Applying Lean in Process Innovation in Healthcare: The Case of Hip Fracture

 ,
,
Abstract
:1. Introduction
- RQ1.
- → What types of waste or muda could be identified around a hip fracture surgery process?
- RQ2.
- → How a process innovation methodology using Lean techniques is applied in healthcare, in particular in a hip fracture surgery processes?
2. Theoretical Framework
3. Methodology
4. Case Study: Hip Fracture Surgery Description
5. Applying Lean in Process Innovation in Hip Fracture: Results
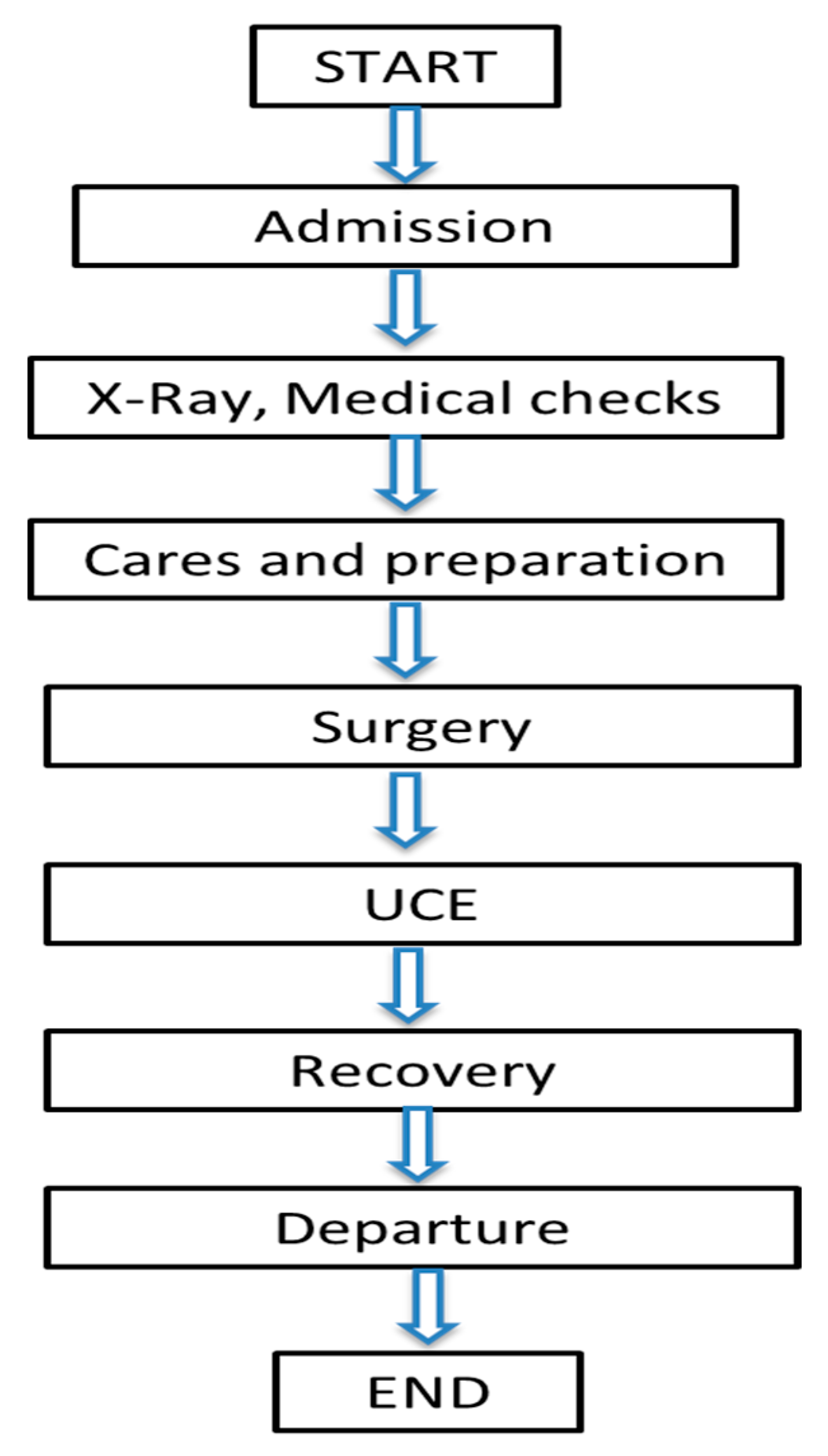
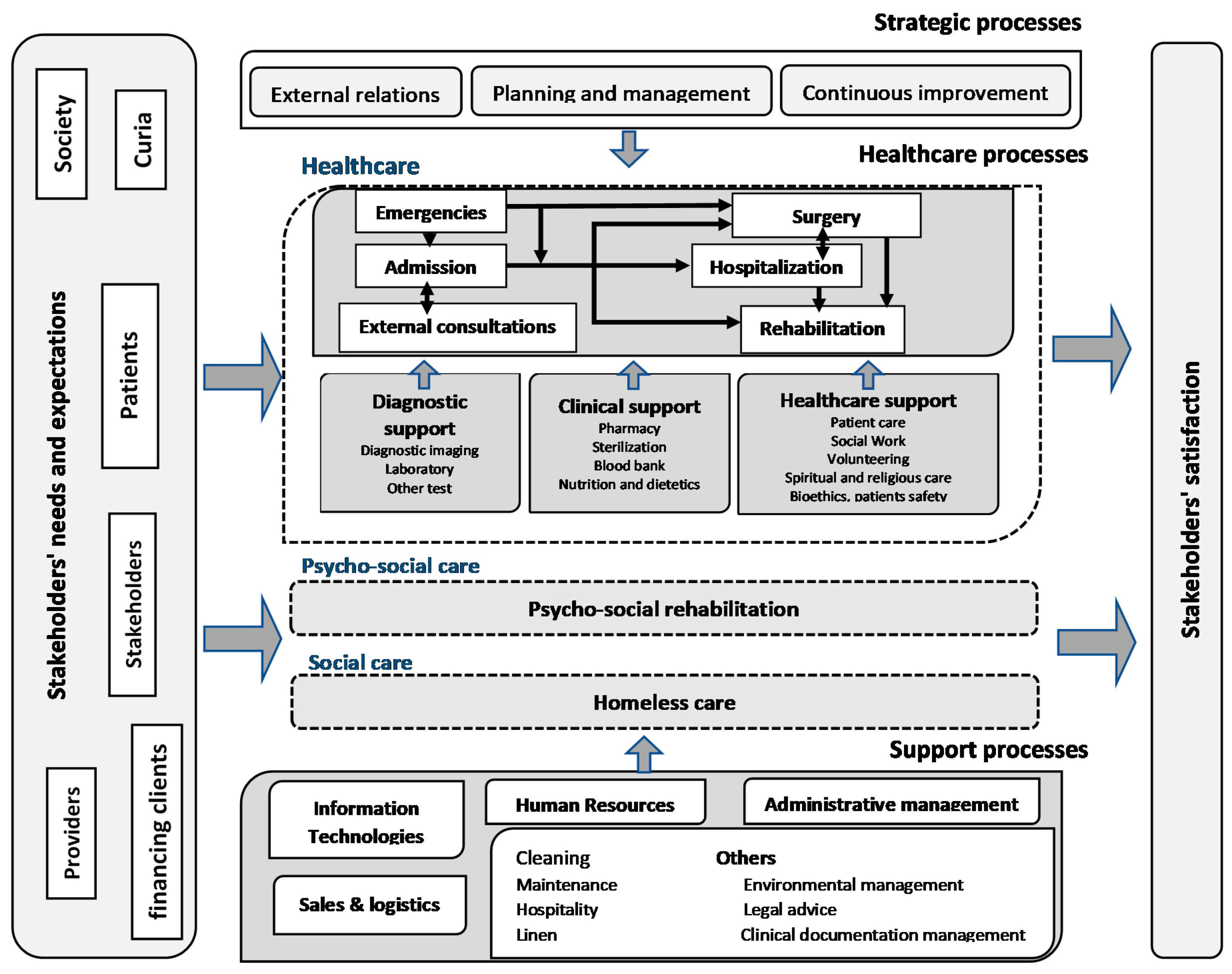
5.1. Process Selection and Understanding the Process
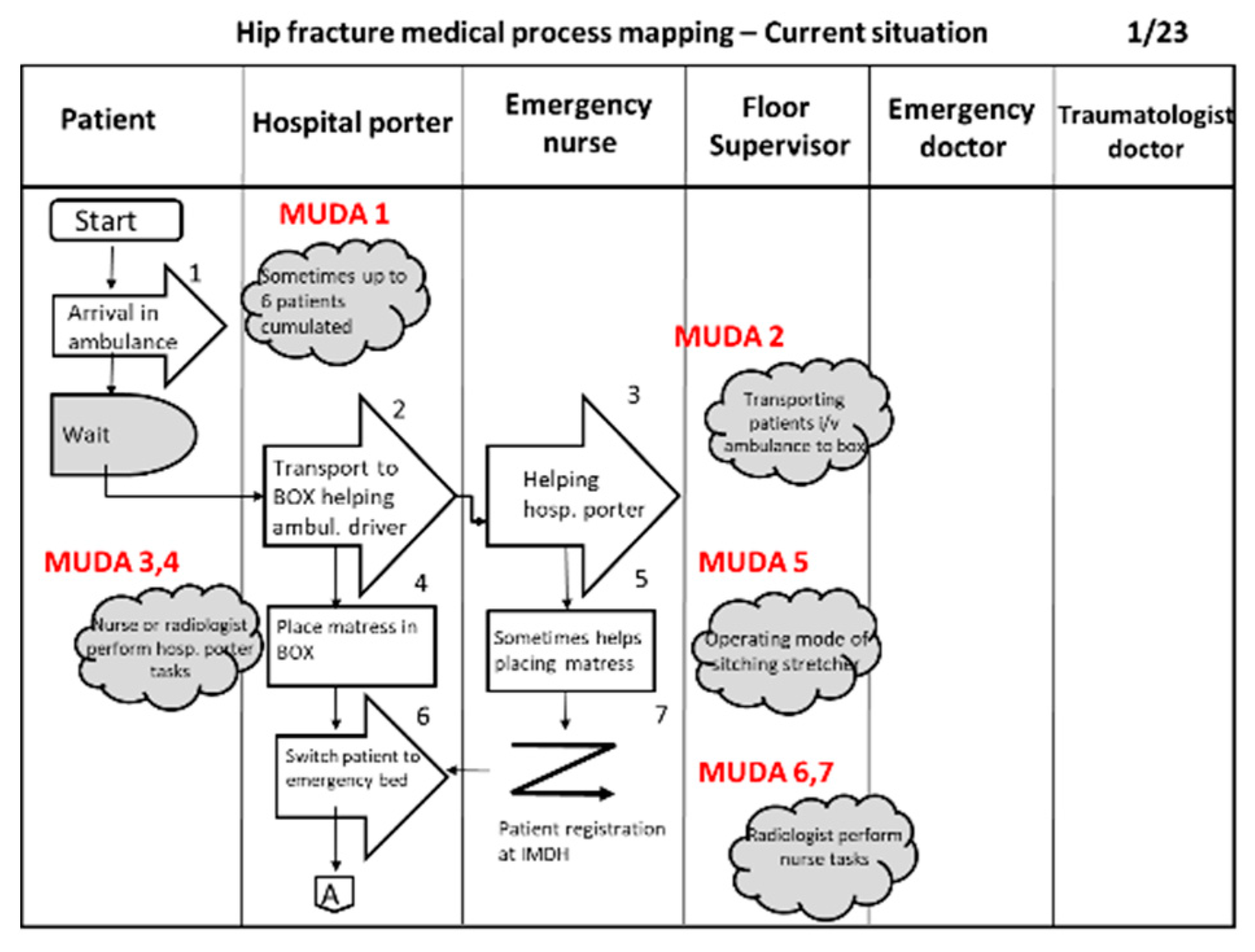
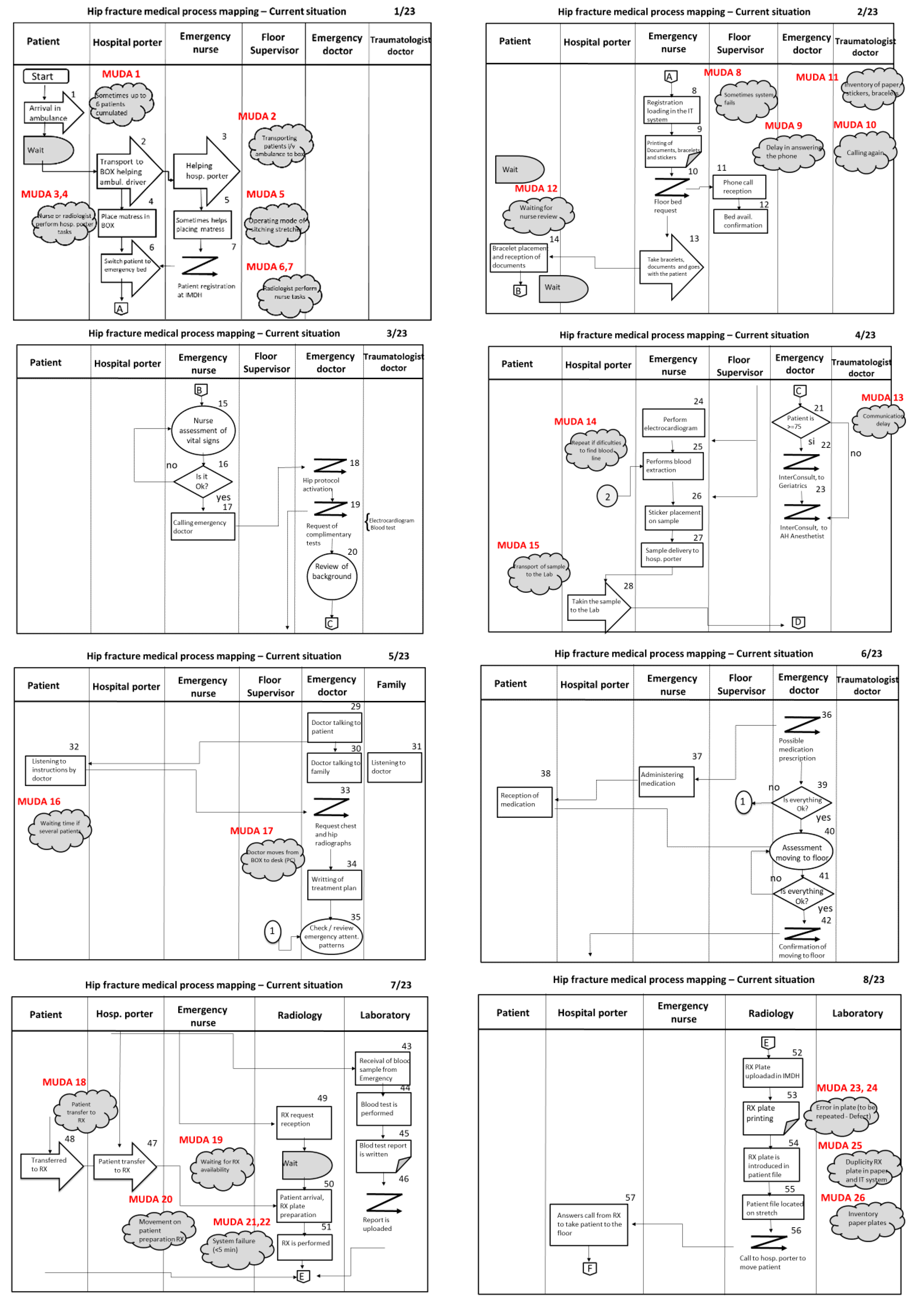
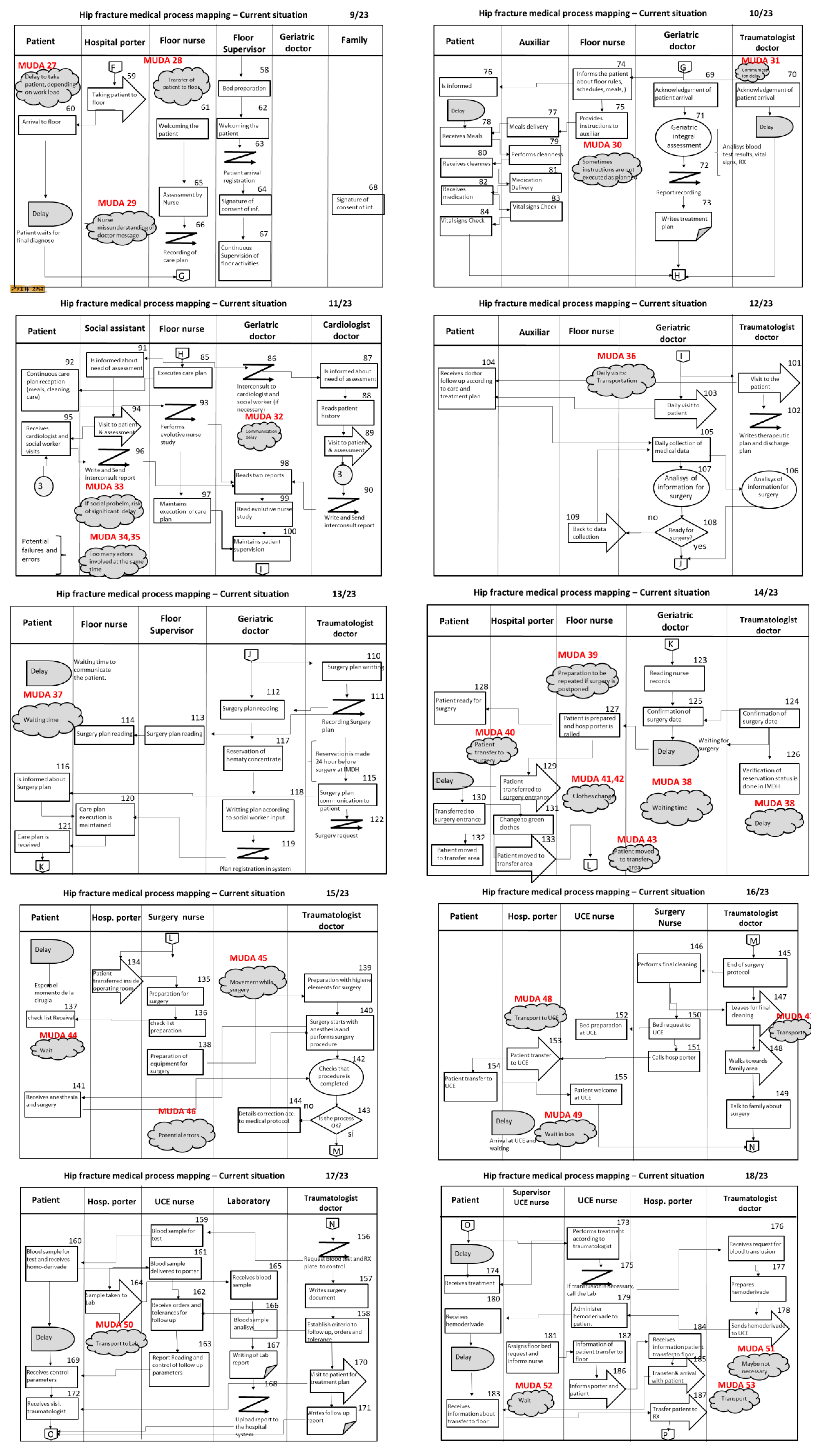
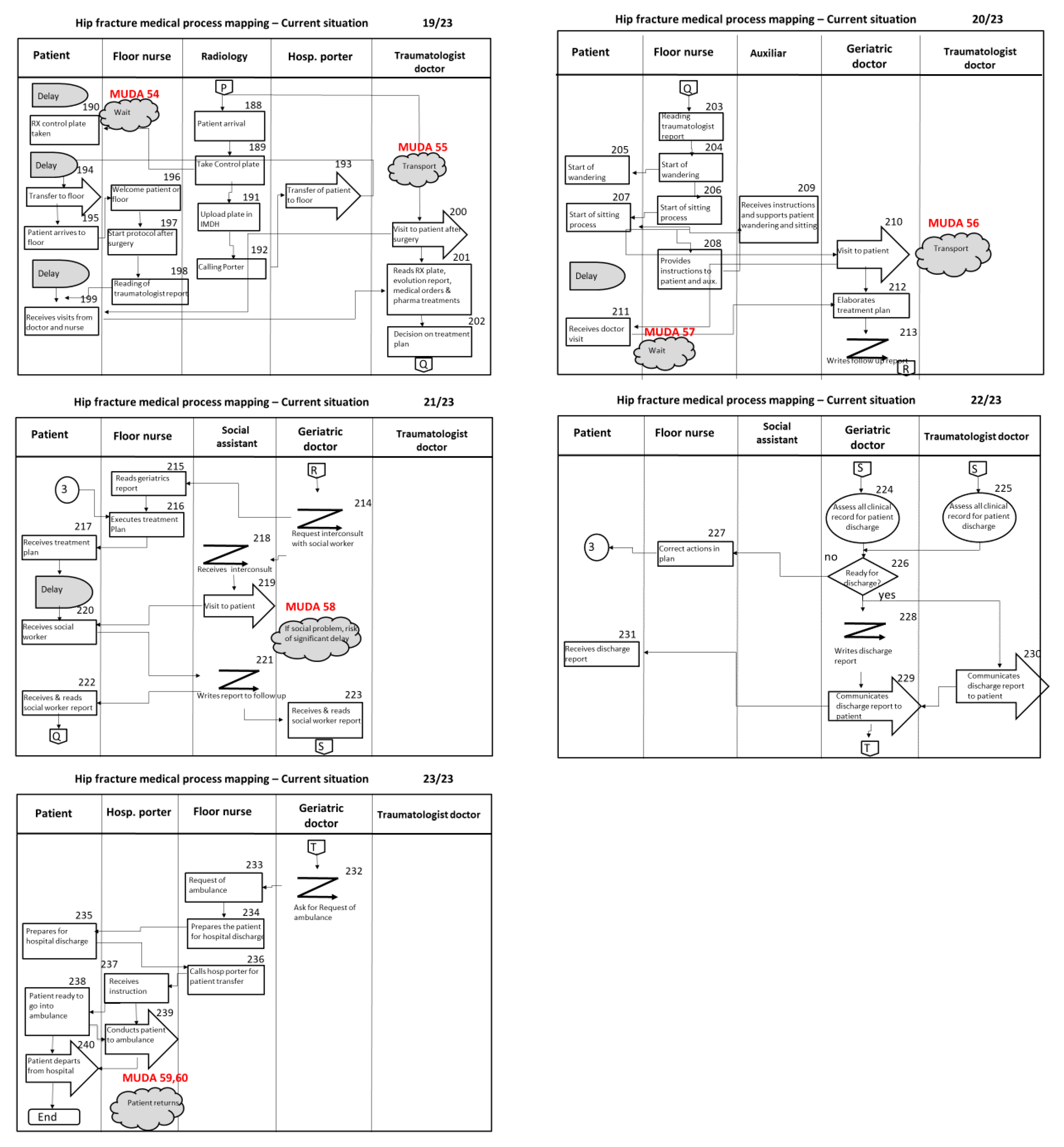
5.2. Mapping the Process
5.3. Process Measurements
- (i)
