Analysis of Epidemiological Characteristics of Notifiable Diseases Reported in Children Aged 0–14 Years from 2008 to 2017 in Zhejiang Province, China

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Resources
2.2. Main Classification Indicators
2.2.1. All Infectious Diseases Were Divided into 3 Categories
2.2.2. Class B Infectious Diseases Were Classified into Five Sub-Classes by Routes of Transmission, Etiology or Sources of Infection
2.3. Data Analysis
2.4. Ethical Statement
3. Results
3.1. General Characteristics of Notifiable Diseases
3.2. Temporal Distribution
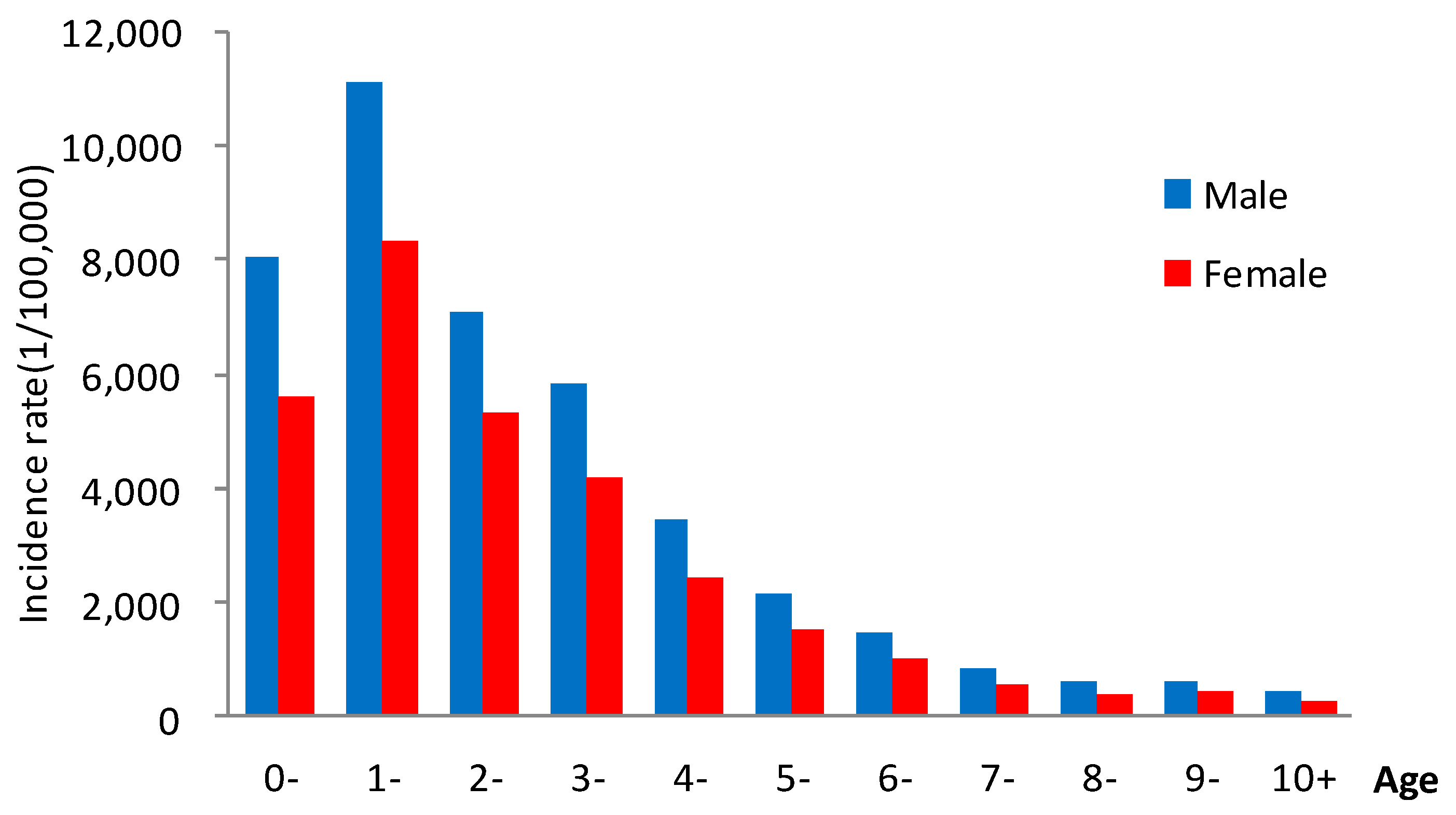
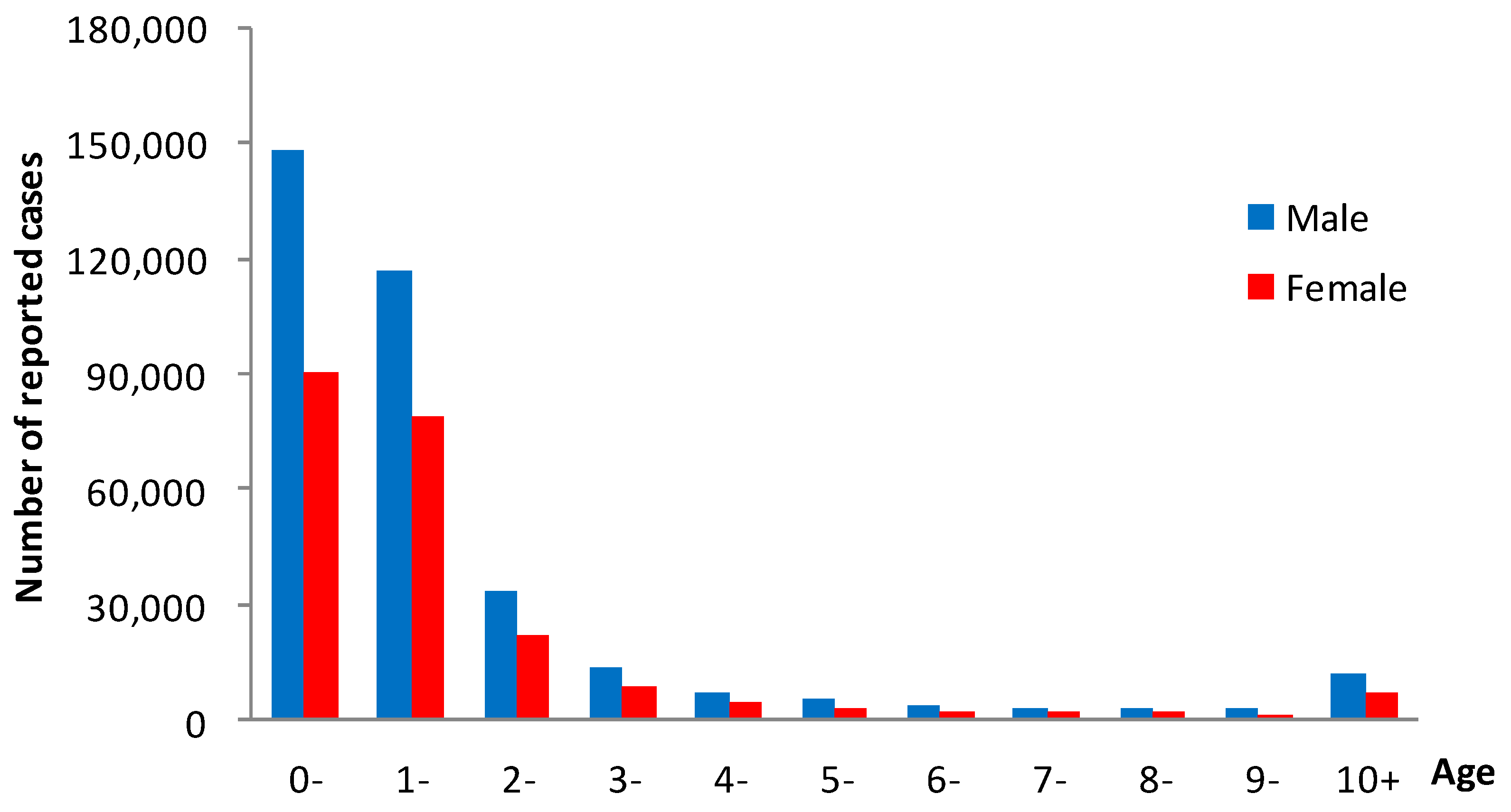
3.3. Population Distribution
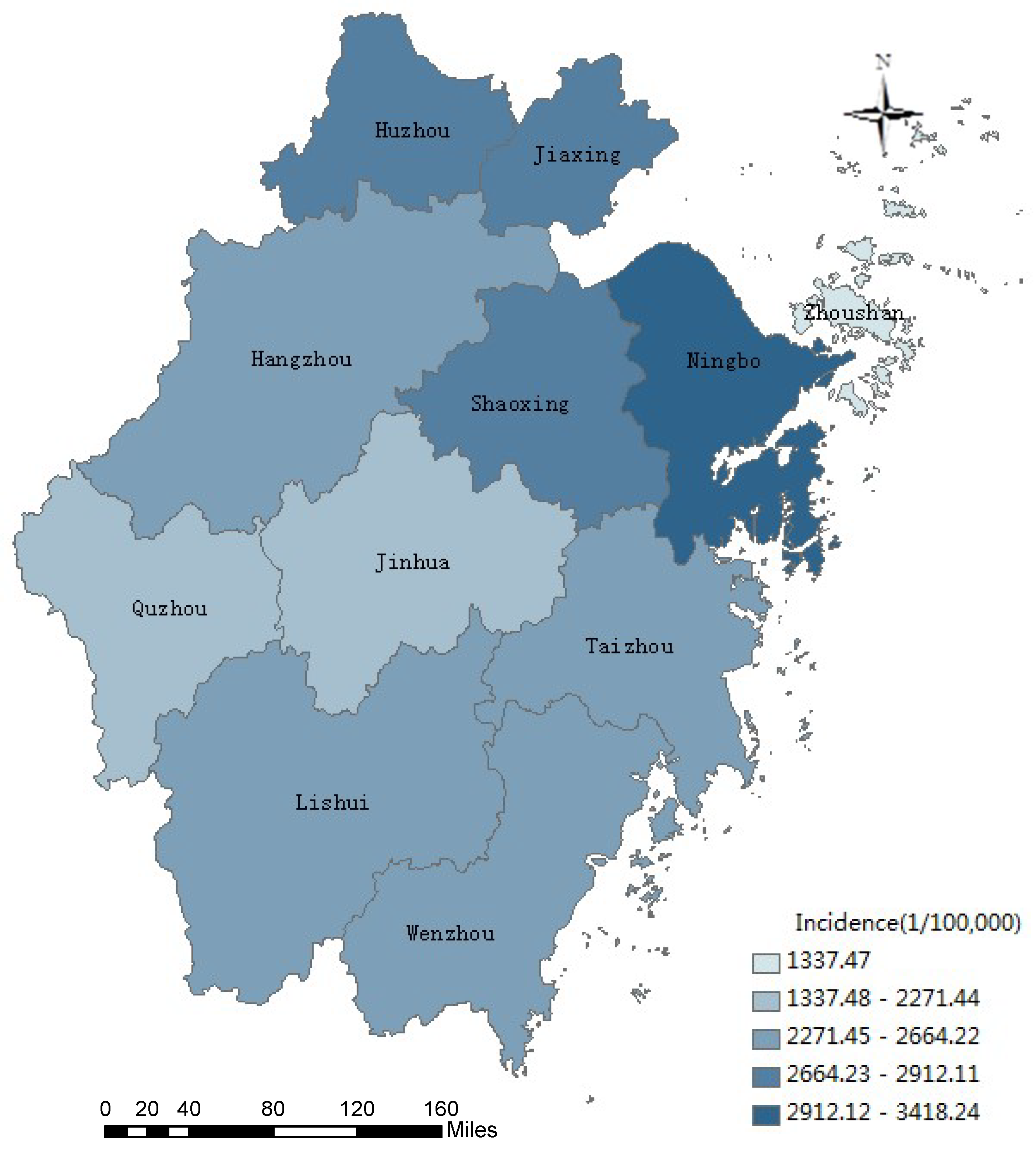
3.4. Geographic Distribution
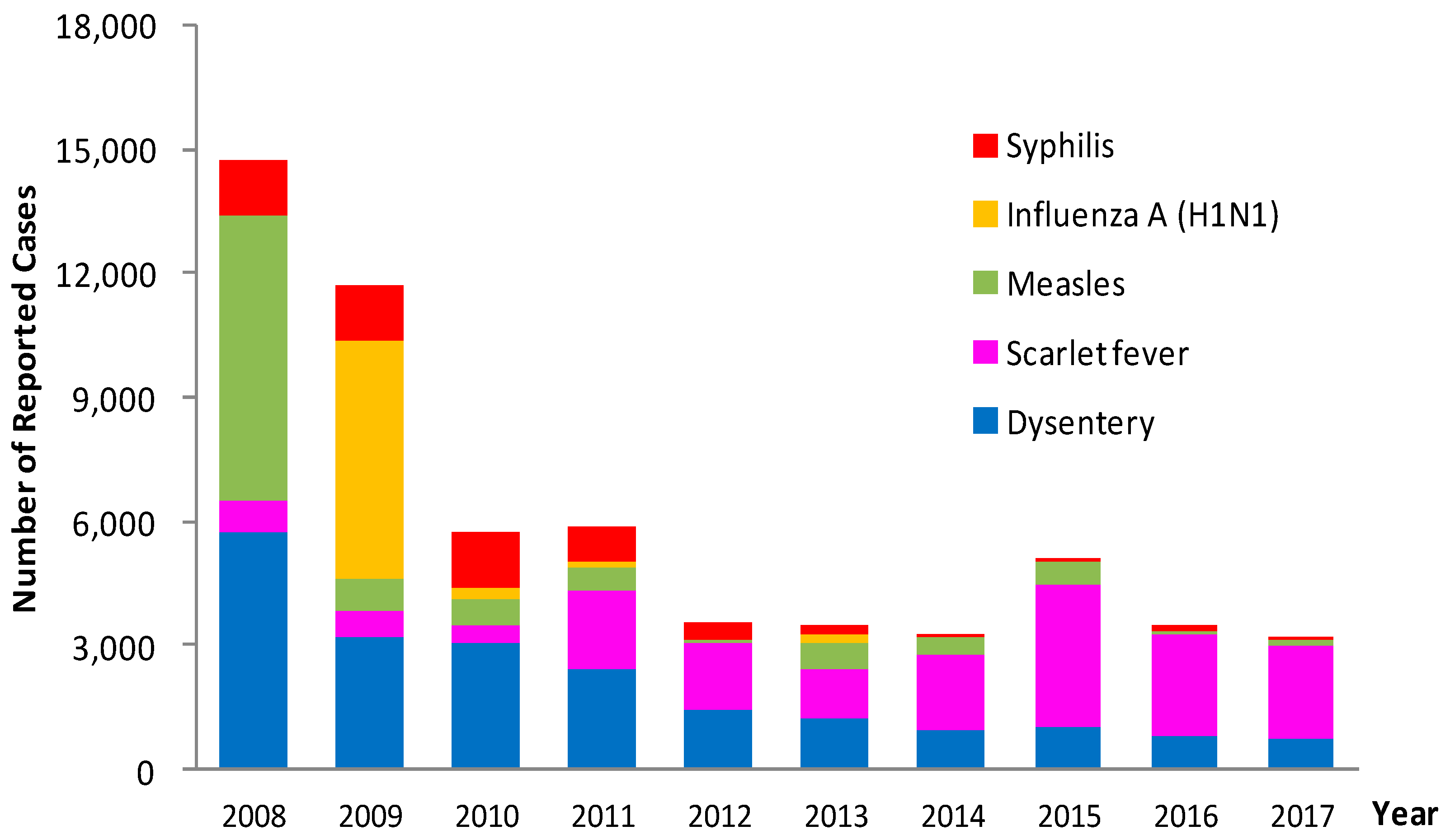
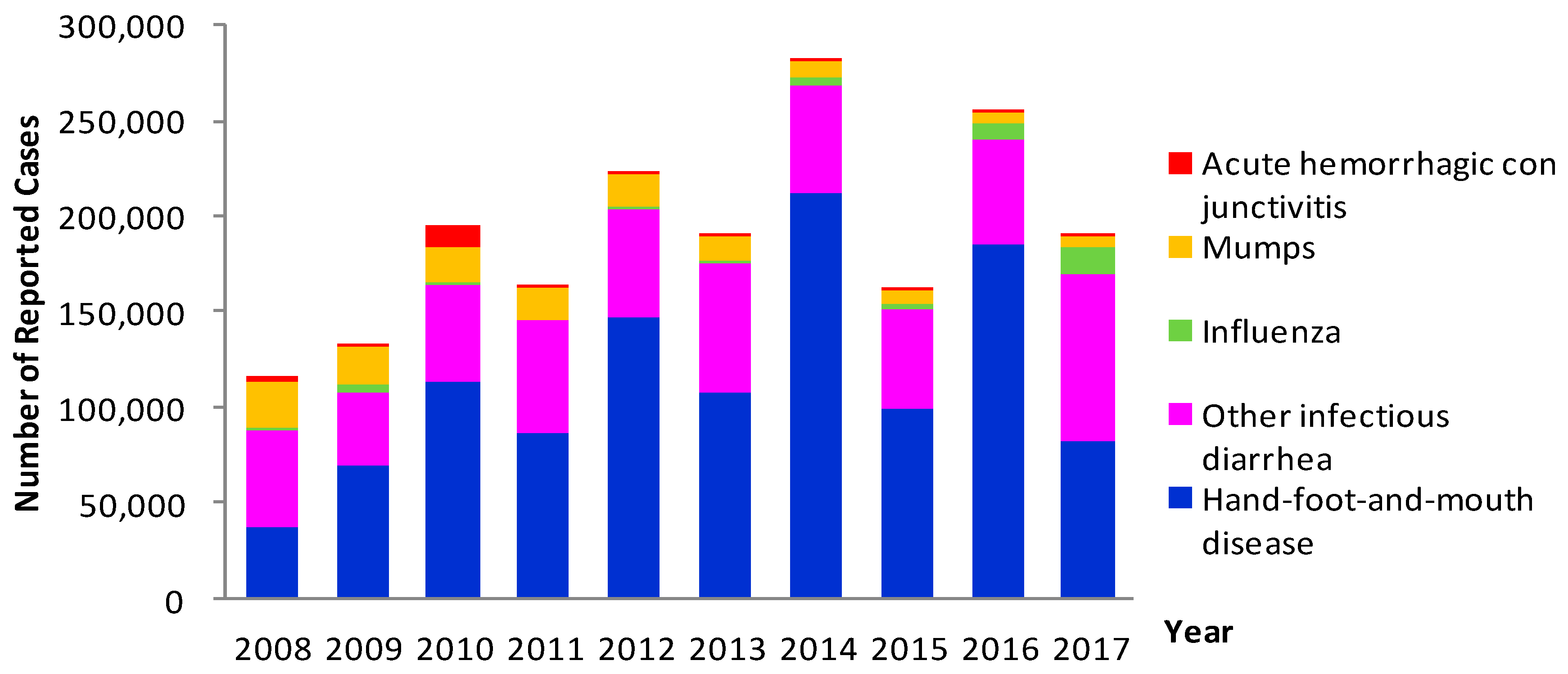
3.5. Infectious Diseases by Classification and Transmission Routes
3.6. Epidemiological Characteristics of Major Infectious Diseases
3.6.1. Hand-Foot-and-Mouth Disease (HFMD)
3.6.2. Other Infectious Diarrheal Diseases
3.6.3. Mumps
3.6.4. Influenza, Influenza A (H1N1) and Avian Influenza A (H7N9)
3.6.5. Dysentery
3.6.6. Hepatitis B
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AIDS | acquired immune deficiency syndrome |
