
Comparison of Medical Comorbidity between Patients with Normal-Tension Glaucoma and Primary Open-Angle Glaucoma: A Population-Based Study in Taiwan

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
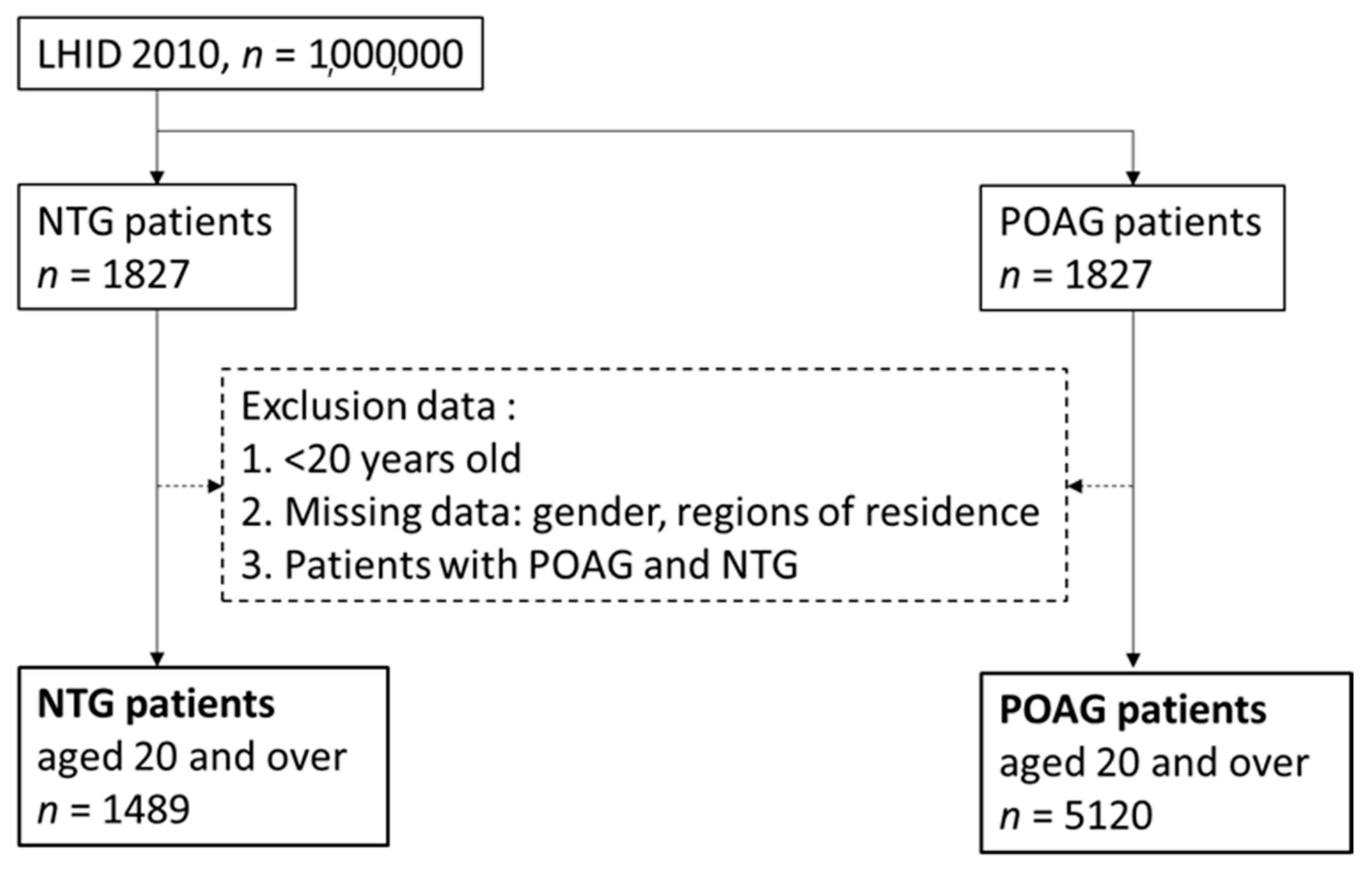
2.1. Data Source
2.2. Study Population
2.3. Comorbidities
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Quigley, H.A.; Broman, A.T. The number of people with glaucoma worldwide in 2010 and 2020. Br. J. Ophthalmol. 2006, 90, 262–267. [Google Scholar]
- Shon, K.; Wollstein, G.; Schuman, J.S.; Sung, K.R. Prediction of glaucomatous field progression: Pointwise analysis. Curr. Eye Res. 2014, 39, 705–710. [Google Scholar]
- Schuster, A.K.; Wagner, F.M.; Pfeiffer, N.; Hoffmann, E.M. Risk factors for open-angle glaucoma and recommendations for glaucoma screening. Der. Ophthalmol. 2021, 118, 145–152. [Google Scholar]
- Cedrone, C.; Culasso, F.; Cesareo, M.; Zapelloni, A.; Cedrone, P.; Cerulli, L. Prevalence of glaucoma in Ponza, Italy: A comparison with other studies. Ophthalmic Epidemiol. 1997, 4, 59–72. [Google Scholar]
- Mallick, J.; Devi, L.; Malik, P.K.; Mallick, J. Update on normal tension glaucoma. J. Ophthalmic Vis. Res. 2016, 11, 204–208. [Google Scholar]
- Ellong, A.; Mvogo, C.E.; Bella-Hiag, A.L.; Mouney, E.N.; Ngosso, A.; Litumbe, C.N. Prevalence of glaucomas in a black cameroonian population. Santé 2006, 16, 83–88. [Google Scholar]
- Baranwal, V.K.; Shyamsundar, K.; Kabuyaya, V.; Biswas, J.; Vannadil, H. Study of onchocerciasis-related visual impairment in North Kivu province of the Democratic Republic of Congo in Africa. Indian J. Ophthalmol. 2020, 68, 890–894. [Google Scholar]
- Ekstrom, C. Incidence of open-angle glaucoma in central Sweden. Acta Ophthalmol. 2008, 86, 747–754. [Google Scholar]
- Zhao, J.; Solano, M.M.; Oldenburg, C.E.; Liu, T.; Wang, Y.; Wang, N.; Lin, S.C. Prevalence of normal-tension glaucoma in the Chinese population: A systematic review and meta-analysis. Am. J. Ophthalmol. 2019, 199, 101–110. [Google Scholar]
- Cho, H.K.; Kee, C. Population-based glaucoma prevalence studies in Asians. Surv. Ophthalmol. 2014, 59, 434–447. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar]
- Bagyinszky, E.; Youn, Y.C.; An, S.S.A.; Kim, S. Mutations, associated with early-onset Alzheimer’s disease, discovered in Asian countries. Clin. Interv. Aging 2016, 11, 1467–1488. [Google Scholar]
- Catindig, J.A.S.; Venketasubramanian, N.; Ikram, M.K.; Chen, C. Epidemiology of dementia in Asia: Insights on prevalence, trends and novel risk factors. J. Neurol. Sci. 2012, 321, 11–16. [Google Scholar]
