
Age-Related Declines in Health and Fitness among Law Enforcement Officers Compared to Population Norms


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Body Composition Assessment
2.3. Cardiovascular Assessment
2.4. Muscular Fitness Assessment
2.5. Muscular Endurance Assessment
2.6. Power Generation Assessment
2.7. Grip Strength Assessment
2.8. Functional Movement Assessment
2.9. Flexibility Assessment
2.10. Statistical Analysis
3. Results
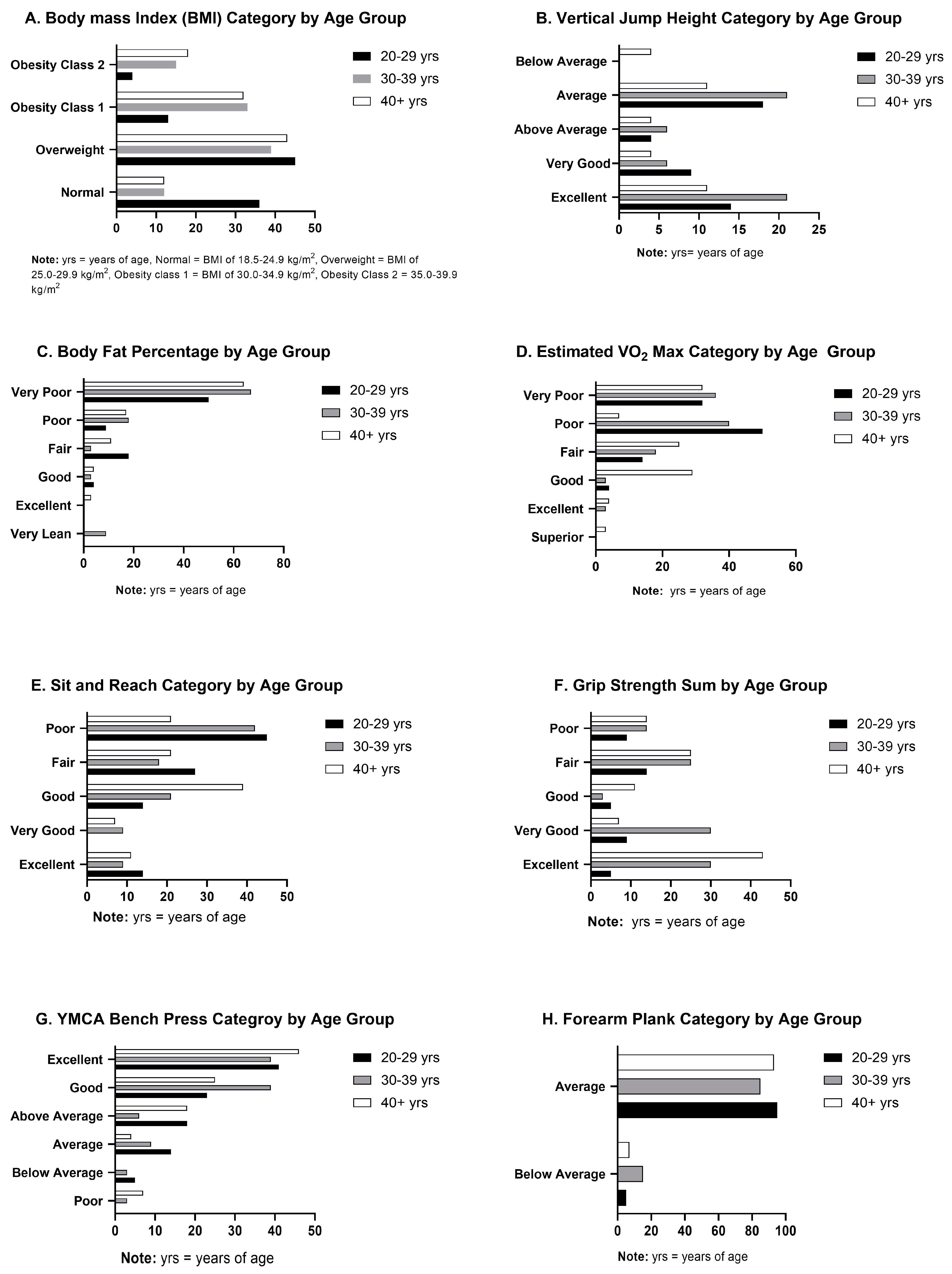
3.1. Body Composition
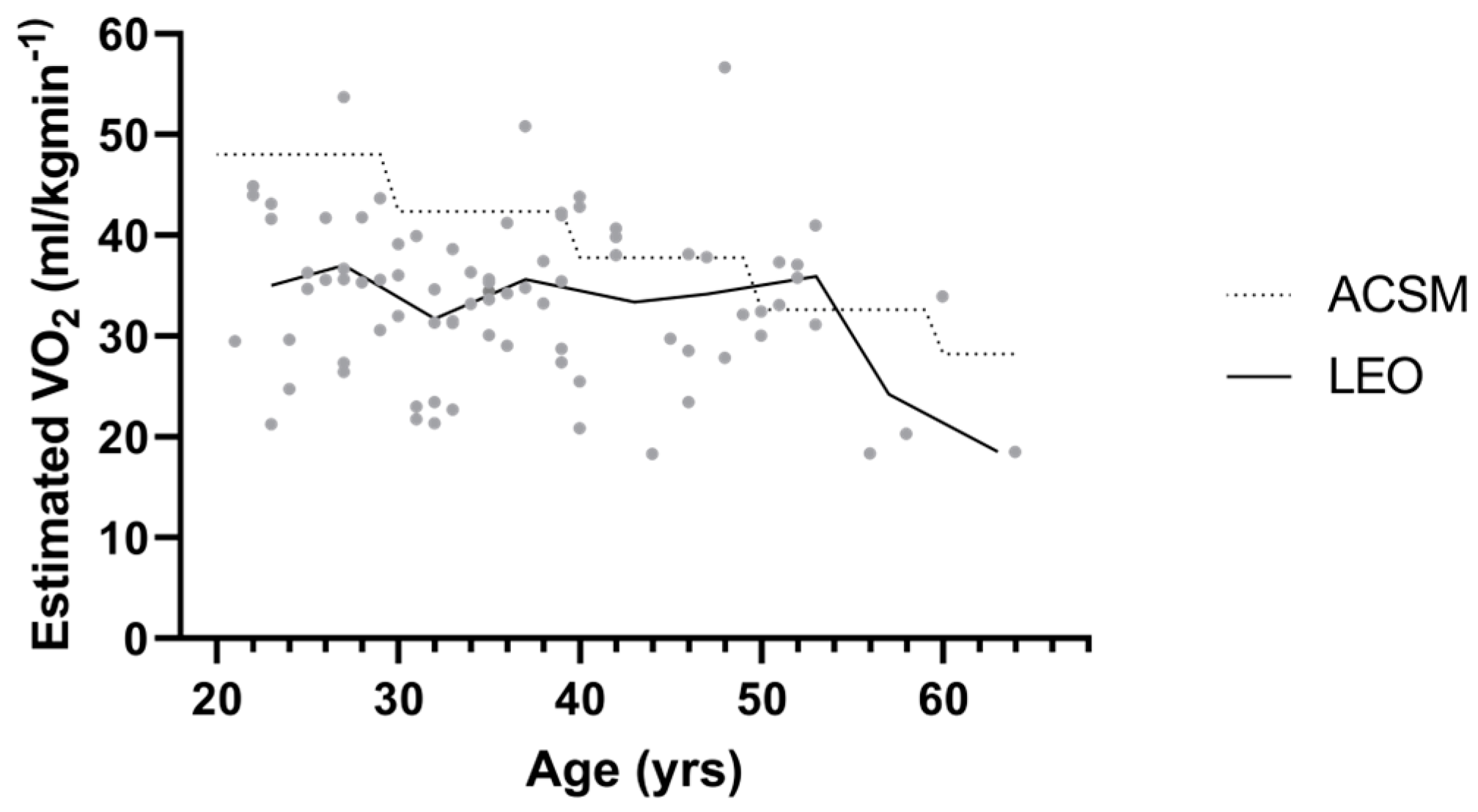
3.2. Cardiovascular
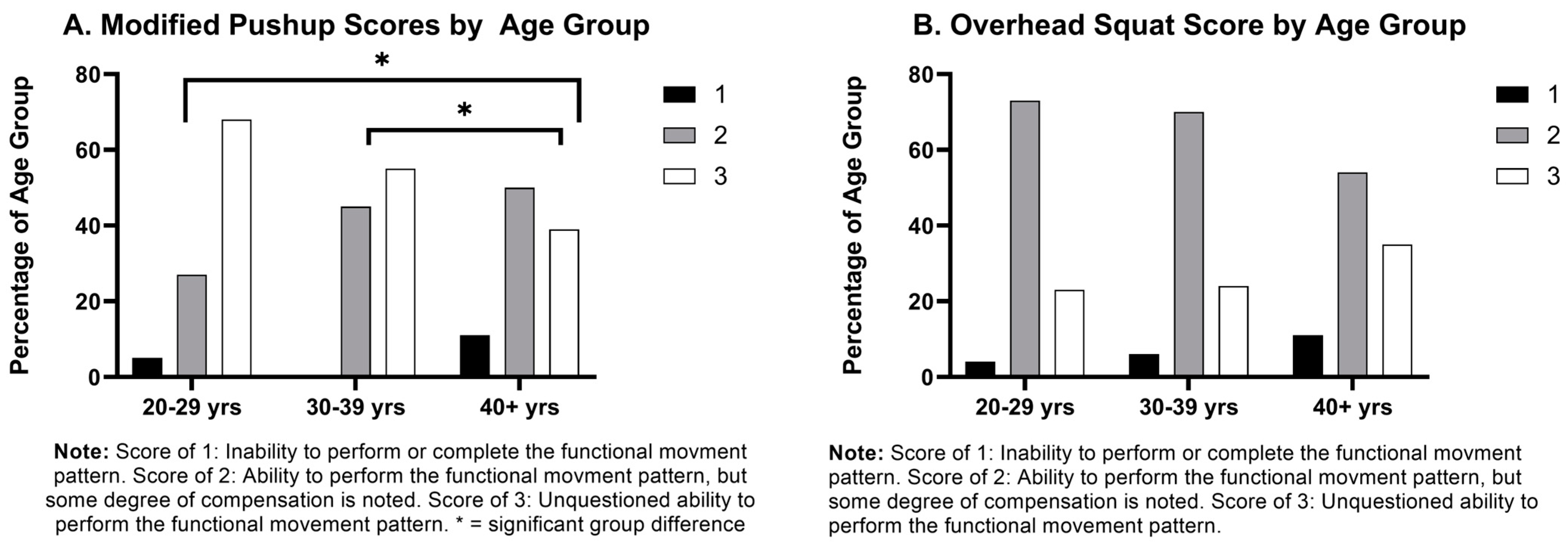
3.3. Muscular Strength and Endurance
4. Discussion
4.1. Cardiovascular
4.2. Body Composition
4.3. Muscular Strength and Endurance
4.4. Functional Movements and Flexibility
4.5. Vertical Jump
4.6. Grip Strength
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lockie, R.G.; Moreno, M.R.; Rodas, K.A.; Dulla, J.M.; Orr, R.M.; Dawes, J.J. With great power comes great ability: Extending research on fitness characteristics that influence work sample test battery performance in law enforcement recruits. Work 2021, 68, 1069–1080. [Google Scholar] [CrossRef]
- Strauss, M.; Foshag, P.; Jehn, U.; Vollenberg, R.; Brzęk, A.; Leischik, R. Exercise capacity, cardiovascular and metabolic risk of the sample of German police officers in a descriptive international comparison. Int. J. Med. Sci. 2021, 18, 2767–2775. [Google Scholar] [CrossRef]
- Anshel, M.H. A conceptual model and implications for coping with stressful events in police work. Crim. Justice Behav. 2000, 27, 375–400. [Google Scholar] [CrossRef]
- Saha, A.; Sahu, S.; Paul, G. Evaluation of cardio-vascular risk factor in police officers. Int. J. Pharma Bio Sci. 2010, 1, 263–271. [Google Scholar]
