
Microbes and Mental Illness: Past, Present, and Future


1
Rutgers-Robert Wood Johnson Medical School, Piscataway, NJ 08854, USA
2
Hackensack Meridian School of Medicine, Nutey, NJ 07110, USA
3
Invisible International, Cambridge, MA 02138, USA
4
Medical Arts Psychotherapy Associates P.A., Summit, NJ 07901, USA
*
Author to whom correspondence should be addressed.
Healthcare 2024, 12(1), 83; https://doi.org/10.3390/healthcare12010083
Submission received: 31 October 2023
/
Revised: 30 November 2023
/
Accepted: 6 December 2023
/
Published: 29 December 2023
Abstract
:A review of the association between microbes and mental illness is performed, including the history, relevant definitions, infectious agents associated with mental illnesses, complex interactive infections, total load theory, pathophysiology, psychoimmunology, psychoneuroimmunology, clinical presentations, early-life infections, clinical assessment, and treatment. Perspectives on the etiology of mental illness have evolved from demonic possession toward multisystem biologically based models that include gene expression, environmental triggers, immune mediators, and infectious diseases. Microbes are associated with a number of mental disorders, including autism, schizophrenia, bipolar disorder, depressive disorders, and anxiety disorders, as well as suicidality and aggressive or violent behaviors. Specific microbes that have been associated or potentially associated with at least one of these conditions include Aspergillus, Babesia, Bartonella, Borna disease virus, Borrelia burgdorferi (Lyme disease), Candida, Chlamydia, coronaviruses (e.g., SARS-CoV-2), Cryptococcus neoformans, cytomegalovirus, enteroviruses, Epstein–Barr virus, hepatitis C, herpes simplex virus, human endogenous retroviruses, human immunodeficiency virus, human herpesvirus-6 (HHV-6), human T-cell lymphotropic virus type 1, influenza viruses, measles virus, Mycoplasma, Plasmodium, rubella virus, Group A Streptococcus (PANDAS), Taenia solium, Toxoplasma gondii, Treponema pallidum (syphilis), Trypanosoma, and West Nile virus. Recognition of the microbe and mental illness association with the development of greater interdisciplinary research, education, and treatment options may prevent and reduce mental illness morbidity, disability, and mortality.
Keywords:
aggression; anxiety; autism; bipolar; depression; immune; Lyme borreliosis; schizophrenia; suicide; Tuskegee1. Introduction
As human beings, we are interdependent upon both the microbiota within us and those present within our environment. In 2007, the United States National Institutes of Health Human Microbiome Project was established to study the microbial communities that live in and on our bodies, with the goal of elucidating their role in human health and disease [1]. With advancing technology, there is greater recognition that infectious diseases contribute to not only acute but also chronic illness, both physical and mental. Research from the United States Centers for Disease Control and Prevention (CDC) has recognized “that non-communicable chronic diseases can stem from a variety of infectious agents” [2]. Identifying these relationships between pathogens and illnesses can significantly impact human health, both acutely and chronically. Knowledge of these processes creates opportunities for prevention or early invention. The end goal is to reduce or eliminate the impact of illness, especially chronic disease. Scientific evidence demonstrates more support for the role of infectious agents in cancers, immune-mediated syndromes, neurodevelopmental disorders, and other chronic conditions [2,3]. To benefit from this research, clinicians, public health practitioners, and policymakers need to recognize that many chronic diseases may have infectious origins [2].
It is recognized that some infectious diseases can play a significant role in the etiology of neuropsychiatric disturbances. There is little debate that syphilis can cause the development of symptoms of various mental illnesses [4]. Some suspect and others recognize that the novel SARS-CoV-2 virus that is responsible for COVID-19 can contribute to mental illnesses [5]. There exists some uncertainty as to whether some other infections, such as Lyme borreliosis/tick-borne disease, are associated with neuropsychiatric disorders. However, there are over 500 journal articles supporting this association [6,7,8,9,10,11,12,13] (Supplementary S1).
A number of barriers exist that impede medical progress. The obstacles include the following: (1) most psychiatrists have limited knowledge of infectious diseases, (2) most infectious disease specialists have limited awareness of psychiatric diseases, and (3) most physicians have a very limited understanding of psychoneuroimmunology. There are also multiple controversies. How significant are microbes vs. other contributors to the development of mental illness? Etiologically, how important are prior infections vs. current, latent, or active stealth infections? How do infections by multiple pathogens interact with the disease and affect the clinical presentation? How reliable is the present state of laboratory testing in determining the presence or absence of a contributory pathogen? What are the underlying pathophysiological processes involved? Achieving a better understanding of the nature of the association and the possible contribution of infections to the development of mental illness potentially opens up new opportunities for prevention and treatment.
2. Materials and Methods
The review identified and evaluated the literature from electronic databases, including PubMed and Google Scholar, for relevant information on the topics previously identified. The references discovered in searches were also reviewed for additional relevant references. In addition, references were also drawn from the libraries previously accumulated by the three authors. The inclusion criteria were peer-reviewed articles taken from all time periods, all articles except editorials, without age or gender subject restriction. A few review articles were included. Most of the references included were listed on PubMed. The included references were fully read by at least one author. A formal PRISMA analysis of the literature was considered but was not performed since there was an overwhelming number of citations related to microbes and mental illness.
