
The Feasibility of Cervical Elastography in Predicting Preterm Delivery in Singleton Pregnancy with Short Cervix Following Progesterone Treatment

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
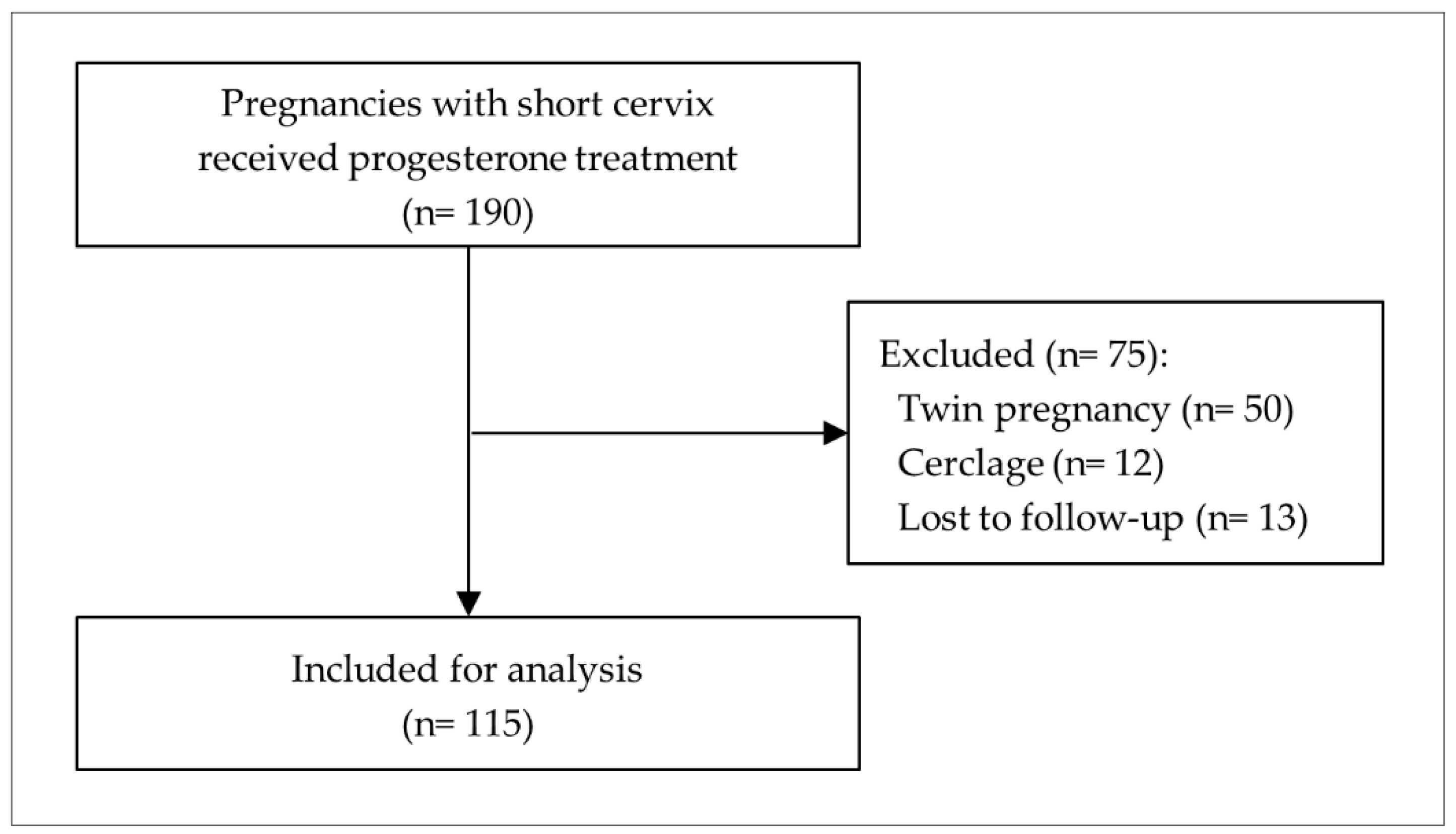
2.1. Study Population
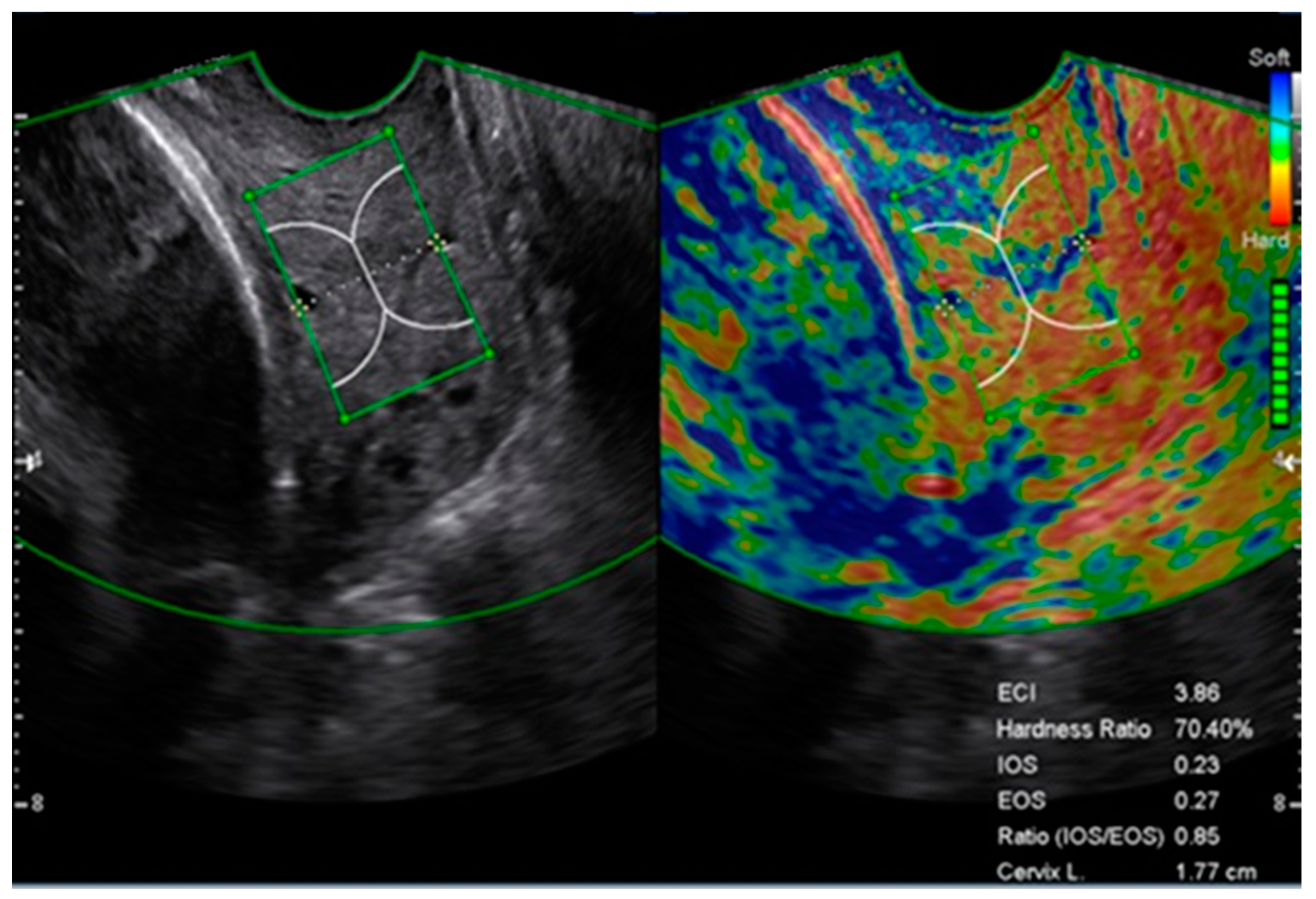
2.2. Cervical Length and Elastography Measurement
2.3. Elastography Image Auditing
2.4. Statistical Analysis
3. Results
3.1. Study Population and Maternal Characteristics
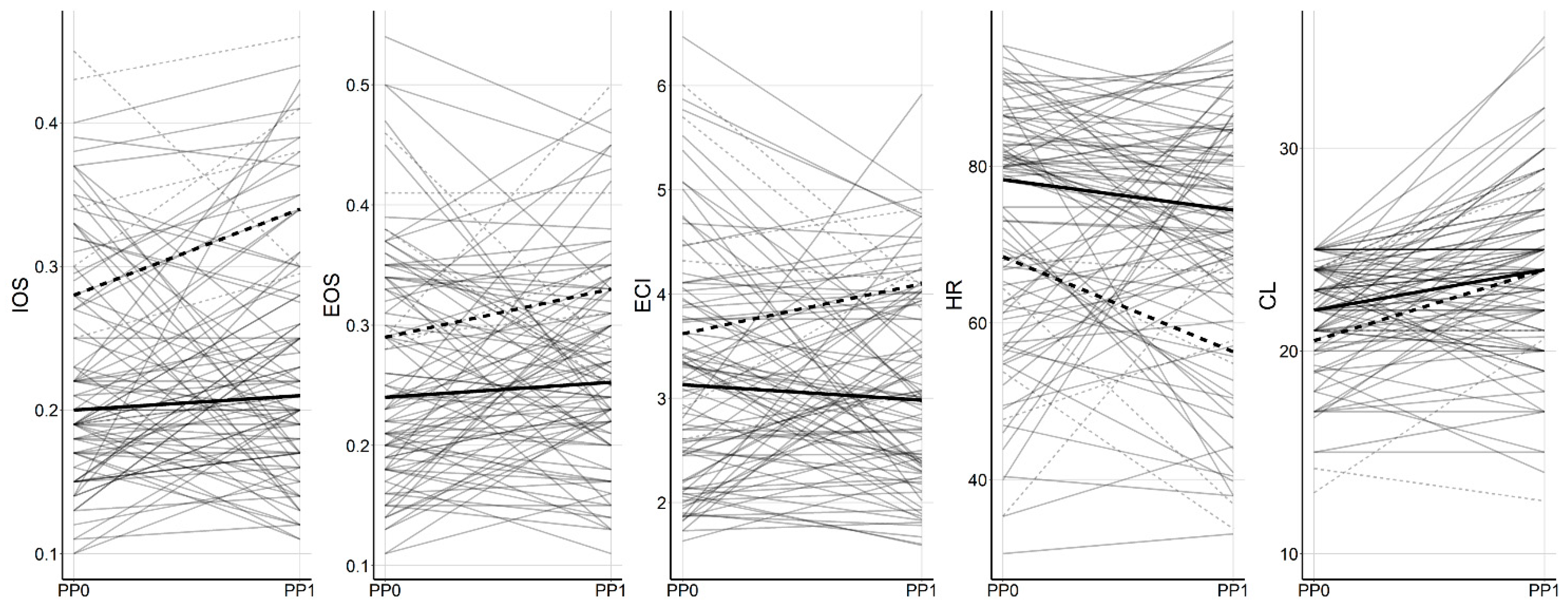
3.2. Pre and Postprogesterone Elastographic Parameters
3.3. Association between Elastographic Parameters and sPTD at <32 Weeks of Gestation
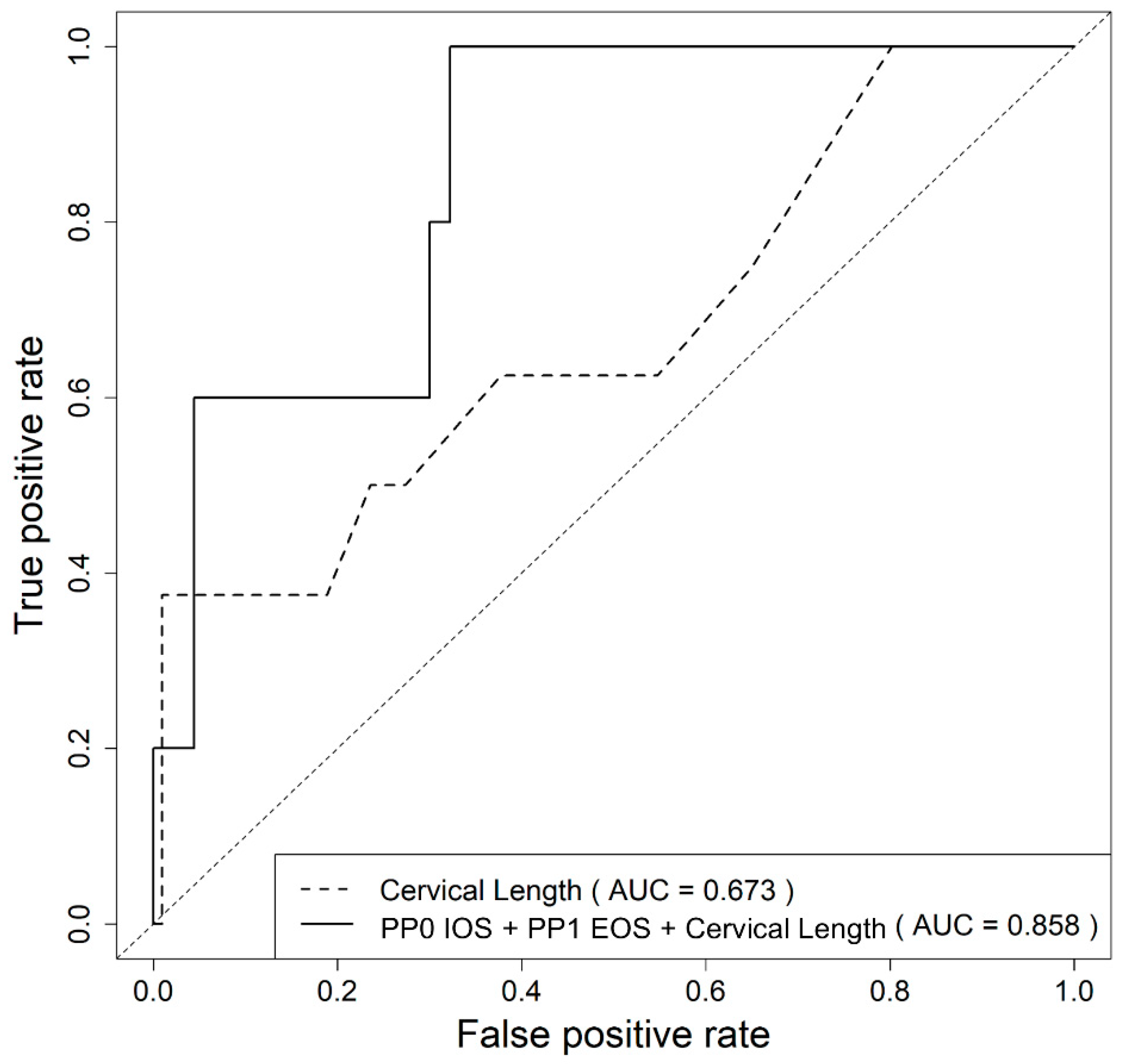
3.4. Prediction of sPTD at <32 Weeks of Gestation Based on Clinical and Elastographic Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Romero, R.; Conde-Agudelo, A.; Da Fonseca, E.; O’Brien, J.M.; Cetingoz, E.; Creasy, G.W.; Hassan, S.S.; Nicolaides, K.H. Vaginal progesterone for preventing preterm birth and adverse perinatal outcomes in singleton gestations with a short cervix: A meta-analysis of individual patient data. Am. J. Obstet. Gynecol. 2018, 218, 161–180. [Google Scholar] [CrossRef] [Green Version]
- Romero, R.; Conde-Agudelo, A.; El-Refaie, W.; Rode, L.; Brizot, M.L.; Cetingoz, E.; Serra, V.; Da Fonseca, E.; Abdelhafez, M.S.; Tabor, A.; et al. Vaginal progesterone decreases preterm birth and neonatal morbidity and mortality in women with a twin gestation and a short cervix: An updated meta-analysis of individual patient data. Ultrasound Obstet. Gynecol. 2017, 49, 303–314. [Google Scholar] [CrossRef] [Green Version]
- Norwitz, E.R.; Caughey, A.B. Progesterone supplementation and the prevention of preterm birth. Rev. Obstet. Gynecol. 2011, 4, 60–72. [Google Scholar]
