Indoor Formaldehyde Concentration, Personal Formaldehyde Exposure and Clinical Symptoms during Anatomy Dissection Sessions, University of Medicine 1, Yangon

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Location
2.3. Preparation of Formaldehyde-Embalmed Cadaver
2.4. Sampling Procedures
2.5. Air Sample Analysis
2.6. Questionnaire for Assessment of Formaldehyde-Related Clinical Symptoms
2.7. Statistical Analysis
3. Results and Discussion
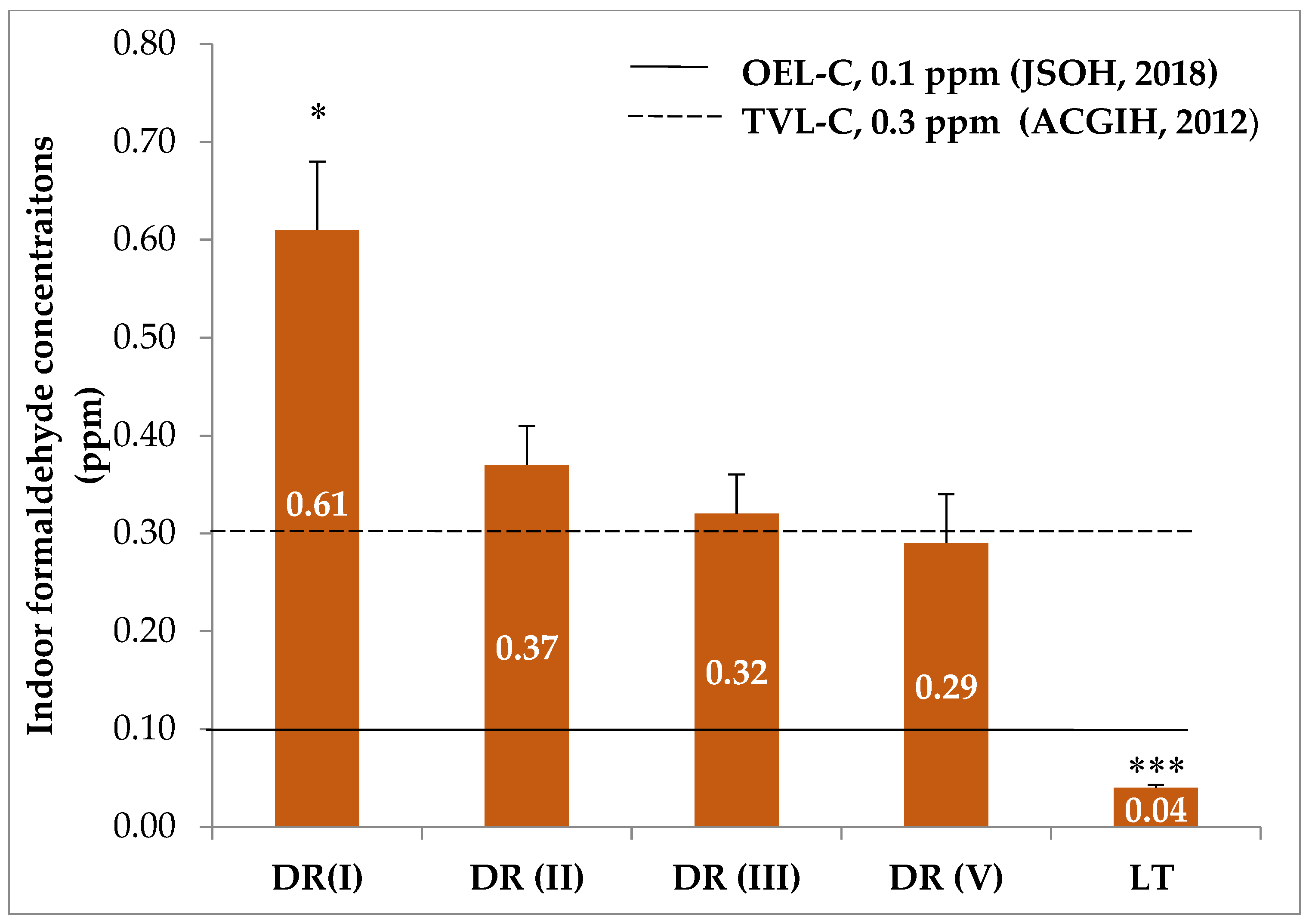
3.1. Indoor Formaldehyde Concentrations
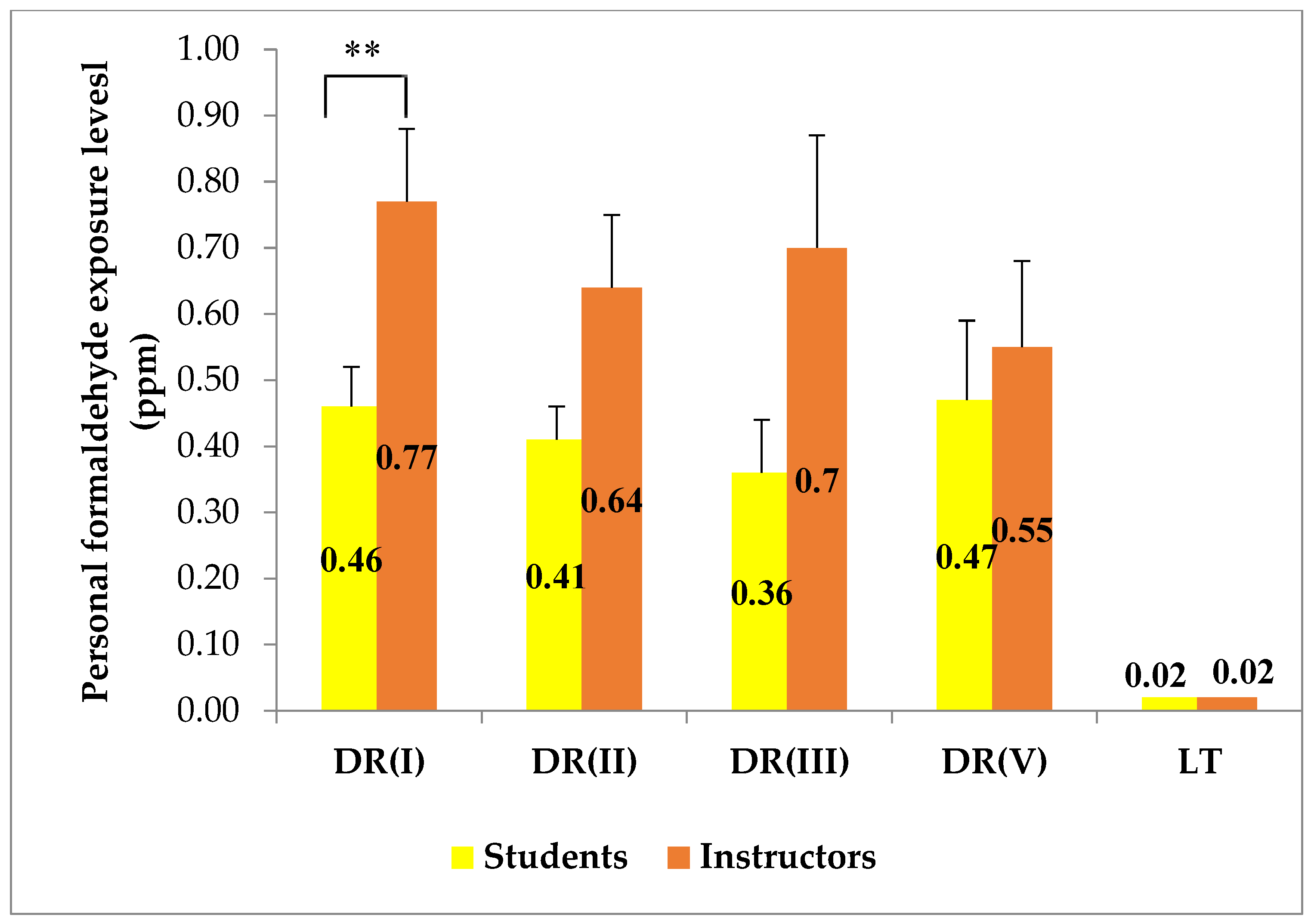
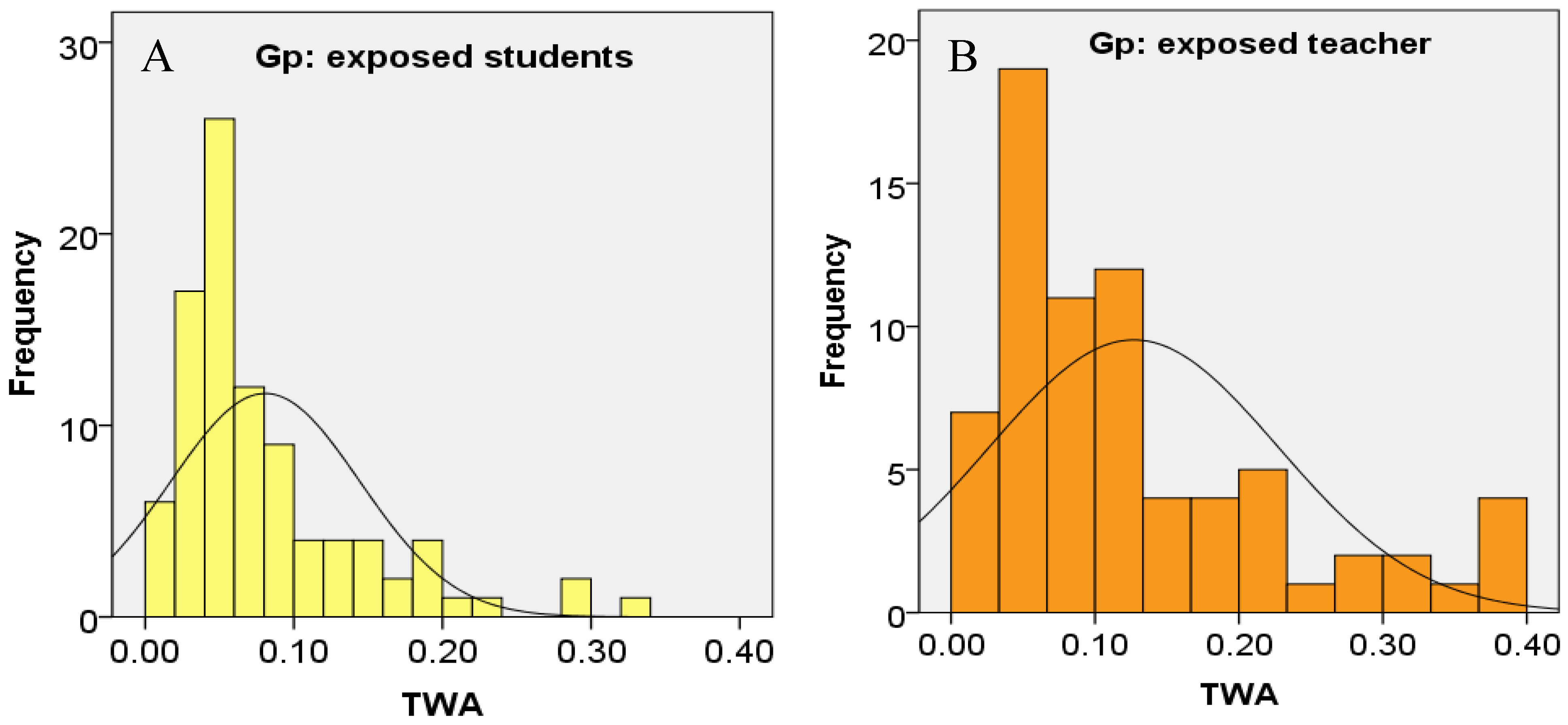
3.2. Personal Exposure Levels of Formaldehyde
3.3. Formaldehyde-Related Clinical Symptoms
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Turney, B.W. Anatomy in a modern medical curriculum. Ann. Roy Coll Surg. 2007, 89, 104–107. [Google Scholar] [CrossRef]
- Granger, N.A. Dissection laboratory is vital to medical gross anatomy education. Anat. Rec. Part B 2004, 281, 6–8. [Google Scholar] [CrossRef]
- Coleman, R.; Kogan, I. An improved low-formaldehyde embalming fluid to preserve cadavers for anatomy teaching. J. Anat. 1998, 192, 443–446. [Google Scholar] [CrossRef]
- Waschke, J.; Bergmann, M.; Bräuer, L.; Brenner, E.; Buchhorn, A.; Deutsch, A.; Dokter, M.; Egu, D.T.; Ergün, S.; Fassnacht, U. Recommendations of the working group of the Anatomische Gesellschaft on reduction of formaldehyde exposure in anatomical curricula and institutes. Ann. Anat. 2019, 221, 179–185. [Google Scholar] [CrossRef]
- Thiel, W. The preservation of the whole corpse with natural color. Ann. Anat. Anat. Anz. 1992, 174, 185–195. [Google Scholar] [CrossRef]