The review of the association between microbes and mental illness was performed in multiple separate stages. As a starting point, we examined the literature tracing the evolution of thinking on the etiology of mental illness. Definitions of relevant terms were then clarified. Next, disease models to understand the causes of diseases were defined. A list of infectious agents with potential psychiatric manifestations was developed (Table 1). Then, a review of examples of mental conditions potentially associated with infections was performed. This review included the five mental illnesses with the greatest psychiatric disability (autism spectrum disorders, schizophrenia, bipolar disorders, depressive disorders, and anxiety disorders) [14] and two behaviors of particular concern in psychiatric patients (suicidality and aggressive or violent behavior) (Table 2). Next, the disease models, pathophysiology, and clinical considerations were summarized. This information was then a foundation to review five different infectious diseases associated with mental illness: syphilis; toxoplasmosis; COVID-19; Lyme borreliosis and associated diseases; and group A streptococcal infections and pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections/pediatric acute-onset neuropsychiatric syndrome (PANDAS/PANS). Syphilis has historical significance. The other illnesses have been the subject of more recent interest.
3. Results
3.1. Overview
What is the evidence for an association between infections and mental illness? Addressing this question requires a multifaceted approach. We shall utilize information from different perspectives to address this question. This includes historical perspectives, definitions of relevant terms, disease models, awareness of infections associated with mental illnesses, examples of mental conditions potentially associated with infections, pathophysiology, and clinical considerations. This information shall then be applied to a more detailed analysis of five quite different infectious diseases associated with mental illnesses.
3.1.1. History of Mental Illness
The earliest evidence of the recognition of mental illness is the discovery of trephination in skulls dating back thousands of years. Trephination is the removal of a small area of the skull using an auger, bore, or saw. This practice was likely to relieve headaches or mental illness based upon the belief in demonic possession [284]. References to what appear to be mood disorders are noted in the writings of ancient Greco-Roman physicians. The oldest written description of a schizophreniform type of illness was written in the Ebers Papyrus from the time of the Egyptian Pharaohs. The Ebers Papyrus is a compendium of ancient Egyptian Medical Papers listing treatments for multiple illnesses. The description was found in a section called Book of the Heart [285]. Ancient Egyptians believed that the mind and the heart were similar to each other. To the Egyptians, “Physical illnesses were regarded as symptoms of the heart and the uterus and originating from the blood vessels or from purulence, fecal matter, a poison or demons” [285].
In the first century, Aretaeus of Cappadocia was the first to determine that there was an association between the brain and the two disparate mood states. Plato spoke of two types of mania, “One involving a mental strain that arises from a bodily cause of origin, the other divine or inspired”. Both Hippocrates and Aretaeus tried to prove that, in some cases, melancholia and mania were of biologic origin, not just a mental response as a reaction to situations. When it came to hallucinations, the Hippocratic doctors recognized it as a sign of a medical problem, while most common people still thought it was due to the gods [286].
A commonly held belief was that mental illness was the result of demonic possession, witchcraft, or an angry god [287]. Based upon this belief, witch-hunting resulted in more than 100,000 presumed “witches” being burned at the stake. This practice did not decline until the 17th and 18th centuries [288,289]. There is speculation that the witch trials in Salem, Massachusetts, in the 1600s may have been a response to an epidemic of autoimmune encephalitis in which individuals had thrashing fits with bizarre behavior, possibly caused by an autoimmune process [290]. Hypothesized causes of the bizarre behavior include encephalitis lethargica, Huntington’s chorea, a rye fungus causing anti-N-methyl-D-aspartate receptor encephalitis, and Lyme disease [289,291,292]. For centuries, based upon the belief in supernatural forces and demonic possession, the mentally ill were treated very poorly, subjected to physical restraints and solitary confinement in asylums.
In the first part of the 1800s, Wilhelm Griesinger, a German psychiatrist and neurologist, was an active proponent of the theory that “All mental illness is disease of the brain” [293]. From this vantage point, mental disorders were placed more clearly in the biological domain of medicine and no longer in the realm of the mystical or supernatural. Griesinger’s strong belief in this postulate led him to become an advocate for better and more humane treatment of those who were mentally ill in asylums. Philippe Pinel and Dorothea Dix further advanced the concept of humane treatment for the mentally ill in the 1800s [294].
In 1887, the German psychiatrist Emile Kraeplin first described what he called “dementia praecox”, which he believed was a disease of the human brain. In 1908, Eugen Bleuler, a Swiss psychiatrist, changed the name to schizophrenia. Furthering this medicalization of psychiatry in the early 1900s was the theoretical belief that a focal infection was the source of mental illness or brain disorders.
