
Association of Serum Calcium Levels of Preterm Neonates at Birth with Calcium Intake from Foods and Supplements by Bedridden Women during Pregnancy

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Approval
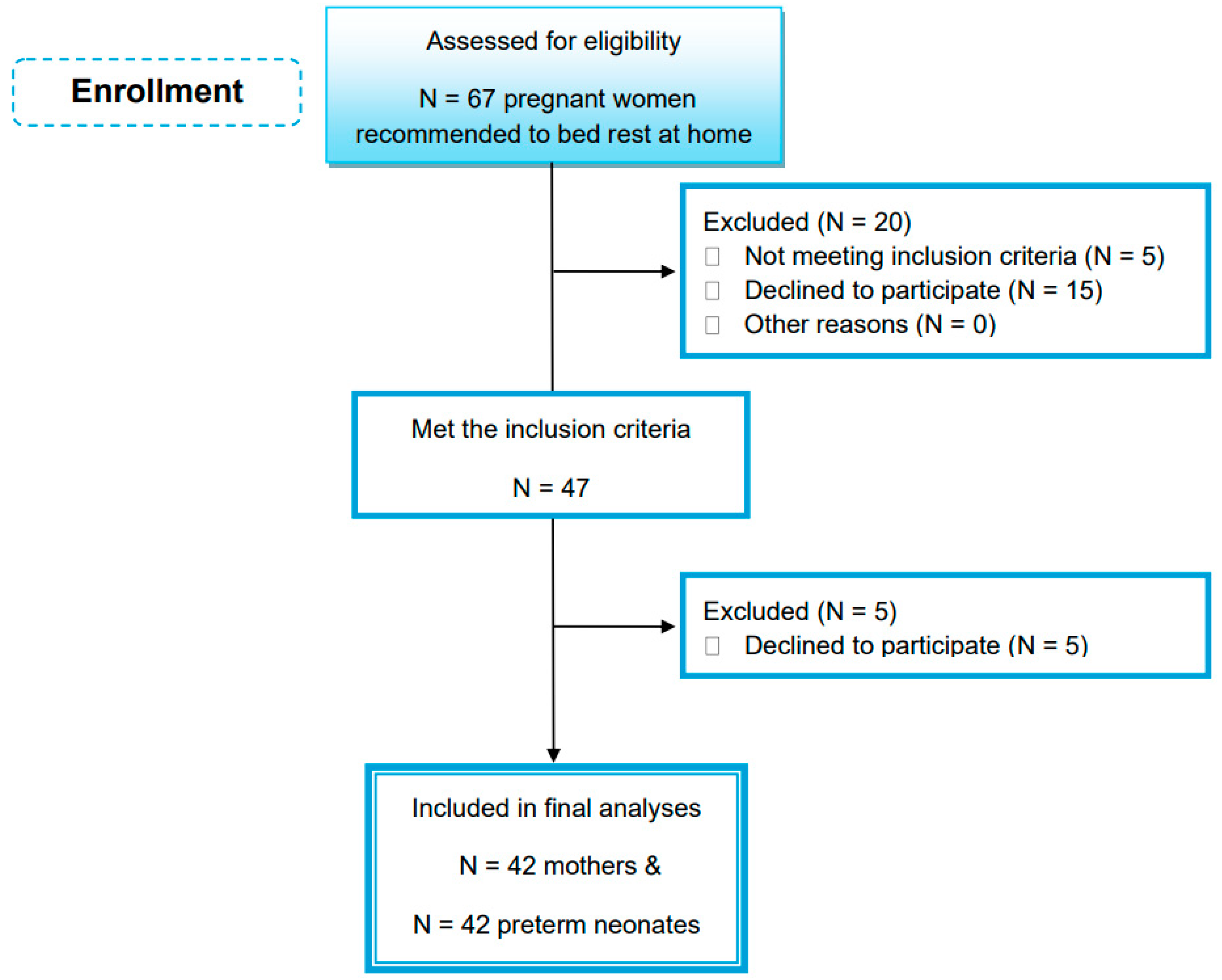
2.2. Participants and Study Design
- (a)
- Women instructed to bed rest within their home for at least two months before delivery (according to the physician’s recommendations) due to multiple gestation, vaginal bleeding, short cervical length, placenta abruption, and placenta previa. Bed rest was defined as limited ambulation of not more than 2–3 h per day with bathroom use.
