
Trans-Inclusive Communication and Self-Perceived Barriers to It, as Reported by Doctors—A Mixed-Methods Survey in Germany


Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment
2.2. Sample
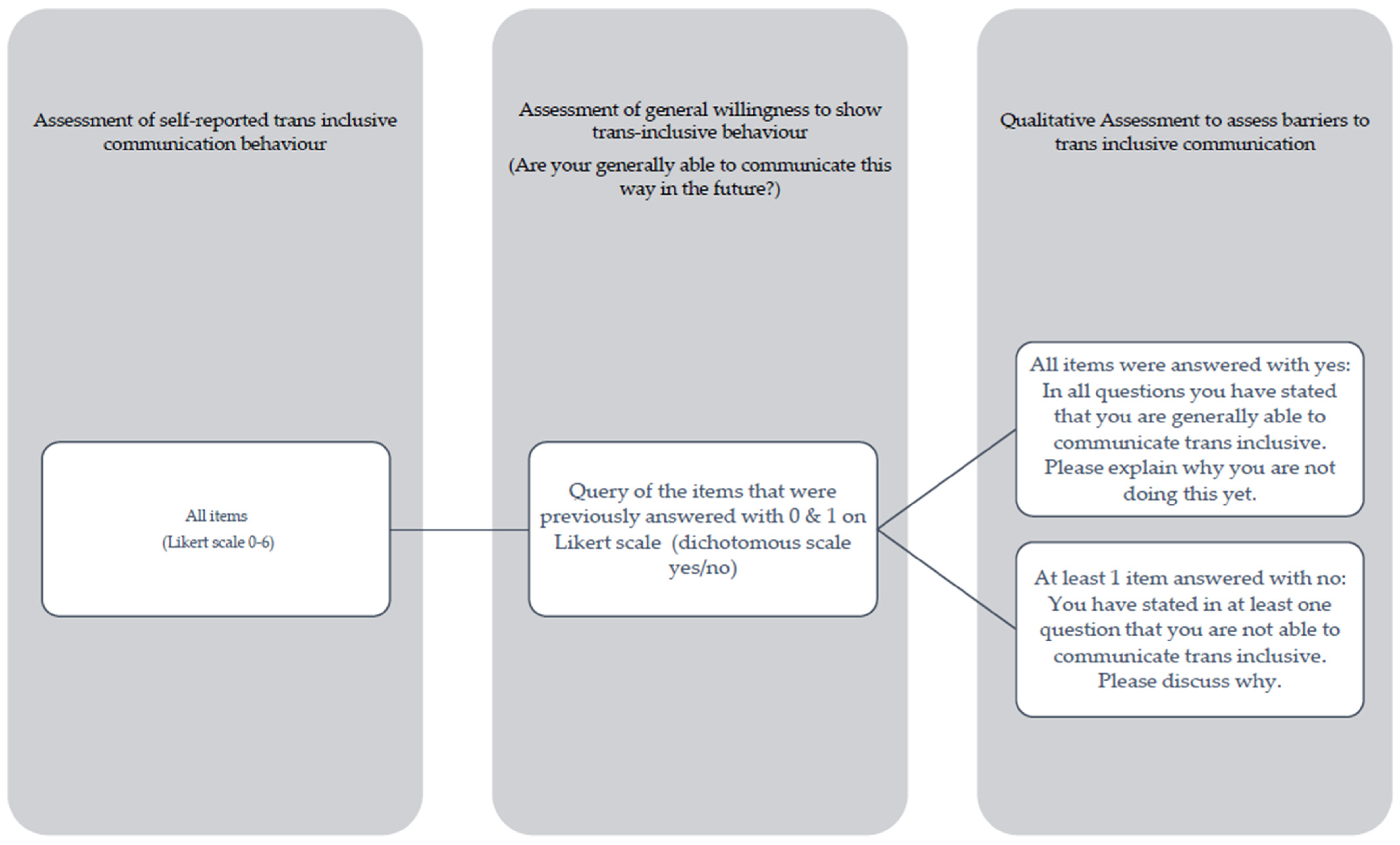
2.3. Instruments and Study Design
2.4. Analysis
3. Results
3.1. Self-Reported Trans-Inclusive Communication
3.2. Self-Reported Barriers to Trans-Inclusive Communication
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychological Association. Guidelines for psychological practice with transgender and gender nonconforming people. Am. Psychol. 2015, 70, 832–864. [Google Scholar] [CrossRef]
- Richards, C.; Bouman, W.P.; Seal, L.; Barker, M.J.; Nieder, T.O.; T’Sjoen, G. Non-binary or genderqueer genders. Int. Rev. Psychiatry 2016, 28, 95–102. [Google Scholar] [CrossRef]
- Koehler, A.; Eyssel, J.; Nieder, T.O. Genders and Individual Treatment Progress in (Non-)Binary Trans Individuals. J. Sex. Med. 2018, 15, 102–113. [Google Scholar] [CrossRef] [PubMed]
- Velasco, R.A.F.; Slusser, K.; Coats, H. Stigma and healthcare access among transgender and gender-diverse people: A qualitative meta-synthesis. J. Adv. Nurs. 2022, 78, 3083–3100. [Google Scholar] [CrossRef] [PubMed]
- Gieles, N.C.; Zinsmeister, M.; Pulles, S.; Harleman, A.; van Heesewijk, J.; Muntinga, M. ‘The medical world is very good at cis people, but trans is a specialisation’. Experiences of transgender and non-binary people with accessing primary sexual and reproductive healthcare services in The Netherlands. Glob. Public Health 2023, 18, 2246059. [Google Scholar] [CrossRef] [PubMed]
- Zimman, L. Pronouns and possibilities: Transgender language activism and reform. In Language and Social Justice in Practice; Avineri, N., Graham, L.R., Johnson, E.J., Riner, R.C., Rosa, J., Eds.; Routledge: New York, NY, USA, 2019; pp. 176–183. [Google Scholar]
- Haire, B.G.; Brook, E.; Stoddart, R.; Simpson, P. Trans and gender diverse people’s experiences of healthcare access in Australia: A qualitative study in people with complex needs. PLoS ONE 2021, 16, e0245889. [Google Scholar] [CrossRef] [PubMed]
- Wall, C.S.J.; Patev, A.J.; Benotsch, E.G. Trans broken arm syndrome: A mixed-methods exploration of gender-related medical misattribution and invasive questioning. Soc. Sci. Med. 2023, 320, 115748. [Google Scholar] [CrossRef]
- Johnson, N.; Pearlman, A.T.; Klein, D.A.; Riggs, D.; Schvey, N.A. Stigma and Barriers in Health Care Among a Sample of Transgender and Gender-Diverse Active Duty Service Members. Med. Care 2023, 61, 145–149. [Google Scholar] [CrossRef]
- Inman, E.M.; Obedin-Maliver, J.; Ragosta, S.; Hastings, J.; Berry, J.; Lunn, M.R.; Flentje, A.; Capriotti, M.R.; Lubensky, M.E.; Stoeffler, A.; et al. Reports of Negative Interactions with Healthcare Providers among Transgender, Nonbinary, and Gender-Expansive People assigned Female at Birth in the United States: Results from an Online, Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2023, 20, 6007. [Google Scholar] [CrossRef] [PubMed]
