The Use of Stents in Children with Nasolacrimal Duct Obstruction Requiring Surgical Intervention: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategies
2.2. Eligibility Criteria
2.3. Study Outcomes
2.4. Screening and Data Extraction
2.5. Quality Assessment
3. Results
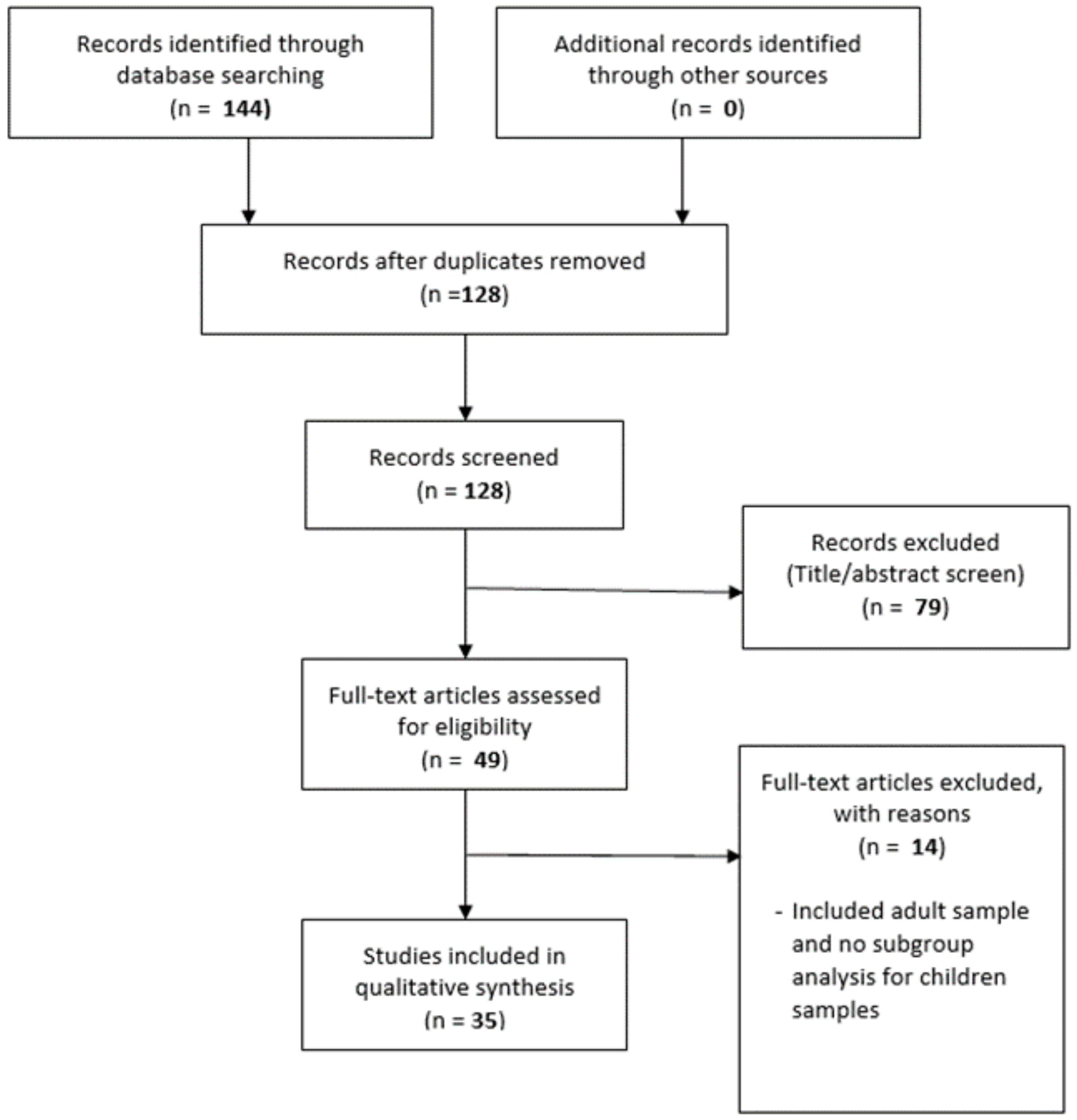
3.1. Literature Search
3.2. Description of the Studies
3.3. Outcomes
3.4. Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ffooks, O.O. Dacryocystitis in Infancy. Br. J. Ophthalmol. 1962, 46, 422–434. [Google Scholar] [CrossRef] [Green Version]
- Cassady, J.V. Developmental anatomy of nasolacrimal duct. AMA Arch. Ophthalmol. 1952, 47, 141–158. [Google Scholar] [CrossRef] [PubMed]
- Moscato, E.E.; Kelly, J.P.; Weiss, A. Developmental anatomy of the nasolacrimal duct: Implications for congenital obstruction. Ophthalmology 2010, 117, 2430–2434. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Kakizaki, H.; Chan, W.O.; Selva, D. Management of congenital nasolacrimal duct obstruction. Acta Ophthalmol. 2010, 88, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Karti, O.; Karahan, E.; Acan, D.; Kusbeci, T. The natural process of congenital nasolacrimal duct obstruction and effect of lacrimal sac massage. Int. Ophthalmol. 2016, 36, 845–849. [Google Scholar] [CrossRef] [PubMed]
- Avram, E. Insights in the treatment of congenital nasolacrimal duct obstruction. Rom. J. Ophthalmol. 2017, 61, 101–106. [Google Scholar] [CrossRef]
- Casady, D.R.; Meyer, D.R.; Simon, J.W.; Stasior, G.O.; Zobal-Ratner, J.L. Stepwise treatment paradigm for congenital nasolacrimal duct obstruction. Ophthal. Plast. Recons. 2006, 22, 243–247. [Google Scholar] [CrossRef]
- Yu, G.; Wu, Q.; Lin, Q.; Liu, W.; Qi, Y.; Quan, X.J.; Cao, W.H.; Bai, D.Y.; Zhang, C.Y.; Wang, Y. Lacrimal intubation with the Ritleng system in congenital nasolacrimal duct obstruction in children. J. Ophthalmol. 2008, 44, 887–891. [Google Scholar]
- Huang, Y.H.; Liao, S.L.; Lin, L.L. Balloon dacryocystoplasty and monocanalicular intubation with Monoka tubes in the treatment of congenital nasolacrimal duct obstruction. Graefes Arch. Clin Exp. Ophthalmol. 2009, 247, 795–799. [Google Scholar] [CrossRef]
- Engel, J.M.; Hichie-Schmidt, C.; Khammar, A.; Ostfeld, B.M.; Vyas, A.; Ticho, B.H. Monocanalicular silastic intubation for the initial correction of congenital nasolacrimal duct obstruction. J. AAPOS 2007, 11, 183–186. [Google Scholar] [CrossRef]
- Kominek, P.; Cervenka, S.; Matousek, P.; Pniak, T.; Zelenik, K. Primary pediatric endonasal dacryocystorhinostomy—A review of 58 procedures. Int. J. Pediatr. Otorhinolaryngol. 2010, 74, 661–664. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: West Sussex, England, 2011. [Google Scholar]
- Thomas, H. Quality assessment tool for quantitative studies. In Effective Public Health Practice Project; McMaster University: Toronto, ON, Canada, 2012. [Google Scholar]
- Abdulwahid, M.A.; Booth, A.; Kuczawski, M.; Mason, S.M. The impact of senior doctor assessment at triage on emergency department performance measures: Systematic review and meta-analysis of comparative studies. Emerg. Med. J. 2016, 33, 504–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sagar-Ouriaghli, I.; Godfrey, E.; Bridge, L.; Meade, L.; Brown, J.S.L. Improving Mental Health Service Utilization Among Men: A Systematic Review and Synthesis of Behavior Change Techniques Within Interventions Targeting Help-Seeking. Am. J. Mens Health 2019, 13. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.; Yoward, S.; Dawson, P. The Role of Physiotherapy Extended Scope Practitioners in Musculoskeletal care with Focus on Decision Making and Clinical Outcomes: A Systematic Review of Quantitative and Qualitative Research. Musculoskelet. Care 2017, 15, 91–103. [Google Scholar] [CrossRef]
