The Impact of Regeneration and Climate Adaptations of Urban Green–Blue Assets on All-Cause Mortality: A 17-Year Longitudinal Study

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Zones
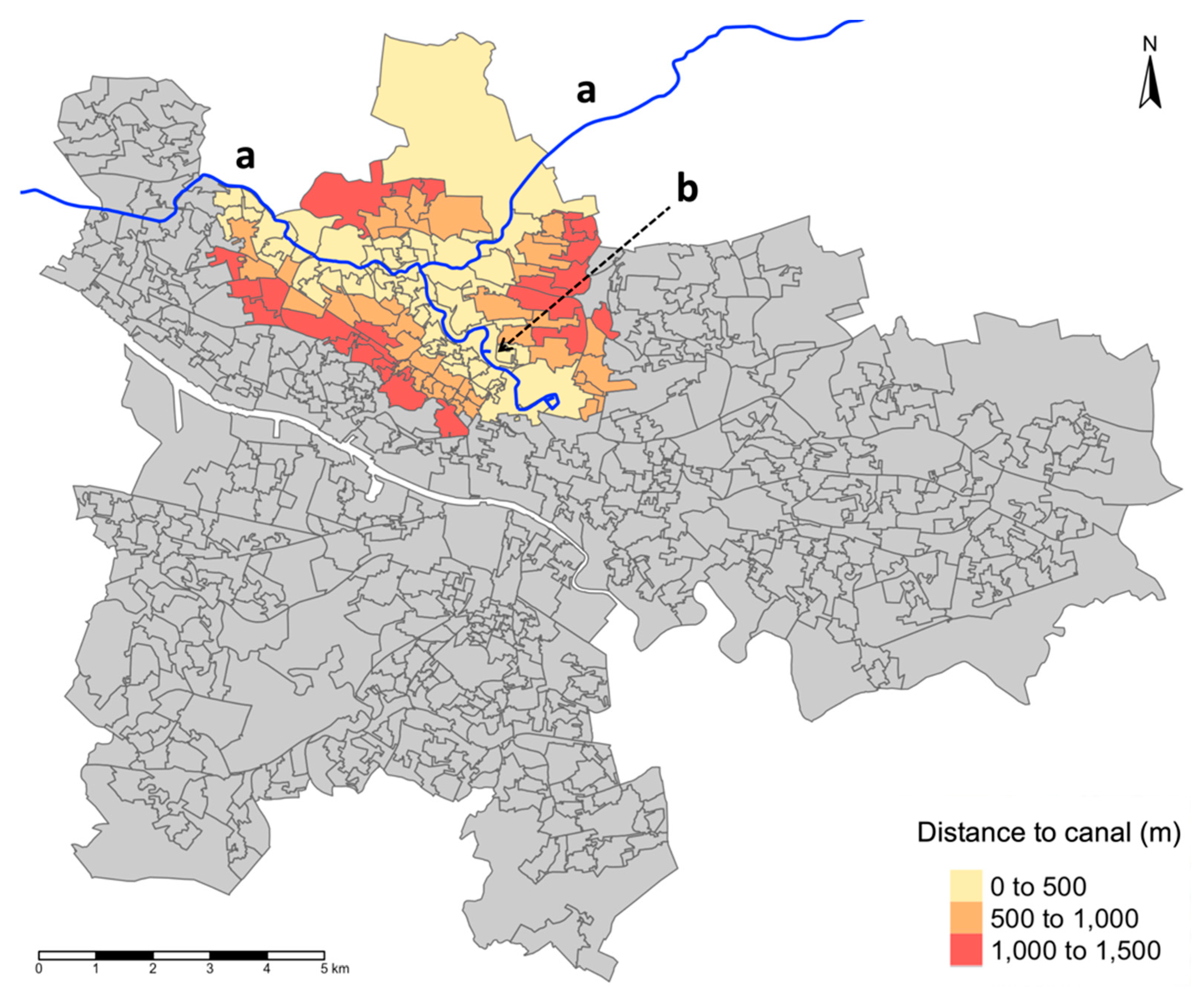
2.3. Exposure: Distance to the Glasgow Canal
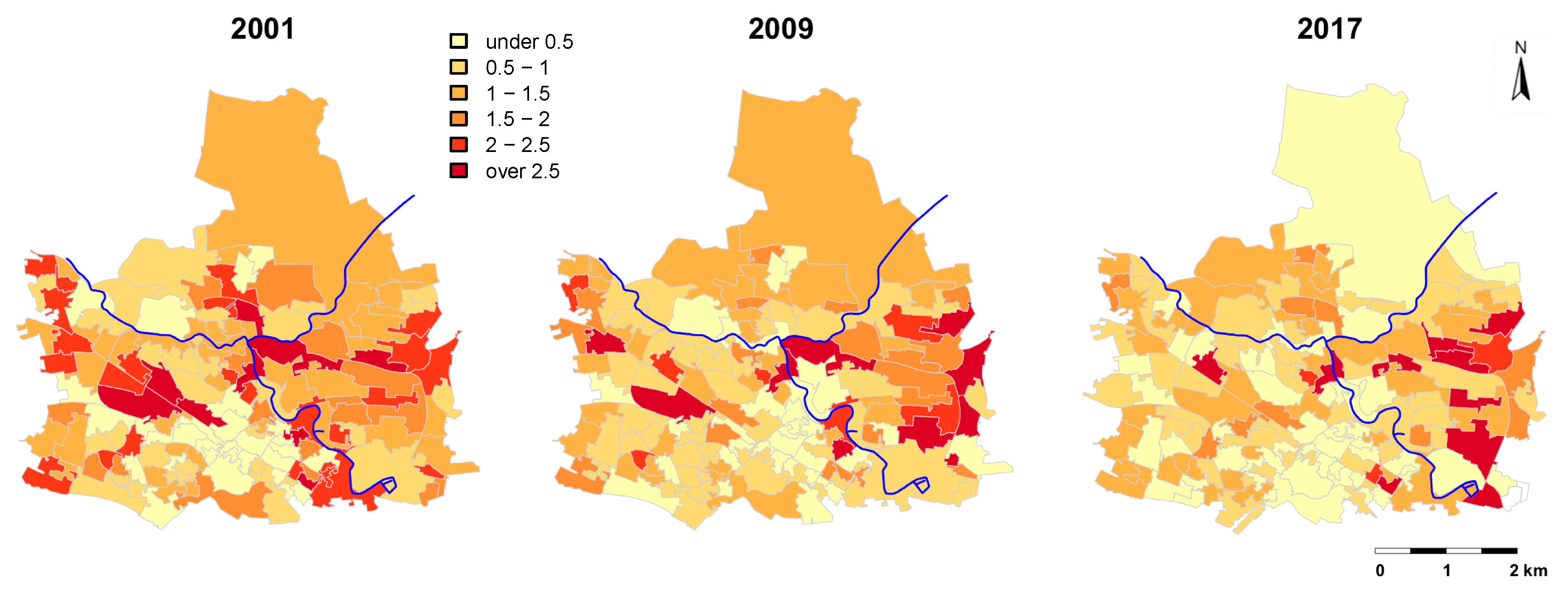
2.4. Outcome Variable: Mortality Rate
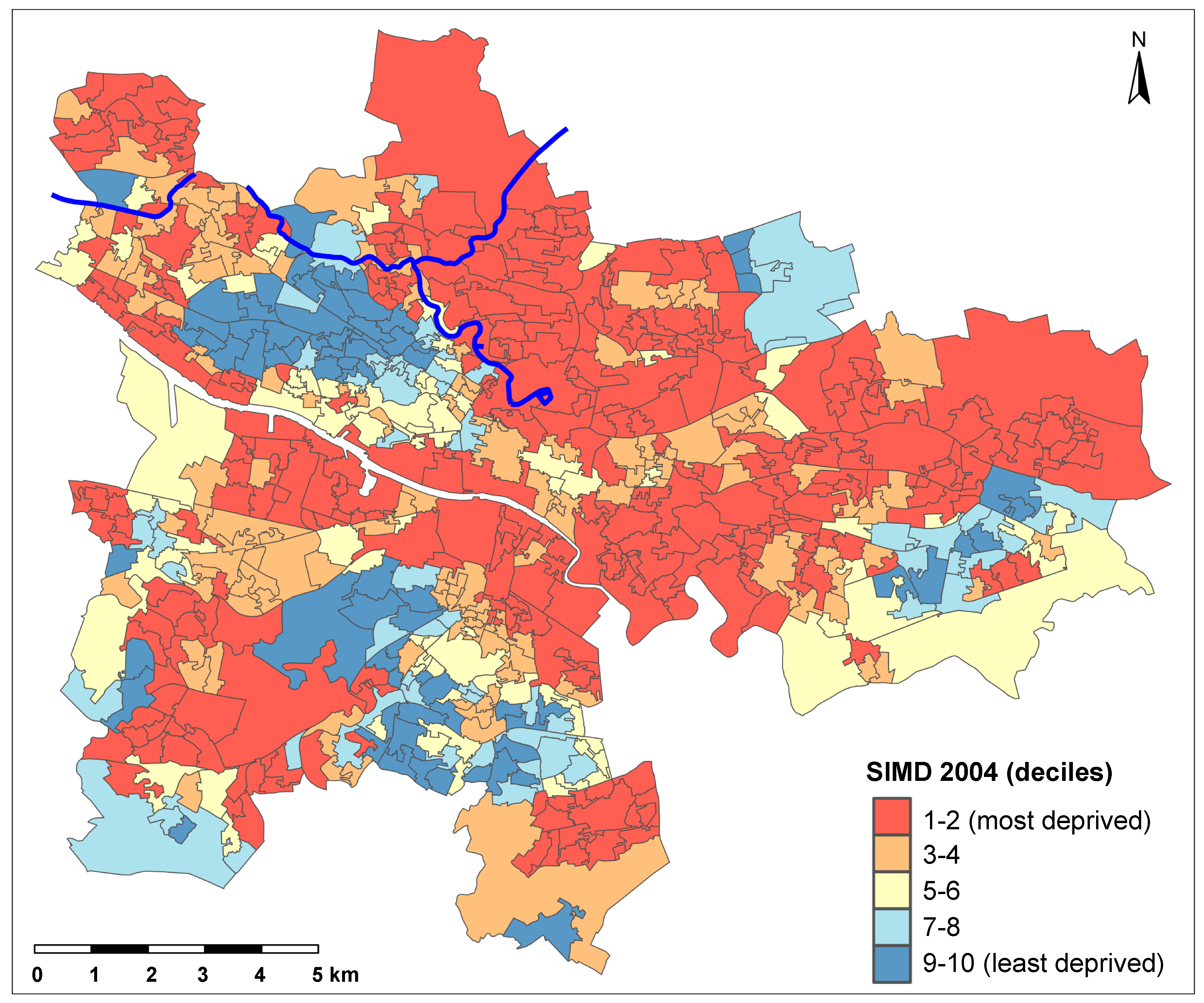
2.5. Covariates