An American psychiatrist, Henry Cotton, who had undergone some psychiatric training in Europe and was a protégé of the renowned psychiatrist Adolf Meyer at John Hopkins, became a strong advocate of this theory [295]. His basic belief was that eliminating the source of infection was the only way to cure an individual’s mental illness. Cotton served as the medical director and superintendent of the New Jersey State Hospital in Trenton, N.J., from 1907 to 1930. He went on to teach that chronic mental illness was the result of ongoing, latent, and somewhat stealth or unrecognized infections. For him, the proper treatment of a mentally ill individual would be the removal of the initiating and offending infectious site. This often led to the removal of the affected organ. In the name of treatment, teeth were pulled, and the uterus or parts of the gastrointestinal tract or other body parts were surgically extracted. Unfortunately, what initially appeared to be a promising concept lacked sufficient evidence and resulted in the maiming and disfigurement of many individuals. In the end, it became clear that this was a horrific treatment intervention. Although the concept that biologic influences, including infections, were at play in mental disorders indicated thinking in the right direction, Dr. Cotton’s interpretation was disfiguring and barbaric.
Sigmund Freud recognized the value of acquiring insight into and an understanding of psychodynamic development to better explain motivation. Anna Freud, Erik Erikson, and others further expanded on defense mechanisms and developmental theories.
In the 1950s, “the catecholamine hypothesis of affective disorders” emerged. This theory attributed mood disorders to deficits or excesses of certain catecholamines as the physiologic cause of mental illness [296].
In the late 1970s, the biopsychosocial model of psychiatric illness was developed by Drs. George Engel and John Romano. This approach recognized that there was a combination of biological, psychological, and social contributors to mental illness.
Understanding the inner workings of the mind and the brain has always been challenging. For its weight, nothing is more complex than the human brain. For many years, the living brain was seen as a mysterious black box that could not be understood. The development of brain imaging technology with computed tomography, magnetic resonance imaging, positron emission technology, single-photon emission technology, and other neuroscience advances allowed the imaging of the anatomy and physiology of the living brain. These techniques improved the capacity to better understand the complexities and brain circuits involved in mental functioning.
Advances in gene technology hastened interest in the genetic causes of mental illnesses. Darwinian or evolutionary medicine recognized that most illness is not caused by disease genes but instead by susceptibility genes interacting with environmental contributors. The environmental contributors include competing organisms, such as microbes [297].
With a greater understanding of genetics came the recognition that the interaction between genes and health is even more complex than previously realized. This awareness has resulted in the recognition of the importance of epigenetic factors. The field of epigenetics, as defined by the CDC, refers to “the study of how your behaviors and environment can cause changes that affect the way your genes work. Unlike genetic changes, epigenetic changes are reversible and do not change your DNA sequence, but they can change how your body reads a DNA sequence” [298]. Focusing only on genes, without attention to epigenetic factors, will only give us part of the genetic picture when studying mental illness. Environmental contributors also play an important role [299].
3.1.2. History of Associating Microbes and Mental Illness
Microbiology began with the lens. It was originally used for millennia for other purposes. The machine to manufacture precision lenses was designed by Leonardo Da Vinci [300,301]. Combining two lenses resulted in the microscope that created the technology to observe both microorganisms and human cells. Hooke and Leeuwenhoek observed microorganisms in the late 1600s [302].
Rudolph Virchow used the microscope to directly visualize anatomical changes in cells and groups of cells when a patient became ill. He proposed that when ill, the whole organism does not get sick. Instead, it is only particular cells or groups of cells that change, thus opening up the new field of cellular biology. The use of a microscope now added the ability to utilize direct visual anatomical changes for identifying diseases. No longer did illnesses need to be diagnosed by clinical symptoms alone. Virchow also coined the term “zoonosis”, indicating the connection between human and animal health, which could be considered the foundation of the concept of One Health or One Medicine [303].
The highly significant work of Robert Koch, Friedrich Loeffler, and Louis Pasteur in the late 1800s led to the discovery that microbes (germs) could cause disease [304]. The science of medicine changed dramatically when the germ theory of disease was proven. This awareness opened up new avenues for exploration. These advances dramatically improved the science of medicine in the 1800s.
As previously noted, theories on the origins of mental illness remained a mix of science, spirituality, and myth for centuries. An early attempt utilizing germ theory in the field of mental health is exemplified in the following report:
“In 1896 Scientific American published an editorial entitled ‘Is Insanity Due to a Microbe?’ Two doctors described how they had injected cerebrospinal fluid of mentally ill patients into rabbits, which later got sick. Subsequently, the rabbits showed behavioral issues. The authors concluded that ‘certain forms of insanity’ could be caused by infectious agents, ‘similar to typhoid, diphtheria and others.”[305]
Although this early work could explain some diseases, the etiology of mental illnesses remained somewhat puzzling. The recognition of a potential connection between infections and mental symptoms may have been partially based on ongoing observations of mental changes, e.g., psychoses, that occurred with some bacterial illnesses. Throughout the 1800s and well into the 1900s, general paralysis of the insane, also known as general paresis and caused by neurosyphilis, was a significant degenerative mental illness known to psychiatry. In 1913, Hideyo Noguchi found traces of Treponema pallidum (the bacteria that causes syphilis) in the brains of deceased general paresis patients who had been hospitalized for mental illnesses at the Central Islip State Hospital for the Insane [20]. In 1943, penicillin became the main treatment for syphilis [306].
