, 56, 189–207. [Google Scholar] [CrossRef]
- Whitehouse, R.M.; Tudway, J.A.; Look, R.; Kroese, B.S. Adapting Individual Psychotherapy for Adults with Intellectual Disabilities: A Comparative Review of the Cognitive-Behavioural and Psychodynamic Literature. J. Appl. Res. Intellect. Disabil. 2006, 19, 55–65. [Google Scholar] [CrossRef]
- Andrews, G.; Slade, T. Interpreting scores on the Kessler Psychological Distress Scale (K10). Aust. N. Z. J. Public Health 2001, 25, 494–497. [Google Scholar] [CrossRef] [PubMed]
- Newby, J.M.; Twomey, C.; Li, S.S.Y.; Andrews, G. Transdiagnostic computerised cognitive behavioural therapy for depression and anxiety: A systematic review and meta-analysis. J. Affect. Disord. 2016, 199, 30–41. [Google Scholar] [CrossRef]
- Spek, V.; Cuijpers, P.; Nyklícek, I.; Riper, H.; Keyzer, J.; Pop, V. Internet-based cognitive behaviour therapy for symptoms of depression and anxiety: A meta-analysis. Psychol. Med. 2006, 37, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Proudfoot, J.; Clarke, J.; Birch, M.-R.; Whitton, A.E.; Parker, G.; Manicavasagar, V.; Harrison, V.; Christensen, H.; Hadzi-Pavlovic, D. Impact of a mobile phone and web program on symptom and functional outcomes for people with mild-to-moderate depression, anxiety and stress: A randomised controlled trial. BMC Psychiatry 2013, 13, 312. [Google Scholar] [CrossRef] [Green Version]
- SPIRIT. SPIRIT 2013 Checklist: Recommended Items to Address in a Clinical Trial Protocol and Related Documents. 1–5 (Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT), Cananda). 2013. Available online: https://www.spirit-statement.org (accessed on 15 June 2019).
- Schulz, K.F.A.D.; Moher, D.; CONSORT Group. CONSORT-EHEALTH Checklist (V.1.6.1): Information to Include When Reporting Ehealth/Mhealth Trials (Web-Based/Internet-Based Intervention and Decision Aids, but also Social Media, Serious Games, DVDs, Mobile Applications, Certain Telehealth Applications). 1–13. 2011. Available online: http://www.consort-statement.org (accessed on 15 June 2019).
- Maulik, P.K.; Mascarenhas, M.N.; Mathers, C.D.; Dua, T.; Saxena, S. Prevalence of intellectual disability: A meta-analysis of population-based studies. Res. Dev. Disabil. 2011, 32, 419–436. [Google Scholar] [CrossRef]
- Petterson, B.; Bourke, J.; Leonard, H.; Jacoby, P.; Bower, C. Co-occurrence of birth defects and intellectual disability. Paediatr. Perinat. Epidemiol. 2007, 21, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Leonard, H.; Petterson, B.; Bower, C.; Sanders, R. Prevalence of intellectual disability in Western Australia. Paediatr. Perinat. Epidemiol. 2003, 17, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Wen, X. The Definition and Prevalence of Intellectual Disability in Australia; Australian Institute of Health & Welfare: Canberra, Australia, 1997.
- Messer, D.; Nash, G. An evaluation of the effectiveness of a computer-assisted reading intervention. J. Res. Read. 2017, 41, 140–158. [Google Scholar] [CrossRef] [Green Version]
- Watfern, C.; Heck, C.; Rule, C.; Baldwin, P.; Boydell, K.M.; Vereenooghe, L.; Tao, S. Feasibility and Acceptability of a Mental Health Website for Adults with an Intellectual Disability: Qualitative Evaluation. JMIR Ment. Health 2019, 6, e12958. [Google Scholar] [CrossRef] [Green Version]
- Ware, R.S.; McPherson, L.; Lennox, N.G. Drop-out during a randomized trial with adolescents with intellectual disability was associated with participant burden, while drop-out at study exit was associated with carer and household characteristics. Res. Dev. Disabil. 2017, 71, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Esbensen, A.J.; Rojahn, J.; Aman, M.G.; Ruedrich, S. Reliability and Validity of an Assessment Instrument for Anxiety, Depression, and Mood among Individuals with Mental Retardation. J. Autism Dev. Disord. 2003, 33, 617–629. [Google Scholar] [CrossRef]
- WHO. Measuring Health and Disability: Manual for WHO Disability Assessment Schedule (WHODAS 2.0); World Health Organization: Geneva, Switzerland, 2010; Available online: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health/who-disability-assessment-schedule (accessed on 15 June 2019).
