
Exploring the Impact of Web-Based vs. In-Person Exercise Training on Benefits and Adherence in Substance Use Disorder Interventions: A Pilot Study
 , , , , , ,
, , , , , ,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
Training Program
2.3. Evaluation
2.3.1. Physical Fitness Test for SUD
- 6-min Walk Test (6MWT)
- Curl Test (Upper-body strength)
- Chair Stand Test (lower-body strength)
2.3.2. Quality of Life
2.3.3. Physical Fitness Test for HA
- Aerobic capacity
- Upper body strength
- Lower body strength
2.3.4. Adherence
2.4. Data Analysis
3. Results
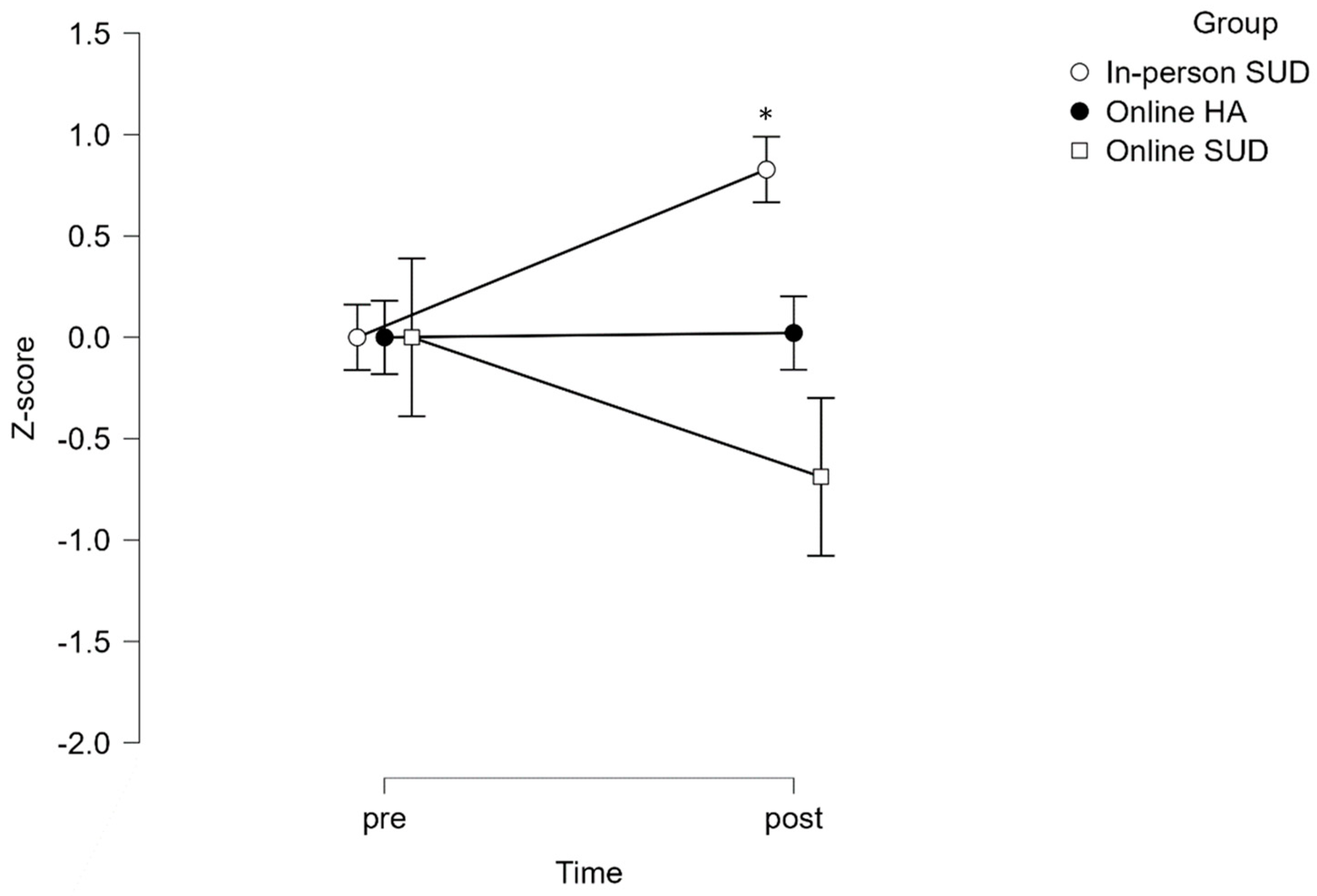
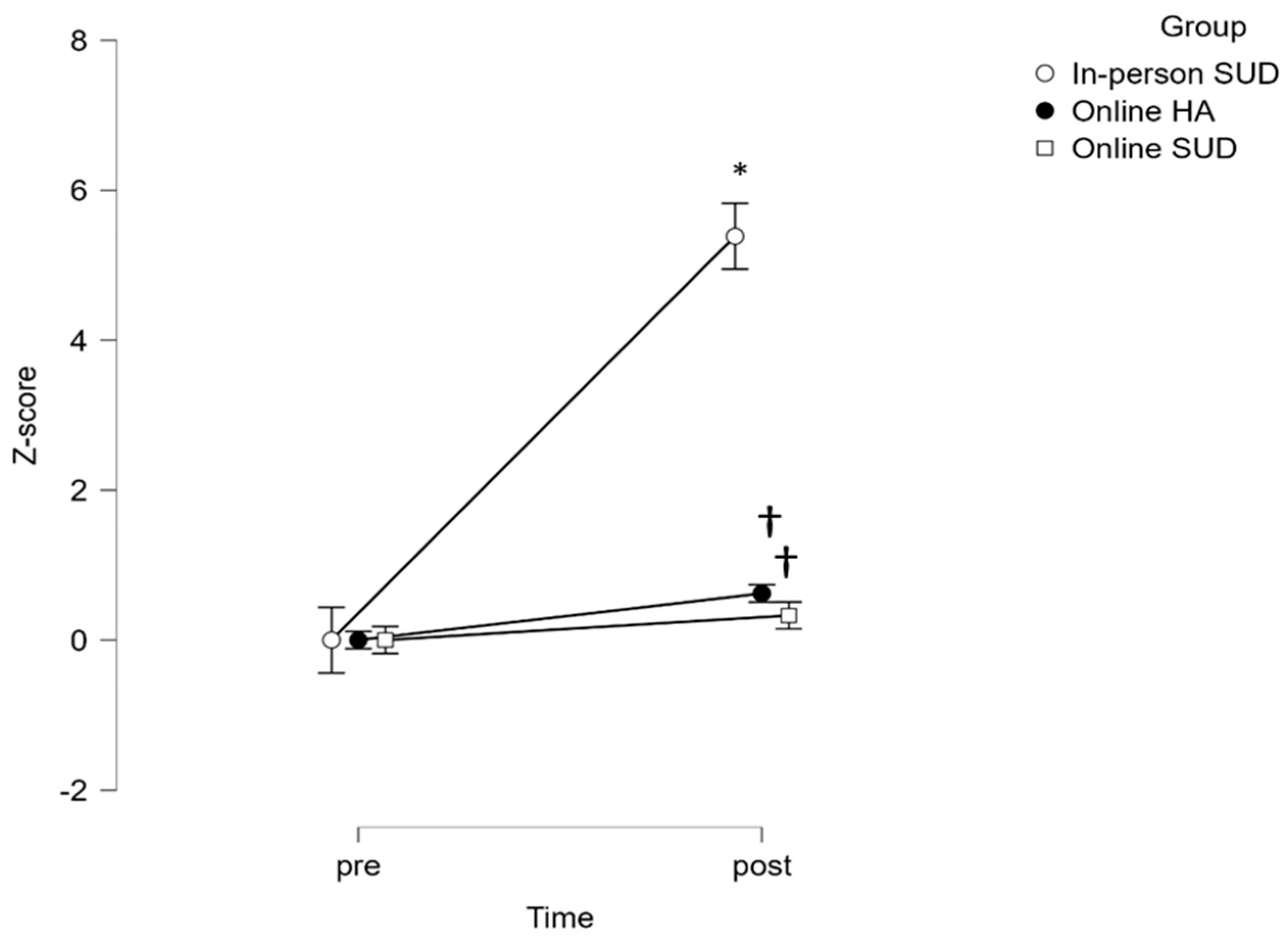
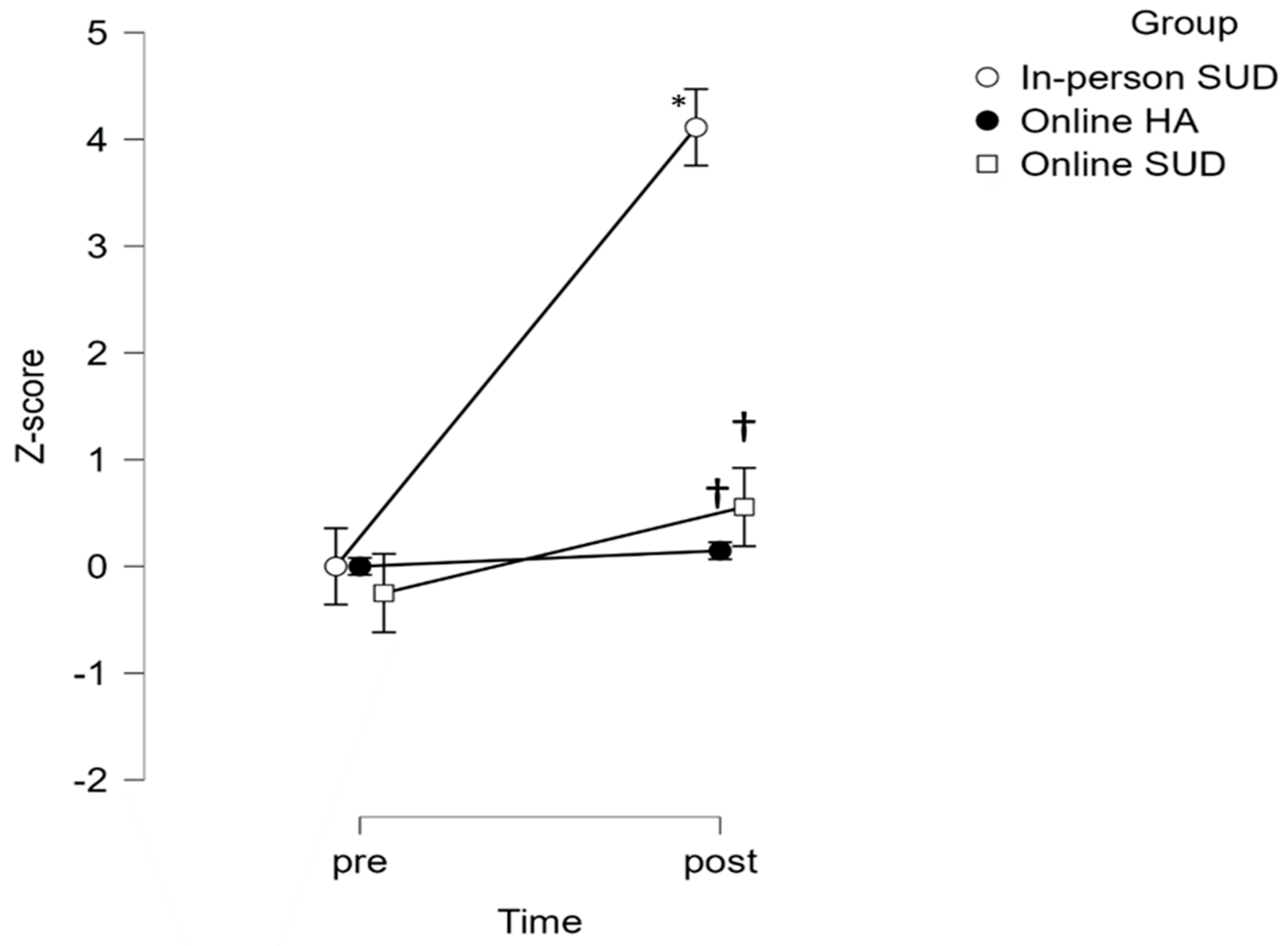
3.1. Fitness
3.2. Adherence
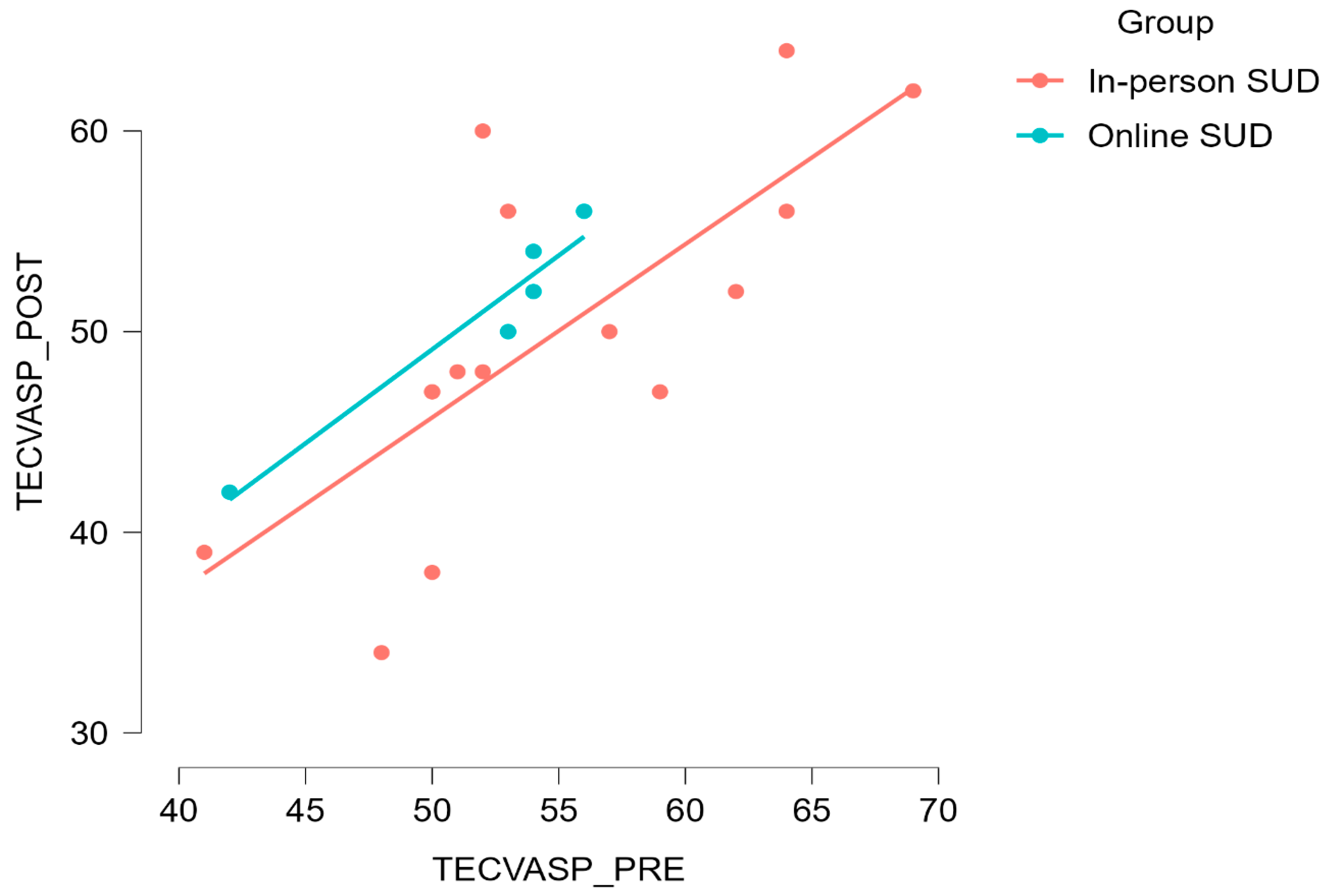
3.3. Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Publishing: Arlington, VA, USA, 2013; ISBN 0-89042-555-8. [Google Scholar]
- Méndez-Aguado, C.; Cangas, A.J.; Lirola, M.J.; Cerezuela, J.L.; López-Pardo, A.; Méndez-Aguado, C.; Cangas, A.J.; Lirola, M.J.; Cerezuela, J.L.; López-Pardo, A. Benefits and Barriers of Physical Activity in Social Inclusion and Quality of Life in People with Serious Mental Disorders. In Mental Health-Preventive Strategies; IntechOpen: London, UK, 2022. [Google Scholar] [CrossRef]
- Hosseinbor, M.; Ardekani, S.M.Y.; Bakhshani, S.; Bakhshani, S. Emotional and Social Loneliness in Individuals with and without Substance Dependence Disorder. Int. J. High Risk Behav. Addict. 2014, 3, 22688. [Google Scholar] [CrossRef]
- Piche, F.; Daneau, C.; Plourde, C.; Girard, S.; Romain, A.J. Characteristics and Impact of Physical Activity Interventions during Substance Use Disorder Treatment Excluding Tobacco: A Systematic Review. PLoS ONE 2023, 18, e0283861. [Google Scholar] [CrossRef]