- Hollander, M.A.G.; Greene, M.G. A conceptual framework for understanding iatrophobia. Patient Educ. Couns. 2019, 102, 2091–2096. [Google Scholar] [CrossRef]
- Glick, J.L.; Theall, K.P.; Andrinopoulos, K.M.; Kendall, C. The Role of Discrimination in Care Postponement Among Trans-Feminine Individuals in the U.S. National Transgender Discrimination Survey. LGBT Health 2018, 5, 171–179. [Google Scholar] [CrossRef]
- Thomas, S.D.; King, R.; Murphy, M.; Dempsey, M. Demographic factors associated with healthcare avoidance and delay in the transgender population: Findings from a systematic review. Dialogues Health 2023, 3, 100159. [Google Scholar] [CrossRef]
- Price, M.A.; Hollinsaid, N.L.; McKetta, S.; Mellen, E.J.; Rakhilin, M. Structural transphobia is associated with psychological distress and suicidality in a large national sample of transgender adults. Soc. Psychiatry Psychiatr. Epidemiol. 2023, 59, 285–294. [Google Scholar] [CrossRef] [PubMed]
- de Vries, J.M.A.; Downes, C.; Sharek, D.; Doyle, L.; Murphy, R.; Begley, T.; McCann, E.; Sheerin, F.; Smyth, S.; Higgins, A. An exploration of mental distress in transgender people in Ireland with reference to minority stress and dissonance theory. Int. J. Transgender Health 2023, 24, 469–486. [Google Scholar] [CrossRef] [PubMed]
- Teti, M.; Kerr, S.; Bauerband, L.A.; Koegler, E.; Graves, R. A Qualitative Scoping Review of Transgender and Gender Non-conforming People’s Physical Healthcare Experiences and Needs. Front. Public Health 2021, 9, 598455. [Google Scholar] [CrossRef] [PubMed]
- Canvin, L.; Twist, J.; Solomons, W. How do mental health professionals describe their experiences of providing care for gender diverse adults? A systematic literature review. Psychol. Sex. 2022, 13, 717–741. [Google Scholar] [CrossRef]
- Kanamori, Y.; Cornelius-White, J.H.D.; Pegors, T.K.; Daniel, T.; Hulgus, J. Development and Validation of the Transgender Attitudes and Beliefs Scale. Arch. Sex. Behav. 2017, 46, 1503–1515. [Google Scholar] [CrossRef] [PubMed]
- Landau, N.; Hamiel, U.; Tokatly Latzer, I.; Mauda, E.; Levek, N.; Tripto-Shkolnik, L.; Pinhas-Hamiel, O. Paediatricians’ attitudes and beliefs towards transgender people: A cross-sectional survey in Israel. BMJ Open 2020, 10, e031569. [Google Scholar] [CrossRef] [PubMed]
- Nagoshi, J.L.; Adams, K.A.; Terrell, H.K.; Hill, E.D.; Brzuzy, S.; Nagoshi, C.T. Gender differences in correlates of homophobia and transphobia. Sex Roles J. Res. 2008, 59, 521–531. [Google Scholar] [CrossRef]
- Stroumsa, D.; Shires, D.A.; Richardson, C.R.; Jaffee, K.D.; Woodford, M.R. Transphobia rather than education predicts provider knowledge of transgender health care. Med. Educ. 2019, 53, 398–407. [Google Scholar] [CrossRef]
- Kosenko, K.; Rintamaki, L.; Raney, S.; Maness, K. Transgender patient perceptions of stigma in health care contexts. Med. Care 2013, 51, 819–822. [Google Scholar] [CrossRef]
