
Staff-Facilitated Telemedicine Care Delivery for Treatment of Hepatitis C Infection among People Who Inject Drugs
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Background and Rationale
1.2. Objectives
2. Materials and Methods
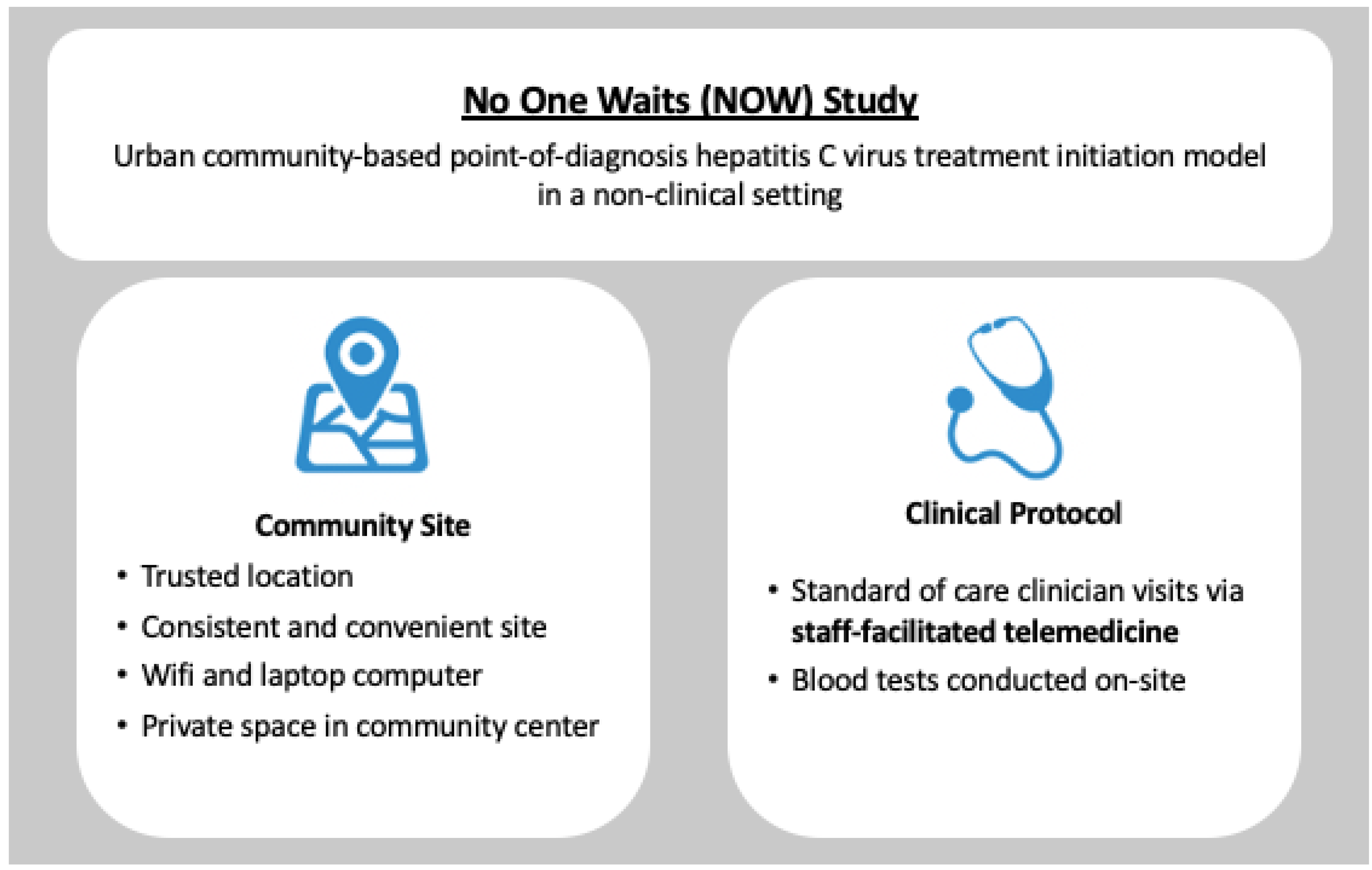
2.1. Study Design
2.2. Setting
2.3. Population to Be Studied and Eligibility Criteria
2.4. Recruitment and Consent
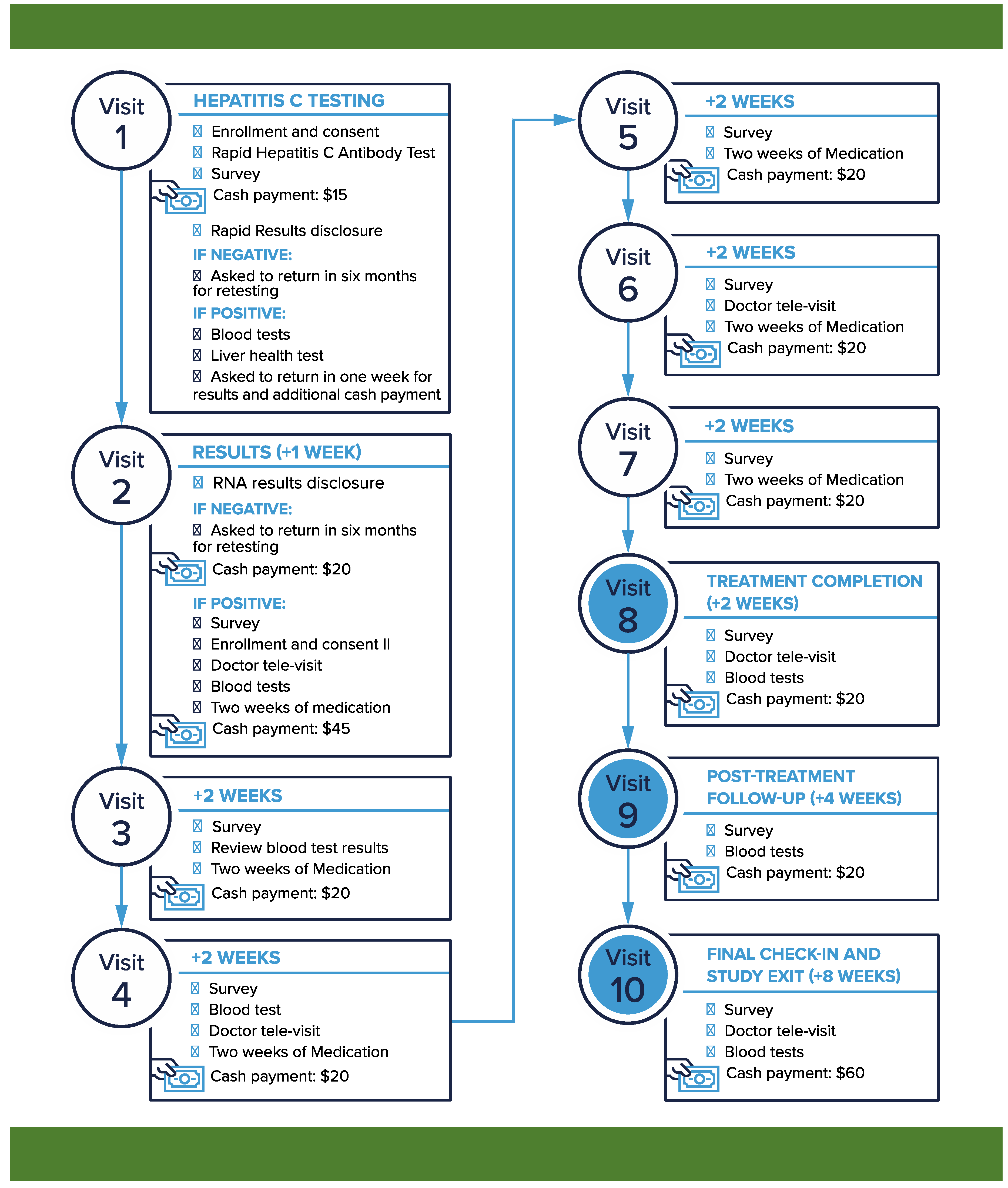
2.5. HCV Telemedicine Intervention
2.6. Staff Members’ Training
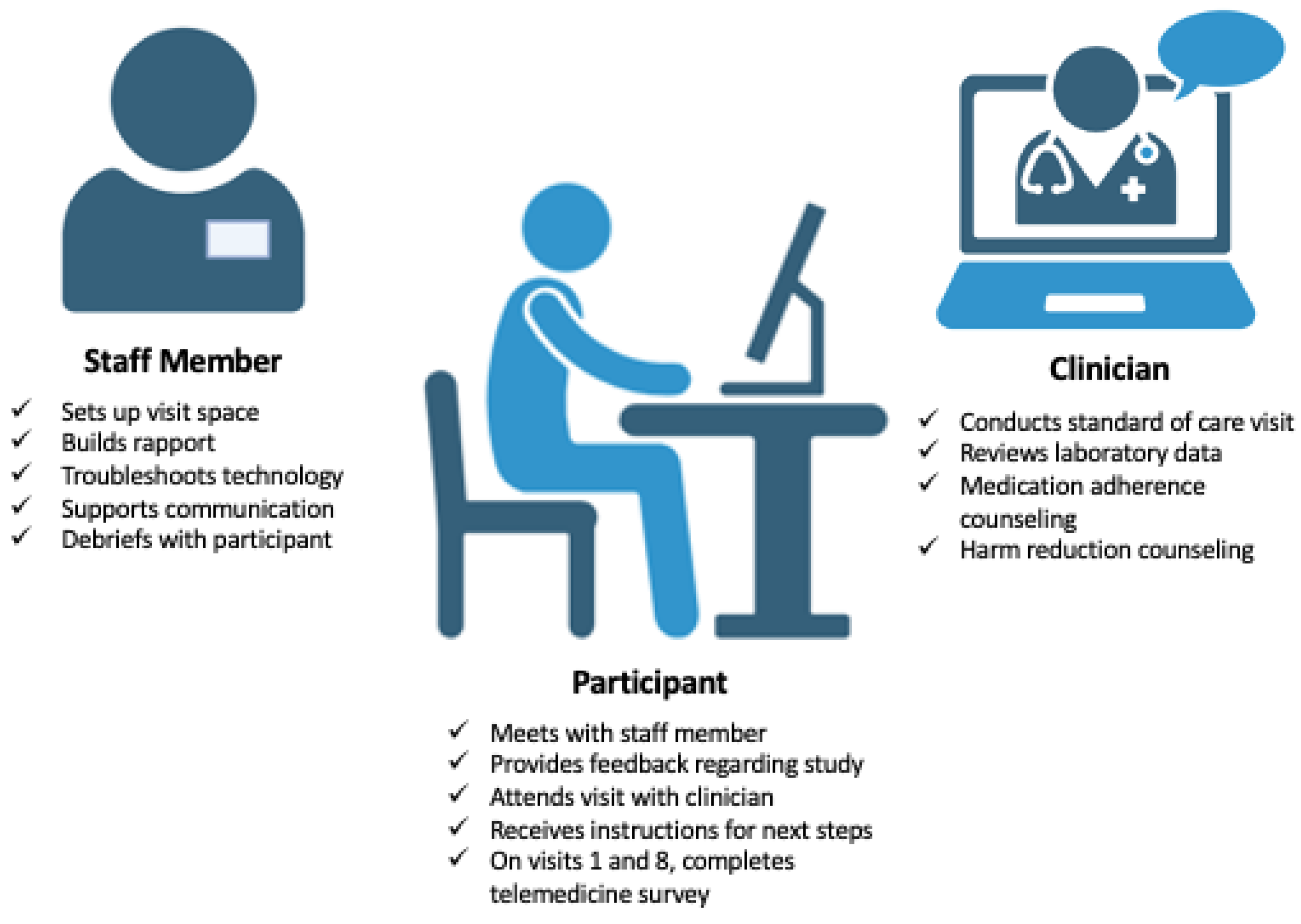
2.7. Staff Members’ Roles
2.7.1. Set up Visit Space
2.7.2. Build Rapport
2.7.3. Troubleshoot Technology
2.7.4. Support Communication between Provider and Participant
2.7.5. Debrief with Participant
2.8. Participants’ Experience
2.9. Clinician’s Approach
2.10. Objectives of Clinic Visits
2.11. Data Management and Analysis
3. Discussion
3.1. Strengths and Limitations of the Study
3.2. Dissemination Plan
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- The Polaris Observatory HCV Collaborators. Global change in hepatitis C virus prevalence and cascade of care between 2015 and 2020: A modelling study. Lancet Gastroenterol. Hepatol. 