
Trunk Muscle Activity and Ratio of Local Muscle to Global Muscle Activity during Supine Bridge Exercises under Unstable Conditions in Young Participants with and without Chronic Low Back Pain
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
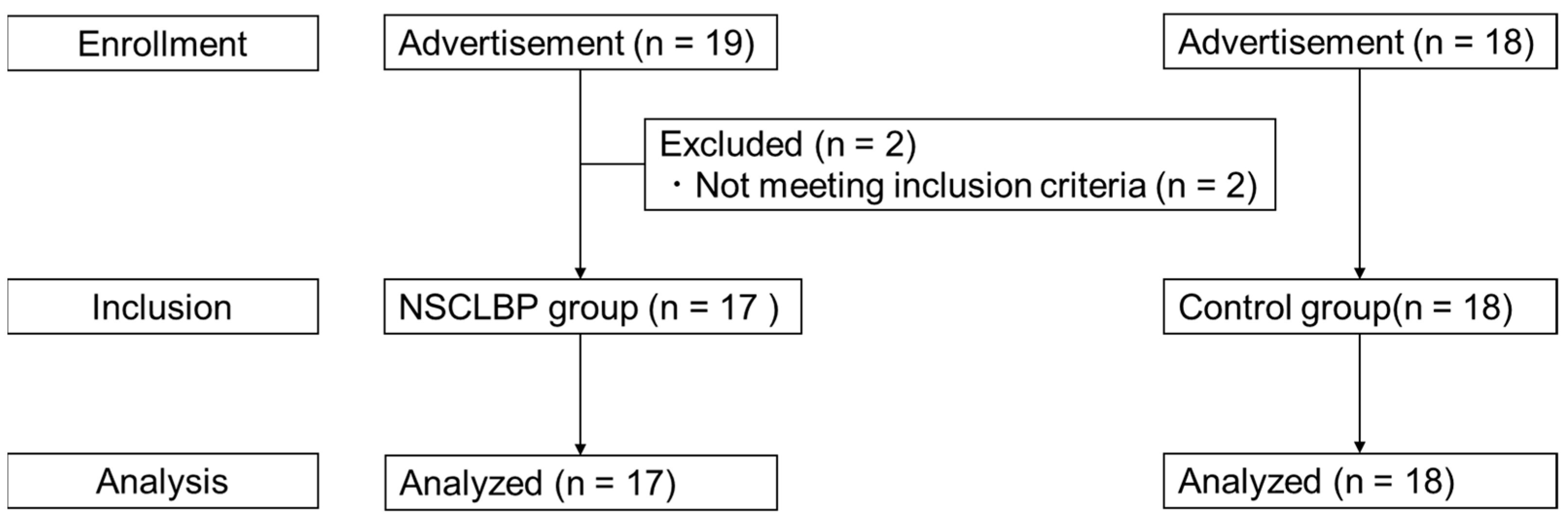
2.1. Participants
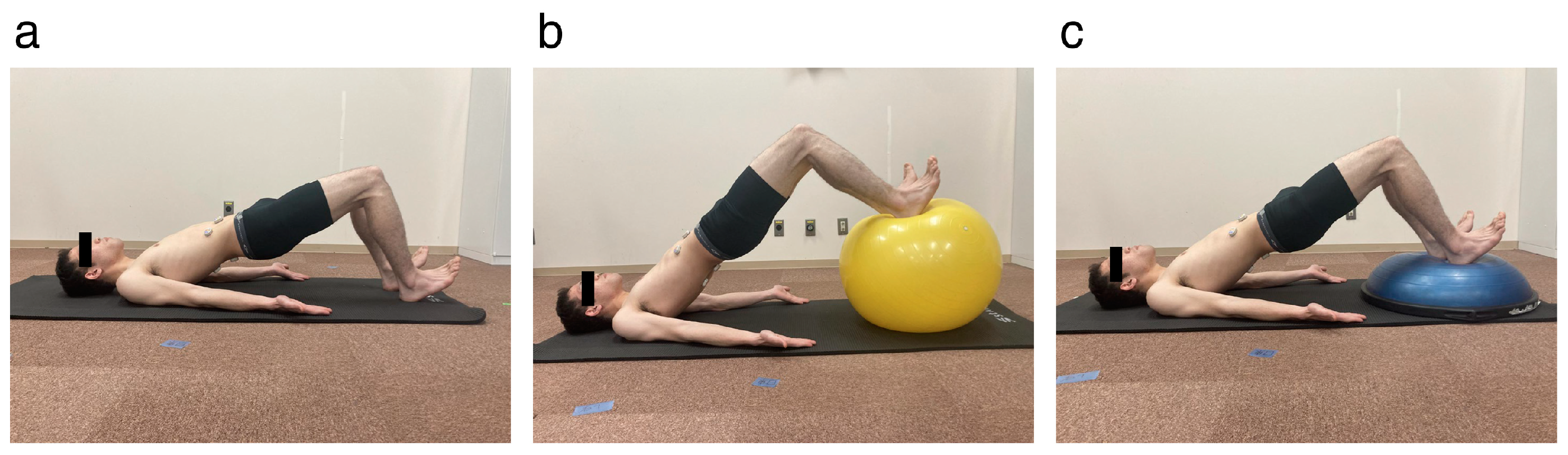
2.2. Experimental Procedures
2.3. Electromyography Evaluation
2.4. Maximum Voluntary Isometric Contraction Trials
2.5. Data Analysis
2.6. Statistical Analyses
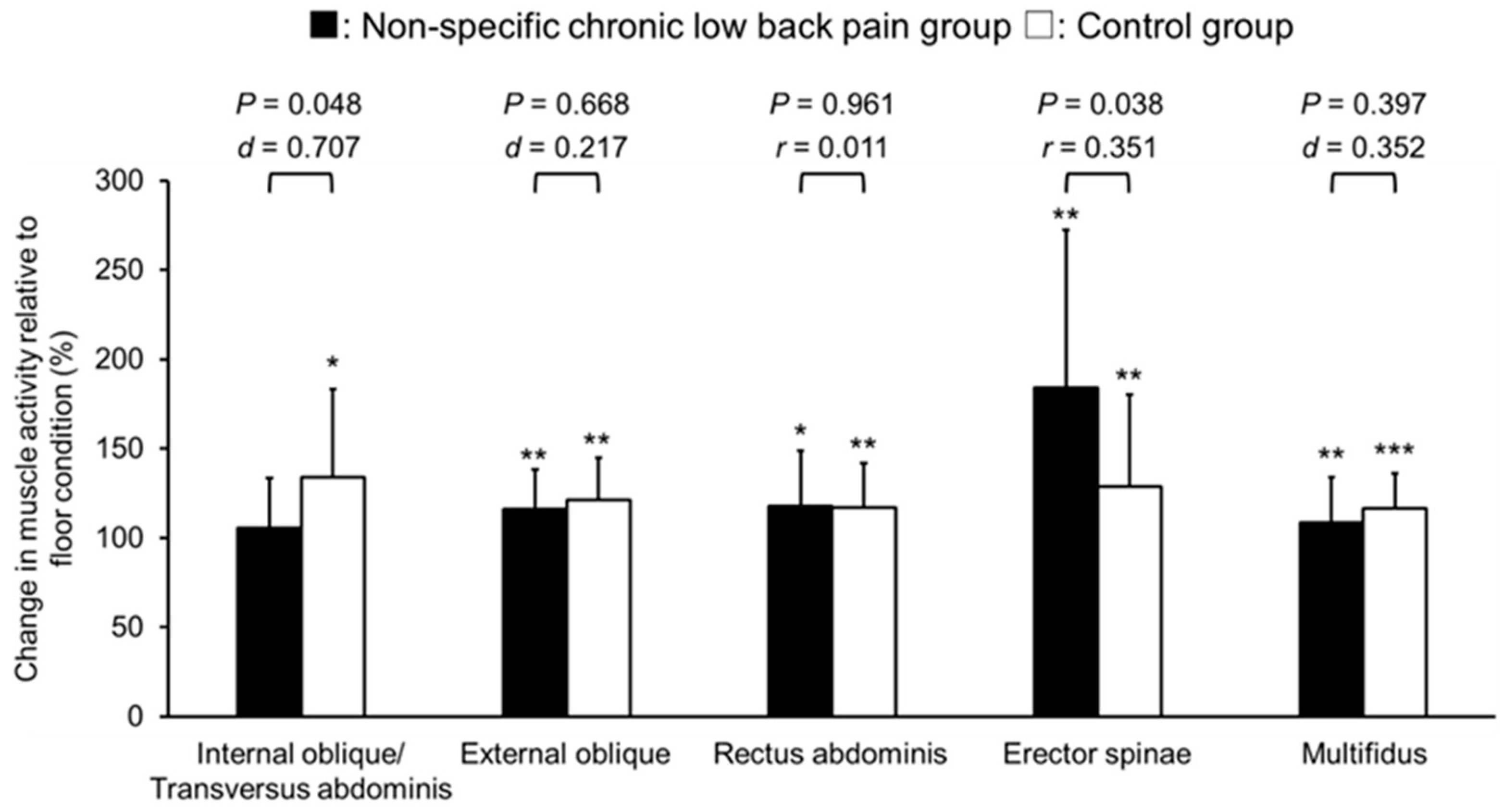
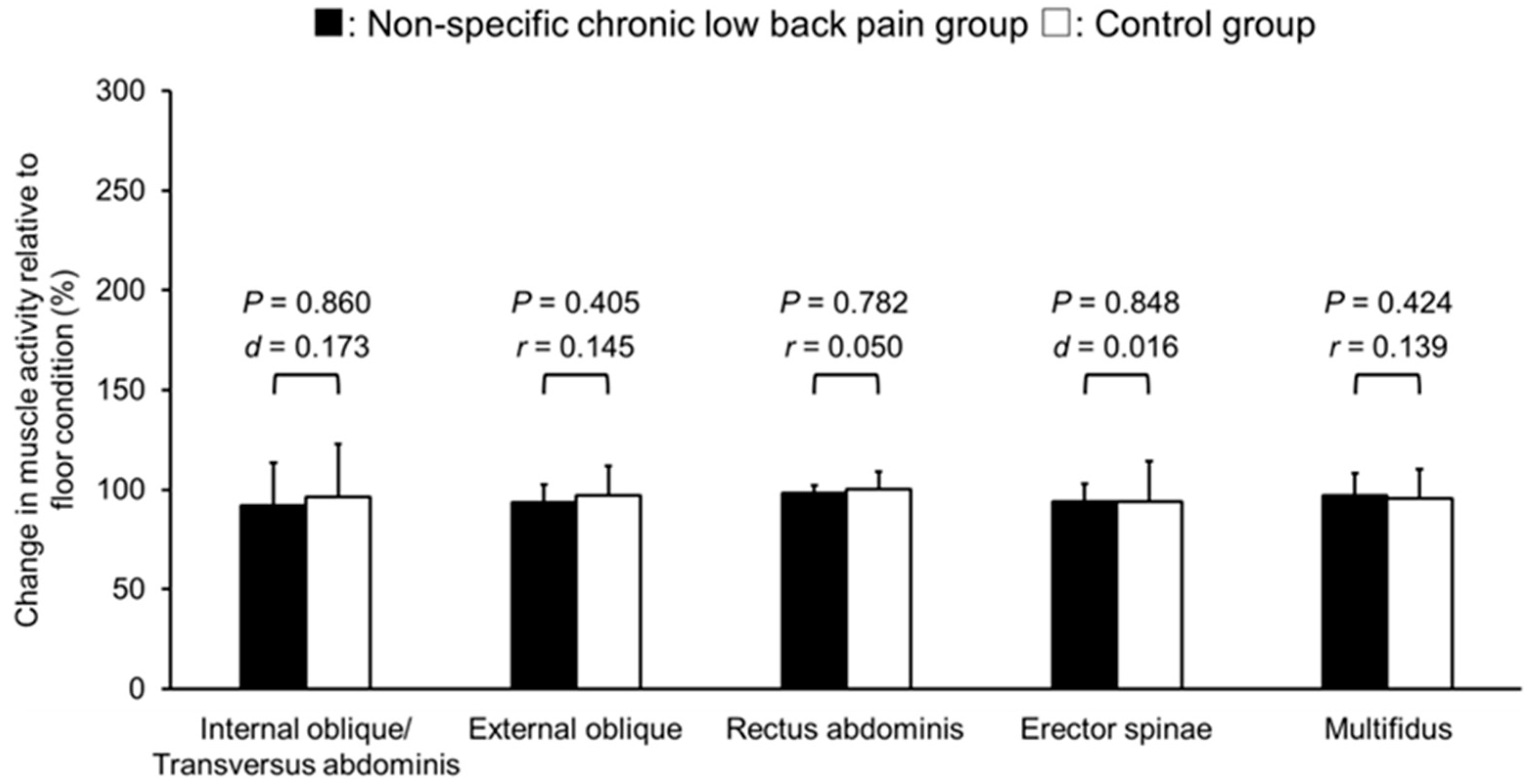
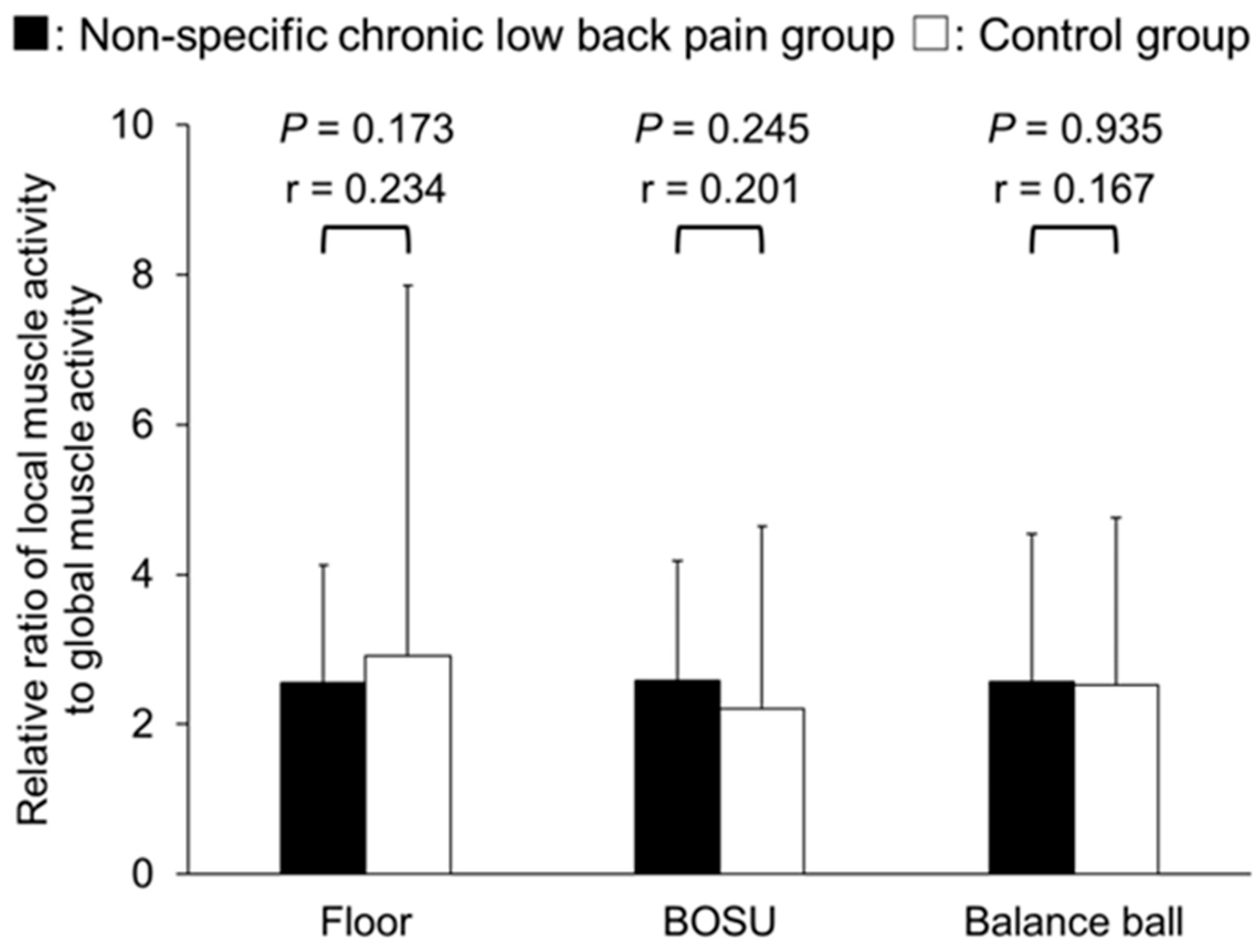
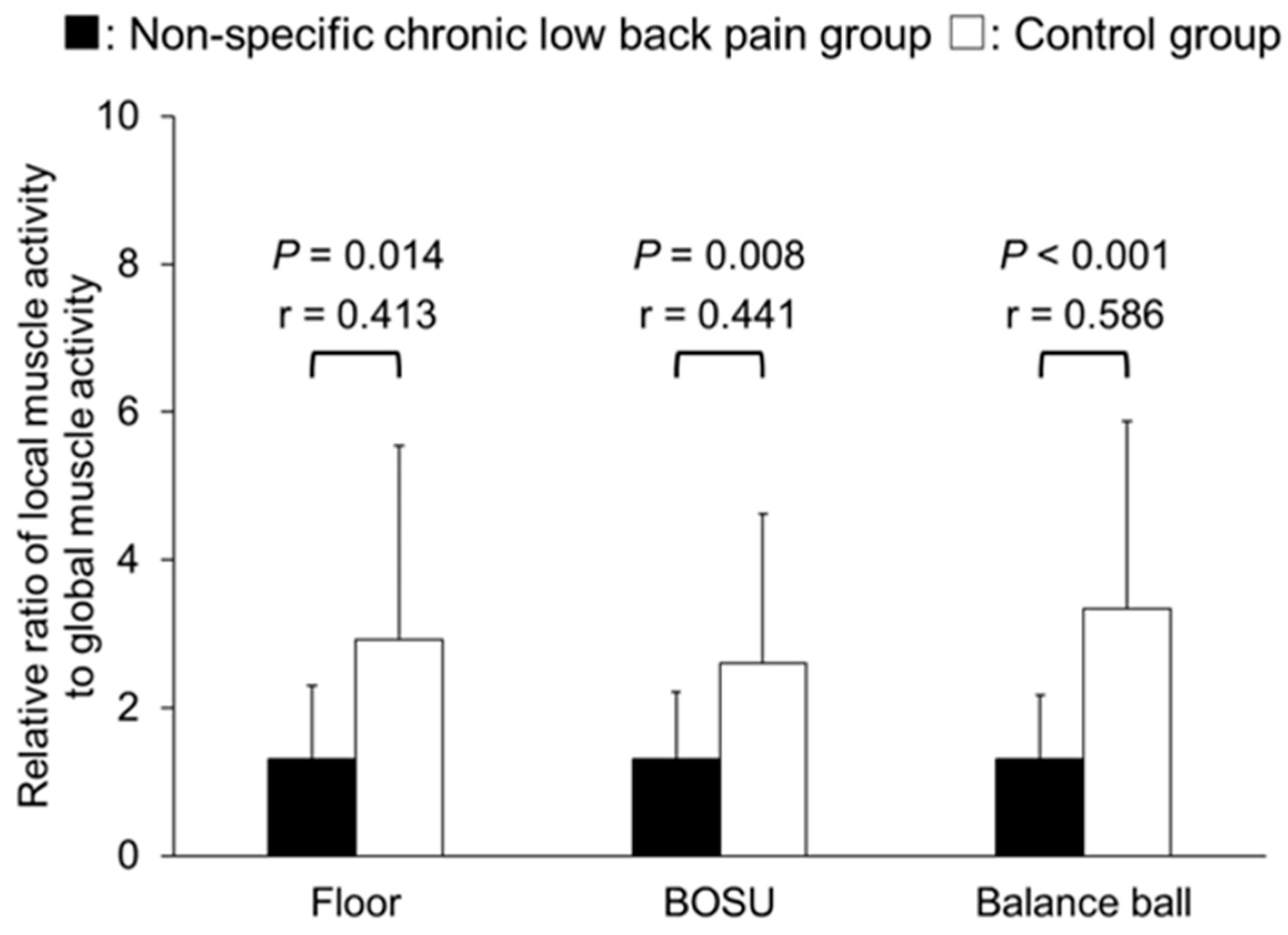
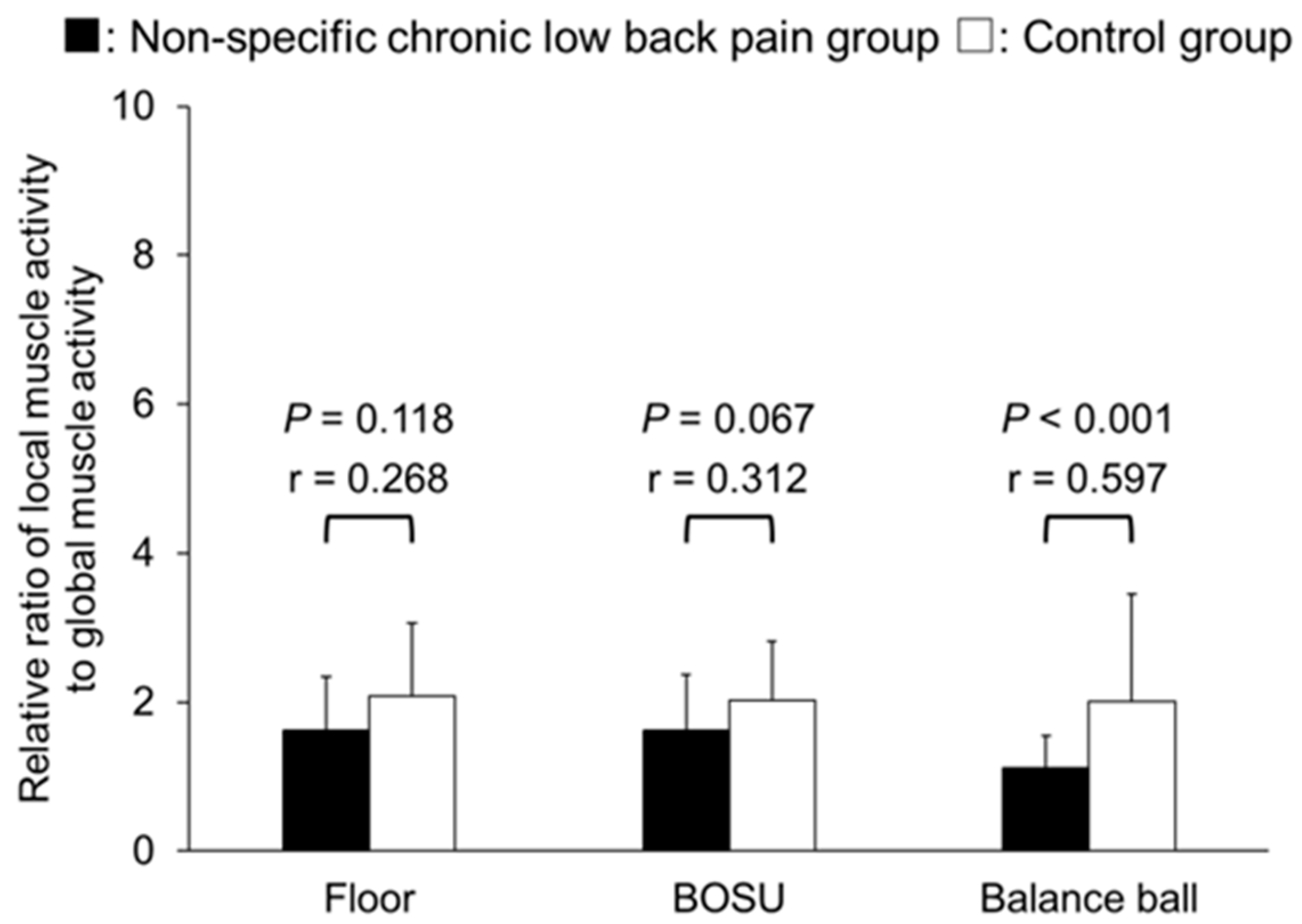
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gore, M.; Sadosky, A.; Stacey, B.R.; Tai, K.S.; Leslie, D. The burden of chronic low back pain: Clinical comorbidities, treatment patterns, and health care costs in usual care settings. Spine 2012, 37, E668–E677. [Google Scholar] [CrossRef]
- Maher, C.; Underwood, M.; Buchbinder, R. Non-specific low back pain. Lancet 2017, 389, 736–747. [Google Scholar] [CrossRef]
- Airaksinen, O.; Brox, J.I.; Cedraschi, C.; Hildebrandt, J.; Klaber-Moffett, J.; Kovacs, F.; Mannion, A.F.; Reis, S.; Staal, J.B.; Ursin, H.; et al. Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur. Spine J. 2006, 15 (Suppl. S2), S192–S300. [Google Scholar] [CrossRef]
- van Tulder, M.; Becker, A.; Bekkering, T.; Breen, A.; del Real, M.T.; Hutchinson, A.; Koes, B.; Laerum, E.; Malmivaara, A.; COST B13 Working Group on Guidelines for the Management of Acute Low Back Pain in Primary Care. Chapter 3. European guidelines for the management of acute nonspecific low back pain in primary care. Eur. Spine J. 2006, 15 (Suppl. S2), S169–S191. [Google Scholar] [CrossRef]