- von der Warth, R.; Metzner, G.; Körner, M.; Farin-Glattacker, E. Exploring communication preferences of trans and gender diverse individuals—A qualitative study. PLoS ONE 2023, 18, e0284959. [Google Scholar] [CrossRef]
- Hansen, S.L.; Bammel, H.; Lübeck, N.; Seibel, R.; Schankweiler, P. Kommunikationspräfenzen im Kontext von Adipositas. Prävent. Gesundh. 2020, 15, 319–325. [Google Scholar] [CrossRef]
- Riedl, D.; Schüßler, G. The Influence of Doctor-Patient Communication on Health Outcomes: A Systematic Review. Z. Für Psychosom. Med. Psychother. 2017, 63, 131–150. [Google Scholar] [CrossRef] [PubMed]
- Jerofke-Owen, T.; Garnier-Villarreal, M.; Fial, A.; Tobiano, G. Systematic review of psychometric properties of instruments measuring patient preferences for engagement in health care. J. Adv. Nurs. 2020, 76, 1988–2004. [Google Scholar] [CrossRef]
- Platonova, E.A.; Qu, H.; Warren-Findlow, J. Patient-centered communication: Dissecting provider communication. Int. J. Health Care Qual. Assur. 2019, 32, 534–546. [Google Scholar] [CrossRef] [PubMed]
- Treharne, G.J.; Carroll, R.; Tan, K.K.H.; Veale, J.F. Supportive interactions with primary care doctors are associated with better mental health among transgender people: Results of a nationwide survey in Aotearoa/New Zealand. Fam. Pract. 2022, 39, 834–842. [Google Scholar] [CrossRef]
- Sastry, S.; Stephenson, M.; Dillon, P.; Carter, A. A Meta-Theoretical Systematic Review of the Culture-Centered Approach to Health Communication: Toward a Refined, “Nested” Model. Commun. Theory 2021, 31, 380–421. [Google Scholar] [CrossRef]
- Degrie, L.; Gastmans, C.; Mahieu, L.; Dierckx de Casterlé, B.; Denier, Y. How do ethnic minority patients experience the intercultural care encounter in hospitals? A systematic review of qualitative research. BMC Med. Ethics 2017, 18, 2. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- von der Warth, R.; Horstmeier, L.M.; Körner, M.; Farin-Glattacker, E. Health communication preferences of transgender and gender diverse individuals—Development and first psychometric evaluation of the CommTrans questionnaire. J. Homosex. 2024. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.L.; Chinna, K.; Lim Abdullah, K.; Zainal Abidin, I. The forward-backward and dual-panel translation methods are comparable in producing semantic equivalent versions of a heart quality of life questionnaire. Int. J. Nurs. Pract. 2019, 25, e12715. [Google Scholar] [CrossRef]
- Pollard, S.; Bansback, N.; Bryan, S. Physician attitudes toward shared decision making: A systematic review. Patient Educ. Couns. 2015, 98, 1046–1057. [Google Scholar] [CrossRef]
- Joseph-Williams, N.; Lloyd, A.; Edwards, A.; Stobbart, L.; Tomson, D.; Macphail, S.; Dodd, C.; Brain, K.; Elwyn, G.; Thomson, R. Implementing shared decision making in the NHS: Lessons from the MAGIC programme. BMJ 2017, 357, j1744. [Google Scholar] [CrossRef] [PubMed]
- Fleisje, A. Paternalistic persuasion: Are doctors paternalistic when persuading patients, and how does persuasion differ from convincing and recommending? Med. Health Care Philos. 2023, 26, 257–269. [Google Scholar] [CrossRef]