- Norman, J.E.; Marlow, N.; Messow, C.M.; Shennan, A.; Bennett, P.R.; Thornton, S.; Robson, S.C.; McConnachie, A.; Petrou, S.; Sebire, N.J.; et al. Vaginal progesterone prophylaxis for preterm birth (the OPPTIMUM study): A multicentre, randomised, double-blind trial. Lancet 2016, 387, 2106–2116. [Google Scholar] [CrossRef] [Green Version]
- Owen, J.; Iams, J.D.; Hauth, J.C. Vaginal sonography and cervical incompetence. Am. J. Obstet. Gynecol. 2003, 188, 586–596. [Google Scholar] [CrossRef]
- Owen, J.; Yost, N.; Berghella, V.; Thom, E.; Swain, M.; Dildy, G.A.; Miodovnik, M.; Langer, O.; Sibai, B.; McNellis, D.; et al. Mid-trimester endovaginal sonography in women at high risk for spontaneous preterm birth. JAMA J. Am. Med. Assoc. 2001, 286, 1340–1348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandez-Andrade, E.; Maymon, E.; Luewan, S.; Bhatti, G.; Mehrmohammadi, M.; Erez, O.; Pacora, P.; Done, B.; Hassan, S.S.; Romero, R. A soft cervix, categorized by shear-wave elastography, in women with short or with normal cervical length at 18–24 weeks is associated with a higher prevalence of spontaneous preterm delivery. J. Perinat. Med. 2018, 46, 489–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, H.S.; Kwon, H.; Kwak, D.W.; Kim, M.Y.; Seol, H.J.; Hong, J.S.; Shim, J.Y.; Choi, S.K.; Hwang, H.S.; Oh, M.J.; et al. Addition of Cervical Elastography May Increase Preterm Delivery Prediction Performance in Pregnant Women with Short Cervix: A Prospective Study. J. Korean Med. Sci. 2019, 34, e68. [Google Scholar] [CrossRef]
- Wozniak, S.; Czuczwar, P.; Szkodziak, P.; Milart, P.; Wozniakowska, E.; Paszkowski, T. Elastography in predicting preterm delivery in asymptomatic, low-risk women: A prospective observational study. BMC Pregnancy Childbirth 2014, 14. [Google Scholar] [CrossRef] [Green Version]
- Köbbing, K.; Fruscalzo, A.; Hammer, K.; Mollers, M.; Falkenberg, M.; Kwiecien, R.; Klockenbusch, W.; Schmitz, R. Quantitative Elastography of the uterine cervix as a predictor of preterm delivery. J. Perinatol. 2014, 34, 774–780. [Google Scholar] [CrossRef] [PubMed]