- Menezes Costa, L.D.C.; Maher, C.G.; Hancock, M.J.; McAuley, J.H.; Herbert, R.D.; Costa, L.O. The prognosis of acute and persistent low-back pain: A meta-analysis. CMAJ 2012, 184, E613–E624. [Google Scholar] [CrossRef]
- Menezes Costa, L.D.C.; Maher, C.G.; McAuley, J.H.; Hancock, M.J.; Herbert, R.D.; Refshauge, K.M.; Henschke, N. Prognosis for patients with chronic low back pain: Inception cohort study. BMJ 2009, 339, b3829. [Google Scholar] [CrossRef]
- Miura, T.; Yamanaka, M.; Ukishiro, K.; Tohyama, H.; Saito, H.; Samukawa, M.; Kobayashi, T.; Ino, T.; Takeda, N. Individuals with chronic low back pain do not modulate the level of transversus abdominis muscle contraction across different postures. Man. Ther. 2014, 19, 534–540. [Google Scholar] [CrossRef]
- van Dieën, J.H.; Cholewicki, J.; Radebold, A. Trunk muscle recruitment patterns in patients with low back pain enhance the stability of the lumbar spine. Spine 2003, 28, 834–841. [Google Scholar] [CrossRef]
- Hodges, P.W.; Coppieters, M.W.; MacDonald, D.; Cholewicki, J. New insight into motor adaptation to pain revealed by a combination of modelling and empirical approaches. Eur. J. Pain 2013, 17, 1138–1146. [Google Scholar] [CrossRef]
- Radebold, A.; Cholewicki, J.; Panjabi, M.M.; Patel, T.C. Muscle response pattern to sudden trunk loading in healthy individuals and in patients with chronic low back pain. Spine 2000, 25, 947–954. [Google Scholar] [CrossRef]
- Bergmark, A. Stability of the lumbar spine. A study in mechanical engineering. Acta Orthop. Scand. Suppl. 1989, 230, 1–54. [Google Scholar] [CrossRef]
- Hodges, P.W.; Richardson, C.A. Inefficient muscular stabilization of the lumbar spine associated with low back pain. A motor control evaluation of transversus abdominis. Spine 1996, 21, 2640–2650. [Google Scholar] [CrossRef]
- Osuka, S.; Koshino, Y.; Yamanaka, M.; Miura, T.; Saito, Y.; Ueno, R.; Ishida, T.; Samukawa, M.; Tohyama, H. The onset of deep abdominal muscles activity during tasks with different trunk rotational torques in subjects with non-specific chronic low back pain. J. Orthop. Sci. 2019, 24, 770–775. [Google Scholar] [CrossRef]
