
Implementing Activity-Based Therapy for Spinal Cord Injury Rehabilitation in Canada: Challenges and Proposed Solutions

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Article Identification
2.3. Data Extraction and Critical Appraisal
2.4. Qualitative Thematic Synthesis
3. Results
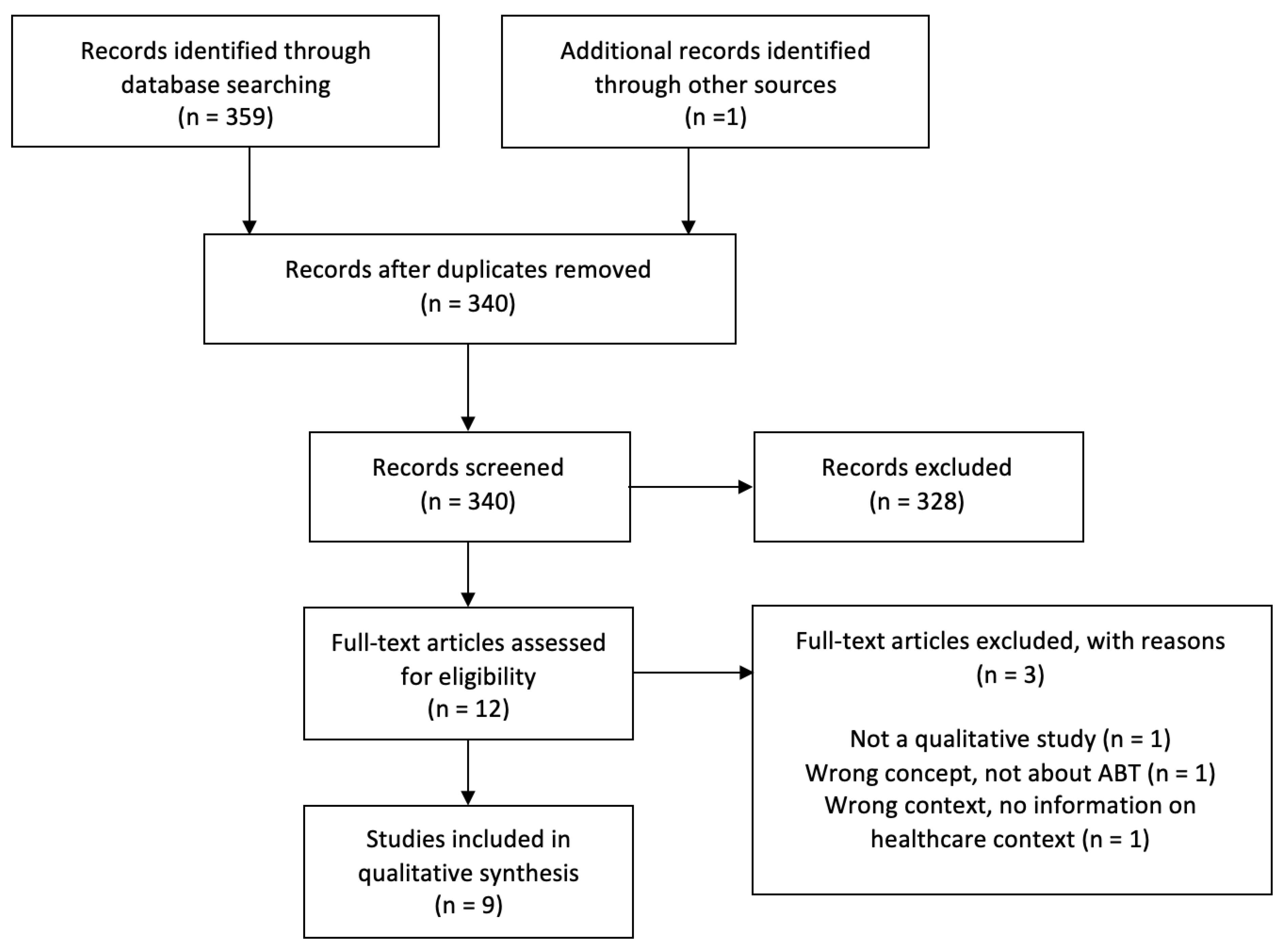
3.1. Included Studies
3.2. Context
3.3. Qualitative Thematic Synthesis
- Theme 1: Factors influencing acceptance and adaptation of ABT across healthcare settings in Canada.