- Andalib, D.; Gharabaghi, D.; Nabai, R.; Abbaszadeh, M. Monocanalicular versus bicanalicular silicone intubation for congenital nasolacrimal duct obstruction. J. AAPOS 2010, 14, 421–424. [Google Scholar] [CrossRef]
- Andalib, D.; Mansoori, H.A. Comparison between monocanalicular and pushed monocanalicular silicone intubation in the treatment of congenital nasolacrimal duct obstruction. Int. J. Ophthalmol. 2014, 7, 1039–1042. [Google Scholar]
- Ceylan, K.; Yuksel, D.; Duman, S.; Samim, E. Comparison of two endoscopically assisted procedures in primary surgical treatment of congenital nasolacrimal duct obstruction in children older than 3 years: Balloon dilatation and bicanalicular silicone tube intubation. Int. J. Pediatr. Otorhinolaryngol. 2007, 71, 11–17. [Google Scholar] [CrossRef]
- Elsawaby, E.A.; El Essawy, R.A.; Abdelbaky, S.H.; Ismail, Y.M. Pushed monocanalicular intubation versus probing as a primary management for congenital nasolacrimal obstruction. Clin. Ophthalmol. 2016, 10, 1487–1493. [Google Scholar]
- Kominek, P.; Cervenka, S.; Matousek, P. Does the length of intubation affect the success of treatment for congenital nasolacrimal duct obstruction? Ophthal. Plast. Reconstr. Surg. 2010, 26, 103–105. [Google Scholar] [CrossRef]
- Eshraghi, B.; Jamshidian-Tehrani, M.; Mirmohammadsadeghi, A. Comparison of the success rate between monocanalicular and bicanalicular intubations in incomplete complex congenital nasolacrimal duct obstruction. Orbit 2017, 36, 215–217. [Google Scholar] [CrossRef] [PubMed]
- Fayet, B.; Racy, E.; Ruban, J.M.; Katowitz, J. Pushed monocanalicular intubation. Pitfalls, deleterious side effects, and complications. J. Fr. Ophtalmol. 2011, 34, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Ahn, J.; Lee, J.M.; Park, M.; Baek, S. Clinical effectiveness of monocanalicular and bicanalicular silicone intubation for congenital nasolacrimal duct obstruction. J. Craniofac. Surg. 2012, 23, 1010–1014. [Google Scholar] [CrossRef] [PubMed]
- Kominek, P.; Cervenka, S.; Pniak, T.; Zelenik, K.; Tomaskova, H.; Matousek, P. Monocanalicular versus bicanalicular intubation in the treatment of congenital nasolacrimal duct obstruction. Graefes Arch. Clin. Experim. Ophthalmol. 2011, 249, 1729–1733. [Google Scholar] [CrossRef] [Green Version]
- Eshraghi, B.; Khalilipour, E.; Ameli, K.; Bazvand, F.; Mirmohammadsadeghi, A. Pushed monocanalicular intubation versus probing for the treatment of simple and incomplete complex types of congenital nasolacrimal duct obstruction in children older than 18 months old. Orbit 2017, 36, 218–222. [Google Scholar] [CrossRef]
- Al-Faky, Y.H.; Al-Sobaie, N.; Mousa, A.; Al-Odan, H.; Al-Huthail, R.; Osman, E.; Al-Mosallam, A.R. Evaluation of treatment modalities and prognostic factors in children with congenital nasolacrimal duct obstruction. J. AAPOS 2012, 16, 53–57. [Google Scholar] [CrossRef]
- Kaufman, L.M.; Guay-Bhatia, L.A. Monocanalicular intubation with Monoka tubes for the treatment of congenital nasolacrimal duct obstruction. Ophthalmology 1998, 105, 336–341. [Google Scholar] [CrossRef]
- Rajabi, M.T.; Zavarzadeh, N.; Mahmoudi, A.; Johari, M.K.; Hosseini, S.S.; Abrishami, Y.; Rajabi, M.B. Bicanalicular versus monocanalicular intubation after failed probing in congenital nasolacrimal duct obstruction. Int. J. Ophthalmol. 2016, 9, 1466–1470. [Google Scholar]