- (b)
- Preterm neonates (24–37 weeks gestational age) transferred to the Neonatal Intensive Care Unit (NICU) of the hospital.
- (a)
- Women suffering from chronic diseases, e.g., inflammatory bowel diseases, irritable bowel syndrome, chronic kidney disease, malabsorption, chronic hypertension, or parathyroid diseases;
- (b)
- Women under medication treatment that could affect serum calcium levels at least for 12 months prior to delivery;
- (c)
- Pregnancy or neonate medical conditions, i.e., congenital anomalies, metabolic disorders, birth injuries, intrauterine infection, perinatal asphyxia, and life-threatening conditions;
- (d)
- Refusal to consent.
2.3. Enrolled Mothers
2.4. Preterm Neonates
2.5. Blood Measurements
2.6. Statistical Analysis
3. Results
3.1. Enrolled Mothers and Preterm Neonates
3.2. Mothers’ Characteristics
3.3. Characteristics and Calcium Status of Preterm Neonates
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raghavan, R.; Dreibelbis, C.; Kingshipp, B.; Wong, Y.C.; Abrams, B.; Gernand, A.D.; Rasmussen, K.M.; Siega-Riz, A.M.; Stang, J.; Casavale, K.O.; et al. Dietary patterns before and during pregnancy and maternal outcomes: A systematic review. Am. J. Clin. Nutr. 2019, 109, 705S–728S. [Google Scholar] [CrossRef] [PubMed]
- Chia, A.; Chen, L.Q.; Lai, J.; Wong, C.; Neelakantan, N.; Van Dam, R.M.; Chong, M.F. Maternal Dietary Patterns and Birth Outcomes: A Systematic Review and Meta-Analysis. Adv. Nutr. 2019, 10, 685–695. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Liu, F.; Li, S. Metabolic Adaptations in Pregnancy: A review. Ann. Nutr. Metab. 2017, 70, 59–65. [Google Scholar] [CrossRef]
- White, C.M. Calcium metabolism in pregnancy and lactation. Obstet. Med. 2009, 2, 2–5. [Google Scholar] [CrossRef] [PubMed]
- Hsu, S.; Levine, M. Perinatal calcium metabolism: Physiology and pathophysiology. Semin. Neonatol. 2004, 9, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, L.S.; Fung, E.B.; Halloran, B.P.; Turnlund, J.R.; Van Loan, M.D.; Cann, C.E.; King, J.R. A longitudinal study of calcium homeostasis during human pregnancy and lactation and after resumption of menses. Am. J. Clin. Nutr. 1998, 67, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Hellmeyer, L.; Ziller, V.; Anderer, G.; Ossendorf, A.; Schmidt, S.; Hadji, P. Biochemical Markers of Bone Turnover during Pregnancy: A Longitudinal Study. Exp. Clin. Endocrinol. Diabetes 2006, 114, 506–510. [Google Scholar] [CrossRef]
- Hacker, A.; Fung, E.B.; King, J.C. Role of calcium during pregnancy: Maternal and fetal needs. Nutr. Rev. 2012, 70, 397–409. [Google Scholar] [CrossRef]
- O’Brien, K.O.; Donangelo, C.M.; Zapata CL, V.; Abrams, S.A.; Spencer, E.M.; King, J.C. Bone calcium turnover during pregnancy and lactation in women with low calcium diets is associated with calcium intake and circulating insulin-like growth factor 1 concentrations. Am. J. Clin. Nutr. 2006, 83, 317–323. [Google Scholar] [CrossRef]
- Cullers, A.; King, J.C.; Van Loan, M.D.; Gildengorin, G.; Fung, E.B. Effect of prenatal calcium supplementation on bone during pregnancy and 1 y postpartum. Am. J. Clin. Nutr. 2019, 109, 197–206. [Google Scholar] [CrossRef]
- Kovacs, C.S. Maternal mineral and bone metabolism during pregnancy, lactation, and Post-Weaning recovery. Physiol. Rev. 2016, 96, 449–547. [Google Scholar] [CrossRef] [PubMed]
- Koo, W.W.; Walters, J.; Esterlitz, J.; Levine, R.J.; Bush, A.; Sibai, B.M. Maternal calcium supplementation and fetal bone mineralization. Obstet. Gynecol. 1999, 94, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, B.; Aygün, C.; Çetinoğlu, E.Ç. Vitamin D levels in newborns and association with neonatal hypocalcemia. J. Matern.-Fetal Neonatal Med. 2018, 31, 1889–1893. [Google Scholar] [CrossRef] [PubMed]