| SARS | severe acute respiratory syndromes |
| HFMD | hand-foot-and-mouth disease |
| EV71 | enterovirus 71 |
| CV-A16 | coxsackieviruses A16 |
| CISDCP | China information system for disease control and prevention |
| SPSS | statistical package for the social sciences |
References
- WHO. Why Infectious Diseases Are Still a Problem and Surveillance Is Still Required [EB]. Available online: http://www.who.int/csr/resources/publications/introduction/en/index1.html (accessed on 9 October 2018).
- Yang, Y.; Liu, Z.Y. Status Quo and Future of Childhood Infectious Diseases. J. Appl. Clin. Pediatr. 2010, 25, 1697–1699. (In Chinese) [Google Scholar]
- Hong, R.T.; Wu, S.G.; Li, Q.; Ou, J.M.; Chen, W.; Yan, Y.S. Current status and outlook of communicable disease surveillance in the mainland of China. Dis. Surveill. 2015, 30, 994–1001. (In Chinese) [Google Scholar]
- Zhang, L.; Wilson, D.P. Trends in notifiable infectious diseases in China: Implications for surveillance and population health policy. PLoS ONE 2012, 7, e31076. [Google Scholar] [CrossRef] [PubMed]
- National Health and Family Planning Commission of the People’s Republic of China. Notification of the National Health and Family Planning Commission on Adjusting the Management of Some Notifiable Diseases (NHFPC Disease Control [2013] No. 28). Available online: http://www.nhfpc.Gov.cn/jkj/s3577/201311/f6ee56b5508a4295a8d552ca5f0f5edd.shtml (accessed on 9 October 2018). (In Chinese)
- Ministry of Health of the People’s Republic of China. Notification of the Ministry of Health on the Inclusion of Hand-Foot-and-Mouth Disease into Management of Notifiable Diseases. Available online: http://www.nhfpc.gov.cn/jkj/s3577/200805/1a8bb3668b7d4540afb0531dfcef978d.shtml (accessed on 9 October 2018). (In Chinese)
- Ministry of Health of the People’s Republic of China. Announcement of the Ministry of Health on the Inclusion of Influenza A (H1N1) into the “Law of the People’s Republic of China on the Prevention and Control of Infectious Diseases” and the “Frontier Health and Quarantine Law of the People’s Republic of China” (MOH, No. 8 Announcement of 2009). Available online: http://www.nhfpc.gov.cn/jkj/s7923/200904/4c8a365461204f3498fc13ac1230b899.shtml (accessed on 9 October 2018). (In Chinese)