- Khatib, L.; Nazemzadeh, M.; Revere, K.; Katowitz, W.R.; Katowitz, J.A. Use of the Masterka for complex nasolacrimal duct obstruction in children. J. Am. Assoc. Pediatr. Ophthalmol. Strabism. 2017, 21, 380–383. [Google Scholar] [CrossRef]
- Okumuş, S.; Öner, V.; Durucu, C.; Coşkun, E.; Aksoy, Ü.; Durucu, E.; Şahin, L.; Erbağcı, I. Nasolacrimal duct intubation in the treatment of congenital nasolacrimal duct obstruction in older children. Eye 2016, 30, 85. [Google Scholar] [CrossRef] [Green Version]
- Orhan, M.; Onerci, M. Intranasal endoscopic silicone intubation for congenital obstruction of the nasolacrimal duct in children. Int. J. Pediatr. Otorhinolaryngol. 1997, 41, 273–278. [Google Scholar] [CrossRef]
- Eshraghi, B.; Aghajani, A.; Kasaei, A.; Tabatabaei, Z.; Akbari, M.; Fard, M.A. “Pushed” stent intubation for treatment of complex congenital nasolacrimal duct obstruction. Eur. J. Ophthalmol. 2014, 24, 650–654. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.J.; Gupta, H.; Naik, M.N.; Honavar, S.G. Endoscopic guided single self-linking silicone stent in pediatric external dacryocystorhinostomy. Minim. Invasive Ther. Allied. Technol. 2013, 22, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Dotan, G.; Ohana, O.; Leibovitch, I.; Stolovitch, C. Early loss of monocanalicular silicone tubes in congenital nasolacrimal duct obstruction: Incidence, predictors, and effect on outcome. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 301–304. [Google Scholar] [CrossRef]
- El-Essawy, R. Effect of timing of silicone tube removal on the result of duct intubation in children with congenital nasolacrimal duct obstruction. Ophthal. Plast. Reconstr. Surg. 2013, 29, 48–50. [Google Scholar] [CrossRef]
- Fayet, B.; Katowitz, W.R.; Racy, E.; Ruban, J.M.; Katowitz, J.A. Pushed monocanalicularintubation: An alternative stenting system for the management of congenital nasolacrimal duct obstructions. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2012, 16, 468–472. [Google Scholar] [CrossRef]
- Eloy, P.; Leruth, E.; Cailliau, A.; Collet, S.; Bertrand, B.; Rombaux, P. Pediatric endonasal endoscopic dacryocystorhinostomy. Int. J. Pediatr. Otorhinolaryngol. 2009, 73, 867–871. [Google Scholar] [CrossRef]
- Han, J.Y.; Lee, H.; Chang, M.; Park, M.; Lee, J.S.; Baek, S. Clinical Effectiveness of Monocanalicular Silicone Intubation for Congenital Nasolacrimal Duct Obstruction Under Nasal Endoscopic Visualization of the Terminal End of the Obstructed Nasolacrimal Duct. J. Craniof. Surg. 2015, 26, 1328–1331. [Google Scholar] [CrossRef]
- Nemet, A.Y.; Fung, A.; Martin, P.A.; Benger, R.; Kourt, G.; Danks, J.J.; Tong, J.C. Lacrimal drainage obstruction and dacryocystorhinostomy in children. Eye (Lond.) 2008, 22, 918–924. [Google Scholar] [CrossRef]
- Napier, M.L.; Armstrong, D.J.; McLoone, S.F.; McLoone, E.M. Congenital nasolacrimal duct obstruction: Comparison of two different treatment algorithms. J. Pediat. Ophth. Strab. 2016, 53, 285–291. [Google Scholar] [CrossRef]
- Yazici, B.; Akarsu, C.; Salkaya, M. Silicone intubation with the Ritleng method in children with congenital nasolacrimal duct obstruction. J. AAPOS 2006, 10, 328–332. [Google Scholar] [CrossRef]
- Pelit, A.; Caylakli, F.; Yaycioglu, R.A.; Akova, Y. Silicone intubation with the Ritleng method using intranasal endoscopy to treat congenital nasolacrimal duct obstruction. Int. J. Pediatr. Otorhinolaryngol. 2009, 73, 1536–1538. [Google Scholar] [CrossRef] [PubMed]
