Relationships between Foot Morphology and Foot Muscle Strength in Healthy Adults


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
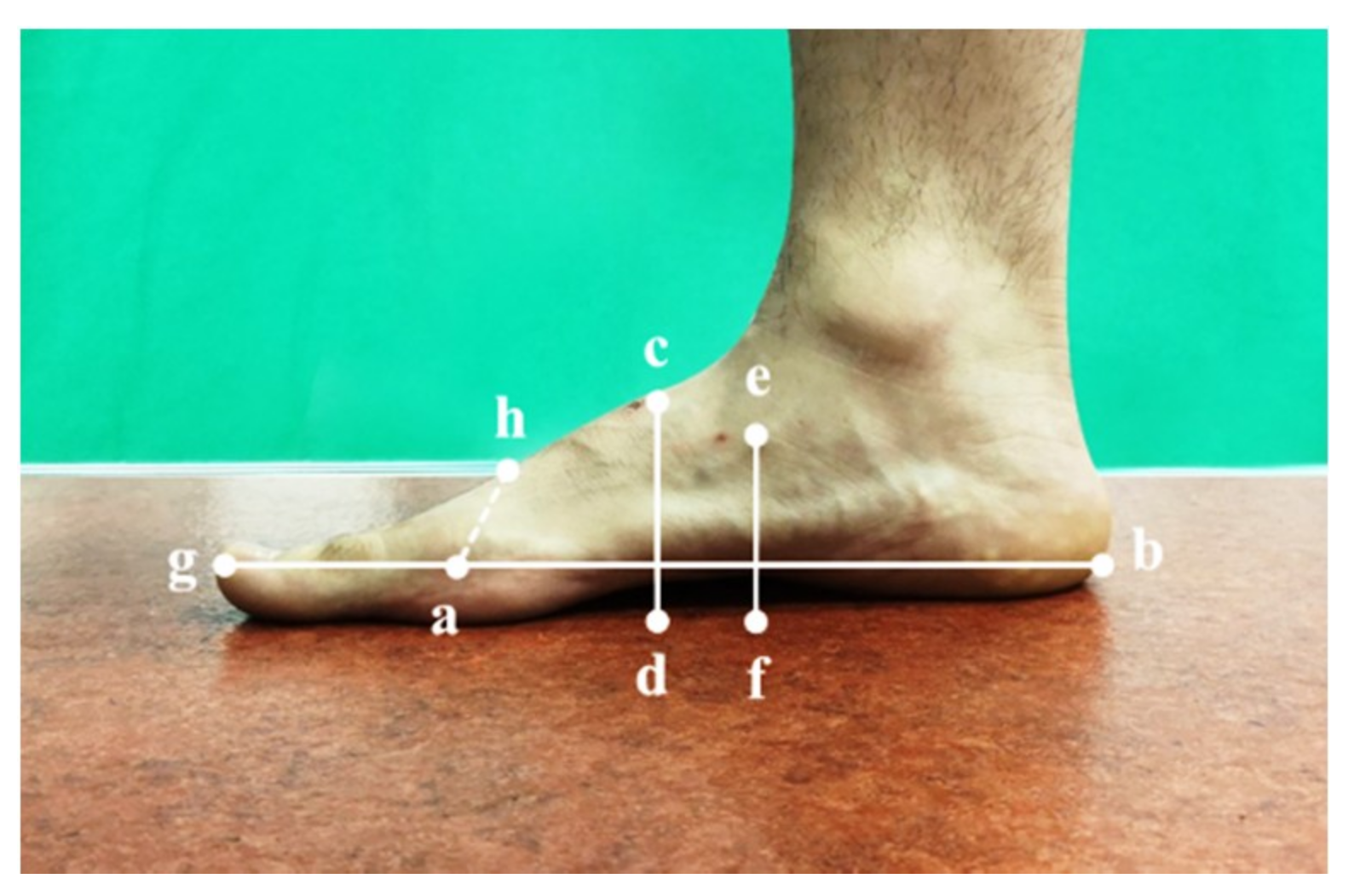
2.2.1. Foot Morphology in Standing and Sitting Positions
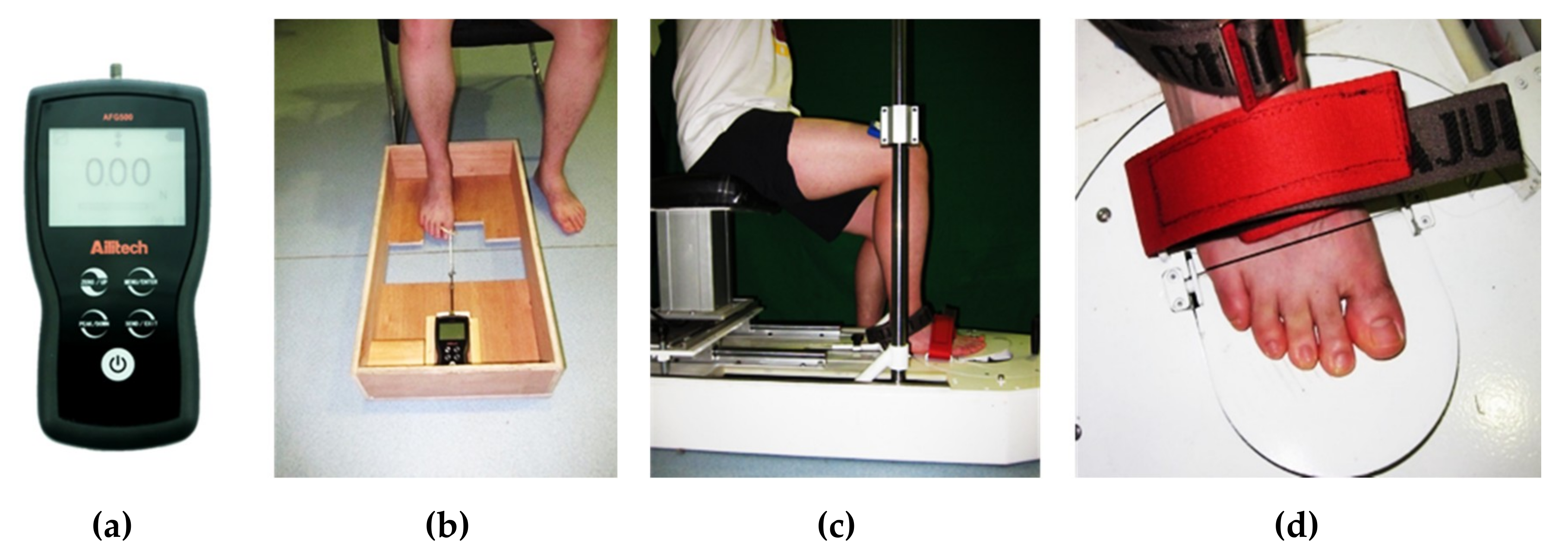
2.2.2. Toe Flexor Strength
2.2.3. Metatarsophalangeal Joint Flexor Strength
2.3. Data Processing
2.4. Statistics
3. Results
3.1. Foot Morphology and Foot Muscle Strength
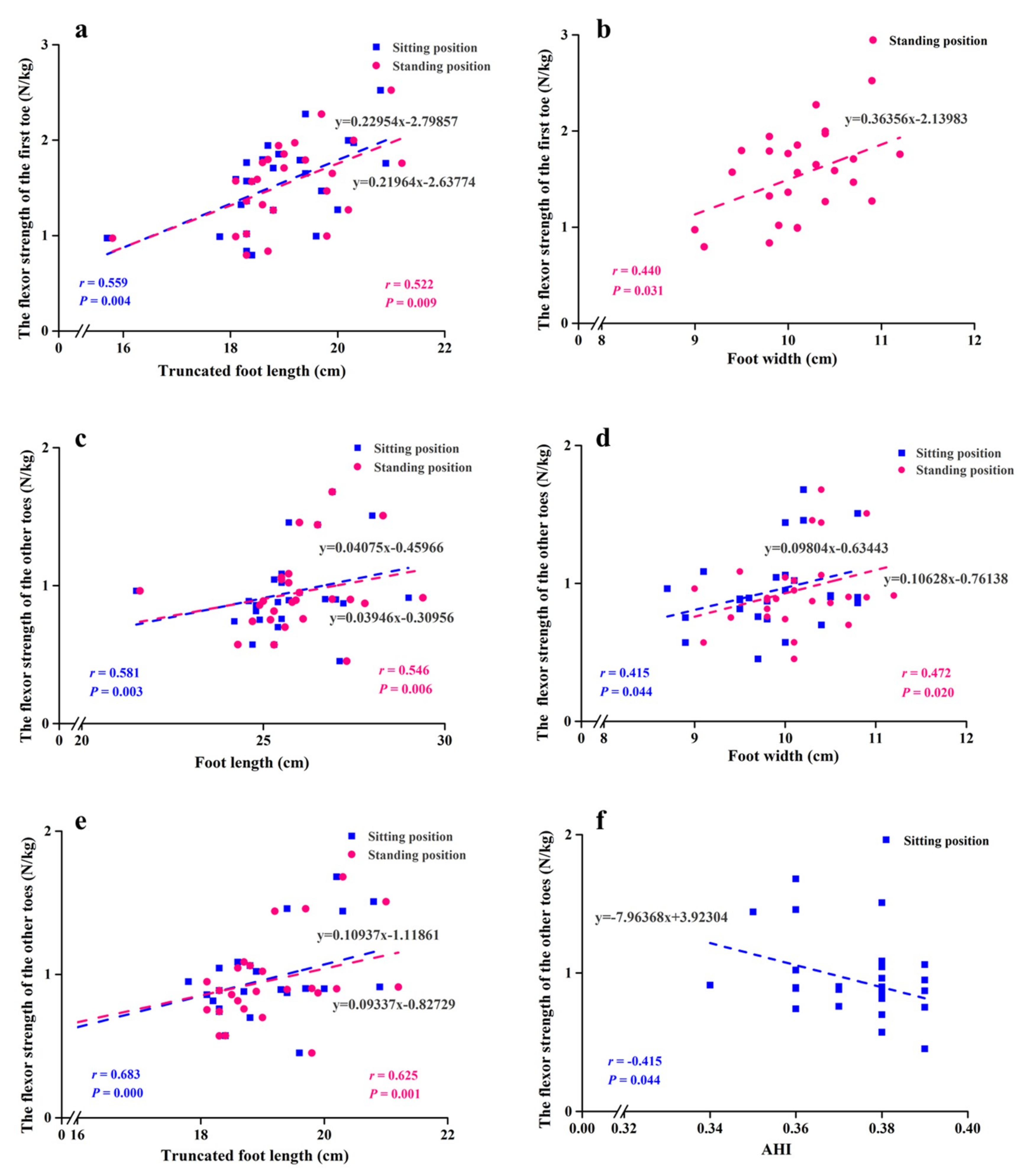
3.2. Relationships Between Foot Morphology and Toe Flexor Strength
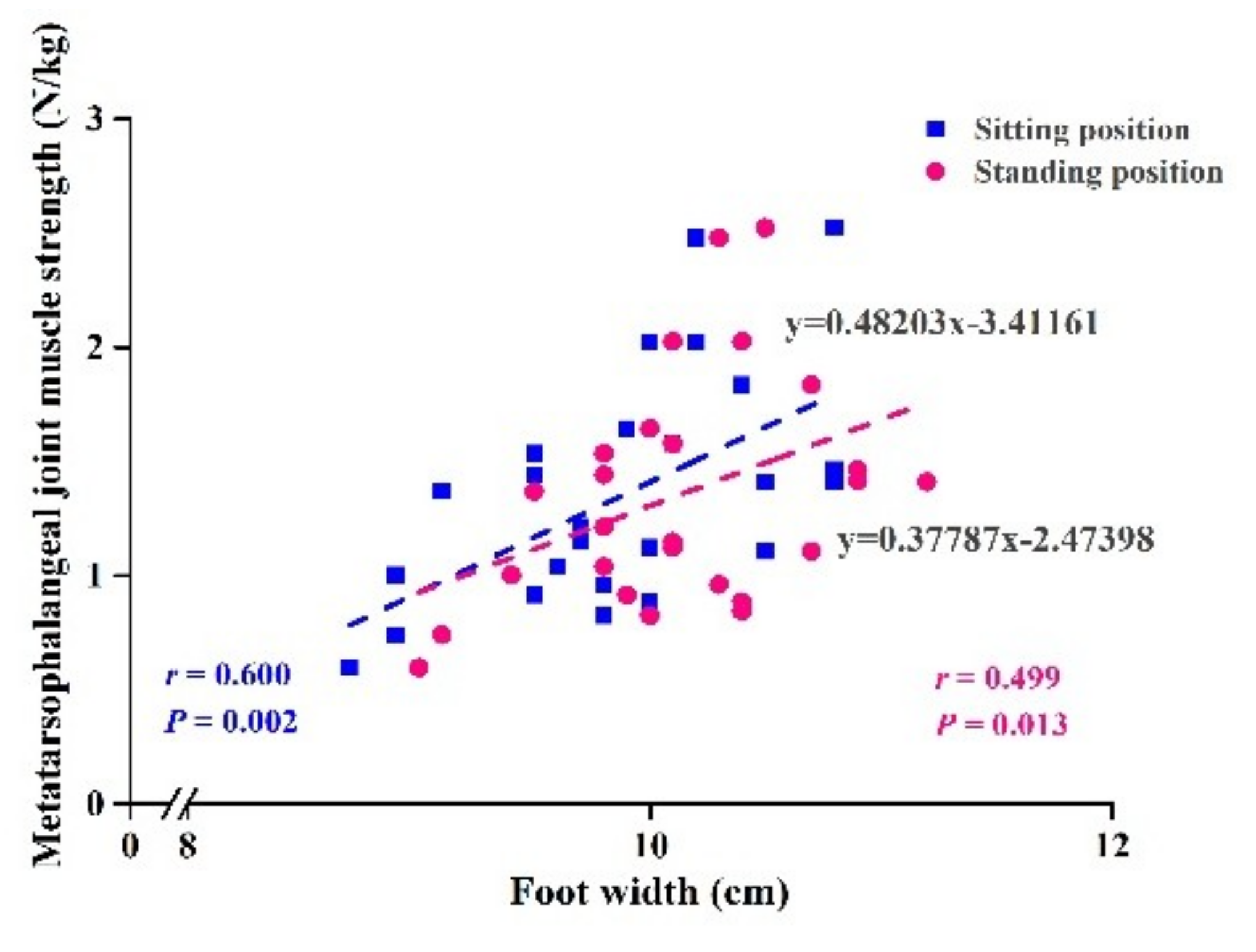
3.3. Relationships Between Foot Morphology and Metatarsophalangeal Joint Flexor Strength
3.4. Relationships Between the Differences in Foot Morphology and Foot Muscle Strength
3.5. Regression Model of Relationships Between Foot Morphology and Foot Muscle Strength
4. Discussion
4.1. Foot Morphology in Sitting and Standing Positions
4.2. Relationships between Foot Morphology and Foot Muscle Strength
4.3. Relationships between the Differences in Foot Morphology and Foot Muscle Strength
4.4. Clinical Applications
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Holowka, N.B.; Lieberman, D.E. Rethinking the evolution of the human foot: insights from experimental research. J. Exp. Biol. 2018, 221 Pt 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Pinillos, F.; Molina-Molina, A.; Párraga-Montilla, J.A.; Latorre-Román, P.A. Kinematic alterations after two high-intensity intermittent training protocols in endurance runners. J. Sport Health Sci. 2019, 8, 442–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shultz, S.P.; Song, J.; Kraszewski, A.P.; Hafer, J.F.; Rao, S.; Backus, S.; Hillstrom, R.M.; Hillstrom, H.J. An investigation of structure, flexibility, and function variables that discriminate asymptomatic foot types. J. Appl. Biomech. 2017, 33, 203–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKeon, P.O.; Hertel, J.; Bramble, D.; Davis, I. The foot core system: a new paradigm for understanding intrinsic foot muscle function. Br. J. Sports Med. 2015, 49, 290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hillstrom, H.J.; Song, J.; Kraszewski, A.P.; Hafer, J.F.; Mootanah, R.; Dufour, A.B.; Chow, B.S.; Deland, J.T. Foot type biomechanics part 1: structure and function of the asymptomatic foot. Gait Posture 2013, 37, 445–451. [Google Scholar] [CrossRef] [Green Version]