- Ferraioli, G.; Tinelli, C.; Dal Bello, B.; Zicchetti, M.; Filice, G.; Filice, C.; Grp, L.F.S. Accuracy of Real-Time Shear Wave Elastography for Assessing Liver Fibrosis in Chronic Hepatitis C: A Pilot Study. Hepatology 2012, 56, 2125–2133. [Google Scholar] [CrossRef]
- Friedrich-Rust, M.; Nierhoff, J.; Lupsor, M.; Sporea, I.; Fierbinteanu-Braticevici, C.; Strobel, D.; Takahashi, H.; Yoneda, M.; Suda, T.; Zeuzem, S.; et al. Performance of Acoustic Radiation Force Impulse imaging for the staging of liver fibrosis: A pooled meta-analysis. J. Viral Hepat. 2012, 19, E212–E219. [Google Scholar] [CrossRef] [PubMed]
- Trimboli, P.; Guglielmi, R.; Monti, S.; Misischi, I.; Graziano, F.; Nasrollah, N.; Amendola, S.; Morgante, S.N.; Deiana, M.G.; Valabrega, S.; et al. Ultrasound Sensitivity for Thyroid Malignancy Is Increased by Real-Time Elastography: A Prospective Multicenter Study. J. Clin. Endocr. Metab. 2012, 97, 4524–4530. [Google Scholar] [CrossRef] [Green Version]
- Dong, F.J.; Li, M.; Jiao, Y.; Xu, J.F.; Xiong, Y.; Zhang, L.; Luo, H.; Ding, Z.M. Acoustic Radiation Force Impulse imaging for detecting thyroid nodules: A systematic review and pooled meta-analysis. Med. Ultrason. 2015, 17, 192–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barr, R.G. Real-Time Ultrasound Elasticity of the Breast Initial Clinical Results. Ultrasound Q. 2010, 26, 61–66. [Google Scholar] [CrossRef]
- Feldmann, A.; Langlois, C.; Dewailly, M.; Martinez, E.F.; Boulanger, L.; Kerdraon, O.; Faye, N. Shear Wave Elastography (SWE): An Analysis of Breast Lesion Characterization in 83 Breast Lesions. Ultrasound Med. Biol. 2015, 41, 2594–2604. [Google Scholar] [CrossRef]