- Thompson, T.P.; Horrell, J.; Taylor, A.H.; Wanner, A.; Husk, K.; Wei, Y.; Creanor, S.; Kandiyali, R.; Neale, J.; Sinclair, J.; et al. Physical Activity and the Prevention, Reduction, and Treatment of Alcohol and Other Drug Use across the Lifespan (the PHASE Review): A Systematic Review. Ment. Health Phys. Act. 2020, 19, 100360. [Google Scholar] [CrossRef]
- Kvam, S.; Kleppe, C.L.; Nordhus, I.H.; Hovland, A. Exercise as a Treatment for Depression: A Meta-Analysis. J. Affect. Disord. 2016, 202, 67–86. [Google Scholar] [CrossRef]
- Dürmüş, P.T.; Vardar, M.E.; Kaya, O.; Tayfur, P.; Süt, N.; Vardar, S.A. Evaluation of the Effects of High Intensity Interval Training on Cytokine Levels and Clinical Course in Treatment of Opioid Use Disorder. Turk Psikiyatr. Derg. 2020, 31, 151–158. [Google Scholar] [CrossRef]
- Abrantes, A.M.; Blevins, C.E. Exercise in the Context of Substance Use Treatment: Key Issues and Future Directions. Curr. Opin. Psychol. 2019, 30, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Helgadóttir, B.; Hallgren, M.; Kullberg, C.L.E.; Forsell, Y. Sticking with It? Factors Associated with Exercise Adherence in People with Mild to Moderate Depression. Psychol. Sport Exerc. 2018, 35, 104–110. [Google Scholar] [CrossRef]
- Hallgren, K.A.; Dembe, A.; Pace, B.T.; Imel, Z.E.; Lee, C.M.; Atkins, D.C. Variability in Motivational Interviewing Adherence across Sessions, Providers, Sites, and Research Contexts. J. Subst. Abuse Treat. 2018, 84, 30–41. [Google Scholar] [CrossRef]
- Lappan, S.N.; Brown, A.W.; Hendricks, P.S. Dropout Rates of In-Person Psychosocial Substance Use Disorder Treatments: A Systematic Review and Meta-Analysis. Addiction 2020, 115, 201–217. [Google Scholar] [CrossRef]