2.6. Statistical Analysis
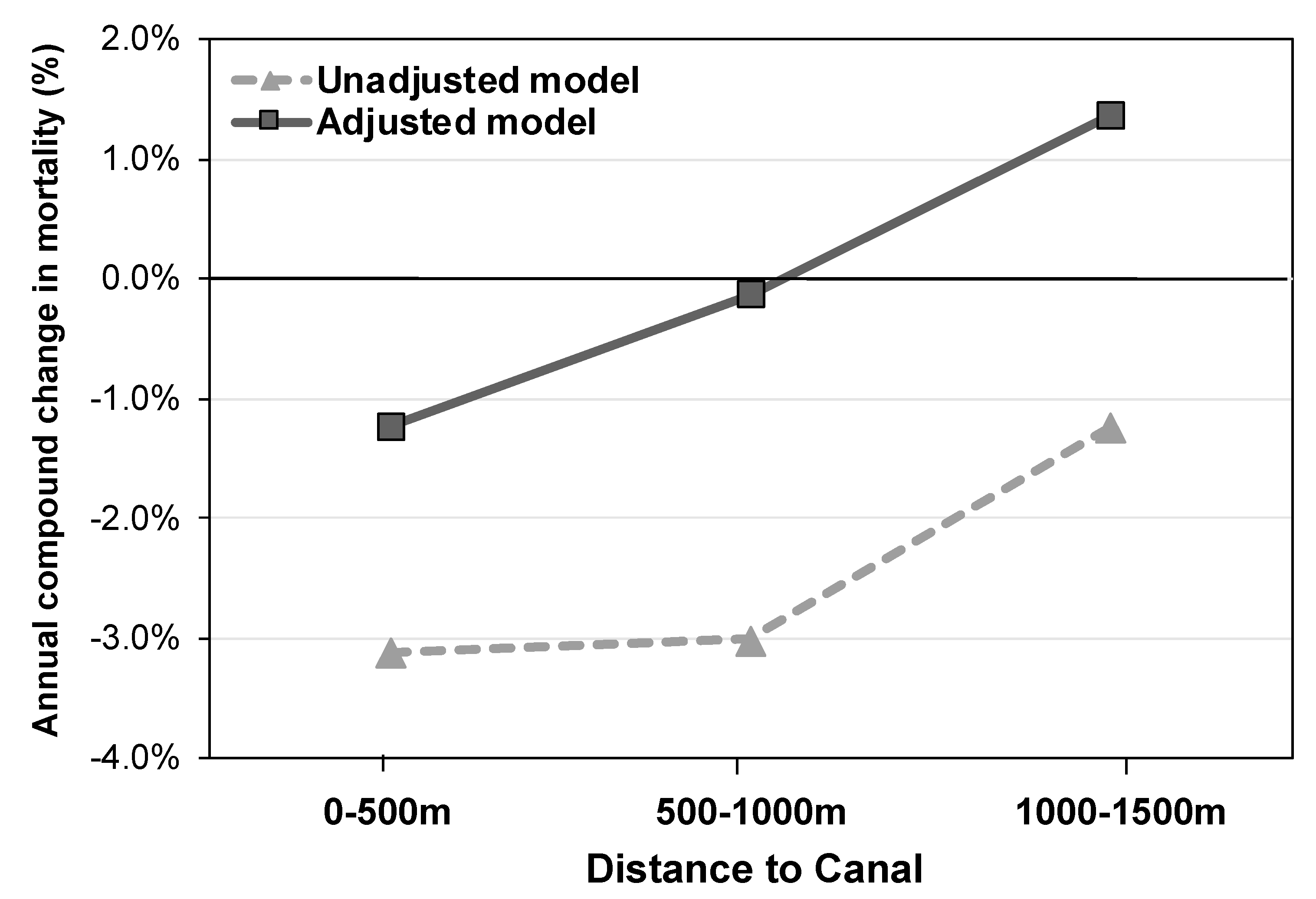
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- United Nations, Population Division. World Urbanization Prospects: The 2018 Revision. Population Division of the Department of Economic and Social Affairs of the United Nations. 2018. Available online: https://population.un.org/wup/Publications/Files/WUP2018-Report.pdf (accessed on 1 June 2020).