- Winder, A.F. Circulating lipoprotein and blood glucose levels in association with low-tension and chronic simple glaucoma. Br. J. Ophthalmol. 1977, 61, 641–645. [Google Scholar]
- Cui, Y.; Yang, X.; Zhang, G.; Guo, H.; Zhang, M.; Zhang, L.; Meng, Q. Intraocular pressure in general and diabetic populations from Southern China: The dongguan eye study. Investig. Ophthalmol. Vis. Sci. 2019, 60, 761–769. [Google Scholar]
- Grzybowski, A.; Och, M.; Kanclerz, P.; Leffler, C.; De Moraes, C.G. Primary open angle glaucoma and vascular risk factors: A review of population based studies from 1990 to 2019. J. Clin. Med. 2020, 9, 761. [Google Scholar]
- Kuo, C.Y.; Ko, Y.C.; Kuang, T.M.; Chou, P.; Chiou, S.H.; Liu, C.J.L. Prevalence of glaucoma in the elderly population in Taiwan: The shihpai eye study. J. Chin. Med Assoc. 2020, 83, 880–884. [Google Scholar]
- Igarashi, N.; Honjo, M.; Asano, S.; Takagi, K.; Aihara, M. Optic disc cupping characteristics of normal pressure hydrocephalus patients with normal-tension glaucoma. Sci. Rep. 2019, 9, 3108. [Google Scholar]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Ozal, D.; Iber, C.; Kapur, V.K.; Tangredi, M.M. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar]
- Lin, L.Y.; Charlotte, W.G.; Liam, S.; Chen, P.C. Data resource profile: The national health insurance research database (NHIRD). Epidemiol. Health 2018, 40, e2018062. [Google Scholar]
- Hsieh, C.Y.; Su, C.C.; Shao, S.C.; Sung, S.F.; Lin, S.J.; Kao Yang, Y.H.; Lai, E.C. Taiwan’s national health insurance research database: Past and future. Clin. Epidemiol. 2019, 3, 349–358. [Google Scholar]
- Lee, J.; Kim, Y.K.; Jeoung, J.W.; Ha, A.; Kim, Y.W.; Park, K.H. Machine learning classifiers-based prediction of normal-tension glaucoma progression in young myopic patients. Jpn. J. Ophthalmol. 2020, 64, 68–76. [Google Scholar]
- Zhang, N.; Wang, J.; Li, Y.; Jiang, B. Prevalence of primary open angle glaucoma in the last 20 years: A meta-analysis and systematic review. Sci. Rep. 2021, 11, 13762. [Google Scholar]
- Adlina, A.R.; Alisa-Victoria, K.; Shatriah, I.; Liza-Sharmini, A.T.; Ahmad, M.S. Optic disc topography in Malay patients with normal-tension glaucoma and primary open-angle glaucoma. Clin. Ophthalmol. 2014, 8, 2533–2539. [Google Scholar]
- Chen, Y.Y.; Lai, Y.J.; Yen, Y.F.; Shen, Y.C.; Wang, C.Y.; Liang, C.Y.; Fan, L.W. Association between normal tension glaucoma and the risk of Alzheimer’s disease: A nationwide population-based cohort study in Taiwan. BMJ Open 2018, 8, e022987. [Google Scholar]
- Lee, J.; Ahn, E.J.; Kim, Y.W.; Ha, A.; Kim, Y.K.; Jeoung, J.W.; Park, K.H. Impact of myopia on the association of long-term intraocular pressure fluctuation with the rate of progression in normal-tension glaucoma. Br. J. Ophthalmol. 2021, 105, 653–660. [Google Scholar]
