Prevalence, Perception, and Predictors of Advance Directives among Hong Kong Chinese: A Population-Based Survey

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
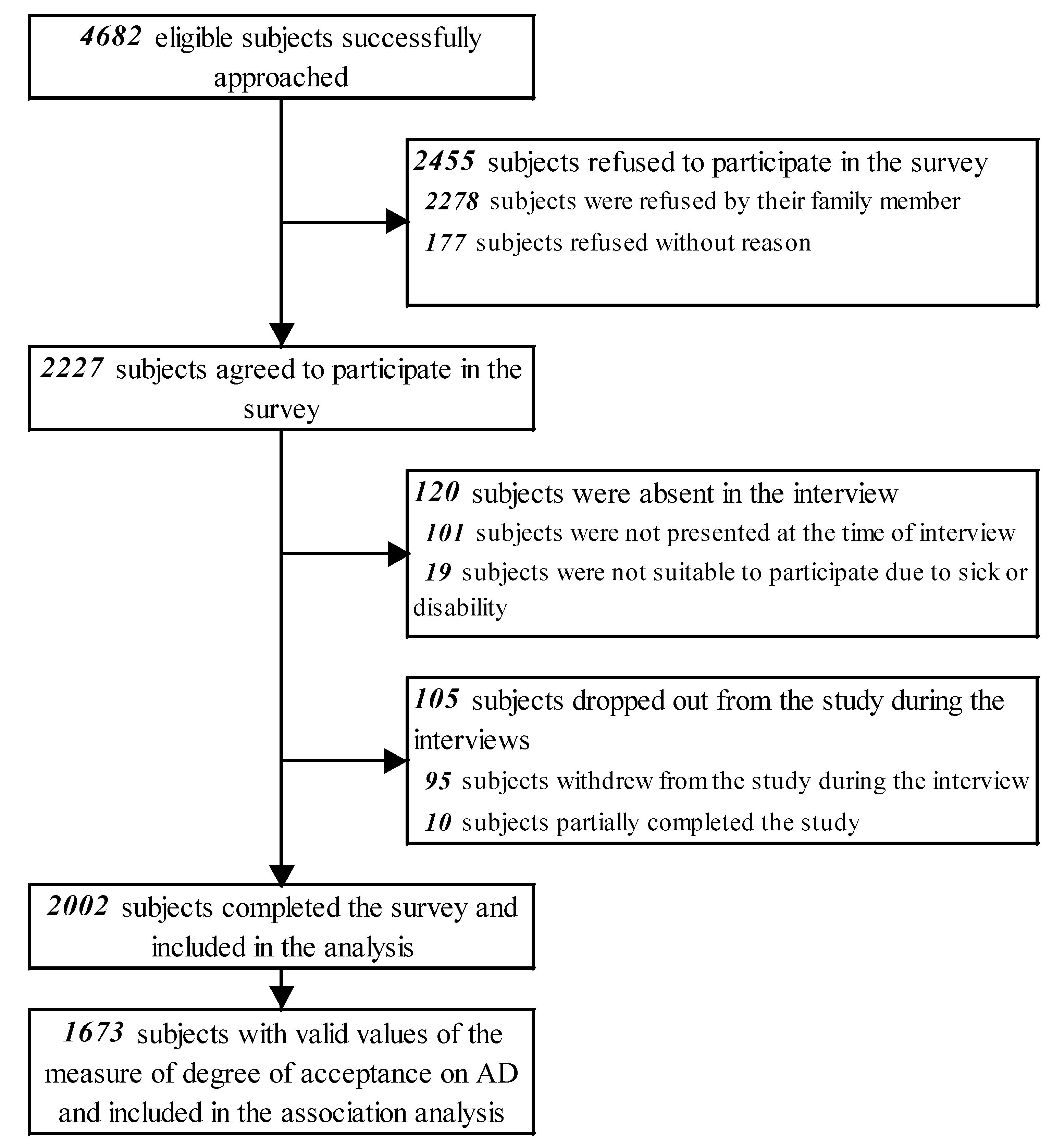
2.1. Study Design and Population
2.2. Measurement
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
3.2. Prevalence and Perception of AD
3.3. Factors Associated with Degree of Acceptance on AD Completion
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Rao, J.K.; Anderson, L.A.; Lin, F.C.; Laux, J.P. Completion of advance directives among US consumers. Am. J. Prev. Med. 2014, 46, 65–70. [Google Scholar] [CrossRef]
- Van Wijmen, M.P.S.; Rurup, M.L.; Pasman, H.R.W.; Kaspers, P.J.; Onwuteaka-Philipsen, B.D. Advance directives in the Netherlands: An empirical contribution to the exploration of a cross-cultural perspective on advance directives. Bioethics 2010, 24, 118–126. [Google Scholar] [CrossRef]
- Alano, G.J.; Pekmezaris, R.; Tai, J.Y.; Hussain, M.J.; Jeune, J.; Louis, B.; El-Kass, G.; Ashraf, M.S.; Reddy, R.; Lesser, M.; et al. Factors influencing older adults to complete advance directives. Palliat. Support. Care 2010, 8, 267–275. [Google Scholar] [CrossRef]
- Gerst, K.; Burr, J.A. Planning for end-of-life care: Black-White differences in the completion of advance directives. Res. Aging 2008, 30, 428–449. [Google Scholar] [CrossRef]
- Johnson, K.S.; Kuchibhatla, M.; Tulsky, A.A. What explains racial differences in the use of advance directives and attitudes toward hospice care? J. Am. Geriatr. Soc. 2008, 56, 1953–1958. [Google Scholar] [CrossRef]
- Pollack, K.M.; Morhaim, D.; Williams, M.A. The public’s perspectives on advance directives: Implications for state legislative and regulatory policy. Health Policy 2010, 96, 57–63. [Google Scholar] [CrossRef]
- Waite, K.R.; Federman, A.D.; McCarthy, D.M.; Sudore, R.; Curtis, L.M.; Baker, D.W.; Wilson, E.A.H.; Hasnain-Wynia, R.; Wolf, M.S.; Paasche-Orlow, M.K. Literacy and race as risk factors for low rates of advance directives in older adults. J. Am. Geriatr. Soc. 2013, 61, 403–406. [Google Scholar] [CrossRef]