3.3.1. Identity
“It’s also specifically with just a higher-level technology. The initial learning curve is varied. Like a lot of therapists will approach it and say, “If this isn’t better or faster than what I’m currently doing, why should I bother with it?” It’s hard for them to get comfortable enough to make it faster than the standard therapy because they’re not using it”.[15]
3.3.2. Knowledge
“From a respiratory point of view, they crash, then that’s when they’ll go down to the ICU and then they’ll come back up again and when patients have a big crash like that then you’re resetting the clock every time because they’ve got to start again when they come back up to us”.
3.3.3. Health System
- Theme 2: Proposed solutions.
3.3.4. Motivation, Empowerment, and Advocacy for ABT
“It’s really hard to motivate yourself when you’re by yourself living alone, and someone says, well, did you do your sit to stands today? Well no, you know? Because you’re just not motivated. And in a group like that, and yes we knew everybody by the time we ended, we could laugh and have a good time with it”.[25]
3.3.5. Desire for Education and Training
3.4. Behavioural Change Wheel and COM-B Model
4. Discussion
4.1. The Behaviour Change Wheel, Intervention Functions, and Behaviour Change Techniques
4.2. Alignment of the Canadian ABT Community of Practice with Environmental Restructuring and Enablement Interventions to Target Social Opportunity
4.3. Alignment of Equipment and facilities with Training, Environmental Restructuring, Enablement, and Restriction to Target Physical Opportunity
4.4. Alignment of Elective and Continuing Education Programs and Materials with Training, Education, Enablement, and Persuasion Interventions to Target Reflective Motivation
4.5. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. MEDLINE Search Strategy: PubMed Version
- <1946 to 15 December 2023>
- spinal cord injur*/
- spinal cord injuries*/
- spinal cord diseas*/
- spinal cord injury/disease
- paraplegi*/
- quadraplegi*/
- tetraplegi*/
- Or/1–7
- “activity-based therapy”
- “activity based therapy”
- ABT
- “exercise therapy”
- “locomotor therapy”
- Or/9–13
- qualitative/
- perspectives/
- Or/15–16
- 8 and 14 and 17
References
- World Health Organization. Spinal Cord Injury 2013. Available online: https://www.who.int/news-room/fact-sheets/detail/spinal-cord-injury (accessed on 10 January 2024).
- Dromerick, A.W.; Lum, P.S.; Hidler, J. Activity-based therapies. NeuroRx 2006, 3, 428–438. [Google Scholar] [CrossRef] [PubMed]
- Musselman, K.E.; Shah, M.; Zariffa, J. Rehabilitation technologies and interventions for individuals with spinal cord injury: Translational potential of current trends. J. Neuroeng. Rehabil. 2018, 15, 40. [Google Scholar] [CrossRef]
- Behrman, A.L.; Ardolino, E.M.; Harkema, S.J. Activity-Based Therapy: From Basic Science to Clinical Application for Recovery After Spinal Cord Injury. J. Neurol. Phys. Ther. 2017, 41 (Suppl. S3), S39–S45. [Google Scholar] [CrossRef]
- Karamian, B.A.; Siegel, N.; Nourie, B.; Serruya, M.D.; Heary, R.F.; Harrop, J.S.; Vaccaro, A.R. The role of electrical stimulation for rehabilitation and regeneration after spinal cord injury. J. Orthop. Traumatol. 2022, 23, 2. [Google Scholar] [CrossRef] [PubMed]
- Marquez-Chin, C.; Popovic, M.R. Functional electrical stimulation therapy for restoration of motor function after spinal cord injury and stroke: A review. Biomed. Eng. Online 2020, 19, 34. [Google Scholar] [CrossRef] [PubMed]