After penicillin became an effective treatment for syphilis, there was little attention to the association between infections and mental illness for many years. In the early 1990s, Fallon began writing about the association between Lyme disease and mental illness [13]. In 1996, the Stanley Laboratory of the Johns Hopkins University School of Medicine was founded as a result of the efforts of Robert Yolken and E Fuller Torrey to elucidate and promote research and training on the role of infection and immunity in the etiology of schizophrenia and bipolar disorders. Work at the Stanley Center, other collaborating centers (Karolinska Institute, University of Heidelberg, University of Cologne, University of Pittsburgh, Centre for Register-Based Research in Denmark, Sheppard Pratt, Washington University, University of Cambridge, University of Maryland, Harvard School of Public Health, etc.), and other projects funded by it has resulted in extensive research and many peer-reviewed publications. This improved the understanding of the association between microbes and mental illness [307]. The field has continued to progress since then. Presently, there are a vast number of articles in the peer-reviewed literature addressing different facets of the association between microbes and mental illness [308].
3.2. Definitions of Relevant Terms
3.2.1. Microbes and Related Terms
A microbe has traditionally been defined as a very small, living thing that can be seen only with the use of a microscope. There are a number of related terms. The human microbiota is the full array of microorganisms that live on and in humans. The human microbiome is the combined genetic material of the microorganisms that live in and on humans. The pathobiome is the set of human-host-associated organisms (crucially encompassing prokaryotes, eukaryotes, and viruses) associated with reduced (or potentially reduced) health status as a result of interactions between members of that set and the human host.
3.2.2. Health
A generally accepted definition of health is the ability to adapt and to self-manage in the face of social, physical, and emotional challenges [309].
3.2.3. Illness
3.2.4. Mental Health
According to the American Psychiatric Association, mental health is a state of mind characterized by emotional well-being, good behavioral adjustment, relative freedom from anxiety and disabling symptoms, and a capacity to establish constructive relationships and cope with the ordinary demands and stresses of life [312]. The World Health Organization defines mental health as “a state of well-being in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community” [313]. In summary, mental health occurs when mental functioning (cognition, emotions, vegetative functioning) reflects the individual’s life situation and facilitates adaptation with the capacity to experience well-being, pleasure, fulfilling relationships, and productive activities; the ability to recognize and contend with adversity; and the mental flexibility to adapt to change.
3.2.5. Mental Illness
The American Psychiatric Association defines a mental disorder as a syndrome characterized by a clinically significant disturbance in an individual’s cognition, emotion regulation, or behavior that reflects a dysfunction in the psychological, biological, or developmental processes underlying mental functioning [312]. In a state of mental illness, mental functioning does not reflect the life situation, and there is an impairment of adaptive capabilities; an impaired capacity to experience well-being, pleasure, fulfilling relationships, and/or productive activities; a diminished ability to recognize and contend with adversity; and/or restricted mental flexibility to adapt to change.
3.2.6. Acute vs. Chronic Illness
Acute illnesses generally develop suddenly and last a short time, often only a few days or weeks. Chronic conditions, by contrast, are long-developing and may worsen over an extended period of time—months to years. Chronic diseases more often can be controlled but not cured. Some define chronic diseases as lasting at least 3 or 6 months. Chronic diseases are defined broadly by the CDC as “conditions that last 1 year or more and require ongoing medical attention or limit activities of daily living or both” [314]. Post-acute is a term that has more recently been used.
3.3. Models for Understanding Disease
Illness is caused by an underlying disease process. To better understand the underlying disease process, a variety of approaches can be used.
3.3.1. A Multisystem Approach to Understanding the Cause of Disease
A multisystem approach is useful when analyzing complex issues, such as the cause of disease. It allows for a complex model with many contributors. All systems are interconnected and affect other systems to varying degrees. Furthermore, they are constantly changing and in dynamic balance with each other. Time is a significant dimension, and different effects occur over time. Systems have evolved over the dimension of time. The combination of the systems and evolutionary approaches allows us to organize current information in a much more efficient manner [315].
3.3.2. An Evolutionary or Darwinian Approach to Understanding the Cause of Disease
An evolutionary or Darwinian approach applies the principles of evolutionary biology to help explain problems in medicine and public health and prevent human disease. It explains how disease occurs from the perspective of evolution. From this perspective, disease can be the result of genetic vulnerabilities from the unique path of evolution, design compromises, and competing organisms. Competing organisms can include microbes. “Core principles drawn from evolutionary biology include selection, drift, plasticity, mismatch, cultural practices, trade-offs, life history traits, antagonistic pleiotropy, heterozygote advantage, constraints, biologic defenses, co-evolution (i.e., microbiome), adaptation/maladaptation, novel environments, and the genome-phenome relationship” [299,316].
