Ethnic Variations in Nutritional Status among Preschool Children in Northern Vietnam: A Cross-Sectional Study


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Prevalence of Various Nutritional Statuses in Our Sample
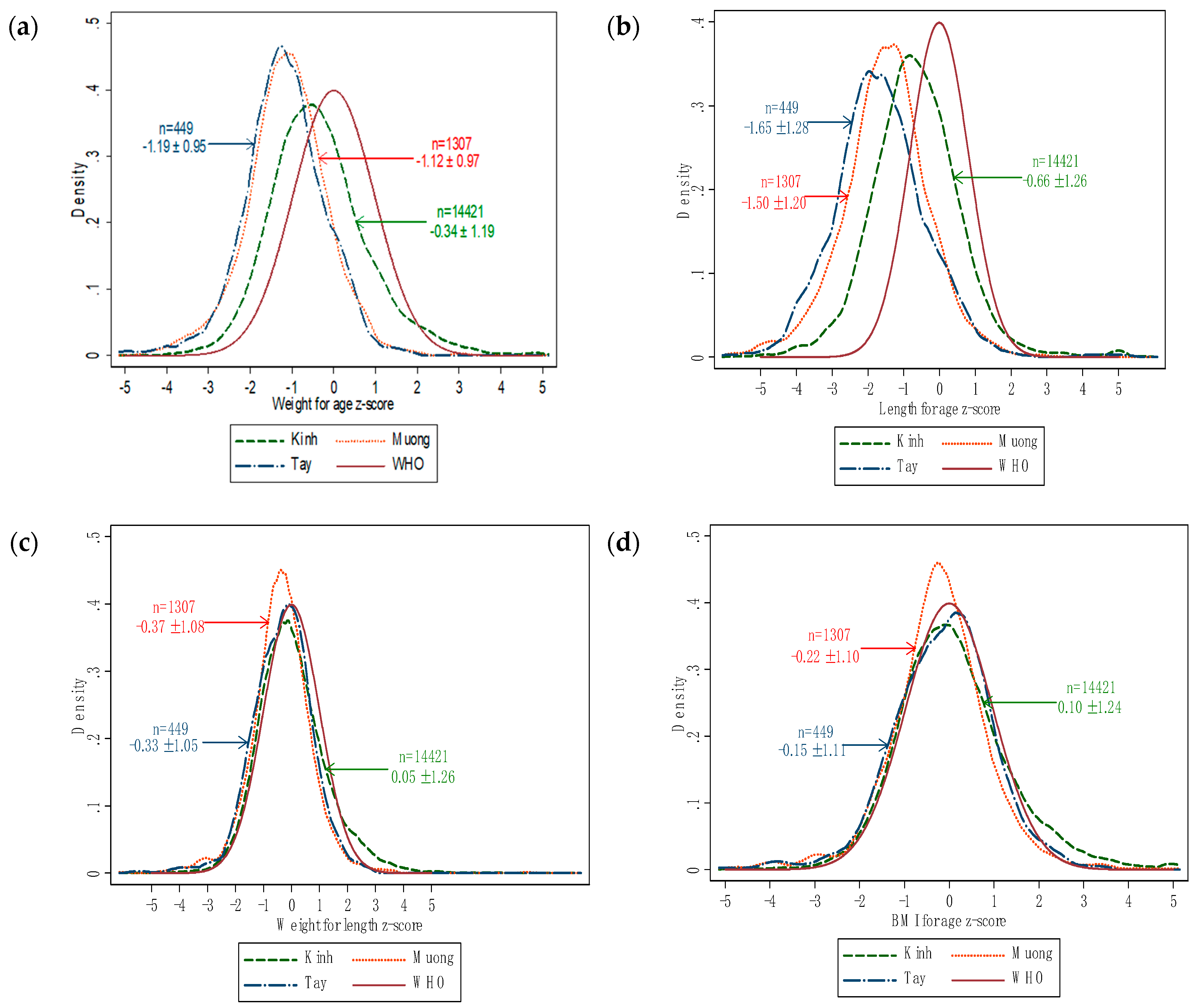
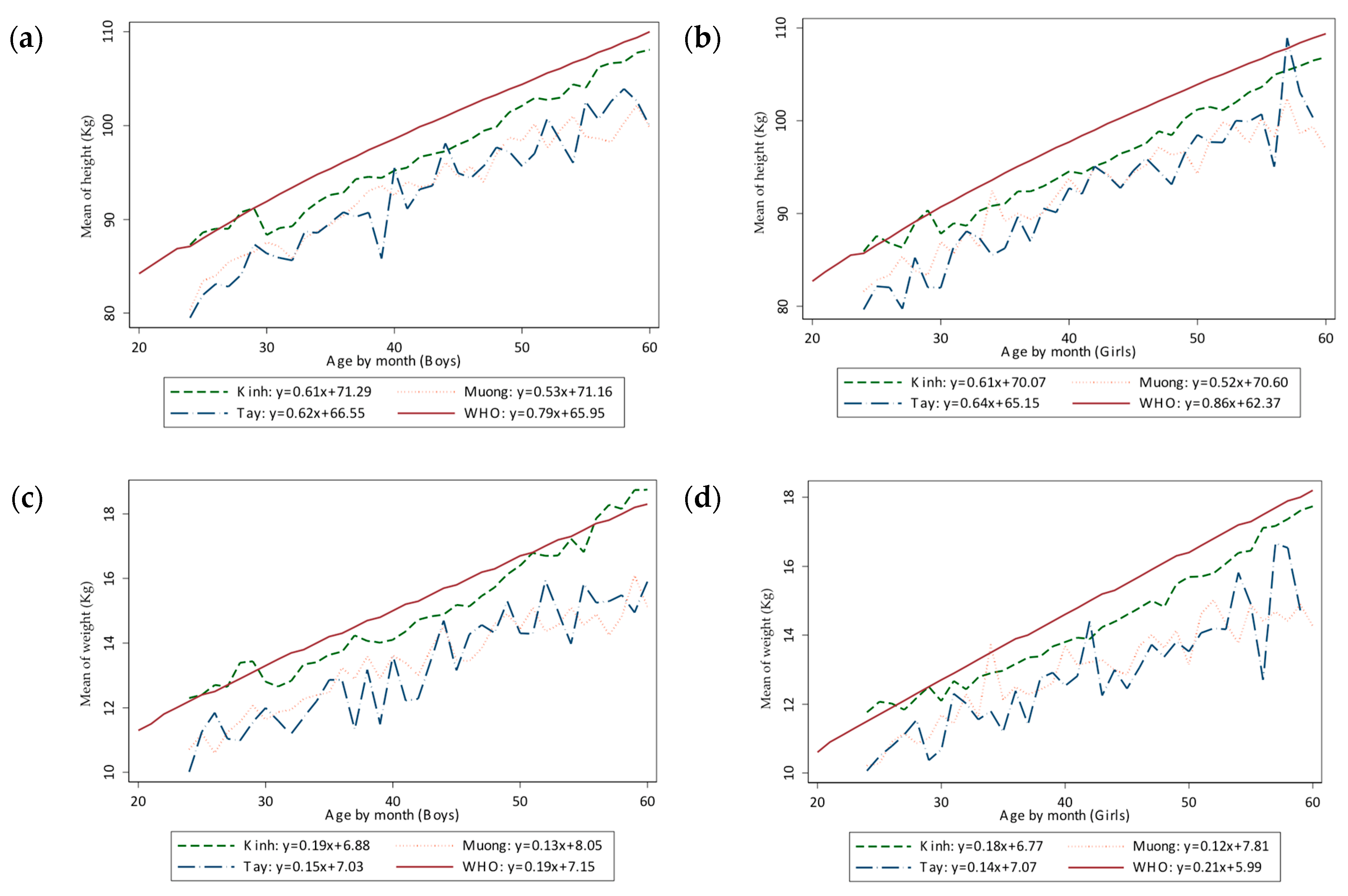
3.2. Comparison of the Main Anthropometric Indices of Preschool Children across Three Ethnicities
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Black, M.M.; Pérez-Escamilla, R.; Fernandez Rao, S. Integrating nutrition and child development interventions: Scientific basis, evidence of impact, and implementation considerations. Adv. Nutr. 2015, 6, 852–859. [Google Scholar] [CrossRef]
- Schoenmaker, C.; Juffer, F.; van IJzendoorn, M.H.; van den Dries, L.; Linting, M.; van der Voort, A.; Bakermans-Kranenburg, M.J. Cognitive and health-related outcomes after exposure to early malnutrition: The Leiden longitudinal study of international adoptees. Child. Youth Serv. Rev. 2015, 48, 80–86. [Google Scholar] [CrossRef]
- Kelsey, M.M.; Zaepfel, A.; Bjornstad, P.; Nadeau, K.J. Age-related consequences of childhood obesity. Gerontology 2014, 60, 222–228. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Double Burden of Malnutrition. 2016. Available online: https://www.who.int/nutrition/double-burden-malnutrition/en/ (accessed on 19 August 2019).