- Driever, E.M.; Stiggelbout, A.M.; Brand, P.L.P. Shared decision making: Physicians’ preferred role, usual role and their perception of its key components. Patient Educ. Couns. 2020, 103, 77–82. [Google Scholar] [CrossRef]
- Reisner, S.L.; Poteat, T.; Keatley, J.; Cabral, M.; Mothopeng, T.; Dunham, E.; Holland, C.E.; Max, R.; Baral, S.D. Global health burden and needs of transgender populations: A review. Lancet 2016, 388, 412–436. [Google Scholar] [CrossRef]
- Tebbe, E.A.; Budge, S.L. Factors that drive mental health disparities and promote well-being in transgender and nonbinary people. Nat. Rev. Psychol. 2022, 1, 694–707. [Google Scholar] [CrossRef]
- Chegini, Z.; Kakemam, E.; Behforoz, A.; Lotfollah-Zadeh, F.; Jafari-Koshki, T.; Khodayari Zarnag, R. Impact of Patient Communication Preferences on the Patient Trust in Physicians: A Cross-Sectional Study in Iranian Outpatient’s Clinics. J. Patient Exp. 2022, 9, 23743735211069809. [Google Scholar] [CrossRef]
- Shires, D.A.; Stroumsa, D.; Jaffee, K.D.; Woodford, M.R. Primary care providers’ willingness to continue gender-affirming hormone therapy for transgender patients. Fam. Pract. 2018, 35, 576–581. [Google Scholar] [CrossRef]
- Shires, D.A.; Stroumsa, D.; Jaffee, K.D.; Woodford, M.R. Primary Care Clinicians’ Willingness to Care for Transgender Patients. Ann. Fam. Med. 2018, 16, 555–558. [Google Scholar] [CrossRef] [PubMed]
- Giroldi, E.; Veldhuijzen, W.; Geelen, K.; Muris, J.; Bareman, F.; Bueving, H.; van der Weijden, T.; van der Vleuten, C. Developing skilled doctor-patient communication in the workplace: A qualitative study of the experiences of trainees and clinical supervisors. Adv. Health Sci. Educ. Theory Pract. 2017, 22, 1263–1278. [Google Scholar] [CrossRef] [PubMed]
- Ruprecht, K.; Dunlop, W.; Wah, E.; Phillips, C.; Martin, S. ‘A human face and voice’: Transgender patient-educator and medical student perspectives on gender-diversity teaching. BMC Med. Educ. 2023, 23, 621. [Google Scholar] [CrossRef] [PubMed]
- Puckett, J.A.; Hanson, C.; Dunn, T.; Kuehn, K.; DuBois, L.Z. An Examination of Predictors of Prejudice against Transgender Individuals. J. Homosex. 2024, 71, 645–665. [Google Scholar] [CrossRef] [PubMed]
- Verheijden, M.; Giroldi, E.; van den Eertwegh, V.; Luijkx, M.; van der Weijden, T.; de Bruin, A.; Timmerman, A. Identifying characteristics of a skilled communicator in the clinical encounter. Med. Educ. 2023, 57, 418–429. [Google Scholar] [CrossRef] [PubMed]
- Carrard, V.; Schmid Mast, M. Physician behavioral adaptability: A model to outstrip a “one size fits all” approach. Patient Educ. Couns. 2015, 98, 1243–1247. [Google Scholar] [CrossRef] [PubMed]
- Carrard, V.; Schmid Mast, M.; Jaunin-Stalder, N.; Junod Perron, N.; Sommer, J. Patient-Centeredness as Physician Behavioral Adaptability to Patient Preferences. Health Commun. 2018, 33, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Zimman, L. Transgender language reform: Some challenges and strategies for promoting trans-affirming, gender-inclusive language. J. Lang. Discrim. 2017, 1, 84–105. [Google Scholar] [CrossRef]