- Andersson, H.W.; Steinsbekk, A.; Walderhaug, E.; Otterholt, E.; Nordfjærn, T. Predictors of Dropout from Inpatient Substance Use Treatment: A Prospective Cohort Study. Subst. Abuse 2018, 12, 1178221818760551. [Google Scholar] [CrossRef]
- Vancampfort, D.; Sánchez, C.P.R.; Hallgren, M.; Schuch, F.; Firth, J.; Rosenbaum, S.; Van Damme, T.; Stubbs, B. Dropout from Exercise Randomized Controlled Trials among People with Anxiety and Stress-Related Disorders: A Meta-Analysis and Meta-Regression. J. Affect. Disord. 2021, 282, 996–1004. [Google Scholar] [CrossRef]
- Welford, P.; Gunillasdotter, V.; Andreasson, S.; Herring, M.P.; Vancampfort, D.; Hallgren, M. Sticking with It? Factors Associated with Exercise Adherence in People with Alcohol Use Disorder. Addict. Behav. 2023, 144, 107730. [Google Scholar] [CrossRef]
- Abrantes, A.M.; Battle, C.L.; Strong, D.R.; Ing, E.; Dubreuil, M.E.; Gordon, A.; Brown, R.A. Exercise Preferences of Patients in Substance Abuse Treatment. Ment. Health Phys. Act. 2011, 4, 79–87. [Google Scholar] [CrossRef]
- Carneiro, L.; Rosenbaum, S.; Ward, P.B.; Clemente, F.M.; Ramirez-Campillo, R.; Monteiro-Junior, R.S.; Martins, A.; Afonso, J. Web-Based Exercise Interventions for Patients with Depressive and Anxiety Disorders: A Systematic Review of Randomized Controlled Trials. Braz. J. Psychiatry 2022, 44, 331–341. [Google Scholar] [CrossRef]
- Vandelanotte, C.; Duncan, M.J.; Plotnikoff, R.C.; Rebar, A.; Alley, S.; Schoeppe, S.; To, Q.; Mummery, W.K.; Short, C.E. Impact of a Web-Based Personally Tailored Physical Activity Intervention on Depression, Anxiety, Stress and Quality of Life: Secondary Outcomes from a Randomized Controlled Trial. Ment. Health Phys. Act. 2022, 23, 100477. [Google Scholar] [CrossRef]