- Yalaz, M.; Ozcan, A.A.; Akcali, C.; Soylu, L. Lacrimal intubation with the Ritleng system in recurrent congenital nasolacrimal duct obstruction in children. ORL J. Otorhinolaryngol. Relat. Spec. 2004, 66, 35–37. [Google Scholar] [CrossRef] [PubMed]
- Fayet, B.; Racy, E.; Ruban, J.-M.; Katowitz, J. “Pushed” monocanalicular intubation in children under general anesthesia with spontaneous ventilation. A. preliminary report. J. Fr. Ophtalmol. 2010, 33, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Pe, M.R.; Langford, J.D.; Linberg, J.V.; Schwartz, T.L.; Sondhi, N. Ritleng intubation system for treatment of congenital nasolacrimal duct obstruction. Arch. Ophthalmol. 1998, 116, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Fayet, B.; Racy, E.; Renard, G. Pushed monocanalicularintubation: A preliminary report. J. Fr. Ophtalmol. 2010, 33, 145–151. [Google Scholar] [CrossRef]
- Abdu, L.; Salisu, A.D. Pattern and outcome of surgical management of nasolachrymal duct obstruction in children: A five year review. Ann. Afr. Med. 2014, 13, 130–133. [Google Scholar] [CrossRef] [Green Version]
- Kushner, B.J. The management of nasolacrimal duct obstruction in children between 18 months and 4 years old. J. AAPOS. 1998, 2, 57–60. [Google Scholar] [CrossRef]
- Leone, C.R., Jr. The management of pediatric lacrimal problems. Ophthalm. Plast. Reconstr. Surg. 1989, 5, 34–39. [Google Scholar] [CrossRef]
- Gupta, N.; Singla, P.; Kumar, S.; Ganesh, S.; Dhawan, N.; Sobti, P.; Aggarwal, S. Role of dacryoendoscopy in refractory cases of congenital nasolacrimal duct obstruction. Orbit 2019. [Google Scholar] [CrossRef]
- Maheshwari, R. Success rate and cause of failure for late probing for congenital nasolacrimal duct obstruction. J. Pediat. Ophth. Strab. 2008, 45, 168–171. [Google Scholar] [CrossRef]
- Kashkouli, M.B.; Beigi, B.; Parvaresh, M.M.; Kassaee, A.; Tabatabaee, Z. Late and very late initial probing for congenital nasolacrimal duct obstruction: What is the cause of failure? Br. J. Ophthalmol. 2003, 87, 1151–1153. [Google Scholar] [CrossRef] [Green Version]
- Yu, G.; Hu, M.; Wu, Q.; Cao, W.H.; Fan, Y.W.; Lin, Q.; Liu, W. Factors affected therapeutic results in treatment of children congenital nasolacrimal duct obstruction by Ritleng lacrimal intubation. Zhonghua Yan Ke Za Zhi 2012, 48, 423–427. [Google Scholar] [PubMed]
- Robb, R.M. Probing and irrigation for congenital nasolacrimal duct obstruction. Arch. Ophthalmol. 1986, 104, 378–379. [Google Scholar] [CrossRef] [PubMed]
- Chong, K.K.; Lai, F.H.; Ho, M.; Luk, A.; Wong, B.W.; Young, A. Randomized trial on silicone intubation in endoscopic mechanical dacryocystorhinostomy (SEND) for primary nasolacrimal duct obstruction. Ophthalmology 2013, 120, 2139–2145. [Google Scholar] [CrossRef] [PubMed]
- Cannon, P.S.; Chan, W.; Selva, D. Incidence of canalicular closure with endonasal dacryocystorhinostomy without intubation in primary nasolacrimal duct obstruction. Ophthalmology 2013, 120, 1688–1692. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Ahn, J.; Shin, H.H.; Park, M.; Baek, S. Effectiveness of primary monocanalicularnasal intubation with Monoka tubes and nasal endoscopic findings for congenital nasolacrimal duct obstruction with enlarged lacrimal sac and chronic dacryocystitis. J. Craniof. Surg. 2012, 23, 1638–1641. [Google Scholar] [CrossRef]
- Al-Faky, Y.H.; Mousa, A.; Kalantan, H.; Al-Otaibi, A.; Alodan, H.; Alsuhaibani, A.H.A. Prospective, randomised comparison of probing versus bicanalicular silastic intubation for congenital nasolacrimal duct obstruction. Br. J. Ophthalmol. 2015, 99, 246–250. [Google Scholar] [CrossRef]