- Mootanah, R.; Song, J.; Lenhoff, M.W.; Hafer, J.F.; Backus, S.I.; Gagnon, D.; Deland, J.T.; Hillstrom, H.J. Foot Type Biomechanics Part 2: are structure and anthropometrics related to function? Gait Posture 2013, 37, 452–456. [Google Scholar] [CrossRef] [Green Version]
- Yamauchi, J.; Koyama, K. Force-generating capacity of the toe flexor muscles and dynamic function of the foot arch in upright standing. J. Anat. 2019, 234, 515–522. [Google Scholar] [CrossRef]
- Lopez Lopez, D.; Bouza Prego Mde, L.; Requeijo Constenla, A.; Saleta Canosa, J.L.; Bautista Casasnovas, A.; Tajes, F.A. The impact of foot arch height on quality of life in 6–12 year olds. Colomb. Med. (Cali). 2014, 45, 168–172. [Google Scholar] [CrossRef]
- Lopez-Lopez, D.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Palomo-Lopez, P.; Rodriguez-Sanz, D.; Brandariz-Pereira, J.M.; Calvo-Lobo, C. Evaluation of foot health related quality of life in individuals with foot problems by gender: a cross-sectional comparative analysis study. BMJ Open. 2018, 8, e023980. [Google Scholar] [CrossRef] [Green Version]
- Kurihara, T.; Yamauchi, J.; Otsuka, M.; Tottori, N.; Hashimoto, T.; Isaka, T. Maximum toe flexor muscle strength and quantitative analysis of human plantar intrinsic and extrinsic muscles by a magnetic resonance imaging technique. J. Foot Ankle Res. 2014, 7, 26. [Google Scholar] [CrossRef]
- Nagano, K.; Okuyama, R.; Taniguchi, N.; Yoshida, T. Gender difference in factors affecting the medial longitudinal arch height of the foot in healthy young adults. J. Phys. Ther. Sci. 2018, 30, 675–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, J.; Clark, P.; Klenerman, L. The importance of the toes in walking. J. Bone Joint Surg. Br. 1990, 72, 245–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mickle, K.J.; Munro, B.J.; Lord, S.R.; Menz, H.B.; Steele, J.R. ISB Clinical Biomechanics Award 2009: toe weakness and deformity increase the risk of falls in older people. Clin. Biomech. (Bristol, Avon.) 2009, 24, 787–791. [Google Scholar] [CrossRef] [PubMed]
