
Exploration of Evaluation Practices in Social Prescribing Services in Ireland: A Cross-Sectional Observational Study
 ,
,  , and
, and
Abstract
:1. Introduction
2. Methods and Materials
2.1. Participants
2.2. Data Collection Methods
2.3. Data Analysis
3. Results
3.1. Profile of Social Prescribing Services
3.2. Evaluation Methods
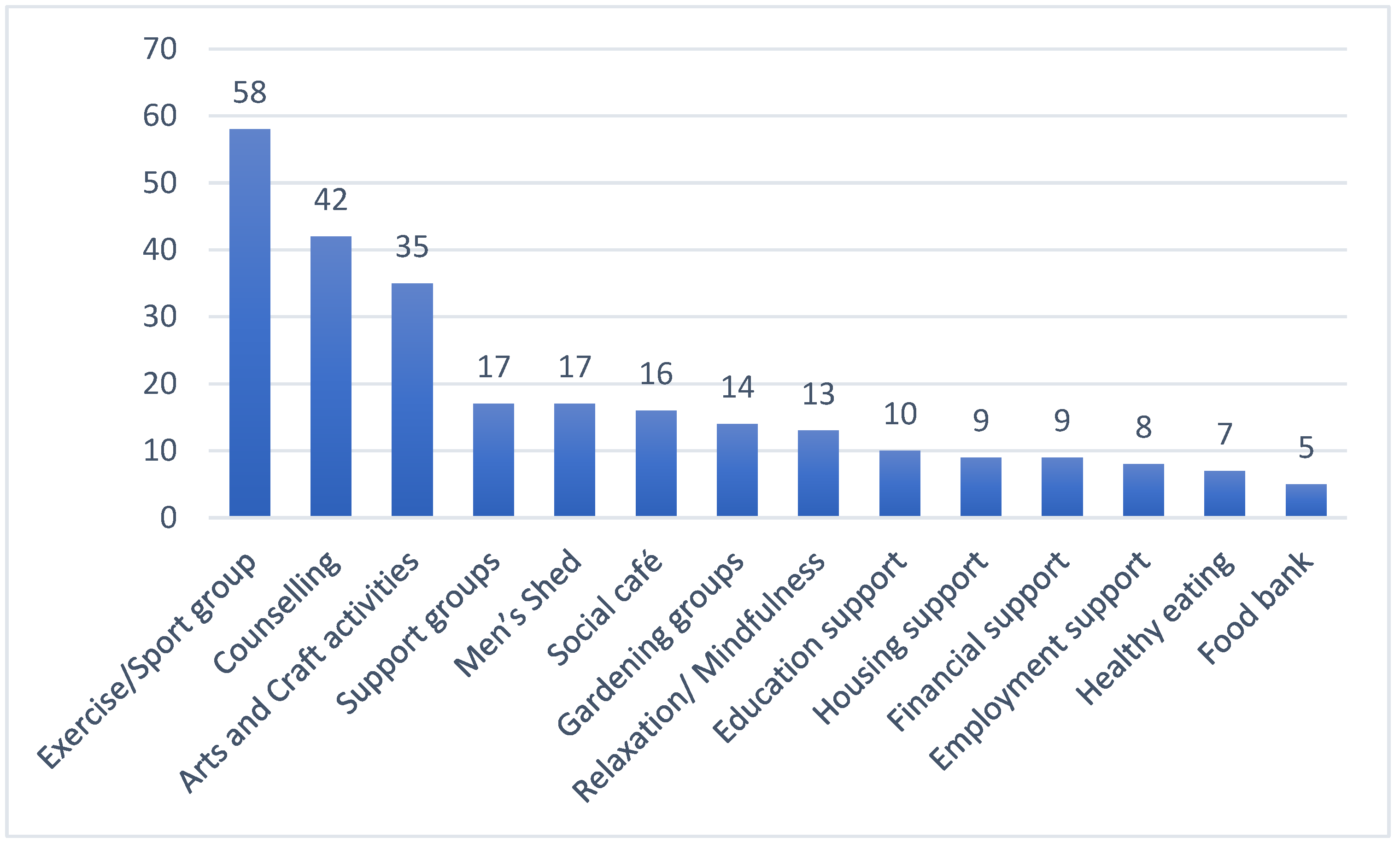
3.3. Community Services and Activities
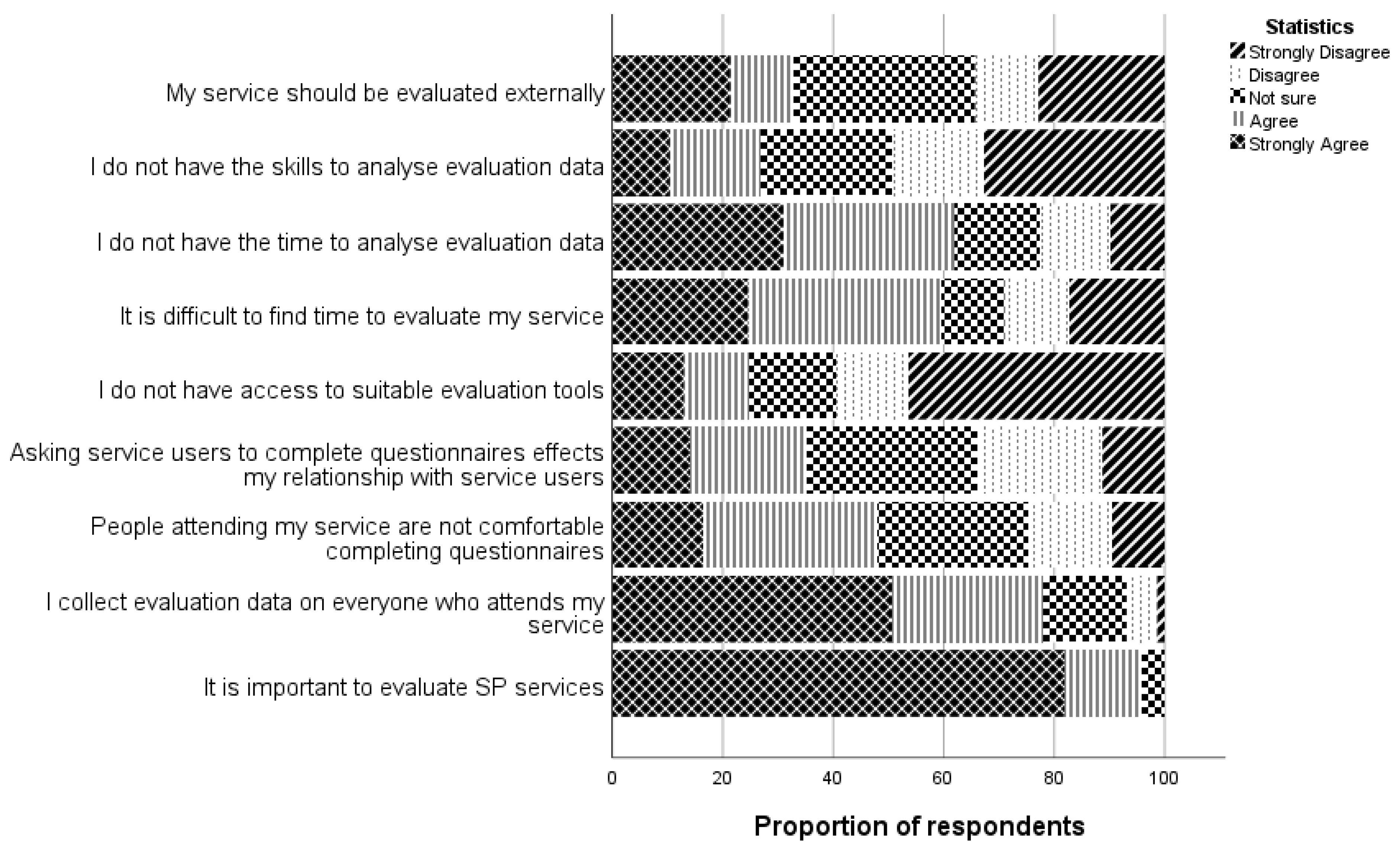
3.4. Respondents’ Experiences of Evaluation
4. Discussion
4.1. Service Profiles
4.2. Approaches to Evaluation
4.3. Barriers and Facilitators to Evaluation
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Calderón-Larrañaga, S.; Milner, Y.; Clinch, M.; Greenhalgh, T.; Finer, S. Tensions and opportunities in social prescribing. Developing a framework to facilitate its implementation and evaluation in primary care: A realist review. BJGP Open 2021, 5, BJGPO.2021.0017. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, S.; Lian, T.; Drake, C.; Moffatt, S.; Wildman, J.; Wildman, J. Intervention components of link worker social prescribing programmes: A scoping review. Health Soc. Care Community 2022, 30, e3761–e3774. [Google Scholar] [CrossRef] [PubMed]