- Moreno, V.; Nucci, C.; Dolz-Marco, R.; Zanón-Moreno, V.; Nucci, C.; Dolz-Marco, R.; Díaz-Llópis, M. Oxidative stress and its downstream signaling in aging eyes. Clin. Interv. Aging 2014, 9, 637–652. [Google Scholar]
- Nitta, E.; Hirooka, K.; Tenkumo, K.; Fujita, T.; Nishiyama, A.; Nakamura, T.; Shiraga, F. Aldosterone: A mediator of retinal ganglion cell death and the potential role in the pathogenesis in normal-tension glaucoma. Cell Death Dis. 2013, 4, e711. [Google Scholar]
- Yilmaz, N.; Deniz, T.C.; Asli, B.; Erol, M.K.; Ellidag, H.Y.; Giray, O.; Eren, E. Higher serum lipids and oxidative stress in patients with normal tension glaucoma, but not pseudoexfoliative glaucoma. Bosn. J. Basic Med Sci. 2016, 16, 21–27. [Google Scholar]
- Cao, Q.; Rui, G.; Liang, Y. Study on PM2.5 pollution and the mortality due to lung cancer in China based on geographic weighted regression model. BMC Public Health 2018, 18, 925. [Google Scholar]
- Nwanaji-Enwerem, J.C.; Wang, W.; Nwanaji-Enwerem, O.; Vokonas, P.; Baccarelli, A.; Weisskopf, M.; Schwartz, J. Association of long-term ambient black carbon exposure and oxidative stress allelic variants with intraocular pressure in older men. JAMA Ophthalmol. 2019, 137, 129–137. [Google Scholar]
- Noriko, H.; Hiroshi, K.; Yukihiro, S.; Omodaka, K.; Maruyama, K.; Takahashi, H.; Nakazawa, T. The association between systemic oxidative stress and ocular blood flow in patients with normal-tension glaucoma. Graefe’s Arch. Clin. Exp. Ophthalmol. 2016, 254, 333–341. [Google Scholar]
- Fan, N.; Wang, P.; Tang, L.; Liu, X. Ocular blood flow and normal tension glaucoma. Biomed Res. Int. 2015, 2015, 308505. [Google Scholar]
- Nakazawa, T. Ocular blood flow and influencing factors for glaucoma. Asia Pac. J. Ophthalmol. 2016, 5, 38–44. [Google Scholar]
- Sano, H.; Namekata, K.; Kimura, A.; Shitara, H.; Guo, X.; Harada, C.; Harada, T. Differential effects of N-acetylcysteine on retinal degeneration in two mouse models of normal tension glaucoma. Cell Death Dis. 2019, 10, 75. [Google Scholar]
- Mozaffarieh, M.; Grieshaber, M.C.; Flammer, J. Oxygen and blood flow: Players in the pathogenesis of glaucoma. Mol. Vis. 2008, 14, 224–233. [Google Scholar]
- Mozaffarieh, M.; Flammer, J. New insights in the pathogenesis and treatment of normal tension glaucoma. Curr. Opin. Pharmacol. 2013, 13, 43–49. [Google Scholar]
- Samsudin, A.; Isaacs, N.; Tai, M.L.S.; Ramli, N.; Mimiwati, Z.; Choo, M.M. Ocular perfusion pressure and ophthalmic artery flow in patients with normal tension glaucoma. BMC Ophthalmol. 2016, 16, 39. [Google Scholar]