3.3.3. An Organismal Approach to Understanding Disease
Disease results from an interaction of host vulnerabilities and environmental contributors. Host vulnerabilities may be genetic or otherwise, and the environmental contributors may be of infectious or non-infectious origin. While acknowledging that there are many non-infectious contributors associated with mental illness, this article specifically focuses upon the infectious contributors. The infectious and/or non-infectious contributors may then provoke immune activity that can result in the impairment of adaptive mechanisms, resulting in disease progression [139,317,318,319,320,321,322,323,324,325] (Figure 1).
3.3.4. Infections Associated with Mental Illness
A myriad of journal articles address different aspects of the possible connection between infections and mental illnesses. Some mental illness symptoms, such as those associated with delirium, are generally, although not exclusively, associated with the acute phase of infection [326,327]. Viruses and vector-borne diseases have drawn some of the greatest attention. There are at least 320,000 different species of viruses in mammals [328]. Vector-borne diseases are mostly zoonotic, i.e., diseases that are transmitted between species, from animals to humans, or from humans to animals. It appears that vector-borne diseases are increasing, and possible explanations include heightened awareness, climate change, changing ecosystems, globalization, human population growth, and toxic warfare environments [329,330].
3.3.5. What Mental Illnesses Are Associated with Specific Microbes?
A systematic review and meta-analysis was previously conducted on mental illnesses associated with SARS-CoV-2 infection [331], and a prior PRISMA analysis was performed on mental illnesses associated with Lyme borreliosis [7].
A search was conducted for specific microbes associated with five mental illnesses with the greatest psychiatric disability and two behaviors of particular concern in psychiatric patients (Table 2).
The microbes identified with these conditions collectively included Aspergillus, Babesia, Bartonella, relapsing fever group Borrelia, Borrelia burgdorferi, Borna disease virus, Candida, Chlamydia, SARS-CoV-2 (COVID-19) and other coronaviruses, cytomegalovirus, enterovirus, Epstein–Barr virus, hepatitis C virus, herpes simplex virus, human endogenous retroviruses, human herpesvirus-6, human immunodeficiency virus (HIV), human T-cell lymphotropic virus type 1 (HTLV-1), influenza viruses, measles virus, Mycoplasma, Plasmodium, rubella virus (congenital), Shigella, group A Streptococcus, Taenia solium, Toxoplasma gondii, Treponema pallidum (syphilis), varicella zoster virus, and changes in intestinal microbiota composition.
3.3.6. Disease Models
- Acute vs. chronic infections
As noted earlier, the CDC defines a chronic illness as lasting one year or more [314]. The nomenclature regarding acute vs. chronic infections and acute vs. chronic manifestations of infectious diseases can be confusing. Some acute infections can be “hit and run” and cause residual injury that leads to dysfunction and chronic disease, with the illness continuing and sometimes progressing long after the infection is clearly eradicated. Developing mitral valve stenosis following a streptococcal infection is an example of this. On the other hand, infections can also be recognized as being chronic with ongoing symptoms and often disease progression as the pathogen persists. An example of this is seen with syphilis. Not all infections are easily placed into these two categories. Some infections may be acute, then be latent, and then be reactivated at a later time. An example of this is varicella zoster (chicken pox), which can be reactivated as shingles decades later when the patient is in an immunocompromised state. Some infections may suppress and/or evade the immune system, which results in difficulty detecting them by commonly used immune-based testing. These immune-evasive, persistent infections can cause symptoms that are chronically progressive or chronically relapsing and remitting. An example is Borrelia burgdorferi [332,333,334,335,336,337]. Persistent or progressive symptoms after commonly used treatment for Borrelia burgdorferi infection are viewed by some researchers as caused by a self-perpetuating immune process in the absence of ongoing active infection [338].
- Complex interactive infections
Koch’s initial view of infectious disease is that many human diseases are caused by microbes that exert their effects independently of other microbes, environmental factors, or genes. However, most common human diseases are caused by the interaction of environmental insults and susceptibility genes [339]. Many of the susceptibility genes are diverse determinants of human responses to environmental factors, e.g., infection.
Informative laboratory methods for complex disorders must address both genetic and environmental factors [340].