- Number of activities in the process. The number of activities is a relevant metric, as it is a measure of the complexity of the process. Each activity in the process has been identified and numbered.The total number of activities resulted in 236.
- (ii)
- Number of participants. The number of participants is also a relevant metric, as a high number shows a more complicated process, as the number of interactions between them is higher, so there is a higher opportunity or risk of miscommunication, misunderstanding, delays, and potential errors. We understand the “number of participants” as the number of different jobs or profiles of employees, but the real number of employees intervening in the process is much higher. For instance, “nurse” is considered one participant, but in reality, we can find different persons working as nurses involved in the different activities of the process (same for doctors, assistants, technicians, etc.)The number of participants is 18 (*).They are grouped in different areas (see detail in Table 2).
- (iii)
- Process cycle times. This refers to the total process time, from patient arrival at the hospital to the moment that the patient is discharged and leaves the hospital (also known as total hospitalization times or LOS). Total process cycle times in 2020 are reported above in the case study description, the average being 9.41 days (40.97% less than 2019 data), the median being 9 days, the standard deviation being 4.17, the minimum being 0 days, and the maximum value being 32 days.
5.4. Process Analysis
- (i)
- First, the process is analyzed in detail, identifying the different types of activities within the process. The following Table 3 provides this information:
- (ii)
- Second, the process is analyzed with the aim of identifying the different types of muda all along the different stages. According to the literature, the following types of muda can be found in a process:
- Defects: errors or defects when performing a task, producing a service or making a product.
- Overprocessing: repeating tasks or activities during the process.
- Overproduction: producing more than necessary.
- Movement: unnecessary or inadequate movement of personnel to execute a task (related to ergonomics or efficiency of movements).
- Transportation: carrying out or moving materials or patients from one location to a different location where a new task will be performed. This also refers to the transportation of employees.
- Inventory: excess of materials or goods which are cumulated in case they are needed.
- Delay: additional waiting time when the process stops more than usual.
- Unused Talent: underused qualified workers (it could also be—but not in this case—a bad attitude from employees affecting the process results).