- Choi, J.; Kim, K.H.; Jeong, J.; Cho, H.S.; Lee, C.H.; Kook, M.S. Circadian fluctuation of mean ocular perfusion pressure is a consistent risk factor for normal-tension glaucoma. Investig. Ophthalmol. Vis. Sci. 2007, 48, 104–111. [Google Scholar]
- Okumura, Y.; Yuki, K.; Tsubota, K. Low diastolic blood pressure is associated with the progression of normal-tension glaucoma. Ophthalmologica 2012, 228, 36–41. [Google Scholar]
- Mojon, D.S.; Hess, C.W.; Goldblum, D.; Böhnke, M.; Körner, F.; Mathis, J. Primary open-angle glaucoma is associated with sleep apnea syndrome. Ophthalmologica 2000, 214, 115–118. [Google Scholar]
- Onen, S.H.; Mouriaux, F.; Berramdane, L.; Dascotte, J.C.; Kulik, J.F.; Rouland, J.F. High prevalence of sleep-disordered breathing in patients with primary open-angle glaucoma. Acta Ophthalmol. Scand 2000, 78, 638–641. [Google Scholar]
- Marcus, D.M.; Costarides, A.P.; Gokhale, P.; Papastergiou, G.; Miller, J.J.; Johnson, M.H.; Chaudhary, B.A. Sleep disorders: A risk factor for normal-tension glaucoma? J. Glaucoma 2001, 10, 177–183. [Google Scholar]
- Mojon, D.S.; Hess, C.W.; Goldblum, D.; Boehnke, M.; Koerner, F.; Gugger, M.; Mathis, J. Normal-tension glaucoma is associated with sleep apnea syndrome. Ophthalmologica 2002, 216, 180–184. [Google Scholar]
- Bilgin, G. Normal-tension glaucoma and obstructive sleep apnea syndrome: A prospective study. BMC Ophthalmol. 2014, 14, 27. [Google Scholar]
- Yu, J.G.; Mei, Z.M.; Ye, T.; Feng, Y.F.; Zhao, F.; Jia, J.; Xiang, Y. Changes in retinal nerve fiber layer thickness in obstructive sleep apnea/hypopnea syndrome: A metaanalysis. Ophthalmic Res. 2016, 56, 57–67. [Google Scholar]
- Chuang, L.H.; Koh, Y.Y.; Hery Chen, S.L.; Lo, Y.L.; Yu, C.C.; Yeung, L.; Lai, C.C. Normal tension glaucoma in obstructive sleep apnea syndrome: A structural and functional study. Medicine. 2020, 99, e19468. [Google Scholar]
- Lin, H.C.; Chien, C.W.; Hu, C.C.; Ho, J.D. Comparison of comorbid conditions between open-angle glaucoma patients and a control cohort: A case-control study. Ophthalmology 2010, 117, 2088–2095. [Google Scholar]
- Chen, H.Y.; Lin, C.L. Comparison of medical comorbidity between patients with primary angle-closure glaucoma and a control cohort: A population-based study from Taiwan. BMJ Open 2019, 9, e024209. [Google Scholar]
- Zullo, A.; Ridola, L.; Hassan, C.; Bruzzese, V.; Papini, F.; Vaira, D. Glaucoma and helicobacter: Eyes wide shut? Dig. Liver Dis. 2012, 44, 627–628. [Google Scholar]
- Deshpande, N.; Lalitha, P.; Krishna Das, S.R.; Pillai, R.M.; Robin, A. Helicobacter pylori IgG antibodies in aqueous humor and serum of subjects with primary open angle and pseudo-exfoliation glaucoma in a South Indian population. J. Glaucoma 2008, 17, 605–610. [Google Scholar]