- Ridge, S.T.; Myrer, J.W.; Olsen, M.T.; Jurgensmeier, K.; Johnson, A.W. Reliability of doming and toe flexion testing to quantify foot muscle strength. J. Foot Ankle Res. 2017, 10, 55. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Chen, L.; Liu, W.; Su, B.; Zhang, Y. Early detection of atrophy of foot muscles in Chinese patients of type 2 diabetes mellitus by high-frequency ultrasonography. J. Diabetes Res. 2014, 2014, 927069. [Google Scholar] [CrossRef] [Green Version]
- Chang, R.; Kent-Braun, J.A.; Hamill, J. Use of MRI for volume estimation of tibialis posterior and plantar intrinsic foot muscles in healthy and chronic plantar fasciitis limbs. Clin. Biomech. (Bristol, Avon.) 2012, 27, 500–505. [Google Scholar] [CrossRef]
- Cavanagh, P.R.; Morag, E.; Boulton, A.J.; Young, M.J.; Deffner, K.T.; Pammer, S.E. The relationship of static foot structure to dynamic foot function. J. Biomech. 1997, 30, 243–250. [Google Scholar] [CrossRef]
- Uritani, D.; Fukumoto, T.; Matsumoto, D.; Shima, M. Associations between toe grip strength and hallux valgus, toe curl ability, and foot arch height in Japanese adults aged 20 to 79 years: a cross-sectional study. J. Foot Ankle Res. 2015, 8, 18. [Google Scholar] [CrossRef] [Green Version]
- Yokozuka, M.; Okazaki, K.; Sakamoto, Y.; Takahashi, K. Relationship between foot morphology and toe muscle strength in female university students. J. Phys. Ther. Sci. 2019, 31, 457–461. [Google Scholar] [CrossRef] [Green Version]
- McPoil, T.G.; Cornwall, M.W.; Medoff, L.; Vicenzino, B.; Forsberg, K.; Hilz, D. Arch height change during sit-to-stand: an alternative for the navicular drop test. J. Foot Ankle Res. 2008, 1, 3. [Google Scholar] [CrossRef] [Green Version]
- Williams, D.S.; McClay, I.S. Measurements used to characterize the foot and the medial longitudinal arch: reliability and validity. Phys. Ther. 2000, 80, 864–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, S.; Fu, W.; Liu, Y. Does habitual rear-foot strike pattern with modern running shoes affect the muscle strength of the longitudinal arch? Isoki. Exer. Sci. 2019, 27, 213–218. [Google Scholar] [CrossRef]