- Kummu, M.; de Moel, H.; Ward, P.J.; Varis, O. How close do we live to water? A global analysis of population distance to freshwater bodies. PLoS ONE 2011, 6, e20578. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.D.; Hutchins, M. The impacts of urbanisation and climate change on urban flooding and urban water quality: A review of the evidence concerning the United Kingdom. J. Hydrol. Reg. Stud. 2017, 12, 345–362. [Google Scholar] [CrossRef] [Green Version]
- Gehrels, H.; van der Meulen, S.; Schasfoort, F.; Bosch, P.; Brolsma, R.; van Dinther, D.; Geerling, G.J.; Goossens, M.; Jacobs, C.M.; Kok, S.; et al. Designing Green and Blue Infrastructure to Support Healthy Urban Living; TO2 Federatie: Utrecht, The Netherlands, 2016. [Google Scholar]
- World Health Organization. Connecting Global Priorities: Biodiversity and Human Health: A State of Knowledge Review; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Gascon, M.; Zijlema, W.; Vert, C.; White, M.P.; Nieuwenhuijsen, M.J. Outdoor blue spaces, human health and well-being: A systematic review of quantitative studies. Int. J. Hyg. Environ. Health 2017, 220, 1207–1221. [Google Scholar] [CrossRef] [PubMed]
- Macintyre, S.; Macdonald, L.; Ellaway, A. Do poorer people have poorer access to local resources and facilities? The distribution of local resources by area deprivation in Glasgow, Scotland. Soc. Sci. Med. 2008, 67, 900–914. [Google Scholar] [CrossRef] [Green Version]
- Elliott, L.R.; White, M.P.; Grellier, J.; Rees, P.; Waters, R.D.; Fleming, L.E. Recreational visits to marine and coastal environments in England: Where, what, who, why, and when? Mar. Policy 2018, 97, 305–314. [Google Scholar] [CrossRef] [Green Version]
- Dzhambov, A.M.; Dimitrova, D.D. Urban green spaces’ effectiveness as a psychological buffer for the negative health impact of noise pollution: A systematic review. Noise Health 2014, 16, 157–165. [Google Scholar] [CrossRef]
- Dzhambov, A.M.; Markevych, I.; Lercher, P. Associations of residential greenness, traffic noise, and air pollution with birth outcomes across Alpine areas. Sci. Total Environ. 2019, 678, 399–408. [Google Scholar] [CrossRef]
- European Environment Agency. Rivers and Lakes in European Cities—Past and Future Challenges; European Environment Agency: Copenhagen, Denmark, 2016.
- Scottish Government. Scotland’s Canals: An Asset for the Future. 2002. Available online: https://www.webarchive.org.uk/wayback/archive/20180521044514mp_/http://www.gov.scot/Resource/Doc/46997/0014804.pdf (accessed on 15 May 2020).
- Glasgow’s Smart Canal Is A First for Europe. Available online: https://www.glasgow.gov.uk/index.aspx?articleid=23393 (accessed on 1 May 2020).
- World Health Organisation. Health Statistics and Information Systems. Available online: https://www.who.int/healthinfo/statistics/indadultmortality/en/ (accessed on 1 June 2020).
- Office for National Statistics. 2001 Census Aggregate Data (Edition 2011); UK Data Service; Office for National Statistics: London, UK, 2011.
- Hanlon, P.; Lawder, R.S.; Buchanan, D.; Redpath, A.; Walsh, D.; Wood, R.; Bain, M.; Brewster, D.H.; Chalmers, J. Why is mortality higher in Scotland than in England and Wales? Decreasing influence of socioeconomic deprivation between 1981 and 2001 supports the existence of a ‘Scottish Effect’. J. Public Health 2005, 27, 199–204. [Google Scholar] [CrossRef] [Green Version]
- Maantay, J.A. The collapse of place: Derelict land, deprivation and health inequality in Glasgow, Scotland. In Urban Land Use: Commmunity-Based Planning; Etingoff, K., Ed.; Apple Academic Press: Oakville, ON, Canada, 2017; pp. 3–50. [Google Scholar]
- Fenton, L.; Wyper, G.M.; McCartney, G.; Minton, J. Socioeconomic inequality in recent adverse all-cause mortality trends in Scotland. J. Epidemiol. Community Health 2019, 73, 971–974. [Google Scholar] [CrossRef] [Green Version]
- Scottish Executive. Scottish Neighbourhood Statistics Data Zones; Scottish Executive: Edinburgh, UK, 2004. Available online: https://www.gov.scot/publications/scottish-neighbourhood-statistics-data-zones-background-information/pages/5/ (accessed on 1 June 2020).