- Zavos, C.; Kountouras, J.; Sakkias, G.; Venizelos, I.; Deretzi, G.; Arapoglou, S. Histological presence of Helicobacter pylori bacteria in the trabeculum and iris of patients with primary open-angle glaucoma. Ophthalmic Res. 2011, 47, 150–156. [Google Scholar]
- Galloway, P.H.; Simon, J.W.; Muhammad, G.M.; Mikelberg, F.S. Helicobacter pylori infection and the risk for open-angle glaucoma. Ophthalmology 2003, 110, 922–925. [Google Scholar]
- Kersey, J.P.; Broadway, D.C. Corticosteroid-induced glaucoma: A review of the literature. Eye 2006, 20, 407–416. [Google Scholar]
- Kountouras, J.; Mylopoulos, N.; Boura, P.; Bessas, C.; Chatzopoulos, D.; Venizelos, J.; Zavos, C. Relationship between Helicobacter pylori infection and glaucoma. Ophthalmology 2001, 108, 599–604. [Google Scholar]
- Chung, S.D.; Lin, H.C.; Hung, S.H. Allergic Rhinitis is Associated with open-angle glaucoma: A population-based case–control study. Am. J. Rhinol. Allergy 2014, 28, e148–e151. [Google Scholar]
- Hiramoto, K.; Kobayashi, H.; Orita, K.; Sato, E.F.; Ishii, M. Inducible nitric oxide synthase plays important roles in allergic reactions of pollinosis in mice sensitized with pollen allergy. J. Clin. Biochem. Nutr. 2013, 52, 17–21. [Google Scholar]
- Garrelds, I.M.; van Amsterdam, J.G.; de Graaf-in’t Veld, C.; Van Wijk, R.G.; Zijlstra, F.J. Nitric oxide metabolites in nasal lavage fluid of patients with house dust mite allergy. Thorax 1995, 50, 275–279. [Google Scholar]
- Cellini, M.; Strobbe, E.; Gizzi, C.; Balducci, N.; Toschi, P.G.; Campos, E.C. Endothelin-1 plasma levels and vascular endothelial dysfunction in primary open angle glaucoma. Life Sci. 2012, 91, 699–702. [Google Scholar]


{kind=link}
| Confounding Variables | POAG (n = 5120) | NTG (n = 1489) | p-Value | ||
|---|---|---|---|---|---|
| Gender | |||||
| Female | 2556 | (49.92%) | 713 | (47.88%) | 0.1664 |
| Male | 2564 | (50.08%) | 776 | (52.12%) | |
| Age | |||||
| 20–34 years old | 794 | (15.51%) | 214 | (14.37%) | 0.2323 |
| 35–49 years old | 1127 | (22.01%) | 312 | (20.95%) | |
| 50–64 years old | 1519 | (29.67%) | 481 | (32.3%) | |
| 65 years old and over | 1680 | (32.81%) | 482 | (32.37%) | |
| Low income | |||||
| Yes | 3184 | (62.19%) | 872 | (58.56%) | 0.0115 |
| No | 1936 | (37.81%) | 617 | (41.44%) | |
| Urbanization level | |||||
| Highly urbanized | 1886 | (36.84%) | 646 | (43.38%) | 0.0005 |
| Moderate urbanization | 1646 | (32.15%) | 408 | (27.4%) | |
| Emerging town | 712 | (13.91%) | 191 | (12.83%) | |