- Lockie, R.G.; Orr, R.M.; Dawes, J.J. Fit (and healthy) for duty: Blood lipid profiles and physical fitness test relationships from police officers in a health and wellness program. Int. J. Environ. Res. Public Health 2022, 19, 5408. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, F.H. Cardiovascular disease and risk factors in law enforcement personnel: A comprehensive review. Cardiol. Rev. 2012, 20, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Ramey, S.L.; Downing, N.R.; Knoblauch, A. Developing strategic interventions to reduce cardiovascular disease risk among law enforcement officers: The art and science of data triangulation. AAOHN J. 2008, 56, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Lentz, L.; Randall, J.R.; Guptill, C.A.; Gross, D.P.; Senthilselvan, A.; Voaklander, D. The association between fitness test scores and musculoskeletal injury in police officers. Int. J. Environ. Res. Public Health 2019, 16, 4667. [Google Scholar] [CrossRef] [PubMed]
- Tiesman, H.M.; Gwilliam, M.; Konda, S.; Rojek, J.; Marsh, S. Nonfatal injuries to law enforcement officers: A rise in assaults. Am. J. Prev. Med. 2018, 54, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Gray, S.E.; Collie, A. The nature and burden of occupational injury among first responder occupations: A retrospective cohort study in Australian workers. Injury 2017, 48, 2470–2477. [Google Scholar] [CrossRef] [PubMed]
- Crawley, A.A.; Sherman, R.A.; Crawley, W.R.; Cosio-Lima, L.M. Physical fitness of police academy cadets: Baseline characteristics and changes during a 16-week academy. J. Strength Cond. Res. 2016, 30, 1416. [Google Scholar] [CrossRef]
- Schilling, R.; Colledge, F.; Ludyga, S.; Pühse, U.; Brand, S.; Gerber, M. Does cardiorespiratory fitness moderate the association between occupational stress, cardiovascular risk, and mental health in police officers? Int. J. Environ. Res. Public Health 2019, 16, 2349. [Google Scholar] [CrossRef]