- Suehiro, T.; Ishida, H.; Kobara, K.; Osaka, H.; Kurozumi, C. Trunk muscle activation patterns during active hip abduction test during remission from recurrent low back pain: An observational study. BMC Musculoskelet. Disord. 2021, 22, 671. [Google Scholar] [CrossRef]
- Hodges, P.; van den Hoorn, W.; Dawson, A.; Cholewicki, J. Changes in the mechanical properties of the trunk in low back pain may be associated with recurrence. J. Biomech. 2009, 42, 61–66. [Google Scholar] [CrossRef]
- Gildea, J.E.; van den Hoorn, W.; Hides, J.A.; Hodges, P.W. Trunk dynamics are impaired in ballet dancers with back pain but improve with imagery. Med. Sci. Sports Exerc. 2015, 47, 1665–1671. [Google Scholar] [CrossRef]
- Richardson, C.A.; Jull, G.; Hodges, P.W.; Hides, J.A. Therapeutic Exercise for Spinal Segmental Stabilization in Low Back Pain: Scientific Basis and Clinical Approach; Churchill Livingstone: London, UK, 1999. [Google Scholar]
- O’Sullivan, P.B.; Twomey, L.; Allison, T.G. Altered abdominal muscle recruitment in patients with chronic back pain following a specific exercise intervention. J. Orthop. Sports Phys. Ther. 1998, 27, 114–124. [Google Scholar] [CrossRef]
- Stevens, V.K.; Bouche, K.G.; Mahieu, N.N.; Coorevits, P.L.; Vanderstraeten, G.G.; Danneels, L.A. Trunk muscle activity in healthy subjects during bridging stabilization exercises. BMC Musculoskelet. Disord. 2006, 7, 75. [Google Scholar] [CrossRef]
- Hayden, J.A.; Ellis, J.; Ogilvie, R.; Malmivaara, A.; van Tulder, M.W. Exercise therapy for chronic low back pain. Cochrane Database Syst. Rev. 2021, 9, CD009790. [Google Scholar] [CrossRef]