- Joseph, R.P.; Durant, N.H.; Benitez, T.J.; Pekmezi, D.W. Internet-Based Physical Activity Interventions. Am. J. Lifestyle Med. 2014, 8, 42. [Google Scholar] [CrossRef]
- Moore, B.A.; Fazzino, T.; Garnet, B.; Cutter, C.J.; Barry, D.T. Computer-Based Interventions for Drug Use Disorders: A Systematic Review. J. Subst. Abuse Treat. 2011, 40, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Panagiotou, M.; Zlatintsi, A.; Filntisis, P.P.; Roumeliotis, A.J.; Efthymiou, N.; Maragos, P. A Comparative Study of Autoencoder Architectures for Mental Health Analysis Using Wearable Sensors Data. In Proceedings of the 2022 30th European Signal Processing Conference (EUSIPCO), Belgrade, Serbia, 29 August–2 September 2022; IEEE: Piscataway, NJ, USA, 2022; pp. 1258–1262. [Google Scholar]
- Okobi, O.E.; Sobayo, T.O.; Arisoyin, A.E.; Adeyemo, D.A.; Olaleye, K.T.; Nelson, C.O.; Sanusi, I.A.; Salawu, M.A.; Akinsete, A.O.; Emore, E. Association between the Use of Wearable Devices and Physical Activity among US Adults with Depression and Anxiety: Evidence from the 2019 and 2020 Health Information National Trends Survey. Cureus 2023, 15, e39521. [Google Scholar] [CrossRef] [PubMed]
- Onyeaka, H.; Firth, J.; Enemuo, V.; Muoghalu, C.; Naslund, J.; Baiden, P.; Torous, J. Exploring the Association between Electronic Wearable Device Use and Levels of Physical Activity among Individuals with Depression and Anxiety: A Population Level Study. Front. Digit Health 2021, 3, 707900. [Google Scholar] [CrossRef]
- Zhang, Z.; Liu, X. A Systematic Review of Exercise Intervention Program for People with Substance Use Disorder. Front. Psychiatry 2022, 13, 817927. [Google Scholar] [CrossRef] [PubMed]