- Butler, R.J.; Hillstrom, H.; Song, J.; Richards, C.J.; Davis, I.S. Arch height index measurement system: establishment of reliability and normative values. J. Am. Podiatr. Med. Assoc. 2008, 98, 102–106. [Google Scholar] [CrossRef]
- Zhao, X.; Tsujimoto, T.; Kim, B.; Katayama, Y.; Tanaka, K. Characteristics of foot morphology and their relationship to gender, age, body mass index and bilateral asymmetry in Japanese adults. J. Back Musculoskelet. Rehabil. 2017, 30, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Mulligan, E.P.; Cook, P.G. Effect of plantar intrinsic muscle training on medial longitudinal arch morphology and dynamic function. Man. Ther. 2013, 18, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Krishan, K. Establishing correlation of footprints with body weight--forensic aspects. Forensic Sci. Int. 2008, 179, 63–69. [Google Scholar] [CrossRef]
- Kim, W.; Kim, Y.M.; Yun, M.H. Estimation of stature from hand and foot dimensions in a Korean population. J. Forensic Leg. Med. 2018, 55, 87–92. [Google Scholar] [CrossRef]
- Zhao, X.; Tsujimoto, T.; Kim, B.; Tanaka, K. Association of arch height with ankle muscle strength and physical performance in adult men. Biol. Sport. 2017, 34, 119–126. [Google Scholar] [CrossRef] [Green Version]
- Clermont, C.A.; Phinyomark, A.; Osis, S.T.; Ferber, R. Classification of higher- and lower-mileage runners based on running kinematics. J. Sport Health Sci. 2019, 8, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Morita, N.; Yamauchi, J.; Kurihara, T.; Fukuoka, R.; Otsuka, M.; Okuda, T.; Ishizawa, N.; Nakajima, T.; Nakamichi, R.; Matsuno, S.; et al. Toe flexor strength and foot arch height in children. Med. Sci. Sports Exerc. 2015, 47, 350–356. [Google Scholar] [CrossRef]