- Swiatkowska-Freund, M.; Preis, K. Cervical elastography during pregnancy: Clinical perspectives. Int. J. Women’s Health 2017, 9, 245–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandez-Andrade, E.; Romero, R.; Korzeniewski, S.J.; Ahn, H.; Aurioles-Garibay, A.; Garcia, M.; Schwartz, A.G.; Yeo, L.; Chaiworapongsa, T.; Hassan, S.S. Cervical strain determined by ultrasound elastography and its association with spontaneous preterm delivery. J. Perinat. Med. 2014, 42, 159–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yellon, S.M. Contributions to the dynamics of cervix remodeling prior to term and preterm birth. Biol. Reprod. 2017, 96, 13–23. [Google Scholar] [CrossRef]
- Kirby, M.A.; Heuerman, A.C.; Custer, M.; Dobyns, A.E.; Strilaeff, R.; Stutz, K.N.; Cooperrider, J.; Elsissy, J.G.; Yellon, S.M. Progesterone Receptor-Mediated Actions Regulate Remodeling of the Cervix in Preparation for Preterm Parturition. Reprod. Sci. 2016, 23, 1473–1483. [Google Scholar] [CrossRef] [Green Version]
- Weatherborn, M.; Mesiano, S. Rationale for current and future progestin-based therapies to prevent preterm birth. Best Pract. Res. Clin. Obstet. 2018, 52, 114–125. [Google Scholar] [CrossRef]
- Sfakianaki, A.K.; Norwitz, E.R. Mechanisms of progesterone action in inhibiting prematurity. J. Matern.-Fetal Neonatal Med. 2006, 19, 763–772. [Google Scholar] [CrossRef]
- Swiatkowska-Freund, M.; Preis, K. Elastography of the uterine cervix: Implications for success of induction of labor. Ultrasound Obstet. Gynecol. 2011, 38, 52–56. [Google Scholar] [CrossRef]
- Fruscalzo, A.; Mazza, E.; Feltovich, H.; Schmitz, R. Cervical elastography during pregnancy: A critical review of current approaches with a focus on controversies and limitations. J. Med. Ultrason. 2016, 43, 493–504. [Google Scholar] [CrossRef]
- Feltovich, H.; Carlson, L. New techniques in evaluation of the cervix. Semin. Perinatol. 2017, 41, 477–484. [Google Scholar] [CrossRef]