- Belin, D.; Belin-Rauscent, A.; Murray, J.E.; Everitt, B.J. Addiction: Failure of Control over Maladaptive Incentive Habits. Curr. Opin. Neurobiol. 2013, 23, 564–572. [Google Scholar] [CrossRef]
- Casanova-Lizón, A.; Sarabia, J.M.; Pastor, D.; Javaloyes, A.; Peña-González, I.; Moya-Ramón, M. Designing an App to Promote Physical Exercise in Sedentary People Using a Day-to-Day Algorithm to Ensure a Healthy Self-Programmed Exercise Training. Int. J. Environ. Res. Public Health 2023, 20, 1528. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Functional Fitness Normative Scores for Community-Residing Older Adults, Ages 60–94. J. Aging Phys. Act. 1999, 7, 162–181. [Google Scholar] [CrossRef]
- Lozano Rojas, Ó.M.; Rojas Tejada, A.; Pérez Meléndez, C.; Apraiz Granados, B.; Sánchez Muñoz, F.; Marín Bedoya, A. Test Para La Evaluación de La Calidad de Vida En Adictos a Sustancias Psicoactivas (TECVASP): Estudios de Fiabilidad y Validez. Trastor. Adict. 2007, 9, 97–107. [Google Scholar] [CrossRef]
- Zubaran, C.; Sud, R.; Emerson, J.; Zolfaghari, E.; Foresti, K.; Lozano, O. Validation of the English Version of the Health-Related Quality of Life for Drug Abusers (HRQoLDA) Test. Eur. Addict. Res. 2012, 18, 220–227. [Google Scholar] [CrossRef]
- Bruce, R.A. Exercise Testing of Patients with Coronary Heart Disease. Principles and Normal Standards for Evaluation. Ann. Clin. Res. 1971, 3, 323–332. [Google Scholar]
- Bayles, M.P.; Swank, A.M. ACSM’s Exercise Testing and Prescription. In Sport & Exercise Scientist; LWW: Philadelphia, PA, USA, 2018; pp. 273–275. [Google Scholar]
- Lorenzetti, S.; Ostermann, M.; Zeidler, F.; Zimmer, P.; Jentsch, L.; List, R.; Taylor, W.R.; Schellenberg, F. How to Squat? Effects of Various Stance Widths, Foot Placement Angles and Level of Experience on Knee, Hip and Trunk Motion and Loading. BMC Sport. Sci. Med. Rehabil. 2018, 10, 14. [Google Scholar] [CrossRef] [PubMed]