- Oliveira, C.B.; Maher, C.G.; Pinto, R.Z.; Traeger, A.C.; Lin, C.C.; Chenot, J.F.; van Tulder, M.; Koes, B.W. Clinical practice guidelines for the management of non-specific low back pain in primary care: An updated overview. Eur. Spine J. 2018, 27, 2791–2803. [Google Scholar] [CrossRef]
- Qaseem, A.; Wilt, T.J.; McLean, R.M.; Forciea, M.A. Noninvasive treatments for acute, subacute, and chronic low back pain: A clinical practice guideline from the American College of Physicians. Ann. Intern. Med. 2017, 166, 514–530. [Google Scholar] [CrossRef]
- Marshall, P.; Murphy, B. Changes in muscle activity and perceived exertion during exercises performed on a swiss ball. Appl. Physiol. Nutr. Metab. 2006, 31, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.; Park, S. Immediate effects of isometric trunk stabilization exercises with suspension device on flexion extension ratio and strength in chronic low back pain patients. J. Back Musculoskelet. Rehabil. 2019, 32, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Feldwieser, F.M.; Sheeran, L.; Meana-Esteban, A.; Sparkes, V. Electromyographic analysis of trunk-muscle activity during stable, unstable and unilateral bridging exercises in healthy individuals. Eur. Spine J. 2012, 21 (Suppl. S2), S171–S186. [Google Scholar] [CrossRef] [PubMed]
- Imai, A.; Kaneoka, K.; Okubo, Y.; Shiina, I.; Tatsumura, M.; Izumi, S.; Shiraki, H. Trunk muscle activity during lumbar stabilization exercises on both a stable and unstable surface. J. Orthop. Sports Phys. Ther. 2010, 40, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Czaprowski, D.; Afeltowicz, A.; Gębicka, A.; Pawłowska, P.; Kędra, A.; Barrios, C.; Hadała, M. Abdominal muscle EMG-activity during bridge exercises on stable and unstable surfaces. Phys. Ther. Sport 2014, 15, 162–168. [Google Scholar] [CrossRef]
- Arab, A.M.; Ghamkhar, L.; Emami, M.; Nourbakhsh, M.R. Altered muscular activation during prone hip extension in women with and without low back pain. Chiropr. Man. Therap. 2011, 19, 18. [Google Scholar] [CrossRef]