- Zhang, X.Y.; Hou, F.S.; Li, X.S.; Zhou, L.J.; Liu, Y.Y.; Zhang, T. Study of surveillance data for class B notifiable disease in China from 2005 to 2014. Int. J. Infect. Dis. 2016, 48, 7–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Y.; Chen, Y.P. Evaluating Childhood Vaccination Coverage of NIP Vaccines: Coverage Survey versus Zhejiang Provincial Immunization Information System. Int. J. Environ. Res. Public Health 2017, 14, 758. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.R.; He, H.Q.; Chen, E.F.; Li, Q.; Ling, L.Y. Epidemiological Characteristics of Measles in Zhejiang Province. Zhejiang Prev. Med. 2010, 22, 1–3. (In Chinese) [Google Scholar]
- He, H.Q.; Pan, J.R.; Yan, R.; Zhou, Y.; Li, Q.; Fu, J.; Hu, Y.; Xie, S.Y. Evaluation of implementation of ten measurements for measles elimination in Zhejiang province. Chin. J. Vaccines Immun. 2015, 21, 46–50. (In Chinese) [Google Scholar]
- Karasek, E.; Rogalska, J.; Paradowska-Stankiewicz, I. Measles in Poland in 2010. Przegl. Epidemiol. 2012, 66, 185–190. [Google Scholar]
- Mohammadbeigi, A.; Zahraei, S.M.; Asgarian, A.; Afrashteh, S.; Mohammadsalehi, N.; Khazaei, S.; Ansari, H. Estimation of measles risk using the World Health Organization Measles Programmatic Risk Assessment Tool, Iran. Heliyon 2018, 4, e00886. [Google Scholar] [CrossRef]