- Hammer, N.; Löffler, S.; Feja, C.; Sandrock, M.; Schmidt, W.; Bechmann, I.; Steinke, H. Ethanol-glycerin fixation with thymol conservation: A potential alternative to formaldehyde and phenol embalming. Anat. Sci. Educ. 2012, 5, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Janczyk, P.; Weigner, J.; Luebke-Becker, A.; Kaessmeyer, S.; Plendl, J. Nitrite pickling salt as an alternative to formaldehyde for embalming in veterinary anatomy—A study based on histo-and microbiological analyses. Ann. Anat. Anat. Anz. 2011, 193, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Skog, E. A Toxicologieal Investigation of Lower Aliphatic Aldehydes.: I. Toxicity of Formaldehyde, Acetaldehyde, Propionaldehyde and Butyraldehyde; as well as of Acrolein and Crotonaldehyde. Acta Pharmacol. Toxicol. 1950, 6, 299–318. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Gross, E.; Swenberg, J.; Barrow, C. Nasal cavity deposition, histopathology, and cell proliferation after single or repeated formaldehyde exposures in B6C3F1 mice and F-344 rats. Toxicol. Appl. Pharm. 1983, 68, 161–176. [Google Scholar] [CrossRef]
- Arts, J.H.; de Heer, C.; Woutersen, R.A. Local effects in the respiratory tract: Relevance of subjectively measured irritation for setting occupational exposure limits. Int. Arch. Occup. Environ. Health 2006, 79, 283–298. [Google Scholar] [CrossRef]
- Win-Shwe, T.-T.; Fujimaki, H.; Arashidani, K.; Kunugita, N. Indoor volatile organic compounds and chemical sensitivity reactions. Clin. Dev. Immunol. 2013, 2013, 623812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Formaldehyde. In Selected Pollutants. WHO Guidelines for Indoor Air Quality; WHO, Regional Office for Europe: Copenhagen, Denmark, 2010; pp. 103–156. ISBN 978-92-890-02134. Available online: http://www.euro.who.int/__data/assets/pdf_file/0009/128169/e94535.pdf?ua=1 (accessed on 12 March 2020).
- IARC. International Agency for RC Monographs on the Evaluation of Carcinogenic Risks to Human. Formaldehyde; IARC: Lyon, France, 2012; pp. 401–425. Available online: https://belglas.files.wordpress.com/2016/01/mono100f-29.pdf (accessed on 20 April 2020).