2022, 7, 396–415. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Wong, G.; Anstee, Q.M.; Henry, L. The Global Burden of Liver Disease. Clin. Gastroenterol. Hepatol. 2023, 21, 1978–1991. [Google Scholar] [CrossRef] [PubMed]
- Zibbell, J.E.; Asher, A.K.; Patel, R.C.; Kupronis, B.; Iqbal, K.; Ward, J.W.; Holtzman, D. Increases in Acute Hepatitis C Virus Infection Related to a Growing Opioid Epidemic and Associated Injection Drug Use, United States, 2004 to 2014. Am. J. Public Health 2018, 108, 175–181. [Google Scholar] [CrossRef]
- Noska, A.J.; Belperio, P.S.; Loomis, T.P.; O’Toole, T.P.; Backus, L.I. Prevalence of Human Immunodeficiency Virus, Hepatitis C Virus, and Hepatitis B Virus Among Homeless and Nonhomeless United States Veterans. Clin. Infect. Dis. 2017, 65, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Page, K.; Yu, M.; Cohen, J.; Evans, J.; Shumway, M.; Riley, E.D. HCV screening in a cohort of HIV infected and uninfected homeless and marginally housed women in San Francisco, California. BMC Public Health 2017, 17, 171. [Google Scholar] [CrossRef] [PubMed]