- Wittenberg-Lyles, E.; Villagran, M.M.; Hajek, C. The impact of communication, attitudes, and acculturation on advance directives decision-making. J. Ethnic Cult. Divers. Soc. Work 2008, 17, 349–364. [Google Scholar] [CrossRef]
- Searight, H.R.; Gafford, J. Cultural diversity at the end of life: Issues and guidelines for family physicians. Am. Fam. Physician 2005, 71, 515–522. [Google Scholar]
- Vincent, J.L. Cultural differences in end-of-life care. Crit. Care. Med. 2001, 29 (Suppl. 2), N52–N55. [Google Scholar] [CrossRef]
- Rurup, M.L.; Onwuteaka-Philipsen, B.D.; van der Heide, A.; van der Wal, G.; Deeg, D.J.H. Frequency and determinants of advance directives concerning end-of-life care in the Netherlands. Soc. Sci. Med. 2006, 62, 1552–1563. [Google Scholar] [CrossRef]
- Doorenbos, A.Z.; Nies, M.A. The use of advance directives in a population of Asian Indian Hindus. J. Transcult. Nurs. 2003, 14, 17–24. [Google Scholar] [CrossRef]
- Braun, K.L.; Onaka, A.T.; Horiuchi, B.Y. Advance directive completion rates and end-of-life preferences in Hawaii. J. Am. Geriatr. Soc. 2001, 49, 1708–1713. [Google Scholar] [CrossRef]
- Puente, K.D.; Hidalgo, J.L.T.; Herraez, M.J.S.; Bravo, B.N.; Rodriguez, J.O.; Guillen, V.G. Study of the factors influencing the preparation of advance directives. Arch. Gerontol. Geriat. 2014, 58, 20–24. [Google Scholar] [CrossRef]
- Ko, E.; Lee, J. Completion of advance directives among low-income older adults: Does race/ethnicity matter? Am. J. Hosp. Palliat. Med. 2014, 31, 247–253. [Google Scholar] [CrossRef]
- Blank, R.H. End-of-life decision making across cultures. J. Law Med. Ethics 2011, 39, 201–214. [Google Scholar] [CrossRef]
- Kossman, D.A. Prevalence, views, and impact of advance directives among older adults. J. Gerontol. Nurs. 2014, 40, 44–50. [Google Scholar] [CrossRef]
- Kim, S.H. Factors influencing preferences of Korean people toward advance directives. Nurs. Ethics 2011, 18, 505–513. [Google Scholar]
- Census and Statistics Department, HKSAR. 2016 Population by-Census—Main Results; Census and Statistics Department: Hong Kong, China, 2017. [Google Scholar]
- Bowman, K.W.; Singer, P.A. Chinese seniors’ perspectives on end-of-life decisions. Soc. Sci. Med. 2001, 53, 455–464. [Google Scholar] [CrossRef]