- Zhang, L.; Freeman, L.E.B.; Nakamura, J.; Hecht, S.S.; Vandenberg, J.J.; Smith, M.T.; Sonawane, B.R. Formaldehyde and leukemia: Epidemiology, potential mechanisms, and implications for risk assessment. Environ. Mol. Mutagen. 2010, 51, 181–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, K.; Nishiyama, K.; Yaginuma, H.; Sasaki, A.; Maeda, T.; Kaneko, S.; Onami, T.; Tanaka, M. Formaldehyde exposure levels and exposure control measures during an anatomy dissecting course. J. Anat. 2003, 78, 43–51. [Google Scholar]
- Ohmichi, K.; Komiyama, M.; Matsuno, Y.; Takanashi, Y.; Miyamoto, H.; Kadota, T.; Maekawa, M.; Toyama, Y.; Tatsugi, Y.; Kohno, T. Formaldehyde exposure in a gross anatomy laboratory. Personal exposure level is higher than indoor concentration (5 pp). Environ. Sci. Pollut. Res. 2006, 13, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kim, Y.-D.; Cho, S.-H. Formaldehyde exposure levels and serum antibodies to formaldehyde-human serum albumin of Korean medical students. Arch. Environ. Health 1999, 54, 115–118. [Google Scholar] [CrossRef]
- Chia, S.E.; Ong, C.N.; Foo, S.C.; Lee, H.P. Medical students’ exposure to formaldehyde in a gross anatomy dissection laboratory. J. Am. Coll. Health 1992, 41, 115–119. [Google Scholar] [CrossRef]
- Keil, C.B.; Akbar-Khanzadeh, F.; Konecny, K.A. Characterizing formaldehyde emission rates in a gross anatomy laboratory. Appl. Occup. Environ. Hyg. 2001, 16, 967–972. [Google Scholar] [CrossRef]
- Vohra, M.S. Personal formaldehyde exposure level in the gross anatomy dissecting room at College of Medicine King Saud University Riyadh. Int. J. Occup. Med. Environ. 2011, 24, 108–113. [Google Scholar] [CrossRef]
- Azari, M.R.; Asadi, P.; Jafari, M.J.; Soori, H.; Hosseini, V. Occupational exposure of a medical school staff to formaldehyde in Tehran. Tanaffos 2012, 11, 36–41. [Google Scholar]