5.5. Process Redesign
6. Discussion
7. Conclusions
- (i)
- the identification of all different types of muda all along the hip fracture surgery process provides hospital managers with an opportunity for continuous improvement, by trying to eliminate or minimize them;
- (ii)
- some initiatives have been proposed to redesign the process, which allows the management to take action towards gaining efficiency and service quality, which in turn impacts on operating costs and patient satisfaction;
- (iii)
- the observation and the analysis have been carried out by researchers, but a basic training and a checklist (an audit tool) would help employees to carry out this assessment any time they need in the future.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B



Appendix C

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Muda # | Process Activity # | Direct Observation | Type of Muda |
|---|---|---|---|
| 1 | 1 | Ambulance arrival. Patient cumulation (sometimes up to 6 patients) | Delay |
| 2 | 3 | Transportation of patients from ambulance to emergency box | Transportation |
| 3, 4 | 4 | MRI technician or nurse working as a hospital porter if required | Unused Talent Overprocessing |
| 5 | 5 | Handling patients from an ambulance stretcher to a hospital stretcher and placing mattress | Movement |
| 6, 7 | 7 | MRI technician working as a nurse if required to register patients | Unused Talent Overprocessing |
| 8 | 8 | Registration activities to be redone when IMDH systems fail | Overprocessing |
| 9 | 11 | Waiting time while phone is answered | Delay |
| 10 | 12 | Phone calls to be repeated until somebody answers | Overprocessing |
| 11 | 9 | Excessive or potential lack of inventory of paper, labels, or bracelets | Inventory |
| 12 | 14 | Waiting for a nurse check | Delay |
| 13 | 21 | Communication delay | Delay |
| 14 | 25 | Blood extraction preparation to be repeated in the case of difficulties | Overprocessing |
| 15 | 28 | Transportation of blood sample | Transportation |
| 16 | 32 | Waiting time if several patients are in the emergency area | Delay |
| 17 | 34 | Unnecessary doctor movement between box (patient) and desk (PC) | Movement |
| 18 | 48 | Transportation of patients from emergency box to X-Ray | Transportation |
| 19 | 47 | Waiting times upon X-Ray availability | Delay |
| 20 | 50 | Handling of patients for X-Ray preparation | Movement |
| 21, 22 | 51 | System error provoking delay (up to 5 min) and repeating operations | Delay, Overprocessing |
| 23 | 53 | Defective X-Ray | Defect |
| 24 | 53 | Repeated defective X-Ray | Overprocessing |
| 25 | 54 | Duplicity X-Ray in computer and in paper | Overproduction |
| 26 | 55 | Inventory of paper X-Ray plates | Inventory |
| 27 | 59 | Waiting times to take patient to room | Delay |
| 28 | 60 | Transportation of patients from X-Ray to room | Transportation |
| 29 | 65 | Error in understanding doctor’s orders | Defect |
| 30 | 79 | Deviations from original message given to patients | Defect |
| 31 | 70 | Communication delay | Delay |
| 32 | 86 | Communication delay | Delay |
| 33 | 96 | If social issue, high risk of huge delays | Delay |
| 34, 35 | 85–100 | Many actors, potential failures and errors | Defect, Overprocessing |
| 36 | 101 | Daily visits to patients | Transportation |
| 37 | 114 | Waiting for a decision | Delay |
| 38 | 126 | Waiting for transportation to surgery area | Delay |
| 39 | 127 | If surgery is delayed or postponed, patient preparation must be redone | Overprocessing |
| 40 | 129 | Transportation of patients to surgery level | Transportation |
| 41, 42 | 131 | Clothes changing | Movement, Delay |
| 43 | 133 | Transportation of patient to surgery transfer area | Transportation |
| 44 | 137 | Waiting for surgery | Delay |
| 45 | 135–143 | Movement and preparation before and during surgery | Movement |
| 46 | 143 | Potential errors during surgery | Defects |
| 47 | 147 | Doctor transportation for cleaning and talking to the patient family | Transportation |
| 48 | 153 | Transportation of patient to UCE | Transportation |
| 49 | 155 | Waiting time if busy area | Delay |
| 50 | 164 | Transportation of blood sample to Laboratory | Transportation |
| 51 | 178 | Homoderivative might not be necessary | Overproduction |
| 52 | 183 | Delay | Delay |
| 53 | 187 | Transportation of patient to X-Ray | Transportation |
| 54 | 190 | Delay | Delay |
| 55 | 193 | Transportation of patient to room | Transportation |
| 56 | 210 | Daily visits to patients | Transportation |
| 57 | 211 | Delay | Delay |
| 58 | 218–221 | If social issue, high risk of huge delays | Delay |
| 59, 60 | 240 | Patient returns sooner than expected due to a recovery issue | Defect; Overprocessing |
References
- Henriksen, K.; Dayton, E.; Keyes, M.A.; Carayon, P.; Hughes, R. Understanding Adverse Events: A Human Factors Framework. In Patient Safety and Quality: An Evidence-Based Handbook for Nurses; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2008. [Google Scholar]
- Vincent, C. Understanding and Responding to Adverse Events. N. Engl. J. Med. 2003, 348, 1051–1056. [Google Scholar] [CrossRef] [Green Version]
- Porter, M.E. What Is Value in Health Care? N. Engl. J. Med. 2010, 363, 2477–2481. [Google Scholar] [CrossRef] [PubMed]
- Reason, J. Understanding adverse events: Human factors. Qual. Saf. Health Care 1995, 4, 80–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giraldo, P.; Sato, L.; Martínez-Sánchez, J.M.; Comas, M.; Dwyer, K.; Sala, M.; Castells, X. Eleven-year descriptive analysis of closed court verdicts on medical errors in Spain and Massachusetts. BMJ Open 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Hamelmann, C.; Turatto, F.; Then, V.; Dyakova, M. Social Return on Investment: Accounting for Value in the Context of Implementing Health 2020 and the 2030 Agenda for Sustainable Development; WHO Regional Office for Europe: Copenhagen, Denmark, 2017. [Google Scholar]
- Woodnutt, S. Is Lean sustainable in today’s NHS hospitals? A systematic literature review using the meta-narrative and integrative methods. Int. J. Qual. Health Care 2018, 30, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Womack, J.P.; Jones, D.T.; Roos, D. The Machine That Changed the World; Harper Collins Publishers: New York, NY, USA, 1990. [Google Scholar]
- Ohno, T. The Toyota Production System; Productivity Press: Portland, OR, USA, 1988. [Google Scholar]
- Monden, Y. The Toyota Management System; Productivity Press: Portland, OR, USA, 1993. [Google Scholar]
- Womack, J.P.; Jones, D.T. Lean Thinking: Banish Waste and Create Wealth in Your Corporation; Simon & Schuster: New York, NY, USA, 1996. [Google Scholar]
- Agrawal, N. Review on Just in Time Techniques in Manufacturing Systems. Adv. Prod. Eng. Manag. 2010, 5, 101–110. [Google Scholar]
- Allway, M.; Corbett, S. Shifting to lean service: Stealing a page from manufacturers’ playbooks. J. Organ. Excel. 2002, 21, 45–54. [Google Scholar] [CrossRef]
- George, M.L. Lean Six Sigma for Service: How to Use Lean Speed and Six Sigma Quality to Improve Services and Transactions; McGraw-Hill: New York, NY, USA, 2003. [Google Scholar]
- Makary, M.; Daniel, M. Medical error—The third leading cause of death in the US. BMJ 2016, 353, i2139. [Google Scholar] [CrossRef]
- De Koning, H.; Verver, J.P.S.; Heuvel, J.V.D.; Bisgaard, S.; Does, R.J.M.M. Lean Six Sigma in Healthcare. J. Health Qual. 2006, 28, 4–11. [Google Scholar] [CrossRef]
- De Souza, L.B. Trends and approaches in lean healthcare. Leadersh. Health Serv. 2009, 22, 121–139. [Google Scholar] [CrossRef]
- Waring, J.; Bishop, S. Lean healthcare: Rhetoric, ritual and resistance. Soc. Sci. Med. 2010, 71, 1332–1340. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.; Radnor, Z.J.; Burgess, N.; Worthington, C. SimLean: Utilising simulation in the implementation of lean in healthcare. Eur. J. Oper. Res. 2012, 219, 188–197. [Google Scholar] [CrossRef] [Green Version]
- Drotz, E.; Poksinska, B. Lean in healthcare from employees’ perspectives. J. Health Organ. Manag. 2014, 28, 177–195. [Google Scholar] [CrossRef] [PubMed]
- Tlapa, D.; Zepeda-Lugo, C.A.; Tortorella, G.L.; Baez-Lopez, Y.A.; Limon-Romero, J.; Alvarado-Iniesta, A.; Rodriguez-Borbon, M.I. Effects of Lean Healthcare on Patient Flow: A Systematic Review. Value Health 2020, 23, 260–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aleu, F.G.; Van Aken, E.; Cross, J.; Glover, W. Continuous improvement project within Kaizen: Critical success factors in hospitals. TQM J. 2018, 30, 335–355. [Google Scholar] [CrossRef]
- Altas, Estancia Media en Días y Coste Medio en Euros de los Procesos Obstétricos y Quirúrgicos Más Frecuentes. Hospitales de agudos SNS. In Registro de Atención Especializada—RAE-CMBD; Ministerio de Sanidad, Consumo y Bienestar Social, Roma, Italy; 2017. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/docs/CMBD/INFORME_COSTES_PROCESOS_OBSTETRICOS_HOSPITALES_SNS_2017.pdf (accessed on 5 June 2018).