- Marret, S.; Ancel, P.Y.; Marpeau, L.; Marchand, L.; Pierrat, V.; Larroque, B.; Foix-L’Helias, L.; Thiriez, G.; Fresson, J.; Alberge, C.; et al. Neonatal and 5-year outcomes after birth at 30–34 weeks of gestation. Obstet. Gynecol. 2007, 110, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Seol, H.J.; Sung, J.H.; Seong, W.J.; Kim, H.M.; Park, H.S.; Kwon, H.; Hwang, H.S.; Jung, Y.J.; Kwon, J.Y.; Oh, S.Y. Standardization of measurement of cervical elastography, its reproducibility, and analysis of baseline clinical factors affecting elastographic parameters. Obstet. Gynecol. Sci. 2020, 63, 42–54. [Google Scholar] [CrossRef] [PubMed]
- Conde-Agudelo, A.; Romero, R. Vaginal progesterone to prevent preterm birth in pregnant women with a sonographic short cervix: Clinical and public health implications. Am. J. Obstet. Gynecol. 2016, 214, 235–242. [Google Scholar] [CrossRef] [Green Version]
- Garry, D.J.; Baker, D.A.; Persad, M.D.; Peresleni, T.; Kocis, C.; Demishev, M. Progesterone effects on vaginal cytokines in women with a history of preterm birth. PLoS ONE 2018, 13. [Google Scholar] [CrossRef] [PubMed]
- Pustotina, O. Effectiveness of dydrogesterone, 17-OH progesterone and micronized progesterone in prevention of preterm birth in women with a short cervix. J. Matern.-Fetal Neonatal Med. 2018, 31, 1830–1838. [Google Scholar] [CrossRef]
- Raba, G.; Tabarkiewicz, J. Cytokines in Preterm Delivery: Proposal of a New Diagnostic Algorithm. J. Immunol. Res. 2018, 2018. [Google Scholar] [CrossRef] [Green Version]
- Suff, N.; Story, L.; Shennan, A. The prediction of preterm delivery: What is new? Semin. Fetal Neonatal Med. 2019, 24, 27–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wozniak, S.; Czuczwar, P.; Szkodziak, P.; Wrona, W.; Paszkowski, T. Elastography for predicting preterm delivery in patients with short cervical length at 18-22 weeks of gestation: A prospective observational