- Garg, A.; Pathak, H.; Churyukanov, M.V.; Uppin, R.B.; Slobodin, T.M. Low back pain: Critical assessment of various scales. Eur. Spine J. 2020, 29, 503–518. [Google Scholar] [CrossRef]
- Cholewicki, J.; Panjabi, M.M.; Khachatryan, A. Stabilizing function of trunk flexor-extensor muscles around a neutral spine posture. Spine 1997, 22, 2207–2212. [Google Scholar] [CrossRef] [PubMed]
- Marshall, P.; Murphy, B. The validity and reliability of surface EMG to assess the neuromuscular response of the abdominal muscles to rapid limb movement. J. Electromyogr. Kinesiol. 2003, 13, 477–489. [Google Scholar] [CrossRef]
- Koumantakis, G.A.; Oldham, J.A. Paraspinal strength and electromyographic fatigue in patients with sub-acute back pain and controls: Reliability, clinical applicability and between-group differences. World J. Orthop. 2021, 12, 816–832. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: London, UK, 1988. [Google Scholar]
- Barker, P.J.; Briggs, C.A.; Bogeski, G. Tensile transmission across the lumbar fasciae in unembalmed cadavers: Effects of tension to various muscular attachments. Spine 2004, 29, 129–138. [Google Scholar] [CrossRef]
- Cresswell, A.G.; Grundström, H.; Thorstensson, A. Observations on intra-abdominal pressure and patterns of abdominal intra-muscular activity in man. Acta Physiol. Scand. 1992, 144, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Bartelink, D.L. The role of abdominal pressure in relieving the pressure on the lumbar intervertebral discs. J. Bone Joint Surg. Br. 1957, 39-B, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Ainscough-Potts, A.M.; Morrissey, M.C.; Critchley, D. The response of the transverse abdominis and internal oblique muscles to different postures. Man. Ther. 2006, 11, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Marras, W.S.; Ferguson, S.A.; Burr, D.; Davis, K.G.; Gupta, P. Spine loading in patients with low back pain during asymmetric lifting exertions. Spine J. 2004, 4, 64–75. [Google Scholar] [CrossRef] [PubMed]