- Tzioumis, E.; Adair, L.S. Childhood dual burden of under-and overnutrition in low-and middle-income countries: A critical review. Food Nutr. Bull. 2014, 35, 230–243. [Google Scholar] [CrossRef] [PubMed]
- Pirgon, Ö.; Aslan, N. The role of urbanization in childhood obesity. J. Clin. Res. Pediatr. Endocrinol. 2015, 7, 163. [Google Scholar] [CrossRef]
- The World Bank. the World Bank in Vietnam. 2019. Available online: https://www.worldbank.org/en/country/vietnam/overview (accessed on 15 August 2019).
- Trinh, H.T.; Simioni, M.; Thomas-Agnan, C. A Fresh Look at the Nutrition Transition in Vietnam Using Semiparametric Modeling. 2017. Available online: https://www.tse-fr.eu/sites/default/files/TSE/documents/doc/wp/2017/wp_tse_842.pdf (accessed on 12 September 2019).
- Thi Thu Dieu, H.; Dibley, M.J.; Sibbritt, D.; Thi Minh Hanh, T. Prevalence of overweight and obesity in preschool children and associated socio-demographic factors in Ho Chi Minh City, Vietnam. Int. J. Pediatr. Obes. 2007, 2, 40–50. [Google Scholar] [CrossRef]
- Do, L.M.; Tran, T.K.; Eriksson, B.; Petzold, M.; Nguyen, C.T.; Ascher, H. Preschool overweight and obesity in urban and rural Vietnam: Differences in prevalence and associated factors. Glob. Health Action 2015, 8, 28615. [Google Scholar] [CrossRef]
- Unicef. Monitoring the Situation of Children and Women (Vietnam). 2014. Available online: https://data.unicef.org/country/vnm/ (accessed on 18 April 2019).
- Van Tam, V.; Nhan, N.H.; Tinh, H.Q.; Hung, N.P. The Impacts of Malnutrition Status and Relevant Factors on Preschool Children in Cao Ma Po Commune, Quan Ba District, Ha Giang Province. Available online: https://js.vnu.edu.vn/NST/article/view/3571 (accessed on 25 August 2019).
- Chuc, D.V.; Hung, N.X.; Trang, V.T.; Linh, D.V.; Khue, P.M. Nutritional Status of Children Aged 12 to 36 Months in a Rural District of Hungyen Province, Vietnam. BioMed Res. Int. 2019, 2019, e6293184. [Google Scholar] [CrossRef]
- Thu, N.T.T.; Tuyet, L.T. Anthropometric characteristics and nutritional status in 24–59 months children in Hanoi city, Thanhhoa province and Phutho province in 2018. Hnue J. Sci. 2018, 63, 3–9. [Google Scholar]
- Huynh, G.; Huynh, Q.H.N.; Nguyen, N.H.T.; Do, Q.T.; Van Tran, K. Malnutrition among 6–59-Month-Old Children at District 2 Hospital, Ho Chi Minh City, Vietnam: Prevalence and Associated Factors. BioMed Res. Int. 2019, 2019, 6921321. [Google Scholar] [CrossRef]
- General Statistics Office of Vietnam. Preliminary Report on the Population and Housing Census 2019. 2019. Available online: https://www.gso.gov.vn/default.aspx?tabid=512&idmid=5&ItemID=19279 (accessed on 8 September 2019).