- Ochs, S.d.M.; Grotz, L.d.O.; Factorine, L.S.; Rodrigues, M.R.; Netto, A.D.P. Occupational exposure to formaldehyde in an institute of morphology in Brazil: A comparison of area and personal sampling. Environ. Sci. Pollut. Res. 2012, 19, 2813–2819. [Google Scholar] [CrossRef]
- Kunugita, N.; Arahidani, K.; Yamato, H.; Tanaka, I.; Nakashima, T.; Kikuta, A. Evaluation of formaldehyde exposure during a gross anatomy dissection course. In Proceedings of the International Conference on Indoor Air Quality, Ventilation & Energy Conservation in Buildings IAQVEC 2007 II, Sendai, Japan, 28–31 October 2007; pp. 609–616. [Google Scholar]
- Wei, C.; Harada, K.; Ohmori, S.; Wei, Q.; Minamoto, K.; Ueda, A. Subjective symptoms of medical students exposed to formaldehyde during a gross anatomy dissection course. Int. J. Immunopathol. Pharmacol. 2007, 20, 23–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchiyama, S.; Aoyagi, S.; Ando, M. Evaluation of a diffusive sampler for measurement of carbonyl compounds in air. Atmos. Environ. 2004, 38, 6319–6326. [Google Scholar] [CrossRef]
- Uchiyama, S.; Hasegawa, S. A reactive and sensitive diffusion sampler for the determination of aldehydes and ketones in ambient air. Atmos. Environ. 1999, 33, 1352–2310. [Google Scholar] [CrossRef]
- Aung, W.-Y.; Noguchi, M.; Yi, E.-E.P.-N.; Thant, Z.; Uchiyama, S.; Win-Shwe, T.-T.; Kunugita, N.; Mar, O. Preliminary assessment of outdoor and indoor air quality in Yangon city, Myanmar. Atmos. Pollut. Res. 2019, 10, 722–730. [Google Scholar] [CrossRef]
- JSOH. Recommendation of occupaitonal exposure limits (2018–2019). J. Occup. Health 2018, 60, 419–452. [Google Scholar] [CrossRef]
- ACGIH. Ameican Conference of Governmental Industrial Hygienists: Threshold Limit Values (TLVs) and Biological Exposure Indices (BEIs). Appendix B 2012, 874–1130. Available online: http://www.acgih.org/TLV/ (accessed on 22 February 2020).
- Sugata, Y.; Miyaso, H.; Odaka, Y.; Komiyama, M.; Sakamoto, N.; Mori, C.; Matsuno, Y. Levels of formaldehyde vapor released from embalmed cadavers in each dissection stage. Environ. Sci. Pollut. Res. 2016, 23, 16176–16182. [Google Scholar] [CrossRef] [Green Version]