Some infection-associated symptom presentations are not the result of single pathogens but instead the result of complex interactive infections with multiple infectious agents. These infections could be compared to a foxhunt, in which three different species (humans, horses, and dogs) participate. In this case, the foxhunt would have a very different effect than if only one species were involved. Human immunodeficiency virus infection and acquired immune deficiency syndrome (HIV/AIDS) is one example in which a pathogen (virus) causes immunodeficiency, allowing other microbes to become more pathogenic to the host. This pattern can also be seen with tick-borne diseases, as multiple tick-borne pathogens such as Borrelia, Babesia, Anaplasma, Ehrlichia, other Rickettsia, Nematodes, etc., may be present at the same time [341]. Additional unidentified, non-testable pathogens may also be contributory. The Borrelia bacterium has the capacity to cause immunosuppression and immune evasion [332,333,334,335,336,337]. This can result in previously asymptomatic latent infections becoming symptomatic. These previously acquired latent infections may not have been transmitted via tick bites and may include viruses and Bartonella and Mycoplasma species [342,343,344]. In addition, tick-borne polymicrobial coinfections can have an interactive effect upon the Borrelia infection [345,346,347]. SARS-CoV-2 viral infections have also been associated with complex interactive infections. There is anecdotal evidence that COVID-19 infections have resulted in the re-activation of latent Borrelia infections [348]. Increased levels of Borrelia-specific IgG antibodies strongly correlated with SARS-CoV-2 viral severity and the risk of hospitalization [349]. The human microbiota has been implicated in the development of a variety of mental illnesses, including Alzheimer’s disease, attention-deficit/hyperactivity disorder, anorexia nervosa, autism spectrum disorder, bipolar disorder, major depressive disorder, schizophrenia, and substance use disorders [350]. The human gut microbiome is recognized to have a significant impact upon both health and disease, as well as human metabolism, nutrition, physiology, and immune functioning. An altered gut microbiome is associated with different disease states [138,351]. The human microbiome is not just located in the gut. It can also be located in other parts of the body [350]. Some of the human microbiota can be located deep in connective tissue, where they may be protected from the immune system and attempts at antibiotic treatment [352,353,354].
When there is a complex interactive infection, it is sometimes possible to say that 1 + 1 does not = 2, but instead, 1 + 1 = 11.
- Total load theory
Microbes may also interact with other non-infectious environmental contributors. The initial foundation of this view is based upon the disease triangle, which is a conceptual model showing the interactions between the environment, the host, and an infectious (or abiotic) agent [355]. This concept is addressed in the total load theory. Here, the focus is on how the presence of multiple stressors can result in an increasing number of developmental delays, cognitive problems, behavioral and emotional issues, and other impairments that have been seen in children in recent years. The approach views groups of symptoms as being the result of reaching a tipping point where development is stressed beyond the capacity for healthy adaptation. At that point, the youth shows signs of overload. This state is then manifested as attentional difficulties, developmental delays, mood issues, autoimmune problems, failure to thrive, repeated ear infections, etc. Some of the elements that can lead to developmental issues include birth trauma, pregnancy complications, nutritional deficiencies, frequent ear infections, etc. [356].
3.4. Pathophysiology
3.4.1. Is Trauma from Infection or from the Host’s Immune Reaction to the Infection?
Symptoms associated with infectious disease are a result of both the direct effects of the pathogen upon the host and the indirect effects caused by host immune activation. In an acute infection, the early inflammatory (innate immune) response evolves into a humoral (adaptive immune) response. In a chronic infection, there may instead be a persistence of the inflammatory state without effective adaptive immunity, and sometimes with an autoimmune response. This interaction between pathogen and host contributors results in trauma to the host. Microbial contributors to pathophysiology include toxin release, cell penetration, the effects of bacterial lipoproteins, and the incorporation of pathogen genes into the host genome. Host response contributors can include cytokine release, inflammation, inflammation-causing metabolic changes, the effects of bacterial lipoproteins and other pathogen-associated molecular patterns (PAMPs) such as toll-like receptor signaling, the interaction of heat shock proteins with the immune system, oxidative stress, the action of nitric oxide, other cellular responses, and autoimmune reactions [9,12,357,358,359]. Oxidative stress and changes in nitric oxide are also well recognized as being a part of the stress response and the pathogenesis of depression and other mental illnesses [360,361,362].
In addition, infections outside the central nervous system (CNS) can have immune and toxic effects upon the CNS, with molecular mimicry leading to autoantibody formation and cellular immune responses against host neuronal structures, oxidative stress, glutamate excitotoxicity, changes in homocysteine metabolism, mitochondrial dysfunction, and altered metabolism of tryptophan with decreased production of the neurotransmitter serotonin and increased production of neurotoxic and excitotoxic quinolinic acid and kynurenine metabolites [363,364,365,366,367].
The glymphatic system is important in healthy brain functioning and the prevention of the accumulation of neurotoxic cellular waste products [368,369]. A common neuropsychiatric symptom with a microbial infection is some form of insomnia [370]. During sleep, the glymphatic system expands, and our brain contracts as our immune system attempts to eliminate waste and cleanse itself [371]. If a bacterial toxin released by living organisms or perhaps dead remnants of microbes is not cleared, destructive secretions or ongoing immune stimulation can result in neuroinflammation and neural degeneration. This then has the potential to contribute to cognitive, behavioral, and emotional difficulties.
These pathophysiological processes are hypothesized to result in neuropsychiatric symptoms [12,364,365,366,372,373,374,375]. Bacterial infections are associated with many autoimmune diseases involving chronic inflammation and demyelination [376]. The pathophysiology of how these mechanisms impact the brain is addressed in the field of psychoneuroimmunology [377].
3.4.2. Psychoneuroimmunology or Psychoimmunology
Psychoneuroimmunology (formerly known as psychoimmunology) is the study of the connections between the brain and the immune system. There are basically two major communication networks in the brain—the neurotransmitter system and the immune system. Although the blood–brain barrier is a barrier to some things, it is not an absolute barrier to the immune system. Immune activity in the body releases cytokines, chemokines, antibodies, and other substances that impact immune activity in the brain [378,379].