- Schafer, T.; Schnarrs, P.W.; Baldwin, A. Two Gender Medicine: Provider-Side Barriers to Caring for Transgender and Gender Diverse Patients. J. Homosex. 2024, 1–23. [Google Scholar] [CrossRef]
- Kanamori, Y.; Cornelius-White, J.H.D. Big changes, but are they big enough? Healthcare professionals’ attitudes toward transgender persons. Int. J. Transgend. 2016, 17, 165–175. [Google Scholar] [CrossRef]
- Cutillas-Fernández, M.A.; Jiménez-Barbero, J.A.; Herrera-Giménez, M.; Forcén-Muñoz, L.A.; Jiménez-Ruiz, I. Attitudes and Beliefs of Mental Health Professionals towards Trans People: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2023, 20, 6495. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sex (assigned at birth) | ||
| Female | 37 | 64.9 |
| Male | 20 | 35.1 |
| Completed residency | ||
| Yes | 29 | 51.8 |
| No | 27 | 48.2 |
| Medical speciality | ||
| General medicine | 14 | 26.9 |
| Anaesthesiology | 3 | 5.8 |
| Surgery | 10 | 19.2 |
| 1 | |
| 1 | |
| 1 | |
| 2 | |
| 3 | |
| 1 | |
| 1 | |
| Gynaecology and obstetrics | 1 | 1.9 |
| Otorhinolaryngology | 1 | 1.9 |
| Human genetics | 1 | 1.9 |
| Internal medicine | 10 | 19.2 |
| 1 | |
| 2 | |
| Orthodontics | 1 | 1.9 |
| Paediatrics | 3 | 5.8 |
| Neurology | 1 | 1.9 |
| Psychiatry and psychotherapy | 3 | 5.8 |
| Radiology | 2 | 3.9 |
| Urology | 1 | 1.9 |
| Dentistry | 1 | 1.9 |
| Clinical setting | ||
| Stationary | 26 | 45.6 |
| Partial stationary | 2 | 3.5 |
| Ambulant | 28 | 49.1 |
| Others | 1 | 1.8 |
| Known contact with transgender and gender-nonconforming people | ||
| Yes | 49 | 86.0 |
| No | 2 | 3.5 |
| I don’t know | 6 | 10.5 |
| Mean | Std. Deviation | |
| Age in years | 36.60 | 8.7 |
| Professional experience since license (in years) | 8.61 | 7.7 |
| Transphobia scale | 2.16 | 1.0 |
| I Already Communicate like This with My Patients. | Are You Generally Able to Communicate This Way in the Future? | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Disagree (0 and 1) | Agree (2–6) | Yes | No | ||||||
| N | % | N | % | N | % | N | % | ||
| General interaction communication | I am generally happy for my patients when their treatment progresses positively. * | / | / | 63 | 100 | ||||
| I always manage to encourage my patients when they are nervous. * | / | / | 64 | 100 | |||||
| I always manage to give my patients the feeling that I am aware of how important the treatment is for them. * | / | / | 62 | 100 | |||||
| I always manage to give my patients the feeling that the treatment is individually tailored to them. * | / | / | 63 | 100 | |||||
| I generally enable my patients to ask all their questions. | 3 | 4.7 | 61 | 95.3 | 1 | 33.7 | 2 | 66.7 | |
| I always manage to give my patients the feeling that I will take enough time for their treatment. | / | / | 62 | 100 | |||||
| I generally respond to what my patients say. | 1 | 1.6 | 63 | 98.4 | 1 | 100 | / | / | |