- MHLW. The Ministry of Health Labour and Welfare, Theguideline Value of Indoor Formaldehyde Concen-Tration Report of Chemical Substances Small Com-Mittee, Specialty Section Toestablish Standards Forhealth Residences. 1997. Available online: http://www1.mhlw.go.jp/houdou/1206/h0629-213.html (accessed on 1 February 2020).
- Lakchayapakorn, K.; Watchalayarn, P. Formaldehyde exposure of medical students and instructors and clinical symptoms during gross anatomy laboratory in Thammasat University. J. Med. Assoc. Thail. 2010, 93, S92–S98. [Google Scholar]
- Gahukar, S.; Ramteke, U.; Majumdar, D.; Malviya, R.; Patil, D.; Trivedi, J.; Rao, C.; Kale, A.H. Prevalence of formaldehyde in indoor air of gross anatomy laboratory and cadaver storage room of a medical college. J. Environ. Occup. Sci. 2014, 3, 181–185. [Google Scholar] [CrossRef] [Green Version]
- Pfeil, S.; Hieke, H.; Brohmann, P.; Wimmer, M. Low cost and effective reduction of formaldehyde in gross anatomy: Long throw nozzles and formaldehyde destruction using InfuTrace™. Environ. Sci. Pollut. Res. 2020, 27, 45189–45208. [Google Scholar] [CrossRef]
- Homwutthiwong, K.; Ongwandee, M. Investigation of Formaldehyde in Gross Anatomy Laboratory: Area-Based and Exposure Levels, Ventilation, Health Risk and Clinical Symptoms. AER 2017, 39, 77–90. [Google Scholar] [CrossRef]
- Takayanagi, M.; Sakai, M.; Ishikawa, Y.; Murakami, K.; Kimura, A.; Kakuta, S.; Sato, F. Formaldehyde concentrations in the breathing zone of medical students during gross anatomy laboratory in Toho University. J. Anat. 2007, 82, 45–51. [Google Scholar]
- OSHA. Occupational Safety and Health Adminstration: Formaldehyde (29 CFR 1910.1048). 2011. Available online: https://www.osha.gov/OshDoc/data_General_Facts/formaldehyde-factsheet.html (accessed on 12 February 2020).