- Bateman, L.; Vuppala, S.; Porada, P.; Carter, W.; Baijnath, C.; Burman, K.; Lee, R.; Hargus, J. Medical Management in the Acute Hip Fracture Patient: A Comprehensive Review for the Internist. Ochsner J. 2012, 12, 101–110. [Google Scholar]
- Mazzocato, P.; Stenfors, T.; Schwarz, U.V.T.; Hasson, H.; Nyström, M.E. Kaizen practice in healthcare: A qualitative analysis of hospital employees’ suggestions for improvement. BMJ Open 2016, 6, e012256. [Google Scholar] [CrossRef] [Green Version]
- Marottoli, R.A.; Berkman, L.F.; Leo-Summers, L.; Cooney, L.M. Predictors of mortality and institutionalization after hip fracture: The New Haven EPESE cohort. Established Populations for Epidemiologic Studies of the Elderly. Am. J. Public Health 1994, 84, 1807–1812. [Google Scholar] [CrossRef] [Green Version]
- Wilson, R.T.; Chase, G.A.; Chrischilles, E.A.; Wallace, R.B. Hip Fracture Risk Among Community-Dwelling Elderly People in the United States: A Prospective Study of Physical, Cognitive, and Socioeconomic Indicators. Am. J. Public Health 2006, 96, 1210–1218. [Google Scholar] [CrossRef]
- Bai, J.; Zhang, P.; Liang, X.; Wu, Z.; Wang, J.; Liang, Y. Association between dementia and mortality in the elderly patients undergoing hip fracture surgery: A meta-analysis. J. Orthop. Surg. Res. 2018, 13, 298. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, M.P. Aging Bone and Osteoporosis: Strategies for preventing fractures in the elderly. Arch. Intern. Med. 2003, 163, 2237–2246. [Google Scholar] [CrossRef] [PubMed]
- Svedbom, A.; Hernlund, E.; Ivergard, M.; Compston, J.; Cooper, C.; Stenmark, J.; McCloskey, E.V.; Jönsson, B.; Kanis, J.A. Osteoporosis in the European Union: A compendium of country-specific reports. Arch. Osteoporos. 2013, 8, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, J.N.; Klein, D.S.; Sreekumar, S.; Liporace, F.A.; Yoon, R.S. Outcomes in Multidisciplinary Team-based Approach in Geriatric Hip Fracture Care: A Systematic Review. J. Am. Acad. Orthop. Surg. 2020, 28, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.Y.; Yan, S.; Low, L.L.; Vasanwala, F.F.; Low, S.G. Predictors of poor functional outcomes and mortality in patients with hip fracture: A systematic review. BMC Musculoskelet. Disord. 2019, 20, 568. [Google Scholar] [CrossRef]
- Veronese, N.; Maggi, S. Epidemiology and social costs of hip fracture. Injury 2018, 49, 1458–1460. [Google Scholar] [CrossRef]
- Monte-Secades, R.; Codesido-Vilar, P.; Pardo-Sobrino, F.; García-Monasterio, E.; Portero-Vázquez, A.; Garcia-Novio, M.; Lamelo, F.F. Vía clínica para pacientes hospitalizados con fractura osteoporótica de cadera. Galicia Clin. 2016, 77, 57–66. [Google Scholar]
- Informe Anual RNFC 2018. Available online: http://rnfc.es/wp-content/uploads/2019/11/Informe-Anual-RNFC-2018.pdf (accessed on 25 August 2019).
- Bradeanu, A.V.; Ciubara, A.B.; Burlea, S.L.; Ciubara, A. The Socio-Economic Impact Produced by Patients with Dementia and Hip Fractures. Brain Broad Res. Artif. Intell. Neurosci. 2020, 11. Available online: https://lumenpublishing.com/journals/index.php/brain/article/view/2844 (accessed on 14 April 2020).
- Salkeld, G.; Cameron, I.D.; Cumming, R.G.; Easter, S.; Seymour, J.; Kurrle, S.E.; Quine, S. Quality of life related to fear of falling and hip fracture in older women: A time trade off study. BMJ 2000, 320, 341–346. [Google Scholar] [CrossRef] [Green Version]
- Laing, C.M.; Moules, N.J. Social Return on Investment: A New Approach to Understanding and Advocating for Value in Healthcare. J. Nurs. Adm. 2017, 47, 623–628. [Google Scholar] [CrossRef]
- Simons, P.A.; Backes, H.; Bergs, J.; Emans, D.; Johannesma, M.; Jacobs, M.; Marneffe, W.; Vandijck, D. The effects of a lean transition on process times, patients and employees. Int. J. Health Care Qual. Assur. 2017, 30, 103–118. [Google Scholar] [CrossRef] [PubMed]
- Coulter, A.; Locock, L.; Ziebland, S.; Calabrese, J. Collecting data on patient experience is not enough: They must be used to improve care. BMJ 2014, 348, g2225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heneghan, C.; Mahtani, K.R.; Goldacre, B.; Godlee, F.; Macdonald, H.; Jarvies, D. Evidence based medicine manifesto for better healthcare. BMJ 2017, 357, j2973. [Google Scholar] [CrossRef] [PubMed]
- Improta, G.; Balato, G.; Romano, M.; Carpentieri, F.; Bifulco, P.; Russo, M.A.; Rosa, D.; Triassi, M.; Cesarelli, M. Lean Six Sigma: A new approach to the management of patients undergoing prosthetic hip replacement surgery. J. Evaluation Clin. Pr. 2015, 21, 662–672. [Google Scholar] [CrossRef]
- Mason, S.; Nicolay, C.; Darzi, A. The use of Lean and Six Sigma methodologies in surgery: A systematic review. Surgeon 2015, 13, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Sayeed, Z.; Anoushiravani, A.; El-Othmani, M.; Barinaga, G.; Sayeed, Y.; Cagle, P.; Saleh, K.J. Implementation of a Hip Fracture Care Pathway Using Lean Six Sigma Methodology in a Level I Trauma Center. J. Am. Acad. Orthop. Surg. 2018, 26, 881–893. [Google Scholar] [CrossRef]
- Sáez-López, P.; Brañas, F.; Sánchez-Hernández, N.; Alonso-García, N.; González-Montalvo, J.I. Hip fracture registries: Utility, description, and comparison. Osteoporos. Int. 2016, 28, 1157–1166. [Google Scholar] [CrossRef]
- Rojas, E.; Munoz-Gama, J.; Sepúlveda, M.; Capurro, D. Process mining in healthcare: A literature review. J. Biomed. Inf. 2016, 61, 224–236. [Google Scholar] [CrossRef]
- Padial, M.; Pinzón, S.; Navarro, B.; Juan, P.S.; Ruiz, J.; Espinosa, J.M. Implantación efectiva de la Cuádruple Hélice basada en el Modelo de Innovación en envejecimiento activo. Gac. Sanit. 2019, 33, 491–494. [Google Scholar] [CrossRef]
- Schwarz, U.V.T.; Nielsen, K.; Stenfors, T.; Hasson, H. Using kaizen to improve employee well-being: Results from two organizational intervention studies. Hum. Relat. 2016, 70, 966–993. [Google Scholar] [CrossRef] [Green Version]