- Scottish Government. Available online: https://www2.gov.scot/Topics/Statistics/sns/SNSRef/DZMatchingFile (accessed on 9 February 2020).
- Norman, P.; Rees, P.; Boyle, P. Achieving data compatibility over space and time: Creating consistent geographical zones. Int. J. Popul. Geogr. 2003, 9, 365–386. [Google Scholar] [CrossRef] [Green Version]
- Pebesma, E. Simple Features for R: Standardized Support for Spatial Vector Data. R J. 2018, 10, 439–446. [Google Scholar] [CrossRef] [Green Version]
- Labib, S.M.; Lindley, S.; Huck, J.J. Spatial dimensions of the influence of urban green-blue spaces on human health: A systematic review. Environ. Res. 2020, 180, 108869. [Google Scholar] [CrossRef] [PubMed]
- Scottish Government. The Scottish Index of Multiple Deprivation. A National Statistics Publication for Scotland. Available online: http://www.gov.scot/Topics/Statistics/SIMD (accessed on 5 February 2020).
- Scottish Government Office of the Chief Statistician. Analysis Using the SIMD—Change over Time; Scottish Government: Edinburgh, UK, 2010.
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. Available online: https://www.R-project.org/ (accessed on 10 February 2020).
- Bates, D.; Maechler, M.; Bolker, B.; Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Martin, M.H.T.; Whyte, B. Recent Mortality Trends in Glasgow: Age- and Gender-Specific Mortality Compared with the Rest of Scotland, 1981–2015; Glasgow Centre for Population Health: Glasgow, UK, 2017. [Google Scholar]
- Public Health Scotland. Stalling Life Expectancy Is a Warning Light for Public Health in Scotland. Available online: http://www.healthscotland.scot/news/2019/february/stalling-life-expectancy-is-a-warning-light-for-public-health-in-scotland (accessed on 24 April 2020).
- Mears, M.; Bridnley, P. Measuring Urban Greenspace Distribution Equity: The Importance of Appropriate Methodological Approaches. Int. J. Geo-Inf. 2019, 8, 286. [Google Scholar] [CrossRef] [Green Version]
- Apparicio, P.; Abdelmajid, M.; Riva, M.; Shearmur, R. Comparing alternative approaches to measuring the geographical accessibility of urban health services: Distance types and aggregation-error issues. Int. J. Health Geogr. 2008, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Zimmerman, F.J.; Anderson, N.W. Trends in Health Equity in the United States by Race/Ethnicity, Sex, and Income, 1993–2017. JAMA Netw. Open 2019, 2, e196386. [Google Scholar] [CrossRef]
- Mitchell, R.; Popham, F. Effect of exposure to natural environment on health inequalities: An observational population study. Lancet 2008, 372, 1655–1660. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Yan, G.; Wu, Y.; Wang, Y.; Zhang, Z.; Zhang, M. Wetlands with greater degree of urbanization improve PM2.5 removal efficiency. Chemosphere 2018, 207, 601–611. [Google Scholar] [CrossRef]
- Gunawardena, K.R.; Wells, M.J.; Kershaw, T. Utilising green and bluespace to mitigate urban heat island intensity. Sci. Total Environ. 2017, 584–585, 1040–1055. [Google Scholar] [CrossRef]
- Burkart, K.; Meier, F.; Schneider, A.; Breitner, S.; Canario, P.; Alcoforado, M.J.; Scherer, D.; Endlicher, W. Modification of Heat-Related Mortality in an Elderly Urban Population by Vegetation (Urban Green) and Proximity to Water (Urban Blue): Evidence from Lisbon, Portugal. Environ. Health Perspect. 2016, 124, 927–934. [Google Scholar] [CrossRef] [Green Version]
