Personal and Environmental Risk Factors at Birth and Hospital Admission: Direct and Vitamin D-Mediated Effects on Bronchiolitis Hospitalization in Italian Children

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Procedures
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Erickson, E.N.; Bhakta, R.T.; Mendez, M.D. Pediatric Bronchiolitis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Fauroux, B.; Hascoët, J.-M.; Jarreau, P.-H.; Magny, J.-F.; Rozé, J.-C.; Saliba, E.; Schwarzinger, M. Risk Factors for Bronchiolitis Hospitalization in Infants: A French Nationwide Retrospective Cohort Study over Four Consecutive Seasons (2009–2013). PLoS ONE 2020, 15, e0229766. [Google Scholar] [CrossRef]
- Haataja, P.; Korhonen, P.; Ojala, R.; Hirvonen, M.; Korppi, M.; Gissler, M.; Luukkaala, T.; Tammela, O. Hospital Admissions for Lower Respiratory Tract Infections after Early-, Late-, and Post-Term Birth. Paediatr. Perinat. Epidemiol. 2020, 34, 139–149. [Google Scholar] [CrossRef]
- Halasa, N.; Williams, J.; Faouri, S.; Shehabi, A.; Vermund, S.H.; Wang, L.; Fonnesbeck, C.; Khuri-Bulos, N. Natural History and Epidemiology of Respiratory Syncytial Virus Infection in the Middle East: Hospital Surveillance for Children under Age Two in Jordan. Vaccine 2015, 33, 6479–6487. [Google Scholar] [CrossRef] [Green Version]
- Roth, D.; Jones, A.; Prosser, C.; Robinson, J.; Vohra, S. Vitamin D Status Is Not Associated with the Risk of Hospitalization for Acute Bronchiolitis in Early Childhood. Eur. J. Clin. Nutr. 2009, 63, 297–299. [Google Scholar] [CrossRef]
- Wrotek, A.; Czajkowska, M.; Jackowska, T. Seasonality of Respiratory Syncytial Virus Hospitalization; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Greenfield, J.A.; Park, P.S.; Farahani, E.; Malik, S.; Vieth, R.; McFarlane, N.A.; Shepherd, T.G.; Knight, J.A. Solar Ultraviolet-B Radiation and Vitamin D: A Cross-Sectional Population-Based Study Using Data from the 2007 to 2009 Canadian Health Measures Survey. BMC Public Health 2012, 12, 660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terrazas, C.; Castro-Rodriguez, J.A.; Camargo, C.A., Jr.; Borzutzky, A. Solar Radiation, Air Pollution, and Bronchiolitis Hospitalizations in Chile: An Ecological Study. Pediatr. Pulmonol. 2019, 54, 1466–1473. [Google Scholar] [CrossRef] [PubMed]
- Juzeniene, A.; Ma, L.-W.; Kwitniewski, M.; Polev, G.A.; Lagunova, Z.; Dahlback, A.; Moan, J. The Seasonality of Pandemic and Non-Pandemic Influenzas: The Roles of Solar Radiation and Vitamin D. Int. J. Infect. Dis. 2010, 14, e1099–e1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heikkinen, T.; Marttila, J.; Salmi, A.A.; Ruuskanen, O. Nasal Swab versus Nasopharyngeal Aspirate for Isolation of Respiratory Viruses. J. Clin. Microbiol. 2002, 40, 4337–4339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franchi, B.; Piazza, M.; Sandri, M.; Tenero, L.; Comberiati, P.; Boner, A.L.; Capristo, C. 25-Hydroxyvitamin D Serum Level in Children of Different Ethnicity Living in Italy. Eur. J. Pediatr. 2015, 174, 749–757. [Google Scholar] [CrossRef]
- Karlson, K.B.; Holm, A.; Breen, R. Comparing Regression Coefficients between Same-Sample Nested Models Using Logit and Probit: A New Method. Sociol. Methodol. 2012, 42, 286–313. [Google Scholar] [CrossRef]
- Rathbone, M. Khb: Comparing Nonlinear Regression Models. R Package Version 0.1. Available online: https://rdrr.io/rforge/khb (accessed on 15 December 2020).