- Zewdie, E.T.; Roy, F.D.; Yang, J.F.; Gorassini, M.A. Facilitation of descending excitatory and spinal inhibitory networks from training of endurance and precision walking in participants with incomplete spinal cord injury. Prog. Brain Res. 2015, 218, 127–155. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, C.; Walden, K.; Jervis-Rademeyer, H.; Musselman, K.E.; Kaiser, A.; Wolfe, D.L.; Noonan, V.K.; Donkers, S.J. Technology used in activity based therapy for individuals living with spinal cord injury across Canada. Spinal Cord. Ser. Cases 2023, 9, 1. [Google Scholar] [CrossRef] [PubMed]
- Cheung, L.; Musselman, K.E.; Kaiser, A.; Jervis Rademeyer, H.; Walden, K.; Marshall, S.; Gauthier, C. Activity-based therapy in the community for individuals living with spinal cord injury or disease: Qualitative interviews with clinicians. Disabil. Rehabil. 2022, 44, 4821–4830. [Google Scholar] [CrossRef] [PubMed]
- Swaffield, E.; Cheung, L.; Khalili, A.; Lund, E.; Boileau, M.; Chechlacz, D.; Musselman, K.E.; Gauthier, C. Perspectives of people living with a spinal cord injury on activity-based therapy. Disabil. Rehabil. 2022, 44, 3632–3640. [Google Scholar] [CrossRef]
- Kaiser, A.; Chan, K.; Sessford, J.; McCullum, S.; Athanasopoulos, P.; Rice, C.; Leo, J.; MacRitchie, I.; Zariffa, J.; Musselman, K.E. Providing Insights into the Challenges of Implementing Activity-Based Therapy in Canada: A Comparative Analysis Using Focus Group Interviews with Key Interest Groups. Top. Spinal Cord. Inj. Rehabil. 2023, 29, 53–74. [Google Scholar] [CrossRef] [PubMed]
- Musselman, K.E.; Walden, K.; Noonan, V.K.; Jervis-Rademeyer, H.; Thorogood, N.; Bouyer, L.; Chan, B.; Donkers, S.; Ho, C.; Jeji, T.; et al. Development of priorities for a Canadian strategy to advance activity-based therapies after spinal cord injury. Spinal Cord. 2021, 59, 874–884. [Google Scholar] [CrossRef] [PubMed]
- Canadian Activity-Based Therapy Community of Practice Vancouver, BC, Canada: Praxis Spinal Cord Institute. 2024. Available online: https://praxisinstitute.org/research-care/key-initiatives/activity-based-therapy/abt-cop/ (accessed on 15 January 2024).
- Jervis Rademeyer, H.; Gastle, N.; Walden, K.; Lemay, J.-F.; Ho, C.; Marquez-Chin, C.; Musselman, K.E. Activity-based therapy for individuals with spinal cord injury/disease: Perspectives of acute care therapists. Spinal Cord. Ser. Cases 2022, 8, 39. [Google Scholar] [CrossRef] [PubMed]
- Jervis Rademeyer, H.; Gauthier, C.; Zariffa, J.; Walden, K.; Jeji, T.; McCullum, S.; Musselman, K.E. Using activity-based therapy for individuals with spinal cord injury or disease: Interviews with physical and occupational therapists in rehabilitation hospitals. J. Spinal Cord. Med. 2023, 46, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8, 45. [Google Scholar] [CrossRef]
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S.; Craig, J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med. Res. Methodol. 2012, 12, 181. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, A.; Chan, K.; Pakosh, M.; McCullum, S.; Rice, C.; Zariffa, J.; Musselman, K.E. A Scoping Review of the Characteristics of Activity-based Therapy Interventions Across the Continuum of Care for People Living With Spinal Cord Injury or Disease. Arch. Rehabil. Res. Clin. Transl. 2022, 4, 100218. [Google Scholar] [CrossRef] [PubMed]
- Behrman, A.L.; Harkema, S.J. Physical rehabilitation as an agent for recovery after spinal cord injury. Phys. Med. Rehabil. Clin. N. Am. 2007, 18, 183–202. [Google Scholar] [CrossRef]
- Hong, Q.N.; Pluye, P.; Fàbreques, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool (MMAT); McGill University: Montreal, QC, Canada, 2018. [Google Scholar]
- Cheung, L.; McKay, B.; Chan, K.; Heffernan, M.G.; Pakosh, M.; Musselman, K.E. Exploring sport participation in individuals with spinal cord injury: A qualitative thematic synthesis. J. Spinal Cord. Med. 2023, 46, 658–676. [Google Scholar] [CrossRef]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Cesca, N.; Lin, C.; Abu-Jurji, Z.; Wexler, A.; Mark, J.; McCullum, S.; Kamran, R.; Chan, B.; Musselman, K.E. Exploring knowledge and implementation gaps of activity-based therapy in centers lacking specialized spinal cord injury services: Understanding therapists’ perspectives. Spinal Cord. Ser. Cases 2024, 10, 14. [Google Scholar] [CrossRef]