- Zifchock, R.A.; Davis, I.; Hillstrom, H.; Song, J. The effect of gender, age, and lateral dominance on arch height and arch stiffness. Foot Ankle Int. 2006, 27, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Carson, D.W.; Myer, G.D.; Hewett, T.E.; Heidt, R.S., Jr.; Ford, K.R. Increased plantar force and impulse in American football players with high arch compared to normal arch. Foot (Edinb.) 2012, 22, 310–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tudor, A.; Ruzic, L.; Sestan, B.; Sirola, L.; Prpic, T. Flat-footedness is not a disadvantage for athletic performance in children aged 11 to 15 years. Pediatrics. 2009, 123, e386–e392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez-Lopez, D.; Vilar-Fernandez, J.M.; Barros-Garcia, G.; Losa-Iglesias, M.E.; Palomo-Lopez, P.; Becerro-de-Bengoa-Vallejo, R.; Calvo-Lobo, C. Foot arch height and quality of life in adults: a strobe observational study. Int. J. Environ. Res. Public Health. 2018, 15, 1555. [Google Scholar] [CrossRef] [Green Version]
- Arevalo-Mora, J.F.; Reina-Bueno, M.; Munuera, P.V. Influence of children’s foot type on their physical motor performance. J. Am. Podiatr. Med. Assoc. 2016, 106, 15–21. [Google Scholar] [CrossRef]
- Yamauchi, J.; Koyama, K. Toe flexor strength is not related to postural stability during static upright standing in healthy young individuals. Gait posture 2019, 73, 323–327. [Google Scholar] [CrossRef]
- Uritani, D.; Fukumoto, T.; Matsumoto, D.; Shima, M. Reference values for toe grip strength among Japanese adults aged 20 to 79 years: a cross-sectional study. J. Foot Ankle Res. 2014, 7, 28. [Google Scholar] [CrossRef] [Green Version]
- Price, C.; Nester, C. Foot dimensions and morphology in healthy weight, overweight and obese males. Clin. Biomech. (Bristol, Avon.) 2016, 37, 125–130. [Google Scholar] [CrossRef] [Green Version]
- Xiong, S.; Goonetilleke, R.; Zhao, J.; Li, W.; Witana, C. Foot deformations under different load-bearing conditions and their relationships to stature and body weight. Anthropol. Sci. 2009, 117, 77–88. [Google Scholar] [CrossRef] [Green Version]
- Kelly, L.A.; Cresswell, A.G.; Racinais, S.; Whiteley, R.; Lichtwark, G. Intrinsic foot muscles have the capacity to control deformation of the longitudinal arch. J. R. Soc. Interface. 2014, 11, 20131188. [Google Scholar] [CrossRef] [Green Version]