- Cheadle, C.; Vawter, M.P.; Freed, W.J.; Becker, K.G. Analysis of Microarray Data Using Z Score Transformation. J. Mol. Diagn. 2003, 5, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Wangberg, S.C.; Bergmo, T.S.; Johnsen, J.-A.K. Adherence in Internet-Based Interventions. Patient Prefer. Adherence 2008, 2, 57–65. [Google Scholar] [PubMed]
- Vella, S.A.; Aidman, E.; Teychenne, M.; Smith, J.J.; Swann, C.; Rosenbaum, S.; White, R.L.; Lubans, D.R. Optimising the Effects of Physical Activity on Mental Health and Wellbeing: A Joint Consensus Statement from Sports Medicine Australia and the Australian Psychological Society. J. Sci. Med. Sport 2023, 26, 132–139. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.B.; Stubbs, B. Exercise as a Treatment for Depression: A Meta-Analysis Adjusting for Publication Bias. J. Psychiatr. Res. 2016, 77, 42–51. [Google Scholar] [CrossRef]
- Krentzman, A.R.; Mannella, K.A.; Hassett, A.L.; Barnett, N.P.; Cranford, J.A.; Brower, K.J.; Higgins, M.M.; Meyer, P.S. Feasibility, Acceptability, and Impact of a Web-Based Gratitude Exercise among Individuals in Outpatient Treatment for Alcohol Use Disorder. J. Posit. Psychol. 2015, 10, 477–488. [Google Scholar] [CrossRef] [PubMed]
- Mamen, A.; Pallesen, S.; Martinsen, E.W. Changes in Mental Distress Following Individualized Physical Training in Patients Suffering from Chemical Dependence. Eur. J. Sport Sci. 2011, 11, 269–276. [Google Scholar] [CrossRef]
- Brown, R.A.; Abrantes, A.M.; Read, J.P.; Marcus, B.H.; Jakicic, J.; Strong, D.R.; Oakley, J.R.; Ramsey, S.E.; Kahler, C.W.; Stuart, G.L.; et al. A Pilot Study of Aerobic Exercise as an Adjunctive Treatment for Drug Dependence. Ment. Health Phys. Act. 2010, 3, 27–34. [Google Scholar] [CrossRef]