- Liu, Y.; Chan, T.C.; Yap, L.W.; Luo, Y.; Xu, W.; Qin, S.; Zhao, N.; Yu, Z.; Geng, X.; Liu, S.L. Resurgence of scarlet fever in China: A 13-year population-based surveillance study. Lancet Infect. Dis. 2018, 18, 903–912. [Google Scholar] [CrossRef]
- Lamagni, T.; Guy, R.; Chand, M.; Henderson, K.L.; Chalker, V.; Lewis, J.; Saliba, V.; Elliot, A.J.; Smith, G.E.; Rushton, S.; et al. Resurgence of scarlet fever in England, 2014-16: A population-based surveillance study. Lancet Infect. Dis. 2018, 18, 180–187. [Google Scholar] [CrossRef]
- Kim, J.H.; Cheong, H.K. Increasing number of scarlet fever cases, South Korea, 2011–2016. Emerg. Infect. Dis. 2018, 24, 172–173. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.Q.; Lin, X.; Zeng, B.B.; Liu, B.Y.; He, F. Epidemiological analysis of viral hepatitis B in Zhejiang, 1991–2007. Dis. Surveill. 2010, 25, 263–266. (In Chinese) [Google Scholar]
- Ashraf, H.; Alam, N.H.; Rothermundt, C.; Brooks, A.; Bardhan, P.; Hossain, L.; Salam, M.A.; Hassan, M.S.; Beglinger, C.; Gyr, N. Prevalence and risk factors of hepatitis B and C virus infections in an impoverished urban community in Dhaka, Bangladesh. BMC Infect. Dis. 2010, 10, 208. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.Y.; Yu, Z.X. Epidemiological features analysis of notifiable infectious diseases in mainland China, 2010–2016. Henan J. Prev. Med. 2018, 29, 244–247. (In Chinese) [Google Scholar]