- Facente, S.N.; Burk, K.; Eagen, K.; Mara, E.S.; Smith, A.A.; Lynch, C.S. New Treatments Have Changed the Game: Hepatitis C Treatment in Primary Care. Infect. Dis. Clin. N. Am. 2018, 32, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Litwin, A.H.; Lum, P.J.; Taylor, L.E.; Mehta, S.H.; Tsui, J.I.; Feinberg, J.; Kim, A.Y.; Norton, B.L.; Heo, M.; Arnsten, J.; et al. Patient-centred models of hepatitis C treatment for people who inject drugs: A multicentre, pragmatic randomised trial. Lancet Gastroenterol. Hepatol. 2022, 7, 1112–1127. [Google Scholar] [CrossRef]
- Conway, A.; Valerio, H.; Alavi, M.; Silk, D.; Treloar, C.; Hajarizadeh, B.; Marshall, A.D.; Martinello, M.; Milat, A.; Dunlop, A.; et al. A Testing Campaign Intervention Consisting of Peer-Facilitated Engagement, Point-of-Care HCV RNA Testing, and Linkage to Nursing Support to Enhance Hepatitis C Treatment Uptake among People Who Inject Drugs: The ETHOS Engage Study. Viruses 2022, 14, 1555. [Google Scholar] [CrossRef]