- Lim, C.S.; Martin, F.; Beckenham, T.; Cumming, R.G. Nasolacrimal duct obstruction in children: Outcome of intubation. J. Am. Assoc. Pediatr. Ophthalmol. Strab. 2004, 8, 466–472. [Google Scholar] [CrossRef]
- Peterson, N.J.; Weaver, R.G.; Yeatts, R.P. Effect of short-duration silicone intubation in congenital nasolacrimal duct obstruction. Ophthalmic. Plast. Reconstr. Surg. 2008, 24, 167–171. [Google Scholar] [CrossRef]
- Dortzbach, R.K.; France, T.D.; Kushner, B.J.; Gonnering, R.S. Silicone intubation for obstruction of the nasolacrimal duct in children. Ophthalmic. Plast. Reconstr. Surg. 1982, 94, 585–590. [Google Scholar] [CrossRef]
- Nowinski, T.S.; Flanagan, J.C.; Mauriello, J. Pediatric dacryocystorhinostomy. Arch. Ophthalmol. 1985, 103, 1226–1228. [Google Scholar] [CrossRef] [PubMed]
- Young, J.D.; MacEwen, C.J. Managing congenital lacrimal obstruction in general practice. BMJ 1997, 315, 293–296. [Google Scholar] [CrossRef]
- Ciftci, F.; Ersanl, D.; Civelek, L.; Baloglu, H.; Karaday, K.; Gungor, A. Histopathologic changes in the lacrimal sac of dacryocystorhinostomy patients with and without silicone intubation. Ophthalmic. Plast. Reconstr. Surg. 2005, 21, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Kim, T.H. Changes in cytokines in tears after endoscopic endonasal dacryocystorhinostomy for primary acquired nasolacrimal duct obstruction. Eye 2014, 28, 600–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, M.; Wu, Q.; Fan, Y.W.; Cao, W.W.; Lin, Q.; Yu, G. Comparison of balloon catheter dilatation and silicon intubation as the secondary treatment for congenital nasolacrimal duct obstruction after failed primary probing. Zhonghua Yan Ke Za Zhi 2016, 52, 123–128. [Google Scholar]


{kind=link}
| Study Design | First Author, Year | Country | Procedure | Number of Patients|Number of Eyes | Mean Age in mo/yr (min–max) | Gender in % (male) | Timing of Postoperative Stent Removal in d/wk/mo | Mean Follow–up in wk/mo (min–max) |
|---|---|---|---|---|---|---|---|---|
| Randomised controlled trials | Andalib, 2010 [18] | Iran | LI | 57|70 | MCI: 34.9mo | NR | 3mo | NR |
| (13–71mo) | ||||||||
| BCI: 38.7mo | ||||||||
| (14–84mo) | ||||||||
| Andalib, 2014 [19] | Iran | LI | 49|53 | MCI: 26.25mo | NR | 3mo | NR | |
| (13–49mo) | ||||||||
| PMCI: 26.85mo (16–68mo) | ||||||||
| Ceylan, 2007 [20] | Turkey | LI | 20|24 (BCI) | 50.8mo (36–120mo) | NR | Average 6.2 mo | NR (12mo–NR) | |
| Elsawaby, 2016 * [21] | Egypt | LI | 27|30 | 14.85mo | 50 | At least 3wk | 16wk (NR) | |
| (7–30mo) | ||||||||
| Kominek, 2010 [22] | Czech Republic | LI | 83| 95 (Group 1: 42|48; Group 2:41|47) | NR (15–30mo) | NR | Group 1: 2mo | NR (NR–6mo) | |
| Group 2: 5mo | ||||||||
| Non–randomised controlled trials | Eshraghi, 2017a [23] | Iran | LI | 99|99 (MCI:52|52; BCI:47|47) | 3.56yr | 57.6 | 3mo | NR (NR–12mo) |
| (1.3–10yr) | ||||||||
| Fayet, 2011 # [24] | France | LI | 68|68 (Group 2:6|6; Group 3:62|62) | Group 2: NR | NR | Group 2: 39d Group 3: 29d | Group 2: 14wk (3–30wk) | |
| (1–9yr) | ||||||||
| Group 3: NR | Group 3: 16wk (3–74wk) | |||||||
| (1–6yr) | ||||||||
| Lee, 2012 [25] | South Korea | LI | 46|60 (BCI:22|30; MCI:24|30) | BCI:23.3mo | 52.2 | BCI: 5–22wk | BCI: 16.4 wk (NR) | |
| (9–52mo) | ||||||||
| MCI: 23.1mo | MCI:5–15wk | MCI: 11.6 wk (NR) | ||||||
| (8–62mo) | ||||||||
| Kominek, 2011 [26] | Czech Republic | LI | 53|70 (BCI:24|35; MCI:29|35) | NR (10–36mo) | 44.3 | 3–4mo | NR (NR–6mo) | |