- Saggese, G.; Vierucci, F.; Prodam, F.; Cardinale, F.; Cetin, I.; Chiappini, E.; de’Angelis, G.L.; Massari, M.; Del Giudice, E.M.; Del Giudice, M.M.; et al. Vitamin D in Pediatric Age: Consensus of the Italian Pediatric Society and the Italian Society of Preventive and Social Pediatrics, Jointly with the Italian Federation of Pediatricians. Ital. J. Pediatr. 2018, 44, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacKinnon, D.P.; Fairchild, A.J.; Fritz, M.S. Mediation Analysis. Annu. Rev. Psychol. 2007, 58, 593–614. [Google Scholar] [CrossRef] [PubMed]
- Fink, C.; Peters, R.L.; Koplin, J.J.; Brown, J.; Allen, K.J. Factors Affecting Vitamin D Status in Infants. Children 2019, 6, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, C.C.; Wall, C.R.; Crengle, S.; Scragg, R. Vitamin D Deficiency in Early Childhood: Prevalent in the Sunny South Pacific. Public Health Nutr. 2009, 12, 1893–1901. [Google Scholar] [CrossRef] [Green Version]
- Vierucci, F.; Del Pistoia, M.; Fanos, M.; Gori, M.; Carlone, G.; Erba, P.; Massimetti, G.; Federico, G.; Saggese, G. Vitamin D Status and Predictors of Hypovitaminosis D in Italian Children and Adolescents: A Cross-Sectional Study. Eur. J. Pediatr. 2013, 172, 1607–1617. [Google Scholar] [CrossRef]
- Erol, M.; Kaya, H.; Gayret, Ö.B.; Yiğit, Ö.; Hamilçıkan, Ş.; Can, E. The Effect of Vitamin D Deficiency on the Severity of Bronchiolitis in Infants. J. Pediatr. Res. 2017, 4, 12. [Google Scholar] [CrossRef]
- Mahyar, A.; Ayazi, P.; Abbasi, M.; Dalirani, R.; Taremiha, A.; Javadi, A.; Esmaeily, S. Evaluation of Serum 25-Hydroxy Vitamin D Levels in Children with Acute Bronchiolitis. Arch. Pediatr. Infect. Dis. 2017, 5, e39477. [Google Scholar] [CrossRef] [Green Version]
- Welliver, R.C. Respiratory Syncytial Virus and Other Respiratory Viruses. Pediatr. Infect. Dis. J. 2003, 22, S6–S12. [Google Scholar] [CrossRef]
- Meerhoff, T.J.; Paget, J.W.; Kimpen, J.L.; Schellevis, F. Variation of Respiratory Syncytial Virus and the Relation with Meteorological Factors in Different Winter Seasons. Pediatr. Infect. Dis. J. 2009, 28, 860–866. [Google Scholar] [CrossRef] [Green Version]
- Nenna, R.; Evangelisti, M.; Frassanito, A.; Scagnolari, C.; Pierangeli, A.; Antonelli, G.; Nicolai, A.; Arima, S.; Moretti, C.; Papoff, P.; et al. Respiratory Syncytial Virus Bronchiolitis, Weather Conditions and Air Pollution in an Italian Urban Area: An Observational Study. Environ. Res. 2017, 158, 188–193. [Google Scholar] [CrossRef]