study. Ginekol. Polska 2015, 86, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Andrade, E.; Garcia, M.; Ahn, H.; Korzeniewski, S.J.; Saker, H.; Yeo, L.; Chaiworapongsa, T.; Hassan, S.S.; Romero, R. Strain at the internal cervical os assessed with quasi-static elastography is associated with the risk of spontaneous preterm delivery at ≤ 34 weeks of gestation. J. Perinat. Med. 2015, 43, 657–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassan, S.S.; Romero, R.; Vidyadhari, D.; Fusey, S.; Baxter, J.K.; Khandelwal, M.; Vijayaraghavan, J.; Trivedi, Y.; Soma-Pillay, P.; Sambarey, P.; et al. Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix: A multicenter, randomized, double-blind, placebo-controlled trial. Ultrasound Obstet. Gynecol. 2011, 38, 18–31. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 115) | Delivery ≥32 Weeks (n = 106) | Delivery <32 Weeks (n = 9) | p-Value |
|---|---|---|---|---|
| Maternal age, years | 34 (25–42) | 34 (25–42) | 35 (28–39) | 0.415 |
| Prepregnancy BMI, kg/m2 | 22.9 (19.0–36.2) | 22.9 (19.0–36.2) | 22.8 (20.4–27.3) | 0.577 |
| Current smoking | 1 (0.9%) | 1 (0.9%) | 0 (0.0%) | 1.000 |
| Multiparity | 57 (49.6%) | 54 (50.9%) | 3 (33.3%) | 0.655 |
| Prior miscarriage | 39 (33.9%) | 35 (33.0%) | 4 (44.4%) | 0.803 |
| Prior cesarean section | 20 (17.4%) | 19 (17.9%) | 1 (11.1%) | 0.999 |
| Prior preterm birth | 8 (7.0%) | 8 (7.5%) | 0 (0.0%) | 0.999 |
| IVF-ET | 17 (14.8%) | 14 (13.2%) | 3 (33.3%) | 0.227 |
| Prior conization | 10 (8.7%) | 9 (8.5%) | 1 (11.1%) | 0.844 |
| Pregestational diabetes mellitus | 2 (1.7%) | 1 (0.9%) | 1 (11.1%) | 0.192 |
| GDM | 11 (9.9%) | 10 (9.7%) | 1 (12.5%) | 0.852 |
| Preeclampsia | 2 (1.8%) | 1 (1.0%) | 1 (12.5%) | 0.182 |
| Chronic hypertension | 3 (2.6%) | 2 (1.9%) | 1 (11.1%) | 0.299 |
| Thyroid disease | 6 (5.2%) | 4 (3.8%) | 2 (22.2%) | 0.098 |