- Araujo, A.O.; Cancela, J.M.; Bezerra, P.; Chaves, C.; Rodrigues, L.P. Age-related influences on somatic and physical fitness of elite police agents (Influencias de la edad en la aptitud física y somática de los agentes de policía de élite). Retos 2020, 40, 281–288. [Google Scholar] [CrossRef]
- Boyce, R.W.; Jones, G.R.; Hiatt, A.R. Physical fitness capacity and absenteeism of police officers. J. Occup. Med. 1991, 33, 1137–1143. [Google Scholar] [CrossRef] [PubMed]
- Ramey, S.L.; Perkhounkova, Y.; Moon, M.; Tseng, H.C.; Wilson, A.; Hein, M.; Hood, K.; Franke, W. Physical activity in police beyond self-report. J. Occup. Environ. Med. 2014, 56, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Ramey, S.L.; Perkhounkova, Y.; Moon, M.; Budde, L.; Tseng, H.-C.; Clark, M.K. The effect of work shift and sleep duration on various aspects of police officers’ health. Workplace Health Saf. 2012, 60, 215–222. [Google Scholar]
- Ma, C.C.; Burchfiel, C.M.; Fekedulegn, D.; Andrew, M.E.; Charles, L.E.; Gu, J.K.; Mnatsakanova, A.; Violanti, J.M. Association of shift work with physical activity among police officers: The Buffalo cardio-metabolic occupational police stress study. J. Occup. Environ. Med. 2011, 53, 1030–1036. [Google Scholar] [CrossRef]
- Violanti, J.M.; Vena, J.E.; Petralia, S. Mortality of a police cohort: 1950–1990. Am. J. Ind. Med. 1998, 33, 366–373. [Google Scholar] [CrossRef]
- Zwingmann, L.; Zedler, M.; Kurzner, S.; Wahl, P.; Goldmann, J.P. How fit are special operations police officers? A comparison with elite athletes from Olympic disciplines. Front. Sports Act. Living 2021, 3, 347. [Google Scholar] [CrossRef] [PubMed]