| Eshraghi, 2017b [27] | Iran | LI | 45|45 (LI only, study compared LI and probing) | 28mo (NR) | NR | Average 9.2 wk | NR (1wk–6mo) | |
| Retrospective with comparative groups | Al–Faky, 2012 $ [28] | Iran | LI | 350|454 | 32.6mo | 46 | 3mo | 15.3mo |
| (12–132mo) | (3–108mo) | |||||||
| Kaufman, 1998 & [29] | United States | LI | 64|73 (Prospective:39|48 | 31.8mo | NR | 4–6mo | NR (3–12wk) | |
| Retrospective:25|25) | (12–87mo) | |||||||
| Rajabi, 2016 [30] | Iran | LI | 338|338 (Crawford:248|248; Monoka:52|52; Masteka:38|38) | NR | 56.1 | 3mo | Schedule follow up 3mo | |
| (1–4yr) | ||||||||
| Khatib, 2017 [31] | United States | LI | 53|72 (complex; simple) | 22mo | NR | 2–3mo | 14mo | |
| (5–65mo) | (6–29mo) | |||||||
| Retrospective/prospective with single group/non–comparative/consecutive cases | Okumus, 2016 [32] | Turkey | LI | 30|30 | 10.7yr | 60 | Average 4.6mo | 8.8mo |
| (7–15yr) | (6–16mo) | |||||||
| Orhan, 1997 [33] | Turkey | LI | 16|18 | 25mo | 43.8 | 4–7mo | 12mo | |
| (18–48mo) | (4–24mo) | |||||||
| Eshraghi, 2014 [34] | Iran | LI | 44|44 | 3.2yr (NR) | 45.5 | 2mo | 9mo | |
| (6.5–13mo) | ||||||||
| Ali, 2013 [35] | India | ExtDCR | 10|11 | 9.4yr | 30 | 12–16wk | NR (3–6mo) | |
| (6–15yr) | ||||||||
| Engel, 2007 [10] | United States | LI | 635|803 | 18mo | 45 | Median of 8wk | Median of 12wk | |
| (6.5–103.8mo) | ||||||||
| Dotan, 2015 [36] | Israel | LI | 46|54 | 37.6mo (NR) | 52.2 | 4–6mo | NR | |
| El–Essawy, 2013 [37] | Egypt | LI | 192|236 | 21.2mo | 51 | 3–6mo | 5mo (3–16mo) | |
| (8–48mo) | ||||||||
| Fayet, 2012 [38] | France | LI | 88|110 | 2.4yr | NR | 3wk | 33.7wk (4–139wk) | |
| (1–8yr) | ||||||||
| Casady, 2006 [7] | United States | LI | NR|7 | NR | NR | 3–3.5mo | NR (4–6wk) | |
| (12–18mo) | ||||||||
| Eloy, 2009 [39] | Belgium | EDCR | 8|10 | 4.3yr | 87.5 | 1–3mo | 10.5mo | |
| (8mo–9yr) | (6–15wk) | |||||||
| Han, 2015 [40] | South Korea | LI | 56|77 | 29.8mo | 53.6 | 2–3mo | NR | |
| (6mo–12yr) | ||||||||
| Nemet, 2008 [41] | Australia | ExtDCR/ EDCR | 82|104 | 6.6yr (NR) | 51.2 | 6mo | 1.44yr (6mo–8yr) | |
| Napier, 2016 [42] | United Kingdom | LI | 177|246 | 2.1yr (0–9.8yr) | 50.4 | At least 12wk | NR (6–12wk) | |
| Yazici, 2006 [43] | Turkey | LI | 42|50 | 37.3mo | 47.6 | 3mo | 18.1mo | |
| (9mo–7yr) | (3–48mo) | |||||||
| Pelit, 2009 [44] | Turkey | LI | 30|34 | 5yr (2–10yr) | 53.3 | 6mo | 40.32mo (12–96mo) | |
| Yalaz, 2004 [45] | Turkey | LI | 26|29 | 4.85yr (2–12yr) | 46.2 | 6mo | 8.3mo (6–25mo) | |
| Fayet, 2010a [46] | France | LI | 14|18 | 26.2mo (14–46mo) | NR | Average of 34d | 8.7wk (3–26wk) | |
| Pe, 1998 [47] | United States | LI | 28|34 | 19.5mo (5mo–5yr 3mo) | 39.3 | 2–6mo | NR (NR) | |
| Fayet, 2010b [48] | France | LI | 4|6 | 33mo (30–37mo) | NR | 3wk | NR (2–3mo) | |
| Huang 2009 [9] | Taiwan | Balloon dacryocystoplasty and LI (MCI) | 25|33 | 3.5yr | 60 | 4–6mo | 6mo | |
| Five year record review (descriptive study) | Abdu, 2014 [49] | Nigeria | ExtDCR | 17|NA | NR (NR–15yr) | 52.9 | 6wk | Up to 1yr |
| First Author, Year | Criteria for Successful Outcome | Overall Successful Outcome % | Post–Operative Complication |
|---|---|---|---|
| Andalib, 2010 [18] | Munk score of 0 or 1 at 3 months after tube removal | MCI: 86.2 | None |
| BCI: 89 | |||
| Andalib, 2014 [19] | Complete resolution of epihora at 3 months after tube removal | MCI: 90 | Slit punctum in PMCI |
| PMCI: 50 | |||
| Ceylan, 2007 [20] | Complete remission of epiphora at 12 months, maintained for 4 months | 62.5 | Ocular irritation, false lumen in the inferior meatus, iatrogenic punctal laceration |