- Guideliness for Good Indoor Air Quality in Office Premises; Singapore Ministry of Environment, Institute of Envrionmental Epidemiology: Singapore, 1996. Available online: https://www.bca.gov.sg/greenmark/others/NEA_Office_IAQ_Guidelines.pdf (accessed on 24 March 2020).
- Jeong, J.Y.; Lee, B.K.; Phee, Y.G. Assessment of indoor air quality in commercial office buildings. J. Korean Soc. Occup. Environ. Hyg. 2007, 17, 31–42. [Google Scholar]
- El Okda, E.; Abd Elaziz, K.; Samaha, H. Comparative study of risk assessment of formaldehyde exposure among students in public and private Faculties of Medicine in Egypt. Egypt J. Occup. Med. 2009, 33, 143–154. [Google Scholar]
- Khouri, N.A. Management of chemical health hazard fumes emitted during and after embalming procedure and its impact on medical students and embalmers. CER 2012, 2, 32–41. [Google Scholar]
- Onyije, F.; Avwioro, O. Excruciating effect of formaldehyde exposure to students in gross anatomy dissection laboratory. Int. J. Occup. Environ. Med. 2012, 3, 92–95. [Google Scholar]
- Elshaer, N.S.M.; Mahmoud, M.A.E. Toxic effects of formalin-treated cadaver on medical students, staff members, and workers in the Alexandria Faculty of Medicine. Alex. J. Med. 2017, 53, 337–343. [Google Scholar] [CrossRef]