- Leischik, R.; Foshag, P.; Strauß, M.; Littwitz, H.; Garg, P.; Dworrak, B.; Horlitz, M. Aerobic capacity, physical activity and metabolic risk factors in firefighters compared with police officers and sedentary clerks. PLoS ONE 2015, 10, e0133113. [Google Scholar]
- Riebe, D.E.J.; Liguori, G.; Magal, M. ACSM’s Guidelines for Exercise Testing and Prescription 2018; Wolters Kluwer: Philadelphia, PA, USA, 2018. [Google Scholar]
- Mifflin, M.D.; St Jeor, S.T.; Hill, L.A.; Scott, B.J.; Daugherty, S.A.; Koh, Y.O. A new predictive equation for resting energy expenditure in healthy individuals. Am. J. Clin. Nutr. 1990, 51, 241–247. [Google Scholar] [CrossRef]
- Heydari, P.; Varmazyar, S.; Variani, A.S.; Hashemi, F.; Ataei, S.S. Correlation of Gerkin, Queen’s College, George, and Jackson methods in estimating maximal oxygen consumption. Electron. Physician 2017, 9, 5525. [Google Scholar] [CrossRef]
- Pardeshi, T.; Grover, P.; Phadke, S.; Tilak, P. To Study the Co-relation between Muscular Endurance of Timed Forearm Plank Test with Body Mass Index (BMI) in Sedentary Urban Females of Age Group 25 to 55. Int. J. Sci. Res. 2020, 9, 860–865. [Google Scholar]
- Maulder, P.; Cronin, J. Horizontal and vertical jump assessment: Reliability, symmetry, discriminative and predictive ability. Phys. Ther. Sport 2005, 6, 74–82. [Google Scholar] [CrossRef]
- Cook, G.; Burton, L.; Torine, J. Movement: Functional Movement Systems: Screening, Assessment and Corrective Strategies; On Target Publications: Mumbai, India, 2010. [Google Scholar]
- Adams, M.A.; Conway, T.L. Eta Squared. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 1965–1966. [Google Scholar]
- Rhodes, E.C.; Farenholtz, D.W. Police Officer’s Physical Abilities Test compared to measures of physical fitness. Can. J. Sport Sci. 1992, 17, 228–233. [Google Scholar] [PubMed]