- Mok, N.W.; Brauer, S.G.; Hodges, P.W. Failure to use movement in postural strategies leads to increased spinal displacement in low back pain. Spine 2007, 32, E537–E543. [Google Scholar] [CrossRef] [PubMed]
- Wahl, M.J.; Behm, D.G. Not all instability training devices enhance muscle activation in highly resistance-trained individuals. J. Strength. Cond. Res. 2008, 22, 1360c70. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, P.; Twomey, L.; Allison, G.; Sinclair, J.; Miller, K. Altered patterns of abdominal muscle activation in patients with chronic low back pain. Aust. J. Physiother. 1997, 43, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Saragiotto, B.T.; Maher, C.G.; Yamato, T.P.; Costa, L.O.P.; Costa, L.C.M.; Ostelo, R.W.J.G.; Macedo, L.G. Motor Control Exercise for Nonspecific Low Back Pain: A Cochrane Review. Spine 2016, 41, 1284–1295. [Google Scholar] [CrossRef]
- Xu, H.R.; Zhang, Y.H.; Zheng, Y.L. The effect and mechanism of motor control exercise on low back pain: A narrative review. EFORT Open Rev. 2023, 8, 581–591. [Google Scholar] [CrossRef]
- Owen, P.J.; Miller, C.T.; Mundell, N.L.; Verswijveren, S.J.J.M.; Tagliaferri, S.D.; Brisby, H.; Bowe, S.J.; Belavy, D.L. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br. J. Sports Med. 2020, 54, 1279–1287. [Google Scholar] [CrossRef]
- Tsao, H.; Hodges, P.W. Persistence of improvements in postural strategies following motor control training in people with recurrent low back pain. J. Electromyogr. Kinesiol. 2008, 18, 559–567. [Google Scholar] [CrossRef]
- Lee, N.G.; Jung, J.H.; You, J.S.; Kang, S.K.; Lee, D.R.; Kwon, O.Y.; Jeon, H.S. Novel augmented ADIM training using ultrasound imaging and electromyography in adults with core instability. J. Back. Musculoskelet. Rehabil. 2011, 24, 233–240. [Google Scholar] [CrossRef]