- Munuera, P.V.; Dominguez, G.; Palomo, I.C.; Lafuente, G. Effects of rearfoot-controlling orthotic treatment on dorsiflexion of the hallux in feet with abnormal subtalar pronation: a preliminary report. J. Am. Podiatr. Med. Assoc. 2006, 96, 283–289. [Google Scholar] [CrossRef] [Green Version]
- Wright, W.G.; Ivanenko, Y.P.; Gurfinkel, V.S. Foot anatomy specialization for postural sensation and control. J. Neurophysiol. 2012, 107, 1513–1521. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Definition | Source |
|---|---|---|
| Foot length (cm) | Measured from the most posterior point of the calcaneus to the distal end of the longest toe | Butler et al., 2008 [23] |
| Foot width (cm) | Measured from the first metatarsophalangeal joint to the fifth metatarsophalangeal joint | Zhao et al., 2017 [24] |
| Truncated foot length (cm) | Measured from the most posterior point of the calcaneus to the first metatarsophalangeal joint | Butler et al., 2008 [23] |
| Navicular height (cm) | Measured from the ground to the tuberosity of navicular bone | Mulligan et al., 2013 [25] |
| Dorsum height at 50% of the foot length (cm) | Obtained at 50% of foot length with a vertical caliper measured from the ground to the top of the dorsum | Mulligan et al., 2013 [25] |
| Arch height index (AHI) | Calculated as the dorsum height at 50% of the total foot length divided by truncated foot length | Williams et al., 2000 [21] |
| Variables | Sitting Position | Standing Position | Effect Size | Diff. |
|---|---|---|---|---|
| Foot length (cm) | 25.71 ± 1.42 | 25.95 ± 1.47 ** | 1.09 | 0.23 ± 0.22 |
| Foot width (cm) | 9.88 ± 0.58 | 10.12 ± 0.54 ** | 1.21 | 0.24 ± 0.20 |
| Navicular height (cm) | 5.44 ± 0.45 | 4.91 ± 0.54 ** | 1.15 | 0.53 ± 0.46 |
| Dorsum height at 50% of the foot length (cm) | 7.03 ± 0.38 | 6.53 ± 0.41 ** | 2.46 | 0.50 ± 0.20 |
| Truncated foot length (cm) | 18.90 ± 1.08 | 19.02 ± 1.08 | 0.4 | 0.12 ± 0.30 |
| AHI | 0.37 ± 0.01 | 0.34 ± 0.02 ** | 1.95 | 0.03 ± 0.01 |
| Toe Flexor Strength | Position | Foot Morphology | r | p-Value | r (Adjusted) | p-Value |
|---|---|---|---|---|---|---|
| Flexor strength of the first toe | Sitting position | Foot length | 0.390 | 0.049 | 0.327 | 0.118 |