- Maupin, D.; Robinson, J.; Wills, T.; Irving, S.; Schram, B.; Orr, R. Profiling the metabolic fitness of a special operations police unit. J. Occup. Health 2018, 60, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.K.; Charles, L.E.; Burchfiel, C.M.; Fekedulegn, D.; Sarkisian, K.; Andrew, M.E.; Ma, C.; Violanti, J.M. Long work hours and adiposity among police officers in a US northeast city. J. Occup. Environ. Med. 2012, 54, 1374–1381. [Google Scholar] [CrossRef]
- Magnavita, N.; Capitanelli, I.; Garbarino, S.; Pira, E. Work-related stress as a cardiovascular risk factor in police officers: A systematic review of evidence. Int. Arch. Occup. Environ. Health 2018, 91, 377–389. [Google Scholar] [CrossRef]
- Roberts, C.K.; Freed, B.; McCarthy, W.J. Low aerobic fitness and obesity are associated with lower standardized test scores in children. J. Pediatr. 2010, 156, 711–718.e1. [Google Scholar] [CrossRef] [PubMed]
- Dawes, J.J.; Orr, R.M.; Flores, R.R.; Lockie, R.G.; Kornhauser, C.; Holmes, R. A physical fitness profile of state highway patrol officers by gender and age. Ann. Occup. Environ. Med. 2017, 29, 16. [Google Scholar] [CrossRef]
- Thayyil, J.; Jayakrishnan, T.T.; Raja, M.; Cherumanalil, J.M. Metabolic syndrome and other cardiovascular risk factors among police officers. N. Am. J. Med. Sci. 2012, 4, 630. [Google Scholar] [CrossRef]
- Violanti, J.M.; Ma, C.C.; Fekedulegn, D.; Andrew, M.E.; Gu, J.K.; Hartley, T.A.; Charles, L.E.; Burchfiel, C.M. Associations between body fat percentage and fitness among police officers: A statewide study. Saf. Health Work 2017, 8, 36–41. [Google Scholar] [CrossRef]
- F.B.I., Gender Distribution of Full-Time U.S. Law Enforcement Employees 2021, Statista. Available online: https://www.statista.com/statistics/195324/gender-distribution-of-full-time-law-enforcement-employees-in-the-us/ (accessed on 8 March 2024).