- Roessler, K.K. Exercise Treatment for Drug Abuse—A Danish Pilot Study. Scand. J. Public Health 2010, 38, 664–669. [Google Scholar] [CrossRef]
- Giménez-Meseguer, J.; Tortosa-Martínez, J.; de los Remedios Fernández-Valenciano, M. Benefits of Exercise for the Quality of Life of Drug-Dependent Patients. J. Psychoact. Drugs 2015, 47, 409–416. [Google Scholar] [CrossRef]
- Mamen, A.; Martinsen, E.W. Development of Aerobic Fitness of Individuals with Substance Abuse/Dependence Following Long-Term Individual Physical Activity. Eur. J. Sport Sci. 2010, 10, 255–262. [Google Scholar] [CrossRef]
- Muller, A.E.; Clausen, T. Group Exercise to Improve Quality of Life among Substance Use Disorder Patients. Scand. J. Public Health 2015, 43, 146–152. [Google Scholar] [CrossRef]
- Kraal, J.J.; Vromen, T.; Spee, R.; Kemps, H.M.C.; Peek, N. The Influence of Training Characteristics on the Effect of Exercise Training in Patients with Coronary Artery Disease: Systematic Review and Meta-Regression Analysis. Int. J. Cardiol. 2017, 245, 52–58. [Google Scholar] [CrossRef]
- Volkow, N. Drugs, Brains, and Behavior. The Science of Addiction; National Institute on Drug Abuse: North Bethesda, MD, USA, 2014.
- Zschucke, E.; Heinz, A.; Strhle, A. Exercise and Physical Activity in the Therapy of Substance Use Disorders. Sci. World J. 2012, 2012, 901741. [Google Scholar] [CrossRef]
- Garfield, J.B.B.; Lubman, D.I.; Yücel, M. Anhedonia in Substance Use Disorders: A Systematic Review of Its Nature, Course and Clinical Correlates. Aust. N. Z. J. Psychiatry 2014, 48, 36–51. [Google Scholar] [CrossRef] [PubMed]