- The Economist Intelligence Unit. The 2015 Quality of Death Index Ranking Palliative Care across the World; Lien Foundation: Singapore, 2015. [Google Scholar]
- The Law Reform Commission of Hong Kong. Substitute Decision-Making and Advance Directives in Relation to Medical Treatment; The Law Reform Commission of Hong Kong: Hong Kong, China, 2006. [Google Scholar]
- Hospital Authority. Strategic Service Framework for Palliative Care; Hospital Authority: Hong Kong, China, 2017. [Google Scholar]
- Hospital Authority. Guidance for HA Clinicians on Advance Directives in Adults; Hospital Authority: Hong Kong, China, 2016. [Google Scholar]
- Chung, R.Y.-N.; Wong, E.L.-Y.; Kiang, N.; Chau, P.Y.-K.; Lau, J.Y.; Wong, S.Y.-S.; Yeoh, E.-K.; Woo, J.W. Knowledge, attitudes, and preferences of advance decisions, end-of-life care, and place of care and death in Hong Kong. A population-based telephone survey of 1067 adults. J. Am. Med. Dir. Assoc. 2017, 18, 367. [Google Scholar] [CrossRef]
- Reese, D.J.; Chan, C.L.; Chan, W.C.; Wiersgalla, D. A cross-national comparison of Hong Kong and US student beliefs and preferences in end-of-life care: Implications for social work education and hospice practice. J. Soc. Work End Life Palliat. Care 2010, 6, 205–235. [Google Scholar] [CrossRef]
- Chan, C.W.; Wong, M.M.; Choi, K.C.; Chan, H.Y.; Chow, A.Y.; Lo, R.S.; Sham, M.M. What patients, families, health professionals and hospital volunteers told us about advance directives. Asia Pac. J. Oncol. Nurs. 2019, 6, 72. [Google Scholar] [CrossRef]
- Nolan, M.T.; Bruder, M. Patients’ attitudes toward advance directives and end-of-life treatment decisions. Nurs. Outlook 1997, 45, 204–208. [Google Scholar] [CrossRef]
- So, W.K.W.; Choi, K.C.; Chan, D.N.S.; Chan, C.W.H.; Shiu, A.T.Y.; Ho, S.S.S.; Chan, H.Y.L.; Lam, W.W.T.; Cheng, K.K.F.; Goggins, W.B. Colorectal cancer testing and associated factors among older Chinese adults. Prev. Med 2012, 54, 104–105. [Google Scholar] [CrossRef]
- Department of Health, HKSAR. Report of Population Health Survey 2014/15; Department of Health: Hong Kong, China, 2017.