| General town | 537 | (10.49%) | 143 | (9.6%) | |
| Aged Township | 84 | (1.64%) | 20 | (1.34%) | |
| Agricultural town | 130 | (2.54%) | 42 | (2.82%) | |
| Remote township | 125 | (2.44%) | 39 | (2.62%) | |
| Comorbidities | |||||
| Arterial hypertension | 1671 | (32.64%) | 444 | (29.82%) | 0.0402 |
| Hypotension | 33 | (0.64%) | 22 | (1.48%) | 0.2590 |
| Ischemic heart disease | 87 | (1.7%) | 20 | (1.34%) | 0.3380 |
| Sleep disturbances | 1145 | (22.36%) | 441 | (29.62%) | <0.0001 |
| Ischemic stroke | 46 | (0.9%) | 17 | (1.14%) | 0.3952 |
| Alzheimer disease | 4 | (0.08%) | 1 | (0.07%) | 0.8923 |
| Diabetes | 1200 | (23.44%) | 308 | (20.69%) | 0.0259 |
| Parkinson’s disease | 76 | (1.48%) | 17 | (1.14%) | 0.3231 |
| Coronary heart disease | 859 | (16.78%) | 283 | (19.01%) | 0.0453 |
| Peripheral artery disease | 67 | (1.31%) | 23 | (1.54%) | 0.4891 |
| Atrial fibrillation | 60 | (1.17%) | 29 | (1.95%) | 0.0223 |
| Headaches | 1375 | (26.86%) | 458 | (30.76%) | 0.0031 |
| Migraines | 134 | (2.62%) | 61 | (4.1%) | 0.0030 |
| Epilepsy and recurrent | 45 | (0.88%) | 13 | (0.87%) | 0.9830 |
| Rheumatoid arthritis | 87 | (1.7%) | 27 | (1.81%) | 0.7660 |
| Systemic lupus erythematosus | 2 | (0.04%) | 1 | (0.07%) | 0.6542 |
| Chronic kidney disease | 125 | (2.44%) | 40 | (2.69%) | 0.5939 |
| Hepatitis B | 159 | (3.11%) | 55 | (3.69%) | 0.2590 |
| Fluid, electrolyte, acid–base disorders | 34 | (0.66%) | 12 | (0.81%) | 0.5623 |
| Tuberculosis | 43 | (0.84%) | 15 | (1.01%) | 0.5418 |
| Peptic ulcer | 913 | (17.83%) | 368 | (24.71%) | <0.0001 |
| Depression | 89 | (1.74%) | 23 | (1.54%) | 0.6104 |
| Malignant disease | 349 | (6.82%) | 131 | (8.8%) | 0.0095 |
| Allergic rhinitis | 1029 | (20.1%) | 431 | (28.95%) | <0.0001 |
| Allergic conjunctivitis | 191 | (3.73%) | 47 | (3.16%) | 0.8363 |
| Atopic dermatitis | 1617 | (31.58%) | 448 | (30.09%) | 0.0045 |
| NTG | p-Value | |
|---|---|---|
| Confounding Variables | Adjusted OR (95%CI) | |
| Gender (reference: female) | ||
| Male | 1.111 (0.985–1.253) | 0.0874 |
| Age (reference: 20–34 years old) | ||
| 35–49 years old | 0.957 (0.780–1.174) | 0.6708 |
| 50–64 years old | 1.137 (0.932–1.386) | 0.2054 |
| 65 years old and over | 1.038 (0.840–1.282) | 0.7315 |
| Low-income (reference: No) | ||
| Yes | 0.876 (0.773–0.992) | 0.0368 |
| Urbanization level (reference: Moderate urbanization) | ||
| Highly urbanized | 1.399 (1.213–1.613) | <0.0001 |
| Emerging town | 1.100 (0.904–1.337) | 0.3417 |
| General town | 1.060 (0.851–1.319) | 0.6047 |
| Aged Township | 0.992 (0.596–1.651) | 0.9751 |
| Agricultural town | 1.257 (0.864–1.828) | 0.2319 |
| Remote township | 0.950 (0.615–1.469) | 0.8187 |