- Pasanen, T.P.; White, M.P.; Wheeler, B.W.; Garrett, J.K.; Elliott, L.R. Neighbourhood blue space, health and wellbeing: The mediating role of different types of physical activity. Environ. Int. 2019, 131, 105016. [Google Scholar] [CrossRef] [PubMed]
- Jansen, F.M.; Ettema, D.F.; Kamphuis, C.B.M.; Pierik, F.H.; Dijst, M.J. How do type and size of natural environments relate to physical activity behavior? Health Place 2017, 46, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Arbillaga-Etxarri, A.; Gimeno-Santos, E.; Barberan-Garcia, A.; Benet, M.; Borrell, E.; Dadvand, P.; Foraster, M.; Marin, A.; Monteagudo, M.; Rodriguez-Roisin, R.; et al. Socio-environmental correlates of physical activity in patients with chronic obstructive pulmonary disease (COPD). Thorax 2017, 72, 796–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnberger, A.; Eder, R.; Allex, B.; Ebenberger, M.; Hutter, H.P.; Wallner, P.; Bauer, N.; Zaller, J.G.; Frank, T. Health-Related Effects of Short Stays at Mountain Meadows, a River and an Urban Site-Results from a Field Experiment. Int. J. Environ. Res. Public Health 2018, 15, 2647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hipp, J.R.; Corcoran, J.; Wickes, R.; Li, T. Examining the social porosity of environmental features on neighborhood sociability and attachment. PLoS ONE 2014, 9, e84544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weigand, M.; Wurm, M.; Dech, S.; Taubenböck, H. Remote Sensing in Environmental Justice Research—A Review. Int. J. Geo-Inf. 2019, 8, 20. [Google Scholar] [CrossRef] [Green Version]
- Grellier, J.; White, M.P.; Albin, M.; Bell, S.; Elliott, L.R.; Gascon, M.; Gualdi, S.; Mancini, L.; Nieuwenhuijsen, M.J.; Sarigiannis, D.A.; et al. BlueHealth: A study programme protocol for mapping and quantifying the potential benefits to public health and well-being from Europe’s blue spaces. BMJ Open 2017, 7, e016188. [Google Scholar] [CrossRef] [Green Version]





© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tieges, Z.; McGregor, D.; Georgiou, M.; Smith, N.; Saunders, J.; Millar, R.; Morison, G.; Chastin, S. The Impact of Regeneration and Climate Adaptations of Urban Green–Blue Assets on All-Cause Mortality: A 17-Year Longitudinal Study. Int. J. Environ. Res. Public Health 2020, 17, 4577. https://doi.org/10.3390/ijerph17124577
Tieges Z, McGregor D, Georgiou M, Smith N, Saunders J, Millar R, Morison G, Chastin S. The Impact of Regeneration and Climate Adaptations of Urban Green–Blue Assets on All-Cause Mortality: A 17-Year Longitudinal Study. International Journal of Environmental Research and Public Health. 2020; 17(12):4577. https://doi.org/10.3390/ijerph17124577
Chicago/Turabian StyleTieges, Zoë, Duncan McGregor, Michail Georgiou, Niamh Smith, Josie Saunders, Richard Millar, Gordon Morison, and Sebastien Chastin. 2020. "The Impact of Regeneration and Climate Adaptations of Urban Green–Blue Assets on All-Cause Mortality: A 17-Year Longitudinal Study" International Journal of Environmental Research and Public Health 17, no. 12: 4577. https://doi.org/10.3390/ijerph17124577