| GA at diagnosis | 22 w 6 d (16 w 1 d–28 w 6 d) | 22 w 5 d (16 w 1 d–28 w 6 d) | 23 w 5 d (17 w 0 d–26 w 3 d) | 0.599 |
| Cervical length, mm | 22.0 (10.0–25.0) | 22.0 (10.0–25.0) | 20.5 (13.0–24.0) | 0.103 |
| Funneling | 8 (7.0%) | 6 (5.7%) | 2 (22.2%) | 0.176 |
| Positive fibronectin | 27 (35.5%) | 22 (32.4%) | 5 (62.5%) | 0.256 |
| Progesterone type | ||||
| Vaginal suppository | 110 (95.7%) | 101 (95.3%) | 9 (100.0%) | 0.999 |
| IM injection | 5 (4.3%) | 5 (4.7%) | 0 (0.0%) | |
| GA at delivery | 38 w 2 d (18 w 5 d–41 w 0 d) | 38 w 3 d (33 w 1 d–41 w 0 d) | 27 w 0 d (18 w 5 d–31 w 6 d) | <0.001 |
| Cesarean delivery | 62 (53.9%) | 55 (51.9%) | 7 (77.8%) | 0.337 |
| Birth weight, g | 3040 (830–4030) | 3110 (1760–4030) | 1075 (830–1830) | <0.001 |
| Apgar score <7 at 5 min | 3 (2.9%) | 2 (2.1%) | 1 (12.5%) | 0.296 |
| NICU admission | 21 (20.4%) | 13 (13.7%) | 8 (100.0%) | <0.001 |
| Variables | PP0 (Pretreatment) | p-Value | PP1 (Post-Treatment) | p-Value | ||
|---|---|---|---|---|---|---|
| Delivery ≥ 32 Weeks (n = 105) | Delivery < 32 Weeks (n = 9) | Delivery ≥ 32 Weeks (n = 90) | Delivery < 32 Weeks (n = 6) | |||
| IOS | 0.22 ± 0.07 | 0.30 ± 0.09 | 0.001 | 0.23 ± 0.08 | 0.34 ± 0.09 | 0.002 |
| EOS | 0.26 ± 0.09 | 0.32 ± 0.08 | 0.063 | 0.26 ± 0.08 | 0.35 ± 0.09 | 0.018 |
| ECI | 3.19 ± 1.09 | 4.00 ± 1.23 | 0.037 | 3.09 ± 0.95 | 4.03 ± 0.58 | 0.020 |
| HR | 73.19 ± 14.77 | 61.17 ± 12.74 | 0.020 | 72.29 ± 15.40 | 53.24 ± 14.98 | 0.004 |
| Variable | PP0 (Pretreatment) | PP1 (Post-Treatment) | ||||||
|---|---|---|---|---|---|---|---|---|
| Unadjusted OR (95% CI) | p-Value | Adjusted OR (95% CI) * | p-Value | Unadjusted OR (95% CI) | p-Value | Adjusted OR (95% CI) * | p-Value | |
| IOS (×0.1) | 3.60 (1.56–9.28) | 0.004 | 2.92 (1.07–8.77) | 0.040 | 3.94 (1.55–12.46) | 0.007 | 4.39 (1.52–17.29) | 0.012 |
| EOS (×0.1) | 1.89 (0.94–3.87) | 0.071 | 2.13 (0.94–5.03) | 0.070 | 2.88 (1.16–7.97) | 0.027 | 3.65 (1.28–13.74) | 0.026 |