- Unicef. Children in Vietnam. 2017. Available online: https://www.unicef.org/vietnam/children-viet-nam (accessed on 21 August 2019).
- World Health Organization. The WHO Child Growth Standards. 2019. Available online: https://www.who.int/childgrowth/standards/en/ (accessed on 22 August 2019).
- Kholmatova, K.; Gorbatova, M.; Kharkova, O.; Grjibovski, A. Cross-sectional studies: Planning, sample size, data analysis. Ekol. Cheloveka 2016, 2, 49–56. (In Russian) [Google Scholar]
- Helsinki, D. World Medical Association Declaration of Helsinki. Bull. World Health Organ. 2001, 79, 373–374. [Google Scholar]
- Guilmoto, C.Z.; Hoang, X.; Van, T.N. Recent increase in sex ratio at birth in Viet Nam. PLoS ONE 2009, 4, e4624. [Google Scholar] [CrossRef] [PubMed]
- General Statistics Office of Vietnam. Statistics Data. 2017. Available online: http://www.gso.gov.vn/default.aspx?tabid=714 (accessed on 2 September 2019).
- Biswas, S.; Bose, K.; Mukhopadhyay, A.; Bhadra, M. Prevalence of undernutrition among pre-school children of Chapra, Nadia District, West Bengal, India, measured by composite index of anthropometric failure (CIAF). Anthropol. Anz. 2009, 67, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Kavosi, E.; Rostami, Z.H.; Kavosi, Z.; Nasihatkon, A.; Moghadami, M.; Heidari, M. Prevalence and determinants of under-nutrition among children under six: A cross-sectional survey in Fars province, Iran. Int. J. Health Policy Manag. 2014, 3, 71. [Google Scholar] [CrossRef]
- Huong, L.T.; Xuan, L.T.T.; Phuong, L.H.; Huyen, D.T.T.; Rocklöv, J. Diet and nutritional status among children 24–59 months by seasons in a mountainous area of Northern Vietnam in 2012. Glob. Health Action 2014, 7, 23121. [Google Scholar] [CrossRef]
- Thang, N.M.; Popkin, B. Child malnutrition in Vietnam and its transition in an era of economic growth. J. Hum. Nutr. Diet. 2003, 16, 233–244. [Google Scholar] [CrossRef]
- Das, S.; Bose, K. Nutritional profile of preschool children: A review. Anthropologist 2012, 14, 467–472. [Google Scholar] [CrossRef]
- Bloem, M.W.; de Pee, S.; Le Hop, T.; Khan, N.C.; Laillou, A.; Moench-Pfanner, R.; Soekarjo, D.; Solon, J.A.; Theary, C. Key strategies to further reduce stunting in Southeast Asia: Lessons from the ASEAN countries workshop. Food Nutr. Bull. 2013, 34, S8–S16. [Google Scholar] [CrossRef]
- Giao, H.; Le An, P.; Truong Vien, N.; Van Khanh, T.; Quang Vinh, B. Stunting and Overweight among 12-24-Month-Old Children Receiving Vaccination in Ho Chi Minh City, Vietnam. BioMed Res. Int. 2019, 2019, 1547626. [Google Scholar] [CrossRef]
- Zhang, Y.; Huang, X.; Yang, Y.; Liu, X.; Yang, C.; Wang, A.; Wang, Y.; Zhou, H. Double burden of malnutrition among children under 5 in poor areas of China. PLoS ONE 2018, 13, e0204142. [Google Scholar] [CrossRef] [PubMed]
- Anwer, I.; Awan, J. Nutritional status comparison of rural with urban school children in Faisalabad District, Pakistan. Rural Remote Health 2003, 3, 130–136. [Google Scholar] [PubMed]
- Nouri Saeidlou, S.; Babaei, F.; Ayremlou, P. Malnutrition, overweight, and obesity among urban and rural children in north of west Azerbijan, Iran. J. Obes. 2014, 2014, 541213. [Google Scholar] [CrossRef] [PubMed]
- Setboonsarng, S. Child Malnutrition as a Poverty Indicator: An Evaluation in the Context of Different Development Interventions in Indonesia. Available online: https://think-asia.org/handle/11540/3609 (accessed on 1 September 2019).