- Brini, I.; Bhiri, S.; Ijaz, M.; Bouguila, J.; Nouri-Merchaoui, S.; Boughammoura, L.; Sboui, H.; Hannachi, N.; Boukadida, J. Temporal and Climate Characteristics of Respiratory Syncytial Virus Bronchiolitis in Neonates and Children in Sousse, Tunisia, during a 13-Year Surveillance. Environ. Sci. Pollut. Res. 2020, 27, 23379–23389. [Google Scholar] [CrossRef] [PubMed]
- Gökçe, Ş.; Kurugöl, Z.; Koturoğlu, G.; Çiçek, C.; Aslan, A. Etiology, Seasonality, and Clinical Features of Viral Respiratory Tract Infections in Children Hospitalized with Acute Bronchiolitis: A Single-Center Study. Glob. Pediatr. Health 2017, 4, 2333794X17714378. [Google Scholar] [CrossRef] [PubMed]
- Gil-Prieto, R.; Gonzalez-Escalada, A.; Marín-García, P.; Gallardo-Pino, C.; Gil-de-Miguel, A. Respiratory Syncytial Virus Bronchiolitis in Children up to 5 Years of Age in Spain: Epidemiology and Comorbidities: An Observational Study. Med. Baltim. 2015, 94, e831. [Google Scholar] [CrossRef]
- Leung, J.Y.; Lam, H.S.; Leung, G.M.; Schooling, C.M. Gestational Age, Birthweight for Gestational Age, and Childhood Hospitalisations for Asthma and Other Wheezing Disorders. Paediatr. Perinat. Epidemiol. 2016, 30, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Omar, N.; Mosaad, Y. Vitamin D and Immune System. Vitam Min. 2017, 6, 151. [Google Scholar]
- Di Cicco, M.E.; Ferrante, G.; Amato, D.; Capizzi, A.; De Pieri, C.; Ferraro, V.A.; Furno, M.; Tranchino, V.; La Grutta, S. Climate Change and Childhood Respiratory Health: A Call to Action for Paediatricians. Int. J. Environ. Res. Public. Health 2020, 17, 5344. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Controls n = 63 (50%) | Cases n = 63 (50%) | Overall n = 126 (100%) | p-Value 1 | |
|---|---|---|---|---|
| Gender, n (%) | 0.721 | |||
| Male | 32 (51) | 29 (46) | 61 (48) | |
| Female | 31 (49) | 34 (54) | 65 (52) | |
| Age at hospitalization (months), mean (SD) | 5.9 (4.3) | 6.0 (5.3) | 5.9 (4.8) | 0.925 |
| Weight at hospitalization (kg), mean (SD) | 7.1 (2.2) | 6.5 (2.2) | 6.8 (2.2) | 0.185 |
| Hospitalization season, n (%) | <0.001 | |||
| Summer-Autumn | 34 (54) | 11 (17) | 45 (35.7) | |
| Winter-Spring | 29 (46) | 52 (83) | 81 (64.3) | |
| Birth season, n (%) | ||||
| Summer-Autumn | 31 (49.2) | 34 (54.0) | 65 (51.6) | 0.721 |
| Winter-Spring | 32 (50.8) | 29 (46.0) | 61 (48.4) | |