- Larsen, L.B.; Ramstrand, N.; Tranberg, R. Duty belt or load-bearing vest? Discomfort and pressure distribution for police driving standard fleet vehicles. Appl. Ergon. 2019, 80, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Houck, J.M.M.; Mermier, C.M.; Beltz, N.M.; Johnson, K.E.; VanDusseldorp, T.A.; Escobar, K.A.; Gibson, A.L. Physical fitness evaluation of career urban and wildland firefighters. J. Occup. Environ. Med. 2020, 62, e302–e307. [Google Scholar] [CrossRef] [PubMed]
- Chizewski, A.; Box, A.; Kesler, R.; Petruzzello, S.J. Fitness fights fires: Exploring the relationship between physical fitness and firefighter ability. Int. J. Environ. Res. Public Health 2021, 18, 11733. [Google Scholar] [CrossRef] [PubMed]
- Clark, M.; Lucett, S. NASM Essentials of Corrective Exercise Training; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010. [Google Scholar]
- Lockie, R.G.; Moreno, M.R.; Dawes, J.J. A Research Note on Relationships Between the Vertical Jump and Standing Broad Jump in Law Enforcement Recruits: Implications for Lower-Body Power Testing. J. Strength Cond. Res. 2022, 36, 2326–2329. [Google Scholar] [CrossRef] [PubMed]
- Dawes, J.J.; Lockie, R.G.; Kornhauser, C.L.; Holmes, R.J.; Orr, R.M. Relationships between absolute and relative strength and power in male police officers of varying strength levels. J. Sci. Sport Exerc. 2019, 1, 281–288. [Google Scholar] [CrossRef]
- Orr, R.M.; Pope, R.; Stierli, M.; Hinton, B. A functional movement screen profile of an Australian state police force: A retrospective cohort study. BMC Musculoskelet. Disord. 2016, 17, 296. [Google Scholar] [CrossRef] [PubMed]
- Celis-Morales, C.A.; Lyall, D.M.; Anderson, J.; Iliodromiti, S.; Fan, Y.; Ntuk, U.E.; Mackay, D.F.; Pell, J.P.; Sattar, N.; Gill, J.M. The association between physical activity and risk of mortality is modulated by grip strength and cardiorespiratory fitness: Evidence from 498 135 UK-Biobank participants. Eur. Heart J. 2017, 38, 116–122. [Google Scholar] [CrossRef]
- Gubelmann, C.; Vollenweider, P.; Marques-Vidal, P. Association of grip strength with cardiovascular risk markers. Eur. J. Prev. Cardiol. 2017, 24, 514–521. [Google Scholar] [CrossRef]
- Orr, R.; Pope, R.; Stierli, M.; Hinton, B. Grip strength and its relationship to police recruit task performance and injury risk: A retrospective cohort study. Int. J. Environ. Res. Public Health 2017, 14, 941. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Mean ± SD | Minimum | Maximum |
|---|---|---|---|
| Age (yrs) | 36.82 ± 10.00 | 21.00 | 64.00 |
| Height (cm) | 179.02 ± 7.70 | 162.50 | 203.20 |
| Weight (kg) | 95.10 ± 16.26 | 58.42 | 131.45 |
| Body Fat Percentage | 27.73 ± 7.09 | 8.80 | 40.50 |
| LEO 20–29 yrs n = 23 | ACSM 20–29 yrs | LEO 30–39 yrs n = 37 | ACSM 30–39 yrs | LEO ≥ 40 yrs n = 29 | ACSM ≥ 40 yrs | |
|---|---|---|---|---|---|---|
| Estimated VO2 Max (mL/kg/min) | * 36.12 ± 7.85 | 48.00 | * 33.42 ± 6.56 | 42.40 | * 32.65 ± 9.09 | 37.80 |
| YMCA Bench Press (# repetitions) | * 36.27 ± 8.81 | 22.00–26.00 | * 35.12 ± 9.06 | 22.00–26.00 | * 28 ± 11.69 | 12.00–18.00 |
| Forearm Plank (seconds) | 59.25 ± 3.54 | 60.00 | 58.09 ± 5.79 | 60.00 | 58.8 ± 4.48 | 60.00 |
| Grip Strength Sum (kg) | 99.15 ± 22.30 | 95.00–103.00 | 101.08 ± 19.80 | 95.00–103.00 | * 99.86 ± 23.32 | 86.00–92.00 |
| Vertical Jump (p.max/kg) | * 55.81 ± 12.22 | 45.72 | * 50.01 ± 10.09 | 45.72 | 44.19 ± 8.64 | 45.72 |
| Sit and Reach (cm) | * 26.45 ± 9.57 | 30.00–33.00 | * 24.94 ± 9.20 | 28.00–32.00 | * 22.77 ± 9.32 | 24.00–28.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frick, K.A.; Agostinelli, P.J.; Swinford, J.F.; Harris, M.E.; Mobley, C.B.; Sefton, J. Age-Related Declines in Health and Fitness among Law Enforcement Officers Compared to Population Norms. Healthcare 2024, 12, 714. https://doi.org/10.3390/healthcare12070714
Frick KA, Agostinelli PJ, Swinford JF, Harris ME, Mobley CB, Sefton J. Age-Related Declines in Health and Fitness among Law Enforcement Officers Compared to Population Norms. Healthcare. 2024; 12(7):714. https://doi.org/10.3390/healthcare12070714
Chicago/Turabian StyleFrick, Katherine A., Philip J. Agostinelli, Julia F. Swinford, Mick E. Harris, C. Brooks Mobley, and JoEllen Sefton. 2024. "Age-Related Declines in Health and Fitness among Law Enforcement Officers Compared to Population Norms" Healthcare 12, no. 7: 714. https://doi.org/10.3390/healthcare12070714