- Land, C.; Schoenau, E. Fetal and postnatal bone development: Reviewing the role of mechanical stimuli and nutrition. Best Pract. Res. Clin. Endocrinol. Metab. 2008, 22, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Chacham, S.; Pasi, R.; Chegondi, M.; Ahmad, N.; Mohanty, S.B. Metabolic bone disease in premature neonates: An unmet challenge. J. Clin. Res. Pediatr. Endocrinol. 2019, 12, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Lauder, J.R.; Sciscione, A.; Biggio, J.R.; Osmundson, S.S. Society for Maternal-Fetal Medicine Consult Series #50: The role of activity restriction in obstetric management. Am. J. Obstet. Gynecol. 2020, 223, B2–B10. [Google Scholar] [CrossRef] [PubMed]
- Zerwekh, J.E.; Ruml, L.A.; Gottschalk, F.A.; Pak, C.Y. The effects of twelve weeks of bed rest on bone histology, biochemical markers of bone turnover, and calcium homeostasis in eleven normal subjects. J. Bone Miner. Res. 2009, 13, 1594–1601. [Google Scholar] [CrossRef]
- Vuralli, D. Clinical approach to hypocalcemia in newborn period and infancy: Who should be treated? Int. J. Pediatr. 2019, 2019, 4318075. [Google Scholar] [CrossRef]
- WHO, Global Database on Body Mass Index (BMI). Available online: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations (accessed on 6 May 2010).
- Rasmussen, K.M.; Yaktine, A.L. Institute of Medicine (IOM) and National Research Council (NRC) Committee to Reexamine IOM Pregnancy Weight Guidelines. Weight Gain during Pregnancy: Reexamining the Guidelines; National Academies Press (US): Washington, DC, USA, 2009. [Google Scholar]
- Katsouyanni, K.; Rimm, E.B.; Gnardellis, C.; Trichopoulos, D.; Polychronopoulos, E.; Trichopoulou, A. Reproducibility and relative validity of an extensive semi-quantitative food frequency questionnaire using dietary records and biochemical markers among Greek schoolteachers. Int. J. Epidemiol. 1997, 26, S118–S127. [Google Scholar] [CrossRef]
- Institute of Medicine US Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. The National Academies collection: Reports funded by National Institutes of Health. In Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; National Academies Press (US): Washington, DC, USA, 2011. [Google Scholar]
- Fenton, T.R.; Kim, J.N. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef]
- Abrams, S.A. Vitamin D in Preterm and full-term infants. Ann. Nutr. Metab. 2020, 76 (Suppl. 2), 6–14. [Google Scholar] [CrossRef] [PubMed]
- Wagner, C.L.; Greer, F.R. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. Pediatrics 2008, 122, 1142–1152. [Google Scholar] [CrossRef] [PubMed]
- Wójcik, M.J.; Jaworski, M.; Płudowski, P. 25(OH)D concentration in neonates, infants, and toddlers from Poland—Evaluation of trends during years 1981–2011. Front. Endocrinol. 2018, 9, 656. [Google Scholar] [CrossRef] [PubMed]
- Kaji, T.; Yasui, T.; Suto, M.; Mitani, R.; Morine, M.; Uemura, H.; Maeda, K.; Irahara, M. Effect of bed rest during pregnancy on bone turnover markers in pregnant and postpartum women. Bone 2007, 40, 1088–1094. [Google Scholar] [CrossRef] [PubMed]
- Willemse, J.P.M.M.; Meertens, L.J.E.; Scheepers, H.C.; Achten, N.M.J.; Eussen, S.J.P.M.; Van Dongen, M.C.J.M.; Smits, L.J. Calcium intake from diet and supplement use during early pregnancy: The Expect study I. Eur. J. Nutr. 2019, 59, 167–174. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Guideline: Calcium Supplementation in Pregnant Women. Available online: https://www.who.int/publications/i/item/9789240003118 (accessed on 17 April 2020).