- Grebely, J.; Gilliver, R.; McNaughton, T.; Conway, A.; Cunningham, E.; Henderson, C.; Hadlow, B.; Molloy, K.; Doab, A.; Tillakeratne, S.; et al. Single-visit hepatitis C point-of-care testing, linkage to nursing care, and peer-supported treatment among people with recent injecting drug use at a peer-led needle and syringe program: The TEMPO Pilot Study. Int. J. Drug Policy 2023, 114, 103982. [Google Scholar] [CrossRef]
- The Chartis Groups and Kythera Labs. Telehealth Tracker: New Normal Rate for Telehealth Adoption. 31 October 2022. Available online: https://www.chartis.com/insights/telehealth-tracker-new-normal-rate-telehealth-adoption (accessed on 6 September 2023).
- Nouri, S.; Khoong, E.C.; Lyles, C.R.; Karliner, L. Addressing equity in telemedicine for chronic disease management during the COVID-19 pandemic. NEJM Catal. Innov. Care Deliv. 2020, 1. [Google Scholar]
- Telehealth.HHS.gov—Telehealth Policy Updates. Updated 11 May 2023. Available online: https://telehealth.hhs.gov/providers/telehealth-policy/telehealth-policy-updates#:%E2%88%BC:text=The%20Consolidated%20Appropriations%20Act%20of%202023%20allows%20patients%20with%20High,to%20meet%20their%20minimum%20deductible (accessed on 6 September 2023).