- White, B.; Tilse, C.; Wilson, J.; Rosenman, L.; Strub, T.; Feeney, R.; Silvester, W. Prevalence and predictors of advance directives in Australia. Intern. Med. J. 2014, 44, 975–980. [Google Scholar] [CrossRef] [Green Version]
- Kwok, T.; Twinn, S.; Yan, E. The attitudes of Chinese family caregivers of older people with dementia towards life sustaining treatments. J. Adv. Nurs. 2007, 58, 256–262. [Google Scholar] [CrossRef]
- Wong, S.; Lo, S.; Chan, C.; Chui, H.; Sze, W.; Tung, Y. Is it feasible to discuss an advance directive with a Chinese patient with advanced malignancy? A prospective cohort study. Hong Kong Med. J. 2012, 18, 178–185. [Google Scholar]
- Mjelde-Mossey, L.A.; Chan, C.L.W. Survey on death and dying in Hong Kong: Attitudes, beliefs, and preferred, end-of-life care. Soc. Work Health Care 2007, 45, 49–65. [Google Scholar] [CrossRef]
- Hamel, C.F.; Guse, L.W.; Hawranik, P.G.; Bond, J.B. Advance directives and community-dwelling older adults. Western J. Nurs. Res. 2002, 24, 143–158. [Google Scholar] [CrossRef]
- Campbell, M.J.; Edwards, M.J.; Ward, K.S.; Weatherby, N. Developing a parsimonious model for predicting completion of advance directives. J. Nurs. Scholarsh. 2007, 39, 165–171. [Google Scholar] [CrossRef]
- Pang, S.M.C.; Tse, C.; Chan, K.; Chung, B.P.M.; Leung, A.K.A.; Leung, E.M.F.; Ko, S.K.K. An empirical analysis of the decision-making of limiting life-sustaining treatment for patients with advanced chronic obstructive pulmonary disease in Hong Kong, China. J. Crit. Care 2004, 19, 135–144. [Google Scholar] [CrossRef]
- Chu, L.W.; Luk, J.K.H.; Hui, E.; Chiu, P.K.C.; Chan, C.S.Y.; Kwan, F.; Kwok, T.; Lee, D.; Woo, J. Advance directive and end-of-life care preferences among Chinese nursing home residents in Hong Kong. J. Am. Med. Dir. Assoc. 2011, 12, 143–152. [Google Scholar] [CrossRef]
- Lee, M.C.; Hinderer, K.A.; Kehl, K.A. A systematic review of advance directives and advance care planning in Chinese people from Eastern and Western cultures. J. Hosp. Palliat. Nurs. 2014, 16, 75–85. [Google Scholar] [CrossRef]
- Tang, C.; Lam, L.; Chiu, H. Attitudes to end-of-life decisions: A survey of elderly Chinese with dementia and their carers. Asian J. Gerontol. Geriatr. 2007, 2, 119–125. [Google Scholar]
- Siu, M.W.; Cheung, T.Y.; Chiu, M.M.; Kwok, T.Y.; Choi, W.L.; Lo, T.K.; Ting, W.M.; Yu, P.H.; Cheung, C.Y.; Wong, J.G.; et al. The preparedness of Hong Kong medical students towards advance directives and end-of-life issues. East Asian Arch. Psychiatry 2010, 20, 155–162. [Google Scholar]
- Sullivan, A.M.; Lakoma, M.D.; Block, S.D. The status of medical education in end-of-life care: A national report. J. Gen. Intern. Med. 2003, 18, 685–695. [Google Scholar] [CrossRef]
- Barrere, C.C.; Durkin, A.; LaCoursiere, S. The influence of end-of-life education on attitudes of nursing students. Int. J. Nurs. Educ. Scholarsh. 2008, 5, 11. [Google Scholar] [CrossRef]
- Hegedus, K.; Zana, A.; Szabo, G. Effect of end of life education on medical students’ and health care workers’ death attitude. Palliat. Med. 2008, 22, 264–269. [Google Scholar] [CrossRef]