- Husk, K.; Blockley, K.; Lovell, R.; Bethel, A.; Lang, I.; Byng, R.; Garside, R. What approaches to social prescribing work, for whom, and in what circumstances? A realist review. Health Soc. Care Community 2020, 28, 309–324. [Google Scholar] [CrossRef] [PubMed]
- Kimberlee, R. What is social prescribing? Adv. Soc. Sci. Res. J. 2015, 2, 102–110. [Google Scholar] [CrossRef]
- Morse, D.F.; Sandhu, S.; Mulligan, K.; Tierney, S.; Polley, M.; Giurca, B.C.; Slade, S.; Dias, S.; Mahtani, K.R.; Wells, L.; et al. Global developments in social prescribing. BMJ Glob. Health 2022, 7, e008524. [Google Scholar] [CrossRef] [PubMed]
- All Ireland Social Prescribing Network (AISPN). Service Map. 2021. Available online: https://allirelandsocialprescribing.ie/services-map/ (accessed on 9 March 2023).
- Kiely, B.; Croke, A.; O’Shea, M.; Boland, F.; O’Shea, E.; Connolly, D.; Smith, S.M. Effect of social prescribing link workers on health outcomes and costs for adults in primary care and community settings: A systematic review. BMJ Open 2022, 12, e062951. [Google Scholar] [CrossRef] [PubMed]
- Health Service Executive. Building the Capacity for the Evaluation of Social Prescribing: An Evaluability Assessment. Health Service Executive. 2023. Available online: https://www.hse.ie/eng/services/list/4/mental-health-services/connecting-for-life/publications/social-prescribing.pdf (accessed on 13 October 2023).
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [PubMed]
- National Health Service (NHS). Social Prescribing England. 2020. Available online: https://www.england.nhs.uk/personalisedcare/social-prescribing/ (accessed on 16 October 2023).
- Kesmodel, U.S. Cross-sectional studies—What are they good for? Acta Obstet. Gynecol. Scand. 2018, 97, 388–393. [Google Scholar] [CrossRef]
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, 34. [Google Scholar] [CrossRef]
- Erlingsson, C.; Brysiewicz, P. A hands-on guide to doing content analysis. Afr. J. Emerg. Med. 2017, 7, 93–99. [Google Scholar] [CrossRef]
- Haver, A.; Akerjordet, K.; Caputi, P.; Furunes, T.; Magee, C. Measuring mental well-being: A validation of the Short Warwick–Edinburgh Mental Well-Being Scale in Norwegian and Swedish. Scand. J. Public Health 2015, 43, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Sweet, D.; Winter, K.; Neeson, L.; Connolly, P. Assessing the reliability and validity of an outcomes star. J. Child. Serv. 2020, 15, 109–122. [Google Scholar] [CrossRef]
- Social Prescribing Service- Bromley by Bow Centre. Annual Report. 2019. Available online: https://www.bbbc.org.uk (accessed on 15 September 2023).