- Koh, W.M.; Bogich, T.; Siegel, K.; Jin, J.; Chong, E.Y.; Tan, C.Y.; Chen, M.I.; Horby, P.; Cook, A.R. The Epidemiology of Hand, Foot and Mouth Disease in Asia A Systematic Review and Analysis. Pediatr. Infect. Dis. J. 2016, 35, e285–e300. [Google Scholar] [CrossRef]
- Cao, Y.; Hong, Z.H.; Jin, L.M.; Ou, J.M.; Hong, R.T. Surveillance of hand foot and mouth disease in China, 2011–2012. Dis. Surveill. 2013, 28, 975–980. (In Chinese) [Google Scholar]
- Chang, Y.; Yan, H.M.; Liu, M.; Liu, J.Y. Research on the prevalence situation of the infectious diseases of preschool children in one community of Beijing. China Med. Herald 2013, 10, 118–123. (In Chinese) [Google Scholar]
- Su, Q.R.; Liu, J.; Ma, C.; Fan, C.X.; Wen, N.; Luo, H.M.; Wang, H.Q.; Li, L.; Hao, L.X. Epidemic profile of mumps in China during 2004–2013. Chin. J. Prev. Med. 2016, 50, 611–614. (In Chinese) [Google Scholar]
- WHO. World Now at the Start of 2009 Influenza Pandemic [EB/OL]. Available online: http://www.who.int/mediacentre/news/statements/2009/h1n1_pandemic_phase6_20090611/en/index.html (accessed on 9 October 2018).