- Suehiro, T.; Ishida, H.; Kobara, K.; Osaka, H.; Kurozumi, C.; Watanabe, S. Immediate changes in trunk muscle activation patterns during a lifting task following an abdominal drawing-in exercise in subjects with recurrent low back pain. J. Back. Musculoskelet. Rehabil. 2021, 34, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Osuka, S.; Ishida, T.; Yamanaka, M.; Chiba, T.; Miura, T.; Koshino, Y.; Saito, Y.; Nakata, A.; Samukawa, M.; Kasahara, S.; et al. Abdominal draw-in maneuver changes neuromuscular responses to sudden release from trunk loading in patients with non-specific chronic low back pain. J. Orthop. Sci. 2020, 25, 781–786. [Google Scholar] [CrossRef]
- Fortin, M.; Rye, M.; Roussac, A.; Naghdi, N.; Macedo, L.G.; Dover, G.; Elliott, J.M.; DeMont, R.; Weber, M.H.; Pepin, V. The effects of combined motor control and isolated extensor strengthening versus general exercise on paraspinal muscle morphology and function in patients with chronic low back pain: A randomised controlled trial protocol. BMC Musculoskelet. Disord. 2021, 22, 472. [Google Scholar] [CrossRef] [PubMed]
- Besomi, M.; Hodges, P.W.; Clancy, E.A.; Van Dieën, J.; Hug, F.; Lowery, M.; Merletti, R.; Søgaard, K.; Wrigley, T.; Besier, T.; et al. Consensus for experimental design in electromyography (CEDE) project: Amplitude normalization matrix. J. Electromyogr. Kinesiol. 2020, 53, 102438. [Google Scholar] [CrossRef]
- Tonosu, J.; Takeshita, K.; Hara, N.; Matsudaira, K.; Kato, S.; Masuda, K.; Chikuda, H. The normative score and the cut-off value of the Oswestry Disability Index (ODI). Eur. Spine J. 2012, 21, 1596–1602. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NSCLBP Group (n = 17) | Control Group (n = 18) | p-Value | Effect Size | |
|---|---|---|---|---|
| Age, yrs | 21.8 (2.6, 19–29) | 21.6 (1.0, 20–23) | 0.245 a | 0.208 a |