- Walshe, K. Pseudoinnovation: The development and spread of healthcare quality improvement methodologies. Int. J. Qual. Health Care 2009, 21, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Liberatore, M.J. Six Sigma in healthcare delivery. Int. J. Health Care Qual. Assur. 2013, 26, 601–626. [Google Scholar] [CrossRef] [PubMed]
- Ullah, M.F.; Fleming, C.; Fox, C.L.; Tormey, S. Patient experience in a surgical assessment unit following a closed loop audit using a Kaizen Lean system. Mesentery Peritoneum 2019, 3, AB100. [Google Scholar] [CrossRef] [Green Version]
- Young, T.; Brailsford, S.; Connell, C.; Davies, R.; Harper, P.R.; Klein, J.H. Using industrial processes to improve patient care. BMJ 2004, 328, 162–164. [Google Scholar] [CrossRef] [Green Version]
- Spear, S.J. Fixing health care from the inside, today. Harv. Bus. Rev. 2005, 83, 78–91,158. [Google Scholar]
- Kollberg, B.; Dahlgaard, J.J.; Brehmer, P.-O. Measuring lean initiatives in health care services: Issues and findings. Int. J. Prod. Perform. Manag. 2006, 56, 7–24. [Google Scholar] [CrossRef]
- Bortolotti, T.; Boscari, S.; Danese, P.; Suni, H.A.M.; Rich, N.; Romano, P. The social benefits of kaizen initiatives in healthcare: An empirical study. Int. J. Oper. Prod. Manag. 2018, 38, 554–578. [Google Scholar] [CrossRef] [Green Version]
- Barrios, M.A.O.; Alfaro-Saíz, J.-J. Methodological Approaches to Support Process Improvement in Emergency Departments: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 2664. [Google Scholar] [CrossRef] [PubMed]
- Coelho, S.M.; Pinto, C.F.; Calado, R.D.; Marotta, E.A.; Romano, E.; Silva, M.B. Lean healthcare: Process improvement in a cancer utpatient chemotherapy unit. J. Innov. Heath Manag. 2015, 1, 1–9. [Google Scholar] [CrossRef]
- Curatolo, N.; Lamouri, S.; Huet, J.-C.; Rieutord, A. A critical analysis of Lean approach structuring in hospitals. Bus. Process. Manag. J. 2014, 20, 433–454. [Google Scholar] [CrossRef]
- Meyer, C.; Mitra, S.; Ruebush, E.; Sisler, L.; Wang, K.; Goldstein, A.O. A Lean Quality Improvement Initiative to Enhance Tobacco Use Treatment in a Cancer Hospital. Int. J. Environ. Res. Public Health 2020, 17, 2165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godley, M.; Jenkins, J.B. Decreasing Wait Times and Increasing Patient Satisfaction: A Lean Six Sigma Approach. J. Nurs. Care Qual. 2019, 34, 61–65. [Google Scholar] [CrossRef]
- Cree, M.; Hayduk, L.; Soskolne, C.L.; Suarez-Almazor, M. Modeling changes in health perception following hip fracture. Qual. Life Res. 2001, 10, 651–659. [Google Scholar] [CrossRef]
- Shyu, Y.-I.L.; Tang, W.-R.; Tsai, W.-C.; Liang, J.; Chen, M.-C. Emotional support levels can predict physical functioning and health related quality of life among elderly Taiwanese with hip fractures. Osteoporos. Int. 2005, 17, 501–506. [Google Scholar] [CrossRef] [Green Version]
- Locock, L.; Montgomery, C.; Parkin, S.; Chisholm, A.; Bostock, J.; Dopson, S.; Gager, M.; Gibbons, E.; Graham, C.; King, J.; et al. How do frontline staff use patient experience data for service improvement? Findings from an ethnographic case study evaluation. J. Health Serv. Res. Policy 2020, 25, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Harrington, H.J. Business Process Improvement; The breakthrough strategy for Total Quality, Productivity and Competitiveness; McGraw-Hill: New York, NY, USA, 1991. [Google Scholar]
- Davenport, T.H.; Short, J.E. The new industrial engineering: Information technology and business process redesign. Sloan Manag. Rev. 1990, 31, 11–27. [Google Scholar]
- Hammer, M.; Champy, J. Reengineering the corporation: A manifesto for business revolution. Bus. Horizons 1993, 36, 90–91. [Google Scholar] [CrossRef]
- Elzinga, D.; Horak, T.; Lee, C.-Y.; Bruner, C. Business process management: Survey and methodology. IEEE Trans. Eng. Manag. 1995, 42, 119–128. [Google Scholar] [CrossRef]
- Lee, K.; Chuah, K.B. A SUPER methodology for business process improvement—An industrial case study in Hong Kong/China. Int. J. Oper. Prod. Manag. 2001, 21, 687–706. [Google Scholar] [CrossRef]
- Gardner, R.A. Resolving the process paradox. Quality Prog. 2001, 34, 51–59. [Google Scholar]
- Alänge, S.; Steiber, A. The board’s role in sustaining major organizational change. Int. J. Qual. Serv. Sci. 2009, 1, 280–293. [Google Scholar] [CrossRef]
- Page, S. The Power of Business Process Improvement: 10 Simple Steps to Increase Effectiveness, Efficiency, and Adaptability; AMACOM, American Management Association: New York, NY, USA, 2010. [Google Scholar]
- Suárez-Barraza, M.F.; Hernández, F.P.; González, F.G.R. La Innovación en Procesos en Las Organizaciones; Ágora Medios: Toluca, Mexico, 2019. [Google Scholar]
- Yin, R.K. Case Study Research and Applications: Design and Methods, 6th ed.; Sage Publications: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Eisenhardt, K.M. Building Theories from Case Study Research. Acad. Manag. Rev. 1989, 14, 532–550. [Google Scholar] [CrossRef]
- Eisenhardt, K.M.; Graebner, M.E. Theory Building from Cases: Opportunities and Challenges. Acad. Manag. J. 2007, 50, 25–32. [Google Scholar] [CrossRef]
- Greenwood, D.J.; Levin, M. Reform of the social sciences and of universities through Action Research. In The SAGE Handbook of Qualitative Research, 2nd ed.; Denzin, N.K., Lincoln, Y.S., Eds.; Sage Publications: Thousand Oaks, CA, USA, 2000; pp. 84–106. [Google Scholar]
- Tanco, J.A.A.; Camarero, L.A. Investigación en acción: Cómo impulsar la contribución de la universidad en la competitividad de las organizaciones. Harv. Deusto Bus. Res. 2013, 2. Available online: http://www.hdbresearch.com/index.php/hdbr/article/view/33 (accessed on 27 December 2013).