- Korhonen, P.; Tihtonen, K.; Isojärvi, J.; Ojala, R.; Ashorn, U.; Ashorn, P.; Tammela, O. Calcium supplementation during pregnancy and long-term offspring outcome: A systematic literature review and meta-analysis. Ann. N. Y. Acad. Sci. 2022, 1510, 36–51. [Google Scholar] [CrossRef] [PubMed]
- Dokos, C.; Tsakalidis, C.; Manaridou, K.; Karayianni, P.; Kyrkos, I.; Roussos, I. Clinical-laboratory findings of bone metabolism in healthy premature and full-term neonates: Preliminary results. Clin. Cases Miner. Bone Metab. Off. J. Ital. Soc. Osteoporos. Miner. Metab. Skelet. Dis. 2017, 14, 167–172. [Google Scholar] [CrossRef]
- Kozgar, S.A.M.; Chay, P.; Munns, C.F. Screening of vitamin D and calcium concentrations in neonates of mothers at high risk of vitamin D deficiency. BMC Pediatr. 2020, 20, 332. [Google Scholar] [CrossRef]
- Pettifor, J.M.; Prentice, A. The role of vitamin D in paediatric bone health. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 573–584. [Google Scholar] [CrossRef]
- Skouroliakou, M.; Ntountaniotis, D.; Massara, P.; Koutri, K. Investigation of multiple factors which may contribute to vitamin D levels of bedridden pregnant women and their preterm neonates. J. Matern.-Fetal Neonatal Med. 2015, 29, 2596–2601. [Google Scholar] [CrossRef]
- Laraia, B.A.; Bodnar, L.M.; Siega-Riz, A.M. Pregravid body mass index is negatively associated with diet quality during pregnancy. Public Health Nutr. 2007, 10, 920–926. [Google Scholar] [CrossRef]
- Cormick, G.; Betrán, A.P.; Romero, I.B.; Lombardo, C.F.; Gülmezoglu, A.M.; Ciapponi, A.; Belizán, J.M. Global inequities in dietary calcium intake during pregnancy: A systematic review and meta-analysis. BJOG Int. J. Obstet. Gynaecol. 2019, 126, 444–456. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, K.L.; Heneghan, C.; McNulty, B.; Brennan, L.; McAuliffe, F.M. Lifestyle and dietary habits of an obese pregnant cohort. Matern. Child Health J. 2015, 19, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Jaramillo, P.; Barajas, J.; Rueda-Quijano, S.M.; Lopez-Lopez, C.; Felix, C. Obesity and preeclampsia: Common pathophysiological mechanisms. Front. Physiol. 2018, 9, 1838. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Chen, C.; Zhu, J.; Tang, W.; Jacobs, D.R.; Shikany, J.M.; Kahe, K. Calcium intake is inversely related to risk of obesity among American young adults over a 30-year follow-up. J. Nutr. 2021, 151, 2383–2389. [Google Scholar] [CrossRef] [PubMed]
- Wortsman, J.; Matsuoka, L.Y.; Chen, T.C.; Lu, Z.; Holick, M.F. Decreased bioavailability of vitamin D in obesity. Am. J. Clin. Nutr. 2000, 72, 690–693. [Google Scholar] [CrossRef] [PubMed]
- Bodnar, L.M.; Catov, J.M.; Roberts, J.M.; Simhan, H.N. Prepregnancy obesity predicts poor vitamin D status in mothers and their neonates. J. Nutr. 2007, 137, 2437–2442. [Google Scholar] [CrossRef]


{kind=link}
| Mothers’ Characteristics | N (%) | Mean ± SD |
|---|---|---|
| Age at delivery (years) | 42 (100) | 37.55 ± 6.74 |
| Smoking status | ||
| Smoker | 3 (7.1) | - |
| Non-smoker | 39 (92.9) | - |
| Reasons for bed rest | ||
| Placenta abruption | 40 (95.2) | - |
| Short cervical length | 2 (4.8) | - |
| Duration of bed rest (months) | 42 (100) | 2.26 ± 0.33 |
| Pre-pregnancy BMI (kg/m2) | 42 (100) | 23.66 ± 3.95 |
| Underweight (BMI < 18.5 kg/m2) | 1 (2.4) | - |
| Normal weight (BMI = 18.5–24.9 kg/m2) | 32 (76.2) | 22.14 ± 1.76 |