- de Lucena, J.D.; da Silveira, H.F.; de Paula, L.S.; Junior, H.L.R.; da Costa Sobrinho, O.O.P.; Leal, K.M.B.; Veríssimo, N.A.; Pessoa, R.S.; Scafuri, A.G.; Barreto, J.E.F. The Irritating Effects of Exposure to Formaldehyde in User Students of the Human Anatomy Laboratory. Int. Arch. Med. 2017, 10, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Ya’acob, S.H.; Suis, A.J.; Awang, N.; Sahani, M. Exposure assessment of formaldehyde and its symptoms among anatomy laboratory workers and medical students. Asian J. Appl. Sci. 2013, 6, 50–55. [Google Scholar] [CrossRef] [Green Version]
- Ikuharu, M.; Emiko, H.; Chizuko, S.; Sachiyo, T.; Toshio, K.; Yasuto, T. Formaldehyde concentrations in breathing zone in an anatomy laboratory. Part 2. Effect of deodorization agent and mask. J. Wakayama Med. Soc. 2003, 54, 121–132. [Google Scholar]
- Alnagar, F.A.; Shmela, M.E.; Alrtib, A.M.; Benashour, F.M.; Buker, A.O.; Abdalmula, A.M. Health adverse effects of formaldehyde exposure to students and staff in gross anatomy. IJSRM 2018, 6, 27–36. [Google Scholar] [CrossRef] [Green Version]
- Raja, D.S.; Sultana, B. Potential health hazards for students exposed to formaldehyde in the gross anatomy laboratory. Environ. Health 2012, 74, 36–41. [Google Scholar]
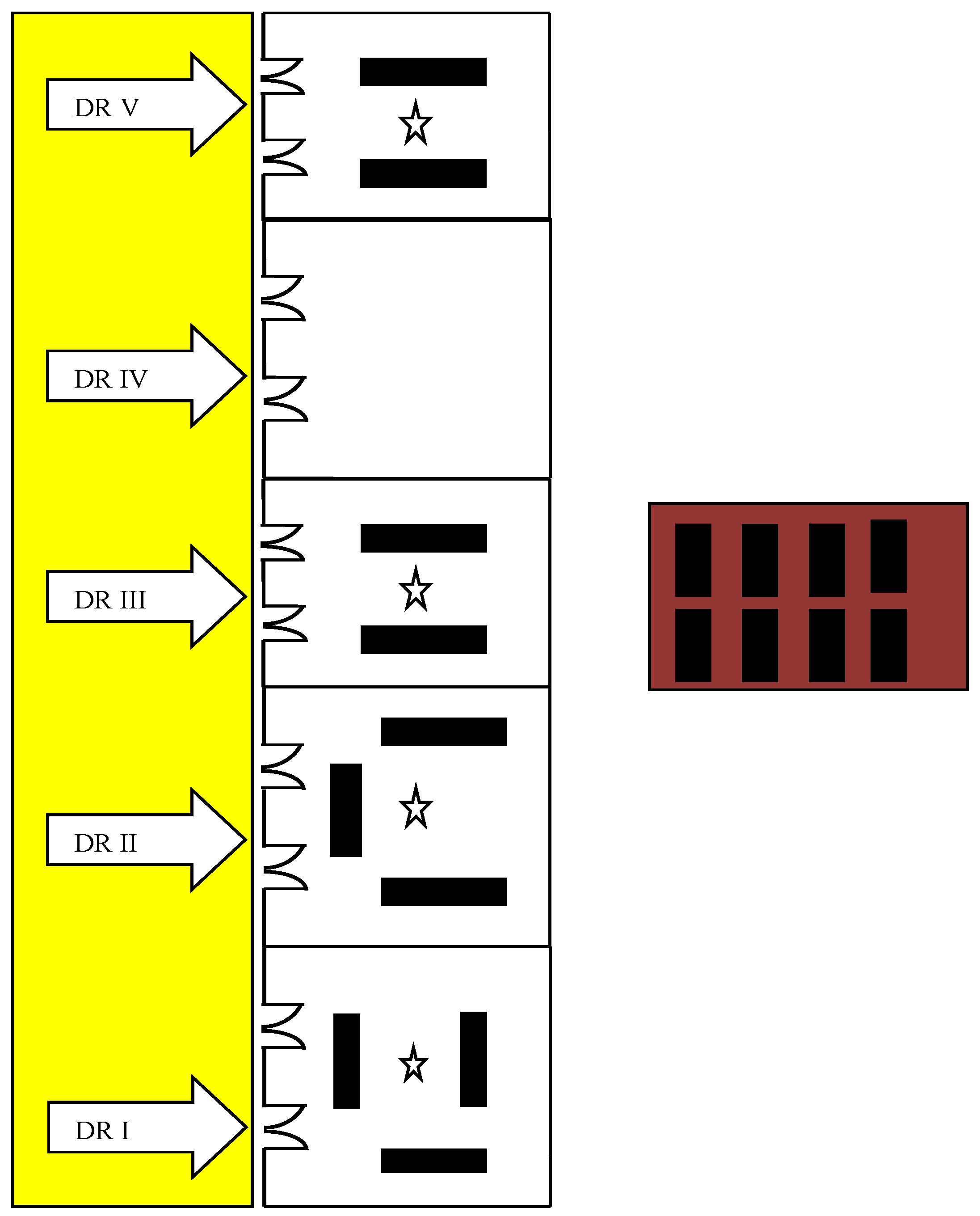
 Corridor,
Corridor,  Cadaver storage room,
Cadaver storage room,  Door (DR, dissection room),
Door (DR, dissection room),  Cadaver, and
Cadaver, and  Diffusive air sampler).
Corridor, Cadaver storage room, Door (DR, dissection room), Cadaver, and Diffusive air sampler).
Diffusive air sampler).