| I generally speak to my patients on an equal level. | 1 | 1.6 | 63 | 98.4 | 1 | 100 | / | / | |
| In all situations, I succeed in showing my patients that I take their concerns and wishes seriously. | / | / | 63 | 100 | |||||
| I always explain the side effects and risks of treatments in detail without sugar-coating or leaving anything out. | 2 | 3.2 | 61 | 96.8 | 1 | 0.5 | 1 | 0.5 | |
| I always show my patients that I take their treatment suggestions/requests seriously. | / | / | 62 | 100 | |||||
| I know my professional limits and communicate these to my patients whenever possible. | / | / | 62 | 100 | |||||
| As a general rule, I do not judge my patients and their life decisions. | / | / | 62 | 100 | |||||
| I always respond to my patients’ questions/treatment requests in a value-neutral manner and discuss them with an open mind. | 1 | 1.6 | 61 | 98.4 | / | / | 1 | 0.5 | |
| Gender-specific communication | I always ask my patients for their pronouns. * | 37 | 59.7 | 25 | 40.3 | 21 | 58.3 | 15 | 41.7 |
| On my/our website, you can already find an indication of the extent to which we use gendered language. * | 39 | 66.1 | 20 | 33.9 | 20 | 55.6 | 16 | 44.4 | |
| During the initial consultation, I always avoid gender-specific language, e.g., when I call patients to the examination room. * | 43 | 69.4 | 19 | 30.6 | 25 | 64.1 | 14 | 35.9 | |
| I always introduce myself with pronouns. * | 50 | 79.4 | 13 | 20.6 | 17 | 38.6 | 27 | 61.4 | |
| I regularly keep myself informed about current terminology and always talk about gender reassignment, for example. * | 20 | 31.7 | 43 | 68.3 | 8 | 44.4 | 10 | 55.6 | |
| I generally avoid phrases like “You can’t even tell”. | 9 | 14.8 | 52 | 85.2 | 5 | 62.5 | 3 | 37.5 | |
| I always give my patients the opportunity to indicate their gender individually at the start of treatment. | 18 | 29.0 | 44 | 71.0 | 11 | 64.7 | 6 | 35.3 | |
| I always manage to give my patients the feeling that they don’t have to explain their gender to me. | 8 | 13.1 | 53 | 86.9 | 3 | 37.5 | 5 | 62.5 | |
| Participants Who Said They Could Communicate Trans-Inclusively in the Future * | Participants Who Said They Could Not Communicate Trans-Inclusively in the Future * | |
|---|---|---|
| Category (Number of Answers in This Category) | Example | Example |
| Necessity (n = 18) | Due to our location in the countryside, we have only treated two transgender patients so far, and I haven’t dealt with the topic enough so far. | Due to the rarity of transsexuality, it currently seems pointless to me to ask someone for their pronouns or to introduce mine. If a person would like to be addressed differently than what their name/appearance suggests, I will be happy to respond to this if they point it out and implement this according to their wishes. |