- Woodall, J.; Trigwell, J.; Bunyan, A.-M.; Raine, G.; Eaton, V.; Davis, J.; Hancock, L.; Cunningham, M.; Wilkinson, S. Understanding the effectiveness and mechanisms of a social prescribing service: A mixed method analysis. BMC Health Serv. Res. 2018, 18, 604. [Google Scholar] [CrossRef]
- Sonke, J.; Manhas, N.; Belden, C.; Morgan-Daniel, J.; Akram, S.; Marjani, S.; Oduntan, O.; Hammond, G.; Martinez, G.; Carroll, G.D.; et al. Social prescribing outcomes: A mapping review of the evidence from 13 countries to identify key common outcomes. Front. Med. 2023, 10, 1266429. [Google Scholar] [CrossRef]
- Eyssen, I.C.; Steultjens, M.P.; Dekker, J.; Terwee, C.B. A Systematic Review of Instruments Assessing Participation: Challenges in Defining Participation. Arch. Phys. Med. Rehabil. 2011, 92, 983–997. [Google Scholar] [CrossRef]
- Mahindru, A.; Patil, P.; Agrawal, V. Role of Physical Activity on Mental Health and Well-Being: A Review. Cureus 2023, 15, e33475. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.; Durstine, L. Physical activity, exercise and chronic diseases: A brief review. Sport Med. Health Sci. 2019, 1, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Tierney, S.; Wong, G.; Roberts, N.; Boylan, A.-M.; Park, S.; Abrams, R.; Reeve, J.; Williams, V.; Mahtani, K.R. Supporting social prescribing in primary care by linking people to local assets: A realist review. BMC Med. 2020, 18, 49. [Google Scholar] [CrossRef]
- Wildman, J.M.; Moffatt, S.; Penn, L.; O’Brien, N.; Steer, M.; Hill, C. Link workers’ perspectives on factors enabling and preventing client engagement with social prescribing. Health Soc. Care Community 2019, 27, 991–998. [Google Scholar] [CrossRef]
- Westlake, D.; Tierney, S.; Wong, G.; Mahtani, K.R. Social prescribing in the NHS—Is it too soon to judge its value? BMJ 2023, 380, 699. [Google Scholar] [CrossRef]
- Elliott, M.; Davies, M.; Davies, J.; Wallace, C. Exploring how and why social prescribing evaluations work: A realist review. BMJ Open 2022, 12, e057009. [Google Scholar] [CrossRef] [PubMed]
- Jolliffe, R.; Seers, H.; Jackson, S.; Caro, E.; Weeks, L.; Polley, M.J. The Responsiveness, Content Validity, and Convergent Validity of the Measure Yourself Concerns and Wellbeing (MYCaW) Patient-Reported Outcome Measure. Integr. Cancer Ther. 2015, 14, 26–34. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n (%) | ||
|---|---|---|
| Location | NI 1 | 42 (50%) |
| ROI 2 | 42 (50%) | |
| Role in SP service | SP Link Worker 3 | 40 (47.1%) |
| SP Coordinator 4 | 22 (25.9%) | |
| Other | 22 (27.0%) | |
| Location of SP service | Community Health Centre | 27 (34.1%) |
| Family Resource Centre | 25 (31.6%) | |
| Partnerships organisations | 12 (15.1%) | |
| Other | 26 (33%) | |
| Source of referrals to SP services | Com MH Service 5 | 69 (82.1%) |
| GP 6 | 67 (79.8%) | |
| Social Worker | 59 (69.4%) | |
| Self-Referral | 57 (67.1%) | |
| Other | 32 (38.1%) | |
| Age (years) of individuals referred to SP | Less than 18 | 12 (14.1%) |
| 19–30 | 74 (87.1%) | |
| 31–65 | 81 (95.3%) | |
| 66+ | 80 (94.1%) | |
| Reasons for referral | Mental Health | 117 |
| Social Health | 104 | |
| Physical Health | 59 | |
| Other | 341 |
| Mental Health | Social Health | Physical Health | Other |
|---|---|---|---|
| Unspecified mental health (n = 32) Anxiety (n = 29) Depression (n = 28) Bereavement (n = 9) | Loneliness (n = 80) Befriending (n = 17) Family Support (n = 5) Relationship breakdown (n = 3) | Chronic disease management (n = 19) Pain management (n = 16) Exercise (n = 14) Nutritional Support (n = 4) Falls prevention (n = 2) | Link to new activities (unspecified) (n = 8) Housing support (n = 5) Education/employment/career advice (n = 3) Financial advice (n = 2) |
| How Often | Approaches Used n (%) | Frequently Used Questionnaires n (%) | ||
|---|---|---|---|---|
| Never/Occasionally n (%) | Always n (%) | |||