| Foot width | 0.427 | 0.029 | 0.393 | 0.057 | ||
| Navicular height | −0.003 | 0.990 | −0.208 | 0.330 | ||
| Dorsum height at 50% of the foot length | 0.407 | 0.039 | 0.324 | 0.122 | ||
| Truncated foot length | 0.561 | 0.003 | 0.559 | 0.004 | ||
| AHI | −0.341 | 0.088 | −0.362 | 0.083 | ||
| Standing position | Foot length | 0.373 | 0.061 | 0.299 | 0.155 | |
| Foot width | 0.440 | 0.025 | 0.440 | 0.031 | ||
| Navicular height | 0.224 | 0.271 | 0.137 | 0.522 | ||
| Dorsum height at 50% of the foot length | 0.382 | 0.054 | 0.295 | 0.161 | ||
| Truncated foot length | 0.536 | 0.005 | 0.522 | 0.009 | ||
| AHI | −0.151 | 0.462 | −0.143 | 0.506 | ||
| Flexor strength of the other toes | Sitting position | Foot length | 0.265 | 0.191 | 0.581 | 0.003 |
| Foot width | 0.316 | 0.115 | 0.415 | 0.044 | ||
| Navicular height | −0.306 | 0.129 | −0.279 | 0.186 | ||
| Dorsum height at 50% of the foot length | 0.181 | 0.377 | 0.341 | 0.103 | ||
| Truncated foot length | 0.403 | 0.041 | 0.683 | 0.000 | ||
| AHI | −0.368 | 0.065 | −0.415 | 0.044 | ||
| Standing position | Foot length | 0.243 | 0.231 | 0.546 | 0.006 | |
| Foot width | 0.309 | 0.125 | 0.472 | 0.020 | ||
| Navicular height | 0.131 | 0.525 | 0.167 | 0.434 | ||
| Dorsum height at 50% of the foot length | 0.174 | 0.395 | 0.294 | 0.164 | ||
| Truncated foot length | 0.344 | 0.085 | 0.625 | 0.001 | ||
| AHI | −0.157 | 0.443 | −0.186 | 0.383 |
| Position | Foot Morphology | r | p-Value | r (Adjusted) | p-Value |
|---|---|---|---|---|---|
| Sitting position | Foot length | 0.141 | 0.491 | 0.091 | 0.673 |
| Foot width | 0.550 | 0.004 | 0.600 | 0.002 | |
| Navicular height | 0.065 | 0.753 | −0.028 | 0.898 | |
| Dorsum height at 50% of the foot length | 0.144 | 0.481 | 0.071 | 0.741 | |
| Truncated foot length | 0.194 | 0.342 | 0.169 | 0.429 | |
| AHI | −0.090 | 0.662 | −0.130 | 0.544 | |
| Standing position | Foot length | 0.110 | 0.593 | 0.039 | 0.855 |
| Foot width | 0.399 | 0.044 | 0.499 | 0.013 | |
| Navicular height | 0.135 | 0.510 | 0.054 | 0.801 | |
| Dorsum height at 50% of the foot length | 0.304 | 0.131 | 0.275 | 0.194 | |
| Truncated foot length | 0.298 | 0.139 | 0.304 | 0.148 | |