- Sanchez, K.; Kitzman, H.; Khan, M.; da Graca, B.; Zsohar, J.; McStay, F. Use of Telehealth Early and Late in the COVID-19 Public Health Emergency: Policy Implications for Improving Health Equity. J. Am. Board. Fam. Med. 2023, 36, 746–754. [Google Scholar] [CrossRef]
- Zahir, A.; Yip, D.; Garcia, C.; Smith, A.N.; Dhatt, Z.; Duke, M.; Kushel, M. “I Needed for You to See What I’m Talking About”: Experiences with Telehealth among Homeless-Experienced Older Adults. Gerontol. Geriatr. Med. 2023, 9, 23337214231172650. [Google Scholar] [CrossRef] [PubMed]
- Bekasi, S.; Girasek, E.; Gyorffy, Z. Telemedicine in community shelters: Possibilities to improve chronic care among people experiencing homelessness in Hungary. Int. J. Equity Health 2022, 21, 181. [Google Scholar] [CrossRef] [PubMed]
- Adams, C.S.; Player, M.S.; Berini, C.R.; Perkins, S.; Fay, J.; Walker, L.; Buffalo, E.; Roach, C.; Diaz, V.A. A Telehealth Initiative to Overcome Health Care Barriers for People Experiencing Homelessness. Telemed. J. E Health 2021, 27, 851–858. [Google Scholar] [CrossRef] [PubMed]
- Haridy, J.; Iyngkaran, G.; Nicoll, A.; Hebbard, G.; Tse, E.; Fazio, T. eHealth Technologies for Screening, Diagnosis, and Management of Viral Hepatitis: A Systematic Review. Clin. Gastroenterol. Hepatol. 2021, 19, 1139–1150.e30. [Google Scholar] [CrossRef] [PubMed]
- Talal, A.H.; Andrews, P.; McLeod, A.; Chen, Y.; Sylvester, C.; Markatou, M.; Brown, L.S. Integrated, Co-located, Telemedicine-based Treatment Approaches for Hepatitis C Virus Management in Opioid Use Disorder Patients on Methadone. Clin. Infect. Dis. 2019, 69, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Paredes, D.; Amoako, A.; Ekmekjian, T.; Engler, K.; Lebouche, B.; Klein, M.B. Interventions to Improve Uptake of Direct-Acting Antivirals for Hepatitis C Virus in Priority Populations: A Systematic Review. Front. Public Health 2022, 10, 877585. [Google Scholar] [CrossRef] [PubMed]
- Talal, A.H.; Sofikitou, E.M.; Wang, K.; Dickerson, S.; Jaanimagi, U.; Markatou, M. High Satisfaction with Patient-Centered Telemedicine for Hepatitis C Virus Delivered to Substance Users: A Mixed-Methods Study. Telemed. J. E Health 2023, 29, 395–407. [Google Scholar] [CrossRef] [PubMed]
- Crotty, B.H.; Hyun, N.; Polovneff, A.; Dong, Y.; Decker, M.C.; Mortensen, N.; Holt, J.M.; Winn, A.N.; Laud, P.W.; Somai, M.M. Analysis of Clinician and Patient Factors and Completion of Telemedicine Appointments Using Video. JAMA Netw. Open 2021, 4, e2132917. [Google Scholar] [CrossRef]
- Price, J.C.; Simpson, D.C. Telemedicine and Health Disparities. Clin. Liver Dis. 2022, 19, 144–147. [Google Scholar] [CrossRef]
- Lyles, C.R.; Sharma, A.E.; Fields, J.D.; Getachew, Y.; Sarkar, U.; Zephyrin, L. Centering Health Equity in Telemedicine. Ann. Fam. Med. 2022, 20, 362–367. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Combating Hepatitis B and C to Reach Elimination by 2030: Advocacy Brief; No. WHO/HIV/2016.04; World Health Organization: Geneva, Switzerland, 2016.
- Morris, M.D.; McDonell, C.; Luetkemeyer, A.F.; Thawley, R.; McKinney, J.; Price, J.C. Community-Based Point-of-Diagnosis Hepatitis C Treatment for Marginalized Populations: A Nonrandomized Controlled Trial. JAMA Netw. Open 2023, 6, e2338792. [Google Scholar] [CrossRef] [PubMed]
- Herink, M.C.; Seaman, A.; Leichtling, G.; Larsen, J.E.; Gailey, T.; Cook, R.; Thomas, A.; Korthuis, P.T. A randomized controlled trial for a peer-facilitated telemedicine hepatitis c treatment intervention for people who use drugs in rural communities: Study protocol for the “peer tele-HCV” study. Addict. Sci. Clin. Pract. 2023, 18, 35. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, R.G.; McDonell, C.; McKinney, J.; Catalli, L.; Price, J.C.; Morris, M.D. Staff-Facilitated Telemedicine Care Delivery for Treatment of Hepatitis C Infection among People Who Inject Drugs. Healthcare 2024, 12, 715. https://doi.org/10.3390/healthcare12070715
Kim RG, McDonell C, McKinney J, Catalli L, Price JC, Morris MD. Staff-Facilitated Telemedicine Care Delivery for Treatment of Hepatitis C Infection among People Who Inject Drugs. Healthcare. 2024; 12(7):715. https://doi.org/10.3390/healthcare12070715
Chicago/Turabian StyleKim, Rebecca G., Claire McDonell, Jeff McKinney, Lisa Catalli, Jennifer C. Price, and Meghan D. Morris. 2024. "Staff-Facilitated Telemedicine Care Delivery for Treatment of Hepatitis C Infection among People Who Inject Drugs" Healthcare 12, no. 7: 715. https://doi.org/10.3390/healthcare12070715