- Mbuya, N.V.; Atwood, S.J.; Huynh, P.N. Persistent Malnutrition in Ethnic Minority Communities of Vietnam: Issues and Options for Policy and Interventions. Available online: https://openknowledge.worldbank.org/bitstream/handle/10986/31908/9781464814327.pdf?sequence=2&isAllowed=y (accessed on 2 September 2019).
- Lu, C.; Black, M.M.; Richter, L.M. Risk of poor development in young children in low-income and middle-income countries: An estimation and analysis at the global, regional, and country level. Lancet Glob. Health 2016, 4, e916–e922. [Google Scholar] [CrossRef]
- Nayak, B.S.; Unnikrishnan, B.; George, A.; Shashidhara, Y.; Mundkur, S.C.; Guddattu, V. Risk factors for malnutrition among preschool children in rural Karnataka: A case-control study. BMC Public Health 2018, 18, 283. [Google Scholar]
- Cetthakrikul, N.; Topothai, C.; Suphanchaimat, R.; Tisayaticom, K.; Limwattananon, S.; Tangcharoensathien, V. Childhood stunting in Thailand: When prolonged breastfeeding interacts with household poverty. BMC Pediatr. 2018, 18, 395. [Google Scholar] [CrossRef]
- Beal, T.; Tumilowicz, A.; Sutrisna, A.; Izwardy, D.; Neufeld, L.M. A review of child stunting determinants in Indonesia. Mater. Child Nutr. 2018, 14, e12617. [Google Scholar] [CrossRef] [PubMed]
- Unicef. UNICEF Data: Monitoring the Situation of Children and Women (Malnutrition). Available online: https://data.unicef.org/topic/nutrition/malnutrition (accessed on 18 April 2019).
- Gragnolati, M.; Bredenkamp, C.; Shekar, M.; Das Gupta, M.; Lee, Y.K. India’s Undernourished Children: A Call for Reform and Action. Available online: http://siteresources.worldbank.org/SOUTHASIAEXT/Resources/223546-1147272668285/IndiaUndernourishedChildrenFinal.pdf (accessed on 15 September 2019).