| Comorbidities (reference: without) | ||
| Arterial hypertension | 0.767 (0.660–0.893) | 0.0006 |
| Hypotension | 1.984 (1.128–3.490) | 0.0174 |
| Ischemic heart disease | 0.656 (0.391–1.100) | 0.1097 |
| Sleep disturbances | 1.323 (1.146–1.528) | 0.0001 |
| Ischemic stroke | 1.276 (0.715–2.278) | 0.4100 |
| Alzheimer disease | 0.727 (0.076–6.913) | 0.7813 |
| Diabetes | 0.850 (0.728–0.993) | 0.0400 |
| Parkinson’s disease | 0.674 (0.389–1.168) | 0.1595 |
| Coronary heart disease | 1.139 (0.952–1.363) | 0.1538 |
| Peripheral artery disease | 1.120 (0.683–1.835) | 0.6542 |
| Atrial fibrillation | 1.511 (0.944–2.419) | 0.0855 |
| Headaches | 1.023 (0.889–1.178) | 0.7465 |
| Migraines | 1.296 (0.935–1.794) | 0.1192 |
| Epilepsy and recurrent | 0.910 (0.483–1.713) | 0.7702 |
| Rheumatoid arthritis | 0.895 (0.565–1.416) | 0.6353 |
| Systemic lupus erythematosus | 1.646 (0.140–19.290) | 0.6915 |
| Chronic kidney disease | 1.062 (0.726–1.554) | 0.7574 |
| Hepatitis B | 1.057 (0.766–1.458) | 0.7361 |
| Fluid, electrolyte, acid–base disorders | 1.086 (0.544–2.167) | 0.8150 |
| Tuberculosis | 1.099 (0.600–2.011) | 0.7598 |
| Peptic ulcer | 1.383 (1.188–1.609) | <0.0001 |
| Depression | 0.728 (0.450–1.178) | 0.1964 |
| Malignant disease | 1.200 (0.964–1.494) | 0.1022 |
| Allergic rhinitis | 1.484 (1.290–1.707) | <0.0001 |
| Allergic conjunctivitis | 0.778 (0.558–1.085) | 0.1396 |
| Atopic dermatitis | 0.869 (0.763–0.990) | 0.0350 |
| Confounding Variables | Adjusted OR (95%CI) | ||||||
|---|---|---|---|---|---|---|---|
| Arterial Hypertension | Hypotension | Sleep Disturbances | Diabetes | Peptic Ulcer | Allergic Rhinitis | Atopic Dermatitis | |
| Gender | |||||||
| Female | 0.727 (0.579–0.913) * | 1.999 (0.898–4.452) | 1.296 (1.060–1.585) * | 0.743 (0.589–0.938) * | 1.338 (1.076–1.665) * | 1.486 (1.216–1.816) * | 0.848 (0.707–1.017) |
| Male | 0.816 (0.665–1.002) | 1.786 (0.792–4.028) | 1.371 (1.113–1.688) * | 0.959 (0.776–1.184) | 1.451 (1.172–1.796) * | 1.464 (1.201–1.785) * | 0.898 (0.744–1.085) |
| Age | |||||||
| 20–35 years old | 0.375 (0.046–3.070) * | 7.275 (0.679–77.911) | 1.152 (0.630–2.109) | 0.645 (0.216–1.927) | 1.258 (0.587–2.697) | 1.641 (1.144–2.352) * | 0.994 (0.716–1.380) |
| 35–49 years old | 0.568 (0.361–0.894) * | 2.128 (0.638–7.096) | 1.208 (0.866–1.686) | 0.795 (0.515–1.228) | 1.252 (0.861–1.821) | 1.596 (1.174–2.172) * | 0.910 (0.685–1.208) |
| 50–64 years old | 0.775 (0.604–0.993) * | 1.935 (0.634–5.906) | 1.283 (0.994–1.657) * | 0.914 (0.709–1.180) | 1.508 (1.159–1.963) * | 1.537 (1.184–1.995) * | 0.711 (0.557–0.908) * |