- Coomaran, V.; Khan, A.; Tyson, E.; Bardutz, H.; Hopper, T.D.; Mang, C.S. Evaluating and Characterizing an Individually-Tailored Community Exercise Program for Older Adults with Chronic Neurological Conditions: A Mixed-Methods Study. J. Aging Phys. Act. 2022, 30, 1047–1060. [Google Scholar] [CrossRef] [PubMed]
- Singh, H.; Shah, M.; Flett, H.M.; Craven, B.C.; Verrier, M.C.; Musselman, K.E. Perspectives of individuals with sub-acute spinal cord injury after personalized adapted locomotor training. Disabil. Rehabil. 2018, 40, 820–828. [Google Scholar] [CrossRef]
- Singh, H.; Sam, J.; Verrier, M.C.; Flett, H.M.; Craven, B.C.; Musselman, K.E. Life after personalized adaptive locomotor training: A qualitative follow-up study. Spinal Cord. Ser. Cases 2018, 4, 6. [Google Scholar] [CrossRef] [PubMed]
- Ortenblad, L.; Maribo, T.; Quistgaard, B.; Madsen, E.; Handberg, C. The ambiguity of goal-setting: A study of patients’ perspectives on goal-setting in outpatient multidisciplinary rehabilitation of patients with spinal cord injury. Disabil. Rehabil. 2023, 45, 3342–3351. [Google Scholar] [CrossRef] [PubMed]
- Ortenblad, L.; Maribo, T.; Quistgaard, B.; Madsen, E.; Handberg, C. Goal-Setting in clinical practice: A study of health-care professionals’ perspectives in outpatient multidisciplinary rehabilitation of patients with spinal cord injury. Disabil. Rehabil. 2023, 45, 3330–3341. [Google Scholar] [CrossRef] [PubMed]
- Maribo, T.; Jensen, C.M.; Madsen, L.S.; Handberg, C. Experiences with and perspectives on goal setting in spinal cord injury rehabilitation: A systematic review of qualitative studies. Spinal Cord. 2020, 58, 949–958. [Google Scholar] [CrossRef] [PubMed]
- Schofield, P.; Shaw, T.; Pascoe, M. Toward Comprehensive Patient-Centric Care by Integrating Digital Health Technology with Direct Clinical Contact in Australia. J. Med. Internet Res. 2019, 21, e12382. [Google Scholar] [CrossRef] [PubMed]
- Renaud, R.; Locke, H.N.; Hariharan, R.; Chamberlain, M.A.; O’Connor, R.J. Developing a Spinal Cord Injury Rehabilitation Service in Madagascar. J. Rehabil. Med. 2018, 50, 402–405. [Google Scholar] [CrossRef]
- Jesus, T.S.; Silva, I.L. Toward an evidence-based patient-provider communication in rehabilitation: Linking communication elements to better rehabilitation outcomes. Clin. Rehabil. 2016, 30, 315–328. [Google Scholar] [CrossRef]
- First Steps Wellness Centre, Regina, SK: First Steps Wellness Centre. 2023. Available online: https://firststepswellnesscentre.ca (accessed on 20 January 2024).
- Taking Care of the Community with Your Help Since 2012: Walk It off Spinal Cord Recovery and Wellness Centre. 2023. Available online: https://walkitoffrecovery.org (accessed on 20 January 2024).
- ReYu. Reconnect. Retrain. Redefine: ReYu Paralysis Recovery Centre. 2023. Available online: https://www.reyu.ca (accessed on 21 January 2024).
- Snoswell, C.L.; Taylor, M.L.; Comans, T.A.; Smith, A.C.; Gray, L.C.; Caffery, L.J. Determining if Telehealth Can Reduce Health System Costs: Scoping Review. J. Med. Internet Res. 2020, 22, e17298. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.; Lai, B.; Rimmer, J.; Powell, D.; Yarar-Fisher, C.; Oster, R.A.; Fisher, G. Telehealth high-intensity interval exercise and cardiometabolic health in spinal cord injury. Trials 2022, 23, 633. [Google Scholar] [CrossRef] [PubMed]
- FES Courses: International Functional Electrical Stimulation Society, Inc. 2024. Available online: https://ifess.org/fes-courses-2/ (accessed on 21 January 2024).