- Woodbury-Smith, M.R.; Robinson, J.; Wheelwright, S.; Baron-Cohen, S. Screening Adults for Asperger Syndrome Using the AQ: A Preliminary Study of its Diagnostic Validity in Clinical Practice. J. Autism Dev. Disord. 2005, 35, 331–335. [Google Scholar] [CrossRef]
- Dunn, K.; Rydzewska, E.; MacIntyre, C.; Rintoul, J.; Cooper, S.-A. The prevalence and general health status of people with intellectual disabilities and autism co-occurring together: A total population study. J. Intellect. Disabil. Res. 2018, 63, 277–285. [Google Scholar] [CrossRef]
- Vereenooghe, L.; Langdon, P.E. Psychological therapies for people with intellectual disabilities: A systematic review and meta-analysis. Res. Dev. Disabil. 2013, 34, 4085–4102. [Google Scholar] [CrossRef]
- Unwin, G.; Tsimopoulou, I.; Kroese, B.S.; Azmi, S. Effectiveness of cognitive behavioural therapy (CBT) programmes for anxiety or depression in adults with intellectual disabilities: A review of the literature. Res. Dev. Disabil. 2016, 51–52, 60–75. [Google Scholar] [CrossRef]
- Mallinckrodt, C.H.; Clark, W.S.; David, S.R. Accounting for dropout bias using mixed-effects models. J. Biopharm. Stat. 2001, 11, 9–21. [Google Scholar] [CrossRef]
- Jo, B. Estimation of Intervention Effects with Noncompliance: Alternative Model Specifications. J. Educ. Behav. Stat. 2002, 27, 385–409. [Google Scholar] [CrossRef]
- Royal Commission. Public Hearing 4—Health Care and Services for People with Cognitive Disability; Commonwealth Government: Sydney, Australia, 2020. Available online: https://disability.royalcommission.gov.au/publications/report-public-hearing-4-healthcare-people-cognitive-disability (accessed on 7 January 2021).
- Eysenbach, G. The Law of Attrition. J. Med. Internet Res. 2005, 7, e11. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcomes | Baseline | Post-Intervention (8 Weeks Post Randomisation) | Follow-Up (3 Months Post Treatment Completion) |
|---|---|---|---|
| Primary outcome measure | |||
| Anxiety Depression and Mood Scale (ADAMS) | X | X | X |
| Secondary measures | |||
| Kessler 10 (K10) | X | X | X |
| WHO Disability Assessment Schedule (WHO-DAS) | X | X | X |
| Autism Quotient (AQ) | X | - | - |
| CBS Health Cognitive Assessment | X | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baldwin, P.A.; Rasmussen, V.; Trollor, J.N.; Zhao, J.L.; Anderson, J.; Christensen, H.; Boydell, K. IDTWO: A Protocol for a Randomised Controlled Trial of a Web-Based Mental Health Intervention for Australians with Intellectual Disability. Int. J. Environ. Res. Public Health 2021, 18, 2473. https://doi.org/10.3390/ijerph18052473
Baldwin PA, Rasmussen V, Trollor JN, Zhao JL, Anderson J, Christensen H, Boydell K. IDTWO: A Protocol for a Randomised Controlled Trial of a Web-Based Mental Health Intervention for Australians with Intellectual Disability. International Journal of Environmental Research and Public Health. 2021; 18(5):2473. https://doi.org/10.3390/ijerph18052473
Chicago/Turabian StyleBaldwin, Peter A., Victoria Rasmussen, Julian N. Trollor, Jenna L. Zhao, Josephine Anderson, Helen Christensen, and Katherine Boydell. 2021. "IDTWO: A Protocol for a Randomised Controlled Trial of a Web-Based Mental Health Intervention for Australians with Intellectual Disability" International Journal of Environmental Research and Public Health 18, no. 5: 2473. https://doi.org/10.3390/ijerph18052473