| 65 years old and over | 0.870 (0.695–1.089) | 1.565 (0.633–3.870) | 1.522 (1.211–1.913) * | 0.838 (0.664–1.057) | 1.364 (1.083–1.718) * | 1.342 (1.046–1.721) * | 0.923 (0.730–1.165) |
| Low-income | |||||||
| Yes | 0.786 (0.647–0.954) * | 1.718 (0.829–3.559) | 1.267 (1.053–1.525) * | 0.841 (0.692–1.022) | 1.420 (1.167–1.728) * | 1.435 (1.198–1.720) | 0.956 (0.809–1.129) |
| No | 0.726 (0.568–0.929) * | 2.363 (0.930–6.003) | 1.451 (1.151–1.830) * | 0.871 (0.673–1.129) | 1.341 (1.052–1.708) * | 1.583 (1.263–1.985) | 0.740 (0.598–0.916)* |
| Urbanization level | |||||||
| Highly urbanized | 0.816 (0.641–1.039) | 3.87 (1.384–10.825) * | 1.390 (1.105–1.748) * | 0.911 (0.714–1.164) | 1.306 (1.023–1.668) * | 1.434 (1.151–1.788) * | 0.831 (0.681–1.014) |
| Moderate urbanization | 0.910 (0.689–1.203) | 2.056 (0.692–6.104) | 1.248 (0.956–1.629) | 0.734 (0.544–0.991) | 1.264 (0.949–1.684) | 1.550 (1.198–2.005) * | 0.974 (0.763–1.244) |
| Emerging town | 0.588 (0.373–0.928) * | 3.826 (0.996–14.699) | 1.025 (0.663–1.584) | 0.905 (0.574–1.427) | 1.722 (1.116–2.657) * | 1.839 (1.226–2.760) * | 0.935 (0.640–1.365) |
| General town | 0.369 (0.218–0.627) * | 0.214 (0.022–2.118) | 1.642 (1.001–2.692) * | 1.094 (0.658–1.821) | 2.340 (1.394–3.927) * | 1.433 (0.875–2.347) | 0.938 (0.600–1.466) |
| Aged township | 0.056 (0.005–0.634) * | - | 9.822 (1.395–69.157) * | 0.131 (0.006–2.944) | 1.402 (0.219–8.951) | 11.113 (0.613–201.385) | 0.309 (0.061–1.563) |
| Agricultural town | 0.488 (0.176–1.353) | - | 2.402 (0.845–6.828) | 1.861 (0.632–5.481) | 0.656 (0.198–2.179) | 0.716 (0.236–2.175) | 0.911 (0.292–2.842) |
| Remote township | 1.145 (0.321–4.085) | - | 0.851 (0.237–3.055) | 0.933 (0.229–3.793) | 0.456 (0.125–1.665) | 0.714 (0.235–2.168) | 0.404 (0.114–1.432) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, W.-Y.; Luo, C.-W.; Chen, S.-T.; Kuan, Y.-H.; Yang, S.-F.; Sun, H.-Y. Comparison of Medical Comorbidity between Patients with Normal-Tension Glaucoma and Primary Open-Angle Glaucoma: A Population-Based Study in Taiwan. Healthcare 2021, 9, 1509. https://doi.org/10.3390/healthcare9111509
Lu W-Y, Luo C-W, Chen S-T, Kuan Y-H, Yang S-F, Sun H-Y. Comparison of Medical Comorbidity between Patients with Normal-Tension Glaucoma and Primary Open-Angle Glaucoma: A Population-Based Study in Taiwan. Healthcare. 2021; 9(11):1509. https://doi.org/10.3390/healthcare9111509
Chicago/Turabian StyleLu, Wei-Yang, Ci-Wen Luo, Shyan-Tarng Chen, Yu-Hsiang Kuan, Shun-Fa Yang, and Han-Yin Sun. 2021. "Comparison of Medical Comorbidity between Patients with Normal-Tension Glaucoma and Primary Open-Angle Glaucoma: A Population-Based Study in Taiwan" Healthcare 9, no. 11: 1509. https://doi.org/10.3390/healthcare9111509