- Billings, M.E.; Engelberg, R.; Curtis, J.R.; Block, S.; Sullivan, A.M. Determinants of medical students’ perceived preparation to perform end-of-life care, quality of end-of-life care education, and attitudes toward end-of-life care. J. Palliat. Med. 2010, 13, 319–326. [Google Scholar] [CrossRef]
- Fraser, H.C.; Kutner, J.S.; Pfeifer, M.P. Senior medical students’ perceptions of the adequacy of education on end-of-life issues. J. Palliat. Med. 2001, 4, 337–343. [Google Scholar] [CrossRef]
- Engelhardt, H.T., Jr.; Iltis, A.S. End-of-life: The traditional Christian view. Lancet 2005, 366, 1045–1049. [Google Scholar] [CrossRef]
- Keown, D. End of life: The Buddhist view. Lancet 2005, 366, 952–955. [Google Scholar] [CrossRef]
- Lin, A.H.M.H. Factors related to attitudes toward death among American and Chinese older adults. Omega-J. Death Dying 2003, 47, 3–23. [Google Scholar] [CrossRef]
- Lynn, T.; Curtis, A.; Lagerwey, M.D. Association between attitude toward death and completion of advance directives. OMEGA-J. Death Dying 2016, 74, 193–211. [Google Scholar] [CrossRef]
- Winterling, J.; Wasteson, E.; Sidenvall, B.; Sidenvall, E.; Glimelius, B.; Sjoden, P.O.; Nordin, K. Relevance of philosophy of life and optimism for psychological distress among individuals in a stage where death is approaching. Support. Care. Cancer 2006, 14, 310–319. [Google Scholar] [CrossRef]
- Murphy, C.P.; Sweeney, M.A.; Chiriboga, D. An educational intervention for advance directives. J. Prof. Nurs. 2000, 16, 21–30. [Google Scholar] [CrossRef]
- Tamayo-Velazquez, M.I.; Simon-Lorda, P.; Villegas-Portero, R.; Higueras-Callejon, C.; Garcia-Gutierrez, J.F.; Martinez-Pecino, F.; Barrio-Cantalejo, I.M. Interventions to promote the use of advance directives: An overview of systematic reviews. Patient Educ. Couns. 2010, 80, 10–20. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | N (%) |
|---|---|
| Socio-demographic characteristics | |
| Sex | |
| Male | 885 (44.2) |
| Female | 1117 (55.8) |
| Age (years) | |
| 18–24 | 243 (12.1) |
| 25–34 | 287 (14.3) |
| 35–44 | 298 (14.9) |
| 45–54 | 365 (18.2) |
| 55–64 | 384 (19.2) |
| ≥65 | 425 (21.2) |
| Education | |
| No formal education | 88 (4.4) |
| Primary school | 229 (11.4) |
| Junior secondary school | 259 (12.9) |
| Senior secondary school | 687 (34.3) |
| Tertiary or above | 719 (35.9) |
| Refused to answer | 20 (1.0) |
| Marital status | |
| Married | 1172 (58.5) |
| Single | 692 (34.6) |
| Divorced/separated/widowed | 114 (5.7) |
| Refused to answer | 24 (1.2) |
| Employment status | |
| Employed | 1073 (53.6) |
| Unemployed | 97 (4.8) |
| Retired | 415 (20.7) |
| Homemaker | 219 (10.9) |
| Students | 168 (8.4) |
| Others/refused to answer | 30 (1.5) |
| Religion | |
| None | 1579 (78.9) |
| Christianity | 186 (9.3) |
| Catholicism | 52 (2.6) |
| Buddhism | 98 (4.9) |
| Chinese folk religion | 41 (2.0) |
| Refused to answer | 46 (2.3) |
| Monthly household income (HK$) | |
| <10,000 | 242 (12.1) |
| 10,000–19,999 | 314 (15.7) |
| 20,000–29,999 | 469 (23.4) |
| 30,000–59,999 | 413 (20.6) |
| ≥60,000 | 204 (10.2) |
| Don’t know/refused to answer | 360 (18.0) |
| Self-perceptions and health status | |
| Self-rated health | |
| Good | 1250 (62.4) |
| Average | 654 (32.7) |