- Coughlan, P.; Coghlan, D. Action research for operations management. Int. J. Oper. Prod. Manag. 2002, 22, 220–240. [Google Scholar] [CrossRef]
- Doman, M.S. A new lean paradigm in higher education: A case study. Qual. Assur. Educ. 2011, 19, 248–262. [Google Scholar] [CrossRef] [Green Version]
- Walters, L.M.; Nickerson, M.A.; Hall, L.A. Improving the 1040 process by applying lean principles: A case study. TQM J. 2019, 32, 249–267. [Google Scholar] [CrossRef]
- Douglas, J.A.; Antony, J.; Douglas, A. Waste identification and elimination in HEIs: The role of Lean thinking. Int. J. Qual. Reliab. Manag. 2015, 32, 970–981. [Google Scholar] [CrossRef]
- Suárez-Barraza, M.F.; Dahlgaard-Park, S.M.; Rodríguez-González, F.G.; Durán-Arechiga, C. In search of “Muda” through the TKJ diagram. Int. J. Qual. Serv. Sci. 2016, 8, 377–394. [Google Scholar] [CrossRef]



| 2019 | 2020 | |||
|---|---|---|---|---|
| Average | Std Dev | Average | Std Dev | |
| Total patient population | ||||
| Total (Women/Men) | 148 (109/39) | 106 (80/26) | ||
| Age (years) | 86.55 | 6.34 | 85.48 | 6.77 |
| In-hospital mortality (%) | 6.77 | 3.7 | ||
| Total hospitalization time (days) | 15.9 | 15.36 | 9.41 | 4.17 |
| Presurgical time (days) | 3.98 | 3.24 | 3.15 | 2.55 |
| Post-surgical average stay (days) | 10.12 | 6.77 | 5.25 | 3.25 |
| General: | Emergency Area: | Surgery: |
|---|---|---|
|
|
|
| Hospital floor level: | UCE (short stay unit): | |
|
|
| Activity Type | Flowchart Symbol | Count |
|---|---|---|
| Activity |  | 151 |
| Delay |  | 20 |
| Transport |  | 35 |
| Decisions |  | 7 |
| Inspection |  | 10 |
| Internal document |  | 6 |
| Electronic transport |  | 31 |
| Type of Muda |  | 60 |
| Total | Process activities Muda | 240 60 |
| Type of Muda | Count | % | Cumul % |  |
| Delay | 20 | 33% | 33% | |
| Transportation | 13 | 22% | 55% | |
| Overprocessing | 10 | 17% | 72% | |
| Defects | 6 | 10% | 82% | |
| Movement | 5 | 8% | 90% | |
| Overproduction | 2 | 3% | 93% | |
| Inventory | 2 | 3% | 97% | |
| Unused Talent | 2 | 3% | 100% | |
| Total | 60 | 100% | 100% | |
| (a) | (b) | |||
| Proposals | Muda |
|---|---|
| Establish a communication protocol with the Public Health system to ensure that every new patient brings a medical history file (in paper or electronic format), thus a more efficient approach will be adopted (some tests might not be necessary, avoiding duplicity and improving patient experience). | Delay Transportation Overprocessing Movement Overproduction |
Reduce the number of activities and the number of participants.
| All 8 types of muda |
| Avoid duplication of tasks (for instance, printing X-Ray in paper and saving it electronically). | Delay Overproduction |
| Reduce distances by locating some areas in a different place. Ex. After surgery doctor speaking to patients in a meeting room. | Delay Transportation |
| Review and maintenance of electronic equipment and IT systems with the aim of detecting potential causes for malfunctioning. | Delay Overprocessing |
| Automate some steps: When starting the process, some actions could be automatically initiated as tests (blood test, X-Ray) and medical consultations (calls to geriatrics or cardiologist). | Delay Overprocessing |
| Implement a system to measure the quality of the delivered service (patient satisfaction, patient experience, etc.). | Overprocessing Defects |
| Implement poka-yokes in operating processes within the operating room: marking leg, surgery checklist to be displayed in operating area, screen or board with main steps identifying critical activities with symbols. | Overprocessing Defects Overproduction |
| Implementation of 5s techniques in operating processes within the operating room. | All 8 types of muda |
| Clinical process standardization (for surgery, doctors and nurses). Administrative and data input process standardization. Training of personnel according to the abovementioned new standardized processes. | All 8 types of muda |
| Implementation of communication practices between doctors and nurses based on documentation of orders and instructions (it could be in the computer system or in patient´s logbooks) with the aim of minimizing errors due to misunderstandings or wrong interpretations. | Transportation Overprocessing Defects Overproduction |
| Implementation of an adequate inventory management system (EOQ, FIFO, etc.). | Inventory |
| Implementation of tools to record and share best practices within the hospital and among different hospitals within the group. Further data analysis to understand the variability of data. | All 8 types of muda |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morales-Contreras, M.F.; Chana-Valero, P.; Suárez-Barraza, M.F.; Saldaña Díaz, A.; García García, E. Applying Lean in Process Innovation in Healthcare: The Case of Hip Fracture. Int. J. Environ. Res. Public Health 2020, 17, 5273. https://doi.org/10.3390/ijerph17155273
Morales-Contreras MF, Chana-Valero P, Suárez-Barraza MF, Saldaña Díaz A, García García E. Applying Lean in Process Innovation in Healthcare: The Case of Hip Fracture. International Journal of Environmental Research and Public Health. 2020; 17(15):5273. https://doi.org/10.3390/ijerph17155273
Chicago/Turabian StyleMorales-Contreras, Manuel Francisco, Pedro Chana-Valero, Manuel F. Suárez-Barraza, Andrés Saldaña Díaz, and Elena García García. 2020. "Applying Lean in Process Innovation in Healthcare: The Case of Hip Fracture" International Journal of Environmental Research and Public Health 17, no. 15: 5273. https://doi.org/10.3390/ijerph17155273