- Robertson, M.K.; Umble, K.E.; Cervero, R.M. Impact studies in continuing education for health professions: Update. J. Contin. Educ. Health Prof. 2003, 23, 146–156. [Google Scholar] [CrossRef]
- Travlos, D.V.; Baumgartner, J.L.; Rouse, M.; Wadelin, J.W.; Vlasses, P.H. Forty Years of ACPE CPE Accreditation. Am. J. Pharm. Educ. 2017, 81, 5998. [Google Scholar] [CrossRef]
- Leist, J.C. Accreditation: Standards for quality continuing professional development. J. Vet. Med. Educ. 2003, 30, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Canada Go. Introduction to Policy: Canadian Heritage Information Network. 2021. Available online: https://www.canada.ca/en/heritage-information-network/services/digital-preservation/concepts-developing-policies/introduction-policy.html (accessed on 12 October 2021).


{kind=link}
| Author(s) | Year | Methodology (Analysis Strategy) | Objective(s) | Inclusion Criteria | Healthcare Setting | Characteristics of Population | Sex/Gender | Number of Interviews or Focus Groups | Major Findings (e.g., Themes, Categories) | Key Takeaways |
|---|---|---|---|---|---|---|---|---|---|---|
| Cesca et al. [24] | 2024 | Qualitative exploratory (interpretive description) | To explore the knowledge, perspectives, and implementation of ABT among physical and occupational therapists in non-SCI-specialized centers. | Physical or occupational therapists working in a non-SCI-specialized center in Canada who have treated at least one person with SCI in the last 18 months. | Non-SCI-specialized centers (acute care, inpatient rehabilitation, long-term care, outpatient rehabilitation, rural outpatient clinic) across Canada (i.e., facilities lacking SCI-specific services). | 7 participants; PTs (n = 4) and OTs (n = 3); Ontario (n = 4) and Alberta (n = 3); experience ranging from 3 to 22 years in current healthcare setting. | Not reported. | 6 semi-structured interviews. All individual interviews, except one, completed with a PT and OT from the same facility. | Three themes: (1) available knowledge, resources, and therapy time in non-SCI-specialized centers challenge ABT implementation, (2) how current therapy practices in non-SCI-specialized centers align with ABT, and (3) desire for ABT knowledge. | The study emphasized the need for tailored ABT education in non-SCI-specialized centres. |
| Cheung et al. [9] | 2022 | Exploratory qualitative (interpretive description) | To understand how ABT was provided to Canadians with SCI/D in the community. To explore the use, perceived barriers, and facilitators of ABT and its associated technologies by therapists (e.g., PTs and OTs) and other clinicians. | Physical and occupational therapists, clinic employees, clinic managers, and clinic owners who work in a Canadian community-based center that offers ABT to individuals living with SCI. | Community-based ABT facilities across Canada. | 13 participants; kinesiologists (n = 6), PTs (n = 4), OTs (n = 1), and clinic directors (n = 2). One PT was also a Clinician Scientist. Ontario (n = 5), Alberta (n = 3), Quebec (n = 1), and Saskatchewan (n = 1). | Male (n = 3) and female (n = 10). | 10 interviews. Each interview consisted of one to two participants from a single site. | Overarching theme: ABT in the community is a client-centered approach characterized by various techniques, clinicians, and clientele. Three main categories within this theme: (1) characteristics of ABT in the community, (2) perceived challenges, and (3) need for advocacy. | The study revealed varied applications of ABT and related technologies across Canadian community-based facilities, unified by a focus on client goals and well-being. Systemic challenges hinder ABT’s implementation and accessibility in Canada. Solutions proposed include earlier ABT introduction, enhanced education, and cost reduction. |
| Coomaran et al. [25] | 2022 | Mixed methods, qualitative descriptive (conventional content analysis) | To characterize the overall experience of those involved in the community exercise program toward identification of key program elements. | Adults (i.e., ≥18 years of age) who (1) self-reported experience of chronic motor impairment related to a stable, neurological condition and (2) provided documentation of physician clearance for exercise. | Community exercise program delivered at the University of Regina Centre for Health, Wellness and Performance between September 2019 and March 2020. | 11 individuals living with a neurological condition who participated in the community exercise program. Neurological conditions included incomplete SCI (n = 1), Parkinson’s