- Hall, A.; Hanh, T.T.M.; Farley, K.; Quynh, T.P.N.; Valdivia, F. An evaluation of the impact of a school nutrition programme in Vietnam. Public Health Nutr. 2007, 10, 819–826. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Nutritional Status | Kinh (n = 14,421; 89.1%) | Muong (n = 1307; 8.1%) | Tay (n = 449; 2.8%) | |||
|---|---|---|---|---|---|---|
| Prevalence (%) | 95% CI (%) | Prevalence (%) | 95% CI (%) | Prevalence (%) | 95% CI (%) | |
| Boys | ||||||
| Malnutrition | 13.9 | 13.1–14.8 | 35.1 | 31.6–38.8 | 48.2 | 41.9–54.7 |
| Underweight | 5.3 | 4.8–5.8 | 16.7 | 14.1–19.7 | 17.8 | 13.4–23.3 |
| Stunting | 11.5 | 10.9–12.3 | 31.9 | 28.5–35.5 | 43.9 | 37.7–50.4 |
| Wasting | 3.1 | 2.7–3.5 | 6.5 | 4.9–8.6 | 5.2 | 3.0–8.9 |
| Overweight | 6.5 | 6.0–7.1 | 1.5 | 0.8–2.7 | 2.2 | 0.9–5.0 |
| Obesity | 3.8 | 3.5–4.3 | 1.2 | 0.6–2.3 | 0.0 | 0–1.6 |
| Girls | ||||||
| Malnutrition | 15.6 | 14.7–16.5 | 33.4 | 29.8–37.2 | 37.9 | 31.7–44.5 |
| Underweight | 6.1 | 5.6–6.7 | 13.8 | 11.3–16.7 | 15.5 | 11.3–20.9 |
| Stunting | 12.6 | 11.8–13.4 | 29 | 25.6–32.1 | 37.4 | 31.3–44.0 |
| Wasting | 3.1 | 2.7–3.6 | 5.2 | 3.7–7.2 | 3.2 | 1.6–6.5 |
| Overweight | 4.3 | 3.9–4.8 | 1.9 | 1.1–3.2 | 2.3 | 1.0–5.2 |
| Obesity | 1.6 | 1.3–1.9 | 0.3 | 0.1–1.2 | 0.9 | 0.3–3.6 |
| Anthropometric Index | Kinh (1) | Muong (2) | Tay (3) | p1–2 | p1–3 | p2–3 | |||
|---|---|---|---|---|---|---|---|---|---|
| Mean | 95% CI | Mean | 95% CI | Mean | 95% CI | ||||
| Weight (kg) | 15.5 | 9.1; 21.9 | 13.2 | 9.0; 17.4 | 12.6 | 8.4; 16.8 | <0.0001 | <0.0001 | 0.001 |
| Height (cm) | 99.2 | 83.2; 115.2 | 92.9 | 77.4; 108.3 | 90.5 | 74.1; 106.9 | <0.0001 | <0.0001 | <0.0001 |
| Weight-for-age Z-score | −0.3 | −2.7; 2.0 | −1.1 | −3.1; 0.8 | −1.2 | −3.1; 0.7 | <0.0001 | <0.0001 | 0.286 |
| Height-for-age Z-score | −0.7 | −3.2; 1.9 | −1.5 | −3.9; 0.9 | −1.7 | −4.2; 0.7 | <0.0001 | <0.0001 | 0.038 |
| Weight-for-height-for-age Z-score | 0.05 | −2.4; 2.6 | −0.37 | −2.5; 1.8 | −0.3 | −2,3; 1.8 | <0.0001 | <0.0001 | 0.654 |
| BMI-for-age Z-score | 0.10 | −2.4; 2.6 | −0.2 | −2.4; 2.0 | −0.2 | −2,4; 2.1 | <0.0001 | <0.0001 | 0.255 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le, T.T.; Le, T.T.D.; Do, N.K.; Nadezhda, V.S.; Andrej, M.G.; Nguyen, T.T.T.; Nguyen, T.T.M.; Vu, T.T.; Le, T.H.; Nguyen, T.T.L.; et al. Ethnic Variations in Nutritional Status among Preschool Children in Northern Vietnam: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 4060. https://doi.org/10.3390/ijerph16214060
Le TT, Le TTD, Do NK, Nadezhda VS, Andrej MG, Nguyen TTT, Nguyen TTM, Vu TT, Le TH, Nguyen TTL, et al. Ethnic Variations in Nutritional Status among Preschool Children in Northern Vietnam: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2019; 16(21):4060. https://doi.org/10.3390/ijerph16214060
Chicago/Turabian StyleLe, Thi Tuyet, Thi Thuy Dung Le, Nam Khanh Do, V. Savvina Nadezhda, M. Grjibovski Andrej, Thi Trung Thu Nguyen, Thi Thanh Mai Nguyen, Thi Tuyen Vu, Thi Huong Le, Thi Thu Lieu Nguyen, and et al. 2019. "Ethnic Variations in Nutritional Status among Preschool Children in Northern Vietnam: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 16, no. 21: 4060. https://doi.org/10.3390/ijerph16214060