Corridor, Cadaver storage room, Door (DR, dissection room), Cadaver, and Diffusive air sampler).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | DR(I) | DR(II) | DR(III) | DR(V) | LT |
|---|---|---|---|---|---|
| 1188 | 1188 | 924 | 924 | 1597 |
| Wall-mounted Fans | Wall-mounted Fans | Wall-mounted Fans | Wall-mounted Fans | Air conditioning |
| 3 | 3 | 2 | 2 | Nil |
| 27–28 | 27–28 | 27–28 | 27–28 | 22–24 |
| 70–85 | 70–85 | 70–85 | 70–85 | 50–65 |
| Authors and Year | Dimension (m3) | Type of Ventilation | Cadaver Number | Indoor FA Concentrations (ppm) |
|---|---|---|---|---|
| 1125 | 12 supply diffuser, 4 air conditioning, 8 air return grills | not mention | 0.23–1.03 |
| 1800 | Central air conditioning system, 4 exhaust fans | 14 | 0.68 (Week 4) 0.85 (Week 10) 0.73 (Week 14) |
| 1400 |
| 25 | 0.76 |
| 0.61 | |||
| 0.05 | |||
| 339 |
| 0.57 | |
| 0.27 | |||
| 0.25 | |||
| 1386 | Natural ventilation system | 16 | |
| 380 | 4 large stand fans | 14 | 0.09–0.176 |
| 11,188 (DRs I, II) | 10 wall fans | 3 (DRs I, II) | DR I, 0.61 DR II, 0.37 |
| 9942 (DRs III, V) | 2 (DRs III, V) | DR III, 0.32 DR V, 0.29 |
| Authors and Year | Country | Concentration of FA (ppm) Min-Max or Average (Min-Max) | |
|---|---|---|---|
| Indoor Concentration | Personal Exposure | ||
| Japan | 0.24–1.05 | 0.46–1.1 |
| Saudi Arabia | 4th week (Upper limb) | 1.27 (0.82–1.72) I |
| 0.68 (0.53–0.80) | 0.75 (0.62–0.89) S | ||
| 10th week (Abdomen) | 1.44 (1.18–1.70) I | ||
| 0.85 (0.64–1.29) | 1.20 (0.98–1.42) S | ||
| 14th week (Head, Neck) | 1.33 (0.94–1.72) I | ||
| 0.73 (0.65–0.93) | 1.10 (0.88–1.31) S | ||
| Brazil | 0.15–1.89 | 0.41–2.80 |
| Thailand | 0.49 (0.40–0.58) | 0.66 (0.47–0.85) |
| Myanmar | 0.43 (0.09–1.22) | 0.68 (0.04–2.11) I 0.44 (0.06–1.72) S |
| Clinical Symptoms | Number of Students Who Reported Symptoms (%) | Odd Ratio (95% CI) | |
|---|---|---|---|
| In Dissection Room | In Lecture Theater | ||
| 82 (78.8%) | 5 (4.8%) | 39.4 (17.2–90.2) *** |
| 50 (48.1%) | 10 (9.6%) | 22.3 (7.6–65.0) *** |
| 38 (36.5%) | 3 (2.9%) | 19.3 (5.7–65.4) *** |
| 37(35.5%) | 10 (9.6%) | 5.2 (2.4–11.2) *** |
| 26 (25.0%) | 5 (4.8%) | 5.4 (2.1–13.9) *** |
| 18 (17.3%) | 3 (2.9%) | 7.0 (2.0–24.7) ** |
| 18 (17.3%) | 4 (3.8%) | 4.2 (1.3–13.2) ** |
| 15 (14.4%) | 6 (5.8%) | 2.8 (1.0–7.4) * |
| 14 (13.5%) | 5 (4.8%) | 3.1 (1.1–8.9) * |
| 11 (10.6%) | 3 (2.9%) | 3.9 (1.1–14.7) * |
| Regular Use of PPE | Percentage of Respondents (n = 104) |
|---|---|
| 96% |
| 91% |
| 45% |
| 0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aung, W.-Y.; Sakamoto, H.; Sato, A.; Yi, E.-E.-P.-N.; Thein, Z.-L.; Nwe, M.-S.; Shein, N.; Linn, H.; Uchiyama, S.; Kunugita, N.; et al. Indoor Formaldehyde Concentration, Personal Formaldehyde Exposure and Clinical Symptoms during Anatomy Dissection Sessions, University of Medicine 1, Yangon. Int. J. Environ. Res. Public Health 2021, 18, 712. https://doi.org/10.3390/ijerph18020712
Aung W-Y, Sakamoto H, Sato A, Yi E-E-P-N, Thein Z-L, Nwe M-S, Shein N, Linn H, Uchiyama S, Kunugita N, et al. Indoor Formaldehyde Concentration, Personal Formaldehyde Exposure and Clinical Symptoms during Anatomy Dissection Sessions, University of Medicine 1, Yangon. International Journal of Environmental Research and Public Health. 2021; 18(2):712. https://doi.org/10.3390/ijerph18020712
Chicago/Turabian StyleAung, Win-Yu, Hironari Sakamoto, Ayana Sato, Ei-Ei-Pan-Nu Yi, Zaw-Lin Thein, Myint-San Nwe, Nanda Shein, Htin Linn, Shigehisa Uchiyama, Naoki Kunugita, and et al. 2021. "Indoor Formaldehyde Concentration, Personal Formaldehyde Exposure and Clinical Symptoms during Anatomy Dissection Sessions, University of Medicine 1, Yangon" International Journal of Environmental Research and Public Health 18, no. 2: 712. https://doi.org/10.3390/ijerph18020712