| Bad | 89 (4.4) |
| Don’t know/unsure | 9 (0.4) |
| Ever had a serious disease or cancer | |
| No | 1894 (94.6) |
| Yes | 99 (4.9) |
| Don’t know/unsure | 9 (0.4) |
| Family history of serious diseases or cancers | |
| No | 1602 (80.0) |
| Yes | 385 (19.2) |
| Don’t know/unsure | 15 (0.7) |
| Playing a key role in family | |
| No | 594 (29.7) |
| Yes | 1288 (64.3) |
| Unsure | 120 (6.0) |
| Self-perceived level of optimism [1 to 7; 1 = very pessimistic, 7 = very optimistic] | |
| 1–3 | 124 (6.2) |
| 4 | 316 (15.8) |
| 5 | 620 (31.0) |
| 6 | 374 (18.7) |
| 7 | 194 (9.7) |
| Don’t know/unsure | 374 (18.7) |
| Level of agreement that patients’ wishes and decisions should be respected [1 to 7; 1 = strongly disagree, 7 = strongly agree] | |
| 1–3 | 46 (2.3) |
| 4 | 124 (6.2) |
| 5 | 371 (18.5) |
| 6 | 614 (30.7) |
| 7 | 738 (36.9) |
| Don’t know/unsure | 109 (5.4) |
| Prevalence of AD | n (%) |
|---|---|
| Ever heard about advance directives | |
| No | 1629 (81.4%) |
| Yes | 368 (18.4%) |
| Can’t remember | 5 (0.2%) |
| Had made advance directives | |
| Had not heard of advance directives/can’t remember | 1634 (81.6%) |
| No | 357 (17.8%) |
| Yes | 11 (0.5%) |
| Had made or intend to made advance directives | |
| Had not heard of advance directives/can’t remember | 1634 (81.6%) |
| No | 39 (1.9%) |
| Yes | 295 (14.7%) |
| Don’t know/unsure | 34 (1.7%) |
| Perceptions Related to AD | n (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| Rating | ||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | Don’t Know/Unsure | |
| 1. Level of agreement that (AD is a basic human right) [1 to 7; 1 = strongly disagree, 7 = strongly agree] | 6 (0.3) | 7 (0.3) | 55 (2.7) | 141 (7.0) | 534 (26.7) | 573 (28.6) | 537 (26.8) | 149 (7.4) |
| 2. Level of agreement that (advance directives should encompass basic nursing care, including pain relief and wound cleansing etc) [1 to 7; 1 = strongly disagree, 7 = strongly agree] | 73 (3.6) | 77 (3.8) | 125 (6.2) | 288 (14.4) | 493 (24.6) | 314 (15.7) | 343 (17.1) | 289 (14.4) |
| 3. Level of agreement that (healthcare professionals should carry out advance directives by legislation) [1 to 7; 1 = strongly disagree, 7 = strongly agree] | 23 (1.1) | 21 (1.0) | 86 (4.3) | 281 (14.0) | 513 (25.6) | 311 (15.5) | 450 (22.5) | 317 (15.8) |
| 4. (Adequacy of promotion on advance directive in the community) [1 to 7; 1 = very inadequate, 7 = very adequate] | 431 (21.5) | 569 (28.4) | 456 (22.8) | 207 (10.3) | 109 (5.4) | 33 (1.6) | 18 (0.9) | 179 (8.9) |
| 4. Level of agreement that (patients should have a clear mind and be mentally prepared when considering making advance directives) [1 to 7; 1 = strongly disagree, 7 = strongly agree] | 5 (0.2) | 8 (0.4) | 13 (0.6) | 74 (3.7) | 213 (10.6) | 469 (23.4) | 876 (43.8) | 344 (17.2) |
| 5. Level of agreement that (healthcare professionals should have good communication skills when discussing making advance directives with patients) [1 to 7; 1 = strongly disagree, 7 = strongly agree] | 9 (0.4) | 6 (0.3) | 32 (1.6) | 54 (2.7) | 292 (14.6) | 522 (26.1) | 701 (35.0) | 386 (19.3) |