| Birth weight (kg), mean (SD) | 3.2 (519.1) | 3.0 (766.3) | 3.1 (0.7) | 0.125 |
| Gestational age (weeks), mean (SD) | 39.1 (1.6) | 38.1 (3.6) | 38.6 (2.8) | 0.030 |
| Preterm birth (<37 weeks), n (%) | 1 (2) | 11 (18) | 12 (10) | 0.006 |
| Serum vitamin D (nmol/L), mean (SD) 1 | 78.6 (31.9) | 66.4 (21.0) | 72.5 (27.6) | 0.012 |
| Vitamin D deficiency-insufficiency (<75 nmol/L), n (%) | 33 (52) | 40 (64) | 73 (58) | 0.279 |
| Vitamin D MD (95% CI) | Bronchiolitis OR (95% CI) | |
|---|---|---|
| Hospitalized in Winter-Spring | ||
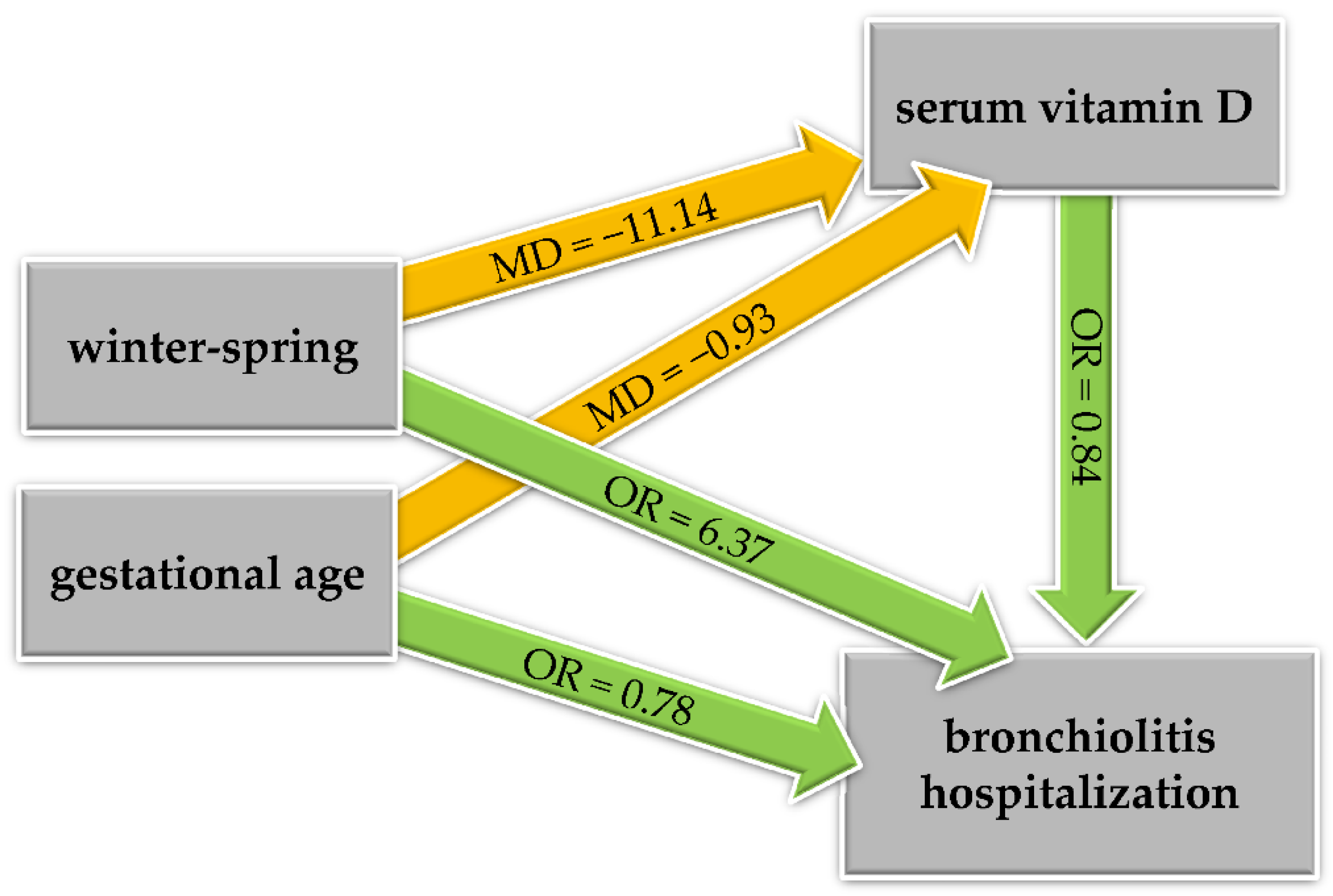
| Total effect | −11.14 (−21.05, −1.23), p = 0.029 | 7.72 (3.09, 19.29), p < 0.001 |
| Direct effect | - | 6.37 (2.58, 15.71), p < 0.001 |
| Indirect (vitamin D-mediated) effect | - | 1.21 (0.95, 1.55), p = 0.125 |
| Percent vitamin D-mediated | - | 9% |
| Gestational age (weeks), unit increase | ||
| Total effect | −0.93 (−2.63, 0.77), p = 0.285 | 0.79 (0.66, 0.95), p = 0.012 |
| Direct effect | - | 0.78 (0.65, 0.94), p = 0.008 |
| Indirect (vitamin D-mediated) effect | - | 1.02 (0.98, 1.05), p = 0.334 |
| Percent vitamin D-mediated | - | - 1 |
| Vitamin D (nmol/L), 10-unit increase | - | 0.84 (0.72, 0.98), p = 0.035 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaffanello, M.; Ferrante, G.; Fasola, S.; Piazza, M.; Piacentini, G.; La Grutta, S. Personal and Environmental Risk Factors at Birth and Hospital Admission: Direct and Vitamin D-Mediated Effects on Bronchiolitis Hospitalization in Italian Children. Int. J. Environ. Res. Public Health 2021, 18, 747. https://doi.org/10.3390/ijerph18020747
Zaffanello M, Ferrante G, Fasola S, Piazza M, Piacentini G, La Grutta S. Personal and Environmental Risk Factors at Birth and Hospital Admission: Direct and Vitamin D-Mediated Effects on Bronchiolitis Hospitalization in Italian Children. International Journal of Environmental Research and Public Health. 2021; 18(2):747. https://doi.org/10.3390/ijerph18020747
Chicago/Turabian StyleZaffanello, Marco, Giuliana Ferrante, Salvatore Fasola, Michele Piazza, Giorgio Piacentini, and Stefania La Grutta. 2021. "Personal and Environmental Risk Factors at Birth and Hospital Admission: Direct and Vitamin D-Mediated Effects on Bronchiolitis Hospitalization in Italian Children" International Journal of Environmental Research and Public Health 18, no. 2: 747. https://doi.org/10.3390/ijerph18020747