- Lin, J.F.; Fang, L.; Fang, Q.S.; Yu, Z. Epidemiological Characteristics of Novel Influenza A(H1N1) in Zhejiang Province in 2009. Zhejiang Prev. Med. 2010, 22, 1–3. (In Chinese) [Google Scholar]
- Yu, Z.; Fang, Q.S.; Zhou, M. Surveillance of influenza in Zhejiang, 2008–2012. Dis. Surveill. 2012, 27, 689–693. (In Chinese) [Google Scholar]
- Maldonado, Y.A.; Zaoutis, T.E.; Banerjee, R.; Barnett, E.D.; Campbell, J.D.; Gerber, J.S.; Kourtis, A.P.; Lynfield, R.; Munoz, F.M.; Nolt, D.; et al. Recommendations for Prevention and Control of Influenza in Children, 2018–2019. Pediatrics 2018, 142, e20182367. [Google Scholar] [CrossRef]
- Blyth, C.C.; Macartney, K.K.; McRae, J.; Clark, J.E.; Marshall, H.S.; Buttery, J.; Francis, J.R.; Kotsimbos, T.; Kelly, P.M.; Cheng, A.C. Influenza Epidemiology, Vaccine Coverage and Vaccine Effectiveness in Children Admitted to Sentinel Australian Hospitals in 2017: Results from the PAEDS-FluCAN Collaboration. Clin. Infect. Dis. 2018, 21. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Cowling, B.J.; Feng, L.; Lau, E.H.; Liao, Q.; Tsang, T.K.; Peng, Z.; Wu, P.; Liu, F.; Fang, V.J.; et al. Human infection with avian influenza A H7N9 virus: An assessment of clinical severity. Lancet 2013, 382, 138–145. [Google Scholar] [CrossRef]
- Li, Q.; Zhou, L.; Zhou, M.H.; Chen, Z.P.; Li, F.R.; Wu, H.Y.; Xiang, N.J.; Chen, E.F.; Tang, F.Y.; Wang, D.Y.; et al. Epidemiology of human infections with avian influenza A (H7N9) virus in China. N. Engl. J. Med. 2014, 370, 520–532. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Yang, K.; Qi, X.; Xu, K.; Ji, H.; Ai, J.; Ge, A.; Wu, Y.; Li, Y.; Dai, Q.; et al. Spatial and temporal analysis of human infection with avian influenza A (H7N9) virus in China, 2013. Euro Surveill. 2013, 18. [Google Scholar] [CrossRef]
- Yu, X.L.; Zhang, X.; He, Y.; Wu, H.Y.; Gao, X.; Pan, Q.C.; Shen, J.R.; Zhu, J.M.; Chen, H.Y.; Zhu, Y.Y.; et al. Mild infection of a novel H7N9 avian influenza virus in children in Shanghai. Emerg. Microbes Infect. 2013, 2, e41. [Google Scholar] [CrossRef]
- Ke, Y.H.; Wang, Y.F.; Liu, S.W.; Guo, J.P.; Zhang, W.Y.; Yuan, X.T.; Zhang, N.; Wang, Z.J.; Song, H.B.; Huang, L.Y.; et al. High Severity and Fatality of Human Infections with Avian Influenza A (H7N9) Infection in China. Clin. Infect. Dis. 2013, 57, 1506–1507. [Google Scholar] [CrossRef]
- Liu, J.J.; Yao, H.Y.; Liu, E.Y. Analysis of factors affecting the epidemiology of tuberculosis in China. Int. J. Tuberc. Lung Dis. 2005, 9, 450–454. [Google Scholar]
- Guo, Q.; Su, X.M.; Wang, X.F.; Zhang, C.X.; Yu, M.; Zhang, Y.W. Assessment on reporting rate of notifiable infectious diseases in hospitals in China, 2013. Chin. J. Dis. Control Prev. 2015, 19, 683–687. (In Chinese) [Google Scholar]
- Jin, L.Z.; Ge, H.; Du, X.J.; Chen, M.; Yu, M.; Zheng, H.; Guo, Q. Reporting quality of notifiable communicable diseases in hospitals in China, 2015. Dis. Surveil. 2016, 31, 883–886. (In Chinese) [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Class B Disease | Class C Disease | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Number of Diseases | Number of Cases | Morbidity * | Number of Diseases | Number of Cases | Morbidity * | Number of Diseases | Number of Cases | Morbidity * | |
| 2008 | 15 | 17,193 | 185.34 | 6 | 125,506 | 1352.97 | 21 | 142,699 | 1538.32 |
| 2009 | 17 | 13,648 | 145.52 | 7 | 135,251 | 1442.12 | 24 | 148,899 | 1587.64 |
| 2010 | 17 | 7244 | 76.52 | 6 | 196,200 | 2072.5 | 23 | 203,444 | 2149.02 |
| 2011 | 19 | 7106 | 98.8 | 8 | 166,054 | 2308.85 | 27 | 173,160 | 2407.65 |
| 2012 | 19 | 4540 | 62.51 | 7 | 223,294 | 3074.24 | 26 | 227,834 | 3136.75 |