| General Health and Well-being | 8/74 (10.8%) | 66/74 (89.2%) | Questionnaire n = 42/60 (70%) | SWEMWBS 1 n = 28/50 (56%) |
| Informal discussion n = 11/60 (18.3%) | Outcome Star n = 13/50 (26%) | |||
| Social Connectedness/Loneliness | 12/75 (16%) | 63/75 (84%) | Questionnaire n = 31/56 (55.4%) | SWEMWBS n = 26/42 (61.9%) |
| Informal discussion n = 19/56 (33.9%) | Outcome Star n = 13/42 (31.0%) | |||
| Participation in Social Activities | 15/76 (19.7%) | 61/76 (80.3%) | Questionnaire n = 21/47 (44.7%) | SWEMWBS n = 11/36 (30.6%) |
| Informal discussion n = 17/47 (36.2%) | Outcome star n = 11/36 (30.6%) | |||
| Stress/Anxiety/Distress | 19/75 (25.3%) | 56/75 (74.7%) | Questionnaire n = 37/53 (43.0%) | SWEMWBS n = 30/45 (66.6%) |
| Informal discussion n= 11/53 (20.7%) | Outcome star n = 10/45 (22.2%) | |||
| Confidence/Self-Esteem | 20/75 (26.6%) | 55/75 (73.4%) | Questionnaire n = 40/59 (67.8%) | SWEMWBS n = 29/47 (61.7%) |
| Informal discussion n = 14/59 (23.7%) | Outcome star n = 12/47 (25.5%) | |||
| Physical Activity levels/Physical activity Health | 23/75 (30.6%) | 52/75 (69.4%) | Informal Discussion n = 20/45 (44.4%) | SWEMWBS n = 9/30 (30.0%) |
| Questionnaire n = 20/45 (44.4%) | Outcome Star n = 8/30 (26.7%) | |||
| PAR-Q 2 n = 4/30 (13.3%) | ||||
| Depression | 25/76 (32.9%) | 51/76 (67.1%) | Questionnaire n = 28/48 (58.3%) | SWEMWBS n = 25/36 (69.5%) |
| Informal discussion n = 15/48 (31.3%) | Outcome Star n = 11/36 (30.6%) | |||
| Change in financial situation | 37/75 (49.3%) | 38/75 (50.7%) | Informal Discussion n = 16/35 (45.7%) | SWEMWBS n = 9/23 (39.1%) |
| Questionnaire n = 11/35 (31.4%) | Outcome star n = 11/23 (47.7%) | |||
| Change in Employment Status | 37/74 (50%) | 37/74 (50.0%) | Questionnaire n = 14/35 (40%) | Outcome star n = 11/24 (45.8%) |
| Informal Discussion n =13/35 (37.1%) | SWEMWBS n = 9/24 (37.5%) | |||
| Questionnaire | Standardised Measures Used in SP Services n = 84 |
|---|---|
| Short Warwick–Edinburgh Mental Well-being Scale (SWEMWEBS) | 38 (45.2%) |
| Outcome Star | 18 (21.4%) |
| Pillars of Positive Health (POPH) | 9 (10.7%) |
| World Health Organisation Well-Being Index (WHO-5) | 8 (9.5%) |
| The Wheel of Life | 4 (4.7%) |
| Physical Activity Readiness Questionnaire (PAR-Q) | 4 (4.7%) |
| Measure Yourself Concerns and Well-being (MYCaW) | 3 (3.5%) |
| General Anxiety Disorder-7 (GAD-7) | 2 (2.3%) |
| Euro QoL 5D * | 2 (2.3%) |
| UCLA Loneliness Scale | 1 (1.2%) |
| Outcomes Related to Service Uptake and Delivery | How Often | Approaches Used to Measure Service-Related Outcomes n (%) | |
|---|---|---|---|
| Never/Occasionally n (%) | Always n (%) | ||
| Number of referrals you received for your service | 13/73 (17.8%) | 59/73 (80.8%) | Digital platform 20/31 (64.5%) |
| Number of individuals referred to your service, but do not attend | 19/73 (26.0%) | 54/73 (74.0%) | Digital 19/28 (67.9%) |
| Record of activities and/or support services accessed by individuals following meetings with LW 1 | 15/73 (20.5%) | 58/73 (79.5%) | Digital 18/34 (52.9%) |
| Type of contact between LW and individuals attending your SP 2 service | 18/76 (23.7%) | 58/76 (76.3%) | Digital 19/37 (51.4%) |
| Number of contacts between LW and individuals attending your SP service | 21/75 (28.0%) | 54/75 (72.0%) | Digital 17/34 (50%) |
| Satisfaction of individuals who attend your service | 36/74 (48.6%) | 38/74 (51.4%) | Questionnaire 11/28 (39.3%) |
| Case studies of individuals who attend your service | 46/73 (67.1%) | 27/73 (36.9%) | Digital 9/19 (47.4%) |
| Satisfaction of HCP and other organisations who refer individuals to your service | 58/73 (79.5%) | 15/73 (20.5%) | Digital 5/14 (35.7%) |
| Category | Sub-Categories | Participant Quotes |
|---|---|---|
| Recommendations for evaluation | National approach | P24 Evaluation tools should be decided nationally so that data can be shared and understood P47 There needs to be consistency in relation to the collection of data and how it is reported on nationally |