| AHI | 0.027 | 0.897 | 0.020 | 0.925 |
| Variables | Differences in Foot Length | Differences in Foot Width | Differences in Navicular Height | Differences in Dorsum Height | Differences in Truncated Foot Length | Differences in AHI |
|---|---|---|---|---|---|---|
| Flexor strength of the first toe | −0.068 | −0.051 | −0.332 | −0.024 | −0.156 | −0.186 |
| Flexor strength of the other toes | −0.052 | −0.033 | −0.425 * | 0.003 | −0.221 | −0.184 |
| Metatarsophalangeal joint flexor strength | −0.212 | −0.515 ** | −0.086 | −0.367 | 0.342 | −0.160 |
| Variables | B | SE | β | t | p | |
|---|---|---|---|---|---|---|
| Flexor strength of the first toe | Constant | −2.799 | 1.311 | |||
| Truncated foot length in sitting | 0.230 | 0.069 | 0.561 | 3.316 | 0.003 | |
| Flexor strength of the other toes | Constant | −0.274 | 0.810 | |||
| Differences in navicular height | −0.480 | 0.125 | −0.756 | −3.853 | 0.001 | |
| Truncated foot length in sitting | 0.155 | 0.046 | 0.573 | 3.405 | 0.003 | |
| Navicular height in standing | −0.298 | 0.115 | −0.551 | −2.598 | 0.016 | |
| Metatarsophalangeal joint flexor strength | Constant | −1.937 | 1.530 | |||
| Foot width in sitting | 0.356 | 0.150 | 0.407 | 2.371 | 0.026 | |
| Differences in foot width | −0.955 | 0.439 | −0.373 | −2.175 | 0.040 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiao, S.; Zhang, X.; Deng, L.; Zhang, S.; Cui, K.; Fu, W. Relationships between Foot Morphology and Foot Muscle Strength in Healthy Adults. Int. J. Environ. Res. Public Health 2020, 17, 1274. https://doi.org/10.3390/ijerph17041274
Xiao S, Zhang X, Deng L, Zhang S, Cui K, Fu W. Relationships between Foot Morphology and Foot Muscle Strength in Healthy Adults. International Journal of Environmental Research and Public Health. 2020; 17(4):1274. https://doi.org/10.3390/ijerph17041274
Chicago/Turabian StyleXiao, Songlin, Xini Zhang, Liqin Deng, Shen Zhang, Kedong Cui, and Weijie Fu. 2020. "Relationships between Foot Morphology and Foot Muscle Strength in Healthy Adults" International Journal of Environmental Research and Public Health 17, no. 4: 1274. https://doi.org/10.3390/ijerph17041274