| Overweight (BMI = 25–29.9 kg/m2) | 6 (14.3) | 27.85 ± 1.91 |
| Obesity (BMI ≥ 30 kg/m2) | 3 (7.1) | 33.56 ± 2.74 |
| Body weight gain during pregnancy (kg) | 42 (100) | 13.45 ± 8.27 |
| Inadequate | 22 (52.4) | 9.05 ± 4.46 |
| Normal | 10 (23.8) | 15.20 ± 6.25 |
| Excessive | 10 (23.8) | 21.40 ± 10.27 |
| Body weight on the day of delivery (kg) | 42 (100) | 74.45 ± 11.56 |
| Body weight on the day after delivery (kg) | 42 (100) | 68.24 ± 9.75 |
| Serum 25-OH-D levels (ng/ml) | 42 (100) | 17.24 ± 10.07 |
| Serum 25-OH-D status | ||
| Adequacy (≥30 ng/mL) | 4 (9.5) | 37.55 ± 10.36 |
| Inadequacy (20–29 ng/mL) | 10 (23.8) | 24.93 ± 2.79 |
| Deficiency (<20 ng/mL) | 28 (66.7) | 11.60 ± 4.85 |
| Women taking oral supplements other than calcium | ||
| Prenatal multivitamin | 10 (23.8) | - |
| Vitamins (D, folic acid) | 7 (16.7) | - |
| Minerals (Fe, Mg) | 6 (14.3) | - |
| Combination of prenatal multivitamins, vitamins (D, folic acid) and minerals (Fe, Mg) | 19 (45.2) | - |
| Daily intake of calcium supplement during pregnancy | ||
| Use of 500 mg calcium supplement /day | 21 (50.0) | - |
| No use of calcium supplement | 21 (50.0) | - |
| Total daily calcium intake from foods and supplements during pregnancy (mg/day) in all women | 42 (100) | 974.33 ± 361.96 |
| Total daily calcium intake during pregnancy | ||
| Equal or greater than 1000 mg/day | 22 (52.4) | 1258.45 ± 145.01 |
| Lower than 1000 mg/day | 20 (47.6) | 661.80 ± 251.37 |
| Daily calcium intake solely from foods during pregnancy (mg/day) in all women | 42 (100) | 701.71 ± 263.12 |
| Daily calcium intake solely from foods during pregnancy | ||
| ≥1000 mg of food derived calcium /day | 5 (11.9) | 1112.00 ± 69.96 |
| <1000 mg of food derived calcium /day | 37 (88.1) | 646.27 ± 227.51 |
| Neonates’ Serum Calcium Levels (mg/dL) (N = 42) | N (N %) | Mean ± SD | p-Value |
|---|---|---|---|
| Based on mothers’ pre-pregnancy BMI status | |||
| Normal weight | 32 (76.2) | 8.47 ± 0.80 | 0.143 |
| Overweight/obesity | 9 (21.4) | 8.92 ± 0.80 | |
| Based on mothers’ calcium supplementation | |||
| Calcium supplementation group | 21 (50.0) | 8.90 ± 0.58 | <0.001 * |
| Non-calcium supplementation group | 21 (50.0) | 8.31 ± 0.97 |
| Tested Association | Unadjusted Model | Adjusted Model 1 | Adjusted Model 2 | |||
|---|---|---|---|---|---|---|
| Neonates’ Ca status | Beta | p-value | Beta | p-value | Beta | p-value |
| Mother’s Ca supplementation | +0.351 | 0.023 | +0.360 | 0.025 | +0.460 | 0.025 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gioxari, A.; Papandreou, P.; Daskalou, E.; Kaliora, A.C.; Skouroliakou, M. Association of Serum Calcium Levels of Preterm Neonates at Birth with Calcium Intake from Foods and Supplements by Bedridden Women during Pregnancy. Healthcare 2024, 12, 693. https://doi.org/10.3390/healthcare12060693
Gioxari A, Papandreou P, Daskalou E, Kaliora AC, Skouroliakou M. Association of Serum Calcium Levels of Preterm Neonates at Birth with Calcium Intake from Foods and Supplements by Bedridden Women during Pregnancy. Healthcare. 2024; 12(6):693. https://doi.org/10.3390/healthcare12060693
Chicago/Turabian StyleGioxari, Aristea, Panos Papandreou, Efstratia Daskalou, Andriana C. Kaliora, and Maria Skouroliakou. 2024. "Association of Serum Calcium Levels of Preterm Neonates at Birth with Calcium Intake from Foods and Supplements by Bedridden Women during Pregnancy" Healthcare 12, no. 6: 693. https://doi.org/10.3390/healthcare12060693