disease (n = 1), mild TBI (n = 2), TBI (n = 1), ABI (n = 1), stroke (n = 3), and MS (n = 2). Time in program ranged from 4 weeks to 20 weeks. | Male (n = 4) and female (n = 7). | 11 interviews with program participants. Interviews were conducted post-program activities in one-on-one format except in two cases where a spouse or caregiver supported the conversation. A sample of the program volunteers was also interviewed. | Four key program elements: 1. Support through supervision; 2. Social connection; 3. Individualized programming; 4. Experiential learning. | The program was feasible and effective in addressing the needs of older adults with varied levels and types of chronic neurological conditions. Key elements for success included personalized exercise prescriptions, social connections, and a supportive environment with knowledgeable supervision. |
| Jervis Rademeyer et al. [14] | 2022 | Exploratory, qualitative descriptive (interpretive description) | To determine if and how occupational and physical therapists in acute care hospital settings use ABT and its associated technologies. | Physical and occupational therapists licensed to practice in Canada and working in an acute care hospital setting with patients with SCI. | Acute care hospital settings in Canada. | 7 participants from 6 sites spanning 4 Canadian provinces: PTs (n = 5) and OTs (n = 2). | Male (n = 1) and female (n = 6). | 6 interviews. One interview with two participants from the same facility. | Three themes: (1) impact of patient acuity on ABT participation, (2) ABT approach unique to the acute care setting, and (3) influence of acute care work environment and therapy practice. | The study indicated that implementing ABT in acute care settings is difficult due to the high dosage of movement practice it demands. Enhancing ABT usage and dosage in these settings could be achieved through early patient education, leveraging social support, and integrating existing portable technology in acute care. |
| Jervis Rademeyer et al. [15] | 2023 | Qualitative (interpretive description) | To understand if and how physical and occupational therapists use ABT and its associated technologies for the rehabilitation of individuals living with SCI in inpatient and outpatient hospital settings in Canada. | Physical and occupational therapists licensed to practice in Canada and working at a rehabilitation hospital part of the Rick Hansen Spinal Cord Registry (RHSCIR). | Canadian rehabilitation hospitals participating in the RHSCIR. | 22 participants from 9 rehabilitation sites across 8 Canadian provinces: PTs (n = 12) and OTs (n = 10). | Not reported. | 10 focus groups, consisting of two or more participants. | Three overarching themes: (1) therapists’ decision-making approach to ABT and technology, (2) therapist perceived individual factors, and (3) access to ABT and equipment. | The application of technology in ABT varied, influenced by both tangible (e.g., equipment cost) and intangible barriers (e.g., departmental relations). ABT usage in Canadian rehabilitation hospitals is inconsistent. To enhance ABT utilization, ongoing education and development of tailored implementation strategies are recommended. |
| Kaiser et al. [8] | 2023 | Qualitative descriptive (conventional content analysis) | To understand and compare the perspectives of key interest groups on the challenges of implementing ABT in Canada for people living with SCI. | Canadian, English speaking, and either participated in, supervised, or had knowledge of ABT and SCI. A screening questionnaire was also used to query the nature and duration of experience with ABT to determine eligibility. | Canadian healthcare system. | 48 participants representing 6 key interest groups: people with SCI (n = 10), hospital PTs and OTs (n = 6), community exercise trainers (n = 12), hospital and community administrators (n = 8), researchers (n = 7), and advocates, funders, and policy experts (n = 5). Experience/knowledge in ABT and SCI ranged from 0.25 to 33 years. | Male (n = 20) and female (n = 28). (M/F): people with SCI (7/3), hospital PTs and OTs (1/5), community exercise trainers (4/8), hospital and community administrators (1/7), researchers (4/3), and advocates, funders, and policy experts (3/2). | 10 focus groups consisting of 2–6 participants. 2 one-on-one interviews. | Six themes: (1) challenge of gaps in knowledge and training, (2) challenge of standardizing ABT, (3) challenge of determining the optimal timing of ABT, (4) challenge of defining, characterizing, and achieving high dosage and intensity, (5) challenge of funding ABT, and (6) challenge of measuring participation and performance in ABT. | The study identified several challenges in implementing ABT in Canada, including gaps in knowledge and training, difficulties in defining and achieving appropriate dosage and intensity, funding challenges, and challenges in measuring participation and performance. These challenges varied among different interest groups, highlighting the need for tailored approaches to address these issues. |