| 2013 | 18 | 4211 | 57.12 | 7 | 189,442 | 2569.74 | 25 | 193,653 | 2626.86 |
| 2014 | 16 | 3965 | 53.38 | 6 | 280,958 | 3782.17 | 22 | 284,923 | 3835.55 |
| 2015 | 18 | 5860 | 78.69 | 7 | 161,219 | 2164.88 | 25 | 167,079 | 2243.57 |
| 2016 | 17 | 4224 | 56.91 | 6 | 254,847 | 3433.46 | 23 | 259,071 | 3490.36 |
| 2017 | 17 | 4050 | 54.36 | 6 | 189,928 | 2549.03 | 23 | 193,978 | 2603.38 |
| Total | 22 | 72,041 | 90.39 | 10 | 1,922,699 | 2412.47 | 32 | 1,994,740 | 2502.87 |
| City | Population Density | Reported Cases Density |
|---|---|---|
| Jaixing | 1178.54 | 3.82 |
| Ningbo | 810.69 | 3.31 |
| Wenzhou | 760.46 | 2.85 |
| Taizhou | 646.05 | 2.74 |
| Shaoxing | 604.17 | 2.21 |
| Hangzhou | 553.63 | 1.70 |
| Huzhou | 511.17 | 1.65 |
| Jinhua | 504.48 | 1.61 |
| Zhoushan | 804.16 | 1.19 |
| Quzhou | 244.43 | 0.86 |
| Lishui | 125.16 | 0.52 |
| Disease Types | Reported Cases | Constituent Ratio (%) | Total Mortality (/100,000) | Deaths | Total Mortality (/100,000) |
|---|---|---|---|---|---|
| Class B infectious diseases | 72,041 | 3.61 | 90.39 | 138 | 0.17 |
| Intestinal infectious diseases | 23,764 | 1.19 | 29.82 | 1 | 0 |
| Respiratory infectious diseases | 36,735 | 1.84 | 46.09 | 31 | 0.04 |
| Blood-borne and sexually transmitted infectious diseases | 10,152 | 0.51 | 12.74 | 7 | 0.01 |
| Natural focal and insect-borne infectious diseases | 600 | 0.03 | 0.75 | 25 | 0.03 |
| Neonatal tetanus | 790 | 0.04 | 0.99 | 74 | 0.09 |
| Class C infectious diseases | 1,922,699 | 96.39 | 2412.47 | 128 | 0.16 |
| Total | 1,994,740 | 100.00 | 2502.87 | 266 | 0.33 |
| Year | Reported Cases | Morbidity * | Deaths | Mortality * | Severe Cases | Laboratory Diagnosed Cases | EV71 | CV-A16 | Other Enteroviruses |
|---|---|---|---|---|---|---|---|---|---|
| 2008 | 36,570 | 394.23 | 7 | 0.08 | 164 | 1455 | 804 | 63 | 588 |
| 2009 | 69,259 | 738.48 | 8 | 0.09 | 148 | 1085 | 461 | 433 | 191 |
| 2010 | 113,103 | 1194.73 | 37 | 0.39 | 1041 | 4338 | 2373 | 1316 | 649 |
| 2011 | 86,858 | 1207.69 | 24 | 0.33 | 251 | 3714 | 2089 | 743 | 882 |
| 2012 | 147,385 | 2029.15 | 17 | 0.23 | 111 | 4380 | 1735 | 1342 | 1303 |
| 2013 | 108108 | 1466.46 | 3 | 0.04 | 44 | 4383 | 975 | 396 | 3012 |
| 2014 | 211,697 | 2849.80 | 13 | 0.18 | 152 | 6619 | 2172 | 1491 | 2956 |
| 2015 | 99,821 | 1340.42 | 1 | 0.01 | 25 | 4258 | 690 | 813 | 2755 |
| 2016 | 185,205 | 2495.20 | 8 | 0.11 | 88 | 5969 | 1482 | 1541 | 2946 |
| 2017 | 81,980 | 1100.26 | 1 | 0.01 | 16 | 4515 | 1251 | 545 | 2719 |
| Total | 1,139,986 | 1430.38 | 119 | 0.15 | 2040 | 40,716 | 14,032 | 8683 | 18,001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, Q.; Ding, Z.; Wu, C.; Wu, H.; Lin, J. Analysis of Epidemiological Characteristics of Notifiable Diseases Reported in Children Aged 0–14 Years from 2008 to 2017 in Zhejiang Province, China. Int. J. Environ. Res. Public Health 2019, 16, 168. https://doi.org/10.3390/ijerph16020168
Lu Q, Ding Z, Wu C, Wu H, Lin J. Analysis of Epidemiological Characteristics of Notifiable Diseases Reported in Children Aged 0–14 Years from 2008 to 2017 in Zhejiang Province, China. International Journal of Environmental Research and Public Health. 2019; 16(2):168. https://doi.org/10.3390/ijerph16020168
Chicago/Turabian StyleLu, Qinbao, Zheyuan Ding, Chen Wu, Haocheng Wu, and Junfen Lin. 2019. "Analysis of Epidemiological Characteristics of Notifiable Diseases Reported in Children Aged 0–14 Years from 2008 to 2017 in Zhejiang Province, China" International Journal of Environmental Research and Public Health 16, no. 2: 168. https://doi.org/10.3390/ijerph16020168