| Elsawaby, 2016 [21] | Munk’s score 0 or 1 after 3 months from surgery | 83.3 * | Corneal ulcer, epistaxis |
| Kominek, 2010 [22] | Fluorescein dye disappearance grade 0–1, corresponding to complete resolution of previous symptoms | Group 1(removal at 2 mo): 89.6 | None |
| Group 2 (removal at 6 mo): 91.5 | |||
| Eshraghi, 2017 [23] | Dye disappearance test grade 0–1 & complete resolution of symptom at 12 months’ follow up | MCI: 59.6 | Loss of tubes |
| BCI: 74.4 | |||
| Fayet, 2011 & [24] | Absence of epiphora, absence of mucous discharge | Group 2 (age 1–9 years): 100 | Group 2: none |
| Group 3 (age 1–6 years): 88.3 | Group 3: Loss of tube, keratitis | ||
| Lee, 2012 [25] | Complete disappearance of symptoms | BCI: 93.3 | Tube prolapse, punctal slitting |
| MCI: 90 | |||
| Kominek, 2011 [26] | Fluorescein dye disappearance test grade 0–1 = complete resolution from symptoms | BCI: 82.86 | Dislodging of tube, premature removal, loss of tube, slitting of punctum and canaliculi, granuloma pyogenicum, corneal erosion |
| MCI: 88.57 | |||
| Eshraghi, 2017b [27] | Complete absence of clinical signs and symptoms of congenital nasolacrimal duct obstruction at 6 months after the procedure | 73.3 | Epiphora with tubes in place |
| Al–Faky, 2012 [28] | Normal dye disappearance test, positive Jones primary dye test | 88 | NR |
| Kaufman, 1998 [29] | Negative dye disappearance test | 79 | Bilateral preseptal cellulitis, migration of punctal anchor into canaliculus, corneal abrasion, corneal ulcer, premature removal of tube |
| Rajabi, 2016 [30] | No sign and symptom of tearing or discharge | BCI:80.2 | Tube dislodging, spontaneous extrusion, corneal abrasion, punctual slitting due to cheese wiring, punctal plug migration to canaliculus |
| MCI:41.1 | |||
| Khatib, 2017 [31] | Complete resolution of symptoms, negative dye disappearance test | 75 | Early tube loss |
| Okumus, 2016 [32] | Complete resolution of previous signs and symptoms and DDT grade 0–1 | 73.3 | None |
| Orhan, 1997 [33] | Resolution of symptoms and previous signs | 100 | Epiphora with tubes in place |
| Eshraghi, 2014 [34] | Complete resolution or partial improvement | 82.6 | None |
| Ali, 2013 [35] | Resolution of symptoms | 91 | NR |
| Engel, 2007 [10] | Good clearance of fluorescein dye and/or absence of symptomatic testing | 96 | Conjunctival–corneal abrasion |
| Dotan, 2015 [36] | Complete resolution of all preoperative CNLDO symptoms and signs | 85 | Spontaneous tube loss |
| El–Essawy, 2013 [37] | Complete resolution of symptoms, no epiphora, no discharge, no increase tear lake | 82.2 | Cheesewiring of canaliculi, late postoperative granuloma formation |
| Fayet, 2012 [38] | Absence of symptoms after stent removal or loss | 85 | Keratitis, tube loss, epiphora with tubes in place |
| Casady, 2006 [7] | Complete resolution of symptoms | 100 | None |
| Eloy, 2009 [39] | Complete resolution of symptoms | 90 | Transient slight epiphora |
| Han, 2015 [40] | Disappearance of epiphora symptoms by a minimum of 2 months | 89.6 | Tube prolapse, tube loss |
| Nemet, 2008 [41] | Objective confirmation of free fluorescein flow to the nose | 95.2 | Jones tube placement |
| Napier, 2016 [42] | Complete resolution of symptoms and signs | 91.7 | NR |
| Yazici, 2006 [43] | Resolution of lacrimal symptoms and signs, normal tear meniscus, and in cooperative patients, normal dye disappearance test and/or patent nasolacrimal duct on irrigation at the last examination. | 86 | Slit punctum |
| Pelit, 2009 [44] | Complete resolution of previous lacrimal symptoms and signs | 100 | None |