| Singh et al. [26] | 2018 | Qualitative descriptive (conventional content analysis) | To understand how participation in Personalized Adaptive Locomotor Training (PALT) impacted participants’ lives, what aspects of PALT they perceived to work well, and what challenges they encountered while in the PALT program. To create recommendations, based on the identified challenges, to guide improvements to the design and implementation of PALT within Canadian tertiary SCI rehabilitation settings. | Traumatic, or non-progressive, non-traumatic, motor iSCI (AIS C or D), sub-acute stage of SCI (i.e., <one year post-injury), no deteriorating medical condition, capacity for generating lower extremity reciprocal alternating flexion/extension stepping pat- terns, compliance to reduce or eliminate the use of lower extremity orthotics, reside within 100 km of the training center, and access to reliable transportation. | Lyndhurst Center—TRI, part of the University Health Network in Canada (i.e., outpatient rehabilitation setting in Canada). | Traumatic SCI (n = 4), non-traumatic SCI (n = 3), AIS C (n = 1), and AIS D (n = 6). Neurological levels of injury ranged from C2 to T8. | Male (n = 5) and female (n = 2). | 7 individual interviews conducted during the last week of the participant’s PALT. | Three main themes: (1) motives for participating, (2) perceived benefits, and (3) perceived challenges. | Participants reported significant physical and functional improvements from PALT but faced challenges in transferring skills learned in a controlled setting to daily walking. Specific challenges included neglect of other commitments, acquiring services for participation, re-integrating daily walking, and dealing with the rigid structure of PALT. |
| Singh et al. [27] | 2018 | Qualitative (thematic analysis) | To gain insight into participants’ perceptions of Personalized Adaptive Locomotor Training (PALT) and whether participation in PALT had an influence on their level of function and community living 1–2 years following discharge from PALT. | Previously participated in PALT and a semi-structured interview conducted upon completion of training, and to be able to participate in a telephone interview lasting 60 min. | PALT was conducted at the Lyndhurst Center—Toronto Rehabilitation Institute, part of the University Health Network in Canada (i.e., outpatient rehabilitation setting in Canada). | Traumatic SCI (n = 4), non-traumatic SCI (n = 2), AIS C (n = 1), and AIS D (n = 5). Neurological levels of injury ranged from C4 to T8. The age of the participants ranged from 49 to 65 years, and at the time of their interviews they had been living with SCI for between 1.9 and 2.7 years. | Male (n = 4) and female (n = 2). | 6 individual interviews conducted 1–2 years following the participants participation in PALT. | Three main themes: (1) PALT outcomes, (2) continuing the rehabilitation journey, and (3) challenges experienced since discharge from PALT. | This study revealed that after discharge from PALT, individuals with SCI experience varying levels of physical and psychological adjustment. Most participants improved in psychological well-being after an initial decline. Challenges included difficulty adjusting, need for medical intervention, and importance of physical activity and social support. The study recommends routine follow-ups post-PALT for psychological well-being and emphasizes the need for socially supportive networks and less abrupt discharges. |