| Height, cm | 166.5 (5.5, 156.4–176.1) | 164.8 (8.3, 156.4–179.5) | 0.522 | 0.241 |
| Weight, kg | 60.6 (7.8, 47.0–71.1) | 56.3 (8.2, 43.0–67.0) | 0.106 | 0.537 |
| BMI, kg/m2 | 21.8 (1.9, 19.2–25.4) | 20.6 (1.9, 17.8–24.7) | 0.061 | 0.632 |
| NRS, /10 | 3.1 (1.7, 2–7) | - | - | - |
| ODI, % | 14.2 (9.2, 2.5–26.0) | - | - | - |
| Duration of pain, yrs | 5.3 (0.25–10) | - | - | - |
| Effect Size | ||
|---|---|---|
| NSCLBP Group (n = 17) | Control Group (n = 18) | |
| Internal oblique/transversus abdominis | 0.465 a | 0.549 a |
| External oblique | 0.718 a | 0.652 a |
| Rectus abdominis | 0.591 a | 0.652 a |
| Erector spinae | 0.729 a | 0.760 |
| Multifidus | 0.752 a | 0.739 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakata, A.; Osuka, S.; Ishida, T.; Saito, Y.; Samukawa, M.; Kasahara, S.; Koshino, Y.; Oikawa, N.; Tohyama, H. Trunk Muscle Activity and Ratio of Local Muscle to Global Muscle Activity during Supine Bridge Exercises under Unstable Conditions in Young Participants with and without Chronic Low Back Pain. Healthcare 2024, 12, 514. https://doi.org/10.3390/healthcare12050514
Nakata A, Osuka S, Ishida T, Saito Y, Samukawa M, Kasahara S, Koshino Y, Oikawa N, Tohyama H. Trunk Muscle Activity and Ratio of Local Muscle to Global Muscle Activity during Supine Bridge Exercises under Unstable Conditions in Young Participants with and without Chronic Low Back Pain. Healthcare. 2024; 12(5):514. https://doi.org/10.3390/healthcare12050514
Chicago/Turabian StyleNakata, Akimi, Satoshi Osuka, Tomoya Ishida, Yuki Saito, Mina Samukawa, Satoshi Kasahara, Yuta Koshino, Naoki Oikawa, and Harukazu Tohyama. 2024. "Trunk Muscle Activity and Ratio of Local Muscle to Global Muscle Activity during Supine Bridge Exercises under Unstable Conditions in Young Participants with and without Chronic Low Back Pain" Healthcare 12, no. 5: 514. https://doi.org/10.3390/healthcare12050514