Infections can have several biochemical effects. One of the most significant effects relevant to mental illness is the effect of inflammation upon the kynurenine pathway. This is a pathway that converts tryptophan into serotonin and melatonin. Chronic infections that do not result in adaptive immunity can instead provoke persistent inflammation. When the brain is exposed to an inflammatory state, there is an increase in an enzyme, indoleamine 2,3-dioxygenase (IDO), that shifts the conversion of tryptophan away from serotonin, melatonin, and kynurenic acid (a neuroprotective compound) and instead pushes the conversion to quinolinic acid, which is a neurotoxin and an N-methyl-D-aspartate (NMDA) agonist [380]. Therefore, ongoing chronic inflammation switches the brain from making necessary neurotransmitters, neurohormones, and neuroprotective substances toward self-destructive activity.
Infections in the body can therefore have immune-mediated effects upon the brain through cytokine and biochemical effects. These changes can result in the dysfunction of limbic and paralimbic brain circuits, impairing emotional functioning and contributing to psychiatric symptoms and illnesses [381,382,383,384,385,386,387].
3.4.3. Clinical Presentation Variability
It is clear from clinical observations of all infectious diseases that the same infection can have a very different presentation in different individuals. This is the result of a combination of different host and pathogen considerations. There are many genetic and other susceptibility and resistance contributors. Microbial variables can include the load of organisms, pathogen strain variability, and coinfections. Host variables include age, genetic, and other susceptibilities.
3.4.4. Infections Early in Life with Later Consequences
Accumulating evidence supports the concept that infections early in life may play a role in the later development of mental disorders. Infections with herpes simplex virus, cytomegalovirus, rubella, and Toxoplasma gondii during the prenatal period are examples of infections that can result in fetal neurodevelopmental abnormalities. These can include structural abnormalities, such as hypoplasia of different areas of the brain, as well as functional problems. The resultant cerebral dysfunction can manifest as behavioral issues, learning problems, autistic spectrum disorders, or mental retardation [9,105].
One population-based cohort study utilizing a large, well-documented Australian database looked at the relationship between early exposure to infection between birth and 4 years and the subsequent development of mental disorders in children aged 5–13 years. The authors found that there was a positive correlation between the rates of childhood mental disorders and infection in the first four years of life. The authors found a moderate association of infection during this time period with autistic spectrum disorder and other developmental disorders, as well as externalizing disorders. In addition, there was a smaller but significant association with internalizing disorders [388].
A review of a nationwide Danish register-based cohort of over one million children born between 1995 and 2012 attempted to determine whether there was any association between hospitalization for infection and the later development of mental illness. The investigators found that youths who were medically hospitalized with infectious illnesses have an 84% increased risk of later developing a mental disorder. The most common mental disorders found included schizophrenia, obsessive–compulsive disorder, tics, attention-deficit hyperactivity disorder, oppositional defiant behavior, conduct disorder, personality and behavior disorders, autism, and mental retardation [389].
In another study, children with autism were found to have substantially greater odds of neonatal and early childhood infections when compared to children with other developmental disorders and healthy controls [136].
In summary, there is increasing evidence that the impact of infections early in life may be an important contributor to the later development of a mental illness. The various mechanisms by which this occurs require further study.
3.5. Clinical Considerations: Assessment
The standard of care in medicine has always been the detailed clinical evaluation. Like other illnesses, the search for the diagnosis and cause of a condition may be initiated by using a screening assessment followed by a thorough history, a review of systems, a comprehensive psychiatric clinical exam, a mental status exam, a neurological exam, and a physical exam relevant to the patient’s complaints. Laboratory or other testing may be ordered based upon the clinical assessment. The diagnosis and the cause of the condition are determined based on a knowledge of the medical literature, clinical judgment, pattern recognition, and a knowledgeable interpretation of all clinical findings [10,390].
3.5.1. Clinical Assessment
The nature of the clinical assessment to determine whether microbes may be causing mental illness is an emerging field. Since infections that contribute to mental illness often cause multisystem illness, a comprehensive multisystem assessment can be helpful in determining the diagnosis and the pathophysiology. It can be challenging to differentiate between psychosomatic, somatopsychic, and multisystem illnesses and medical uncertainty [391]. Two assessments were previously developed for Lyme disease [392,393]. The General Symptom Questionnaire (GSQ-30) was developed and validated to fill the need for a brief patient-reported measure of multisystem symptom burden, and it can be useful in both clinical and research settings [394]. A multisystem assessment has been developed for Lyme borreliosis with a particular emphasis upon neuropsychiatric symptoms, which could be adapted for the assessment of any infection(s) causing mental illness. This assessment is readily available and includes screening questions, three clinical assessment forms (24-item, 61-item, full assessment), and a coinfection screen [10] (Supplementary S2 and S3).