| Flexible approaches | P11 Evaluation systems need to be widespread and not a ‘one-size fits all’ as there are as many individual ways of recording evaluations as there are individuals P25 It need to be less generic, direct evaluation tools for different age groups. One size does not fit all | |
| Qualitative evaluation methods | P49 more qual data needs to be captured along with quant data P61 we need qual tools that are suitable for people with low or no literacy where trauma or panic impacts on ability to think and process—we need to allow people to tell their story safely and confidentially which is accepting/appropriate to funders | |
| Timing of evaluation | P81 I find using evaluation tools easier when the client first engages. Social prescribing is not a service with a set timeframe so a relationship can be ongoing and carrying out a ‘post-assessment’ is challenging. Often once a client is engaging and happy, the priority is to support new clients. P81 The relationship may have changed over time, and you can be working with a client more over the phone so it’s less formal and therefore more difficult to implement an exit interview. Also, there may be ongoing challenges meaning the relationship continues in a different vein or with a different focus. | |
| Multiple perspectives | P32 It would be great to record the LWs assessment of the person’s improvement also. Important to record—is the person now more engaged in their communities and do they plan to continue? P86 Feedback from the services/supports/activities referred to will be useful in guiding future referrals. | |
| Co-design evaluation methods | P78 I do feel there is a system of evaluation which should be developed in conjunction with social prescribers | |
| Resources needed | Measurement tools | P47 there needs to be wide access to evaluation tools. P79 They have no formal evaluation measures available to me and no digital system that they will provide. |
| Funding | P61 need to do invest in quality evidence methods | |
| Time to evaluate change in service users | P69 The depth of work is not being measured—some people just need information some people take months to build up trust/This is not being measured. P69 The impact is much more difficult to measure as the outcomes may be long term and may not be obvious or measurable in the short term. This I think needs further thought, and to ask social prescribers to measure real impact in 8 weeks is not achievable and will not give accurate results. | |
| Time for LW to evaluate | P79 Time constraints stops me from being able to evaluate case studies of individuals who attend my service. I work 11 h weekly with a heavy case load and large waiting lists, high number of referrals, and no opportunity to assess needs and evaluate the service properly. P38 Evaluating is very time consuming so this needs to be considered |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Connolly, H.; Delimata, N.; Galway, K.; Kiely, B.; Lawler, M.; Mulholland, J.; O’Grady, M.; Connolly, D. Exploration of Evaluation Practices in Social Prescribing Services in Ireland: A Cross-Sectional Observational Study. Healthcare 2024, 12, 219. https://doi.org/10.3390/healthcare12020219
Connolly H, Delimata N, Galway K, Kiely B, Lawler M, Mulholland J, O’Grady M, Connolly D. Exploration of Evaluation Practices in Social Prescribing Services in Ireland: A Cross-Sectional Observational Study. Healthcare. 2024; 12(2):219. https://doi.org/10.3390/healthcare12020219
Chicago/Turabian StyleConnolly, Hayley, Natalie Delimata, Karen Galway, Bridget Kiely, Margaret Lawler, Jill Mulholland, Megan O’Grady, and Deirdre Connolly. 2024. "Exploration of Evaluation Practices in Social Prescribing Services in Ireland: A Cross-Sectional Observational Study" Healthcare 12, no. 2: 219. https://doi.org/10.3390/healthcare12020219