| ECI (×0.1) | 1.06 (1.00–1.12) | 0.045 | 1.06 (0.99–1.13) | 0.089 | 1.11 (1.01–1.23) | 0.032 | 1.11 (1.00–1.25) | 0.054 |
| HR | 0.95 (0.91–0.99) | 0.027 | 0.96 (0.91–1.01) | 0.122 | 0.93 (0.88–0.98) | 0.012 | 0.92 (0.86–0.98) | 0.016 |
| Model | AUC (95% CI) | p-Value * |
|---|---|---|
| CL | 0.673 (0.448–0.898) | Reference |
| PP0 IOS (×0.1) + CL | 0.794 (0.607–0.981) | 0.105 |
| PP1 IOS (×0.1) + CL | 0.831 (0.575–1.000) | 0.133 |
| PP1 EOS (×0.1) + CL | 0.827 (0.624–1.000) | 0.103 |
| PP0 IOS (×0.1) + PP1 IOS (×0.1) + CL | 0.831 (0.561–1.000) | 0.149 |
| PP0 IOS (×0.1) + PP1 EOS (×0.1) + CL | 0.858 (0.714–1.000) | 0.041 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, Y.J.; Kwon, H.; Shin, J.; Park, Y.; Heo, S.-J.; Park, H.S.; Oh, S.-y.; Sung, J.-H.; Seol, H.-J.; Kim, H.M.; et al. The Feasibility of Cervical Elastography in Predicting Preterm Delivery in Singleton Pregnancy with Short Cervix Following Progesterone Treatment. Int. J. Environ. Res. Public Health 2021, 18, 2026. https://doi.org/10.3390/ijerph18042026
Jung YJ, Kwon H, Shin J, Park Y, Heo S-J, Park HS, Oh S-y, Sung J-H, Seol H-J, Kim HM, et al. The Feasibility of Cervical Elastography in Predicting Preterm Delivery in Singleton Pregnancy with Short Cervix Following Progesterone Treatment. International Journal of Environmental Research and Public Health. 2021; 18(4):2026. https://doi.org/10.3390/ijerph18042026
Chicago/Turabian StyleJung, Yun Ji, Hayan Kwon, Jeongeun Shin, Yejin Park, Seok-Jae Heo, Hyun Soo Park, Soo-young Oh, Ji-Hee Sung, Hyun-Joo Seol, Hyun Mi Kim, and et al. 2021. "The Feasibility of Cervical Elastography in Predicting Preterm Delivery in Singleton Pregnancy with Short Cervix Following Progesterone Treatment" International Journal of Environmental Research and Public Health 18, no. 4: 2026. https://doi.org/10.3390/ijerph18042026