| 6. Level of agreement that (in addition to healthcare professionals and patients, family members of patient should engage in discussing making advance directives) [1 to 7; 1 = strongly disagree, 7 = strongly agree] | 25 (1.2) | 16 (0.8) | 67 (3.3) | 91 (4.5) | 313 (15.6) | 427 (21.3) | 699 (34.9) | 364 (18.2) |
| 7. Level of agreement that (records throughout the process of discussions and making decisions of advance directives with patients should be kept) [1 to 7; 1 = strongly disagree, 7 = strongly agree] | 10 (0.5) | 8 (0.4) | 28 (1.4) | 65 (3.2) | 274 (13.7) | 513 (25.6) | 680 (34.0) | 424 (21.2) |
| Level of Agreement [Range: 1 to 7; 1 = Strongly Disagree, 7 = Strongly Agree] | n (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| Rating | ||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | Don’t Know/Unsure | |
| 1. (When my health condition is serious enough to have no effective treatment) | 32 (1.6) | 13 (0.6) | 68 (3.4) | 95 (4.7) | 313 (15.6) | 582 (29.1) | 598 (29.9) | 301 (15.0) |
| 2. (In order to reduce the physical and psychological burden of family members) | 12 (0.6) | 16 (0.8) | 47 (2.3) | 95 (4.7) | 251 (12.5) | 649 (32.4) | 631 (31.5) | 301 (15.0) |
| 3. (When considering side effects and adverse effects on quality of life in receiving survival treatments, such as mechanical ventilating and tube feeding) | 28 (1.4) | 42 (2.1) | 67 (3.3) | 196 (9.8) | 395 (19.7) | 443 (22.1) | 492 (24.6) | 339 (16.9) |
| 4. (If healthcare professionals can provide you clear explanation and recommendation on advance directives) | 15 (0.7) | 11 (0.5) | 41 (2.0) | 100 (5.0) | 363 (18.1) | 536 (26.8) | 582 (29.1) | 354 (17.7) |
| 5. (If there is effective communication and coordination among healthcare professionals at different institutes to execute your decisions) | 169 (8.4) | 192 (9.6) | 39 (1.9) | 83 (4.1) | 347 (17.3) | 383 (19.1) | 444 (22.2) | 345 (17.2) |
| 6. (If you can have thorough discussion and follow-up with health professionals about advance directives) | 54 (2.7) | 63 (3.1) | 85 (4.2) | 144 (7.2) | 363 (18.1) | 500 (25.0) | 433 (21.6) | 360 (18.0) |
| 7. (If advance directive is a legally binding instrument) | 74 (3.7) | 176 (8.8) | 143 (7.1) | 154 (7.7) | 340 (17.0) | 322 (16.1) | 390 (19.5) | 403 (20.1) |
| Factors | Univariate Analysis | Multivariable Analysis | |||
|---|---|---|---|---|---|
| Mean (SD) | p-Value | B | SE | p-Value | |
| Socio-demographic characteristics | |||||
| Sex | |||||
| Male (ref) | 74.8 (16.7) | 0.682 | NR | NR | NR |
| Female | 75.2 (17.9) | ||||
| Age (years) | |||||
| 18–24 (ref) | 70.0 (16.8) | <0.001 | NR | NR | NR |
| 25–34 | 73.6 (15.8) | ||||
| 35–44 | 75.6 (17.8) | ||||
| 45–54 | 77.6 (15.9) | ||||
| 55–64 | 77.6 (16.3) | ||||
| ≥65 | 73.8 (20.2) | ||||
| Education | |||||
| No formal education (ref) | 67.8 (21.0) | 0.019 | NR | NR | NR |
| Primary school | 73.3 (19.2) | ||||
| Junior secondary school | 74.3 (15.8) | ||||
| Senior secondary school | 76.4 (16.8) | ||||
| Tertiary or above | 74.7 (17.8) | ||||
| Marital status | |||||
| Single/divorced/separated/ widowed (ref) | 73.1 (17.5) | <0.001 | NR | NR | NR |
| Married | 76.4 (17.2) | ||||
| Employment status | |||||
| Employed (ref) | 75.9 (16.6) | <0.001 | |||
| Unemployed | 74.0 (13.6) | 0.150 | 1.956 | 0.939 | |