| Sample dependency (n = 3) | Many patients, especially older patients, do not understand the question about pronouns or consider this question to be completely unnecessary. In some example cases, even an explanation has not led to understanding from patients, who see such a question as irritating or even an affront. | Communication with the patient is subject to social norms corresponding to age/educational background/social background, which I, as the treating doctor, try to adapt to in the conversation. The topic of ‘gender’ is, therefore, not always part of the content of the conversation/I think about it in everyday life. Furthermore, some phrases may be appropriate for one group of patients but not for another. The question, for example, can, therefore, only be answered with insufficient precision. |
| Habit (n = 5) | Not a habit yet; I often don’t have to use pronouns in conversation. | That would just be difficult for me at the moment. |
| Structural barriers in practice (n = 4) | In practice, I would be very out of line with my colleagues. My boss has a rather conservative attitude towards this. I don’t have the courage to go through with it anyway. | I don’t have the ability to change the website. |
| Uncertainties in dealing with the topic (n = 5) | Although I take the topic seriously and want everyone to feel comfortable with their gender/identification with me, it hasn’t occurred to me so far to do this by asking for pronouns and avoiding gender-specific ones in speech, etc. I don’t know exactly how I could implement this respectfully/tactfully/empathically either. | I wouldn’t know how else to call patients without it being strange. |
| Limits of patient-centredness (n = 2) | In principle, there are wishes and suggestions that go so far outside the scope of the usual or scientific that they must be clearly formulated. | If I know what the better treatment is, I’m happy to explain why. Unfortunately, it’s not possible to be open-ended without letting people die. |
| Gender as a binary concept (n = 3) | / | Patients usually tell us their gender when they give their name. I differentiate between men and women as possible biological genders. |
| Transphobia (n = 2) | / | It is impossible to change your gender. Even mutilation does not make a man a woman. I can’t support someone with mental illness. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
von der Warth, R.; Körner, M.; Farin-Glattacker, E. Trans-Inclusive Communication and Self-Perceived Barriers to It, as Reported by Doctors—A Mixed-Methods Survey in Germany. Healthcare 2024, 12, 707. https://doi.org/10.3390/healthcare12070707
von der Warth R, Körner M, Farin-Glattacker E. Trans-Inclusive Communication and Self-Perceived Barriers to It, as Reported by Doctors—A Mixed-Methods Survey in Germany. Healthcare. 2024; 12(7):707. https://doi.org/10.3390/healthcare12070707
Chicago/Turabian Stylevon der Warth, Rieka, Mirjam Körner, and Erik Farin-Glattacker. 2024. "Trans-Inclusive Communication and Self-Perceived Barriers to It, as Reported by Doctors—A Mixed-Methods Survey in Germany" Healthcare 12, no. 7: 707. https://doi.org/10.3390/healthcare12070707