| Yalaz, 2004 [45] | Relief from symptom and/or positive results in fluorescein dye disappearance test | 93.2 (initial intubation); | Granuloma |
| 100 (reintubation) | |||
| Fayet, 2010a [46] | Absence of epiphora, absence of mucous discharge | 88 | Mildly watery eye |
| Pe, 1998 [47] | Easy, uncomplicated retrieval of the Prolene guide thread during intubation; complete resolution of previous signs and symptoms and a normal result of the dye disappearance test | 97 | None |
| Fayet, 2010b [48] | Residual epiphora after ablation | 100 | None |
| Huang 2009 [9] | Complete resolution of symptoms and normal dye disappearance test | 97 | None |
| Abdu, 2014 [49] | Patent nasolacrimal duct 1 year after surgery | 88 | Extrusion of the tube, infection |
| First Author, Year | Selection Bias | Study Design | Confounders | Blinding | Data Collection Methods | Withdrawals and Dropouts | Global Rating |
|---|---|---|---|---|---|---|---|
| Andalib, 2010 [18] | S | S | S | W | S | S | M |
| Andalib, 2014 [19] | S | S | S | W | S | M | M |
| Ceylan, 2007 [20] | S | S | W | W | S | S | W |
| Elsawaby, 2016 [21] | S | S | W | W | S | S | W |
| Kominek, 2010 [22] | S | S | W | W | S | S | W |
| Eshraghi, 2017 [23] | S | M | W | W | S | S | W |
| Fayet, 2011 [24] | S | M | W | W | S | S | W |
| Lee, 2012 [25] | S | M | S | W | S | S | M |
| Kominek, 2011 [26] | S | M | W | W | S | S | W |
| Eshraghi, 2017b [27] | S | M | W | W | S | S | W |
| Al-Faky, 2012 [28] | S | M | W | W | S | NA | W |
| Kaufman, 1998 [29] | S | M | W | W | S | S | W |
| Rajabi, 2016 [30] | S | M | W | W | S | NA | W |
| Khatib, 2017 [31] | S | M | W | W | S | NA | W |
| Okumus, 2016 [32] | S | W | W | NA | S | S | W |
| Orhan, 1997 [33] | S | W | W | NA | S | S | W |
| Eshraghi, 2014 [34] | S | W | S | NA | S | S | M |
| Ali, 2013 [35] | S | W | W | NA | S | S | W |
| Engel, 2007 [10] | S | W | W | NA | S | NA | W |
| Dotan, 2015 [36] | S | W | W | NA | S | NA | W |
| El-Essawy, 2013 [37] | S | W | W | NA | S | NA | W |
| Fayet, 2012 [38] | S | W | W | NA | S | NA | W |
| Casady, 2006 [7] | S | W | W | NA | S | NA | W |
| Eloy, 2009 [39] | S | W | W | NA | S | NA | W |
| Han, 2015 [40] | S | W | W | NA | S | NA | W |
| Nemet, 2008 [41] | S | W | W | NA | S | NA | W |
| Napier, 2016 [42] | S | W | W | NA | S | NA | W |
| Yazici, 2006 [43] | S | W | W | NA | S | NA | W |
| Pelit, 2009 [44] | S | W | W | NA | S | NA | W |
| Yalaz, 2004 [45] | S | W | W | NA | S | NA | W |
| Fayet, 2010a [46] | S | W | W | NA | S | NA | W |
| Pe, 1998 [47] | S | W | W | NA | S | NA | W |
| Fayet, 2010b [48] | S | W | W | NA | S | NA | W |
| Huang 2009 [9] | S | W | W | NA | S | NA | W |
| Abdu, 2014 [49] | S | W | W | NA | S | NA | W |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tai, E.L.M.; Kueh, Y.C.; Abdullah, B. The Use of Stents in Children with Nasolacrimal Duct Obstruction Requiring Surgical Intervention: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 1067. https://doi.org/10.3390/ijerph17031067
Tai ELM, Kueh YC, Abdullah B. The Use of Stents in Children with Nasolacrimal Duct Obstruction Requiring Surgical Intervention: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(3):1067. https://doi.org/10.3390/ijerph17031067
Chicago/Turabian StyleTai, Evelyn Li Min, Yee Cheng Kueh, and Baharudin Abdullah. 2020. "The Use of Stents in Children with Nasolacrimal Duct Obstruction Requiring Surgical Intervention: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 3: 1067. https://doi.org/10.3390/ijerph17031067