- Hatzigiakoumis, D.S.; Martinotti, G.; Di Giannantonio, M.; Janiri, L. Anhedonia and Substance Dependence: Clinical Correlates and Treatment Options. Front. Psychiatry 2011, 2, 9204. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| In-Person SUD Group | Online SUD Group | Online HA | |
|---|---|---|---|
| Men/women | 10/5 | 4/1 | 3/3 |
| Age (years) | 47.5 ± 6.5 | 46.8 ± 8.5 | 38.0 ± 9.7 |
| Weight (kg) | 81.9 ± 13.0 | 84.0 ± 15.6 | 65.8 ± 13.7 |
| Height (cm) | 170.9 ± 7.8 | 172.5 ± 8.9 | 166.42 ± 7.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montón-Martínez, R.; Ballester-Ferrer, J.A.; Baladzhaeva, S.; Sempere-Ruiz, N.; Casanova-Lizón, A.; Roldan, A.; Pastor, D.; Sarabia, J.M.; Javaloyes, A.; Peña-González, I.; et al. Exploring the Impact of Web-Based vs. In-Person Exercise Training on Benefits and Adherence in Substance Use Disorder Interventions: A Pilot Study. Healthcare 2024, 12, 684. https://doi.org/10.3390/healthcare12060684
Montón-Martínez R, Ballester-Ferrer JA, Baladzhaeva S, Sempere-Ruiz N, Casanova-Lizón A, Roldan A, Pastor D, Sarabia JM, Javaloyes A, Peña-González I, et al. Exploring the Impact of Web-Based vs. In-Person Exercise Training on Benefits and Adherence in Substance Use Disorder Interventions: A Pilot Study. Healthcare. 2024; 12(6):684. https://doi.org/10.3390/healthcare12060684
Chicago/Turabian StyleMontón-Martínez, Roberto, Juan Arturo Ballester-Ferrer, Sabina Baladzhaeva, Noemí Sempere-Ruiz, Antonio Casanova-Lizón, Alba Roldan, Diego Pastor, José Manuel Sarabia, Alejandro Javaloyes, Iván Peña-González, and et al. 2024. "Exploring the Impact of Web-Based vs. In-Person Exercise Training on Benefits and Adherence in Substance Use Disorder Interventions: A Pilot Study" Healthcare 12, no. 6: 684. https://doi.org/10.3390/healthcare12060684