| Retired | 74.9 (19.9) | 0.039 | 1.110 | 0.972 | |
| Homemaker | 76.1 (17.7) | 0.455 | 1.361 | 0.738 | |
| Students | 68.6 (17.4) | −5.890 | 1.411 | <0.001 | |
| Religion | |||||
| None (ref) | 73.5 (17.4) | <0.001 | |||
| Christianity | 80.9 (16.0) | 5.124 | 1.316 | <0.001 | |
| Catholicism | 80.8 (18.8) | 4.775 | 2.368 | 0.044 | |
| Buddhism | 82.4 (15.2) | 8.192 | 1.850 | <0.001 | |
| Chinese folk religion | 75.7 (19.1) | 1.416 | 3.371 | 0.675 | |
| Monthly household income (HK$) | |||||
| <10,000 (ref) | 73.0 (18.8) | 0.002 | NR | NR | NR |
| 10,000–19,999 | 72.3 (17.2) | ||||
| 20,000–29,999 | 74.2 (16.3) | ||||
| 30,000–59,999 | 76.5 (17.8) | ||||
| ≥60,000 | 78.0 (17.7) | ||||
| Don’t know/refused to answer | 75.7 (16.9) | ||||
| Health status and self-perceptions | |||||
| Self-rated health | |||||
| Good (ref) | 74.9 (16.6) | 0.176 | NR | NR | NR |
| Average | 75.8 (18.2) | ||||
| Bad | 71.2 (21.6) | ||||
| Q3. Ever had a serious disease or cancer | |||||
| No (ref) | 74.9 (17.3) | 0.075 | NR | NR | NR |
| Yes | 78.5 (18.7) | ||||
| Q4. Family history of serious diseases or cancers | |||||
| No (ref) | 74.5 (17.2) | 0.032 | NR | NR | NR |
| Yes | 76.8 (18.0) | ||||
| Q2. Play a key role in family | |||||
| No/unsure (ref) | 73.4 (17.0) | 0.006 | NR | NR | NR |
| Yes | 75.8 (17.6) | ||||
| Q24. Self-perceived level of optimism [1 to 7; 1 = very pessimistic, 7 = very optimistic] | |||||
| 1–3 (ref) | 67.9 (18.2) | <0.001 | |||
| 4 | 72.3 (17.8) | 4.319 | 1.782 | 0.015 | |
| 5 | 75.1 (15.8) | 6.359 | 1.648 | <0.001 | |
| 6 | 79.0 (15.2) | 8.811 | 1.736 | <0.001 | |
| 7 | 80.3 (19.0) | 9.493 | 1.912 | <0.001 | |
| Don’t know/unsure | 66.0 (21.0) | −2.127 | 2.321 | 0.360 | |
| Q5. Level of agreement that patients’ wishes and decisions should be respected [1 to 7; 1 = strongly disagree, 7 = strongly agree] | |||||
| 1–3 (ref) | 58.2 (22.6) | <0.001 | |||
| 4 | 64.3 (18.6) | 6.224 | 3.093 | 0.044 | |
| 5 | 71.8 (14.6) | 12.820 | 2.735 | <0.001 | |
| 6 | 74.5 (15.0) | 15.847 | 2.669 | <0.001 | |
| 7 | 79.8 (17.8) | 20.112 | 2.645 | <0.001 | |
| Don’t know/unsure | 66.6 (19.5) | 10.061 | 3.617 | 0.005 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, C.W.H.; Wong, M.M.H.; Choi, K.C.; Chan, H.Y.L.; Chow, A.Y.M.; Lo, R.S.K.; Sham, M.M.K. Prevalence, Perception, and Predictors of Advance Directives among Hong Kong Chinese: A Population-Based Survey. Int. J. Environ. Res. Public Health 2019, 16, 365. https://doi.org/10.3390/ijerph16030365
Chan CWH, Wong MMH, Choi KC, Chan HYL, Chow AYM, Lo RSK, Sham MMK. Prevalence, Perception, and Predictors of Advance Directives among Hong Kong Chinese: A Population-Based Survey. International Journal of Environmental Research and Public Health. 2019; 16(3):365. https://doi.org/10.3390/ijerph16030365
Chicago/Turabian StyleChan, Carmen W. H., Martin M. H. Wong, Kai Chow Choi, Helen Y. L. Chan, Amy Y. M. Chow, Raymond S. K. Lo, and Michael M. K. Sham. 2019. "Prevalence, Perception, and Predictors of Advance Directives among Hong Kong Chinese: A Population-Based Survey" International Journal of Environmental Research and Public Health 16, no. 3: 365. https://doi.org/10.3390/ijerph16030365