| Swaffield and Cheung et al. [10] | 2022 | Qualitative descriptive (conventional content analysis) | To capture the perspectives of individuals living with SCI on community ABT programs in Canada. To explore the benefits and challenges of ABT, the facilitators and barriers to accessing ABT in the community, and the motivations for participating in ABT programs. | Adults (i.e., ≥18 years of age) with chronic (>2 years post-injury) traumatic or non-progressive, non-traumatic SCI who participated in ABT within the past year for a minimum of two months at least, weekly in a community setting in Canada. | Canadian community healthcare setting. | Traumatic SCI (n = 10); involved in ABT programs in Ontario (n = 4), Saskatchewan (n = 4), Quebec (n = 1), and Nova Scotia (n = 1). Years of ABT ranged from 1 to 11. | Male (n = 6) and female (n = 4). | Ten individual interviews. | Overarching theme: ABT is a key part of their evolving and lifelong recovery process. Five categories within the theme: (1) motivation to initiate ABT, (2) participants’ experiences of recovery, (3) participants’ perceptions of how ABT contributes to recovery, (4) participants’ perceptions of factors limiting accessibility and participation in ABT, and (5) taking ABT to the next level. | ABT is viewed as crucial for continuous recovery and well-being in individuals with SCI. Enhancing awareness and accessibility of ABT could lead to increased participation in ABT programs. |
| Theme | Sub-Theme | Category |
|---|---|---|
| 1. Factors influencing acceptance and adaptation of ABT across healthcare settings in Canada | Identity | Person-specific considerations |
| Professional roles and dynamics | ||
| Goals of therapy | ||
| Knowledge | Setting-specific considerations | |
| Current understanding of ABT definition and principles | ||
| Health system | Cost | |
| Equipment, technology, and facilities | ||
| Travel and transportation | ||
| Time | ||
| Staffing | ||
| Transitions in care | ||
| 2. Proposed solutions | Motivation, empowerment, and advocacy for ABT | |
| Desire for education and training |
| Category | Challenges Identified | Intervention Types Proposed |
|---|---|---|
| Physical capability—a person’s abilities arising from their physique and bodily functioning. | ||
| Person-specific considerations |
| Training †; Enablement †. |
| Travel and transportation |
| |
| Psychological capability—a person’s ability to perform a behaviour arising from their psychological functioning. | ||
| Person-specific considerations |
| Motivation, empowerment, and advocacy for ABT *:
Training †; Enablement †. |
| Transitions in Care |
| |
| Social opportunity—a person’s opportunity to enact a behaviour relating to the social world they inhabit, including the rules and norms that are operating and social cues. | ||
| Professional roles and dynamics |
| Motivation, empowerment, and advocacy for ABT *:
Environmental restructuring †; Modelling †; Enablement †. |
| Setting-specific considerations |
| |
| Cost |
| |
| Staffing |
| |
| Transitions in care |
| |
| Physical opportunity—a person’s opportunity to enact a behaviour that arises from objects and events in their environment, the space they inhabit, the time available, or the material and financial resources available to them. | ||
| Person-specific considerations |
| Training †; Restriction †; Environmental restructuring †; Enablement †. |
| Professional roles and dynamics |
| |
| Setting-specific considerations |
| |
| Cost |
| |
| Travel and transportation |
| |
| Staffing |
| |
| Equipment, technology, and facilities |
| |
| Time |
| |
| Transitions in care |
| |
| Reflective motivation—psychological processes of conscious planning and decision making. | ||
| Person-specific considerations |
| Desire for education and training *:
Persuasion †; Incentivization †; Coercion †; Modelling †. |
| Goals of therapy |
| |
| Current understanding of ABT definition and principles |
| |
| Automatic motivation—involves (a) responding habitually or instinctively or (b) wants and needs arising from emotions or drives. | ||
| Staffing |
| Motivation, empowerment, and advocacy for ABT *:
Incentivization †; Coercion †; Training †; Environmental restructuring †; Modelling †; Enablement †. |
| Current understanding of ABT definition and principles |
| |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jervis-Rademeyer, H.; Cheung, L.; Cesca, N.; Gauthier, C.; Walden, K.; Musselman, K.E. Implementing Activity-Based Therapy for Spinal Cord Injury Rehabilitation in Canada: Challenges and Proposed Solutions. Healthcare 2024, 12, 703. https://doi.org/10.3390/healthcare12070703
Jervis-Rademeyer H, Cheung L, Cesca N, Gauthier C, Walden K, Musselman KE. Implementing Activity-Based Therapy for Spinal Cord Injury Rehabilitation in Canada: Challenges and Proposed Solutions. Healthcare. 2024; 12(7):703. https://doi.org/10.3390/healthcare12070703
Chicago/Turabian StyleJervis-Rademeyer, Hope, Lovisa Cheung, Nicole Cesca, Cindy Gauthier, Kristen Walden, and Kristin E. Musselman. 2024. "Implementing Activity-Based Therapy for Spinal Cord Injury Rehabilitation in Canada: Challenges and Proposed Solutions" Healthcare 12, no. 7: 703. https://doi.org/10.3390/healthcare12070703