3.5.2. Laboratory and Other Diagnostic Testing
In addition to a thorough history and physical exam, a number of diagnostic tools can assist the assessment. This includes laboratory testing, structural and functional brain imaging, and neuropsychological testing. The sensitivity and specificity of laboratory testing of body fluids (blood, cerebrospinal fluid, urine) and tissue for the myriad of microbes that are associated with mental illness vary over a wide spectrum. Some are generally considered very accurate and extremely helpful in determining the presence or absence of a pathogen. On the other hand, laboratory assays are presently available only for some microbes, and their interpretative criteria have significant limitations. While serologic testing is commonly used for the lab diagnosis of microbes associated with mental illness, the detection of an antibody response to a pathogen can provide evidence of past exposure and infection but does not necessarily indicate an active, ongoing infection. At the same time, the presence of an infection does not alone prove that an infectious agent caused or contributed to any given psychiatric symptom. Psychiatric and other late-stage manifestations of an infection are more likely to occur when an infection is not adequately diagnosed and/or treated in the earlier stages of infection. A common error contributing to a lack of diagnosis or late diagnosis is confusing public health surveillance criteria with diagnostic criteria. As emphasized by the US CDC, “surveillance definitions are designed to study and identify trends in a population… Alternatively, clinical diagnoses are patient specific. Unlike surveillance definitions, ALL available diagnostic data are considered in a clinical diagnosis, including additional clinical, epidemiological and laboratory data not used for national health system surveillance. Therefore, a clinical diagnosis may be made even when a surveillance definition may not be met and vice versa is also true. Failure to meet a surveillance definition should never impede or override clinical judgment during diagnosis, management, or treatment of patents [sic]” [395]. Future testing may be more dependent upon metabolomics, the measuring and assessing of metabolites to provide specific metabolic profiling of biological fluids to help identify biomarkers for infectious disease diagnosis [263] as well as other “-omics” testing, such as proteomics, transcriptomics and metagenomic next-generation sequencing.
3.6. Treatment Options
Treatment must be individualized, and multidisciplinary approaches are often beneficial. Treatment can be divided into three basic areas—treatment of the infection(s) or other contributor(s), immune interventions, and treatment of the resulting symptoms and any other potential contributor(s). Initial subsequent interventions are dependent upon an understanding of the pathophysiological process, how the disease contributors interact, and the primary driver of disease perpetuation and progression.
When a patient has an inadequate response to psychotropics and infection is a possibility, antimicrobials are a consideration. When directly treating an infection, the choice of antimicrobial(s) is dependent on the microorganism, its expected or laboratory-obtained antimicrobial sensitivities, the location of the infection (e.g., CNS vs. non-CNS infection), and the medication’s adverse effect profile. It is important to note that many psychiatric conditions in which microbes may play an etiologic role are considered to be due not to a direct CNS infection but rather to a non-CNS infection that generates a pathogenic immune response with deleterious CNS effects. Antimicrobial treatment may be associated with a Jarisch–Herxheimer reaction, in which there may be a transient exacerbation of symptoms associated with the infection, including neuropsychiatric symptoms [12]. If there is a plausible mechanism for a non-infection environmental contributor, e.g., environmental toxin exposure, the mitigation of ongoing exposure, if any, to the environmental toxin and other measures to limit toxin exposure must be considered.
When immune-mediated symptoms are present from an active infection, a prior infection, or some non-infection immune provocation, consider immune-modulating interventions. With immune interventions, the choice of treatment is dependent upon whether or not there is immune suppression, excessive inflammation, autoimmunity, and/or a failure of adaptive immunity.
When symptoms such as chronic stress and sleep deprivation contribute to compromised immunity, consider symptomatic treatment. Regarding symptomatic treatment, it is necessary to perform a comprehensive clinical examination and then make a list with the patient, ranking which symptoms are the most severe and which symptoms most impede recovery. It is important to consider how symptoms interact with each other. This can help determine which symptoms are the most critical in contributing to disease perpetuation and progression. This type of reflection will help determine which symptoms to treat and in which order.
When a patient has a relapse, treatments that have been effective in the past are a consideration. When a patient is treatment-resistant, treatments that have not been used in the past are a consideration. Constant treatment revisions are needed depending upon whether the patient is improving or showing further disease progression. What has initially caused a condition may be different from what perpetuates that same condition.
From treating thousands of patients over decades, the authors (RB, RG) have found that the symptoms that usually need to be treated first are non-restorative sleep and the symptom(s) that cause the greatest chronic stress in the patient. Non-restorative sleep is often associated with fatigue and cognitive impairments, sometimes called “the terrible triad” [9,396]. A lack of restorative sleep is particularly significant in causing immune dysfunction, the failure of adaptive immunity, and disease progression [371,397,398]. In addition to non-restorative sleep, other symptoms frequently causing chronic stress in the patient include emotional symptoms (depression, anxiety, depersonalization, mood swings, psychosis, intrusive symptoms), chronic pain (headaches, neuropathy, radiculopathy, musculoskeletal pain), multisystem somatic symptoms (neurological, gastrointestinal, dysautonomia, cardiac, genitourinary, etc.), and addictive disorders [10].
Education to help the patient, the caregivers, and those in the support circle better understand the condition is always a critical component of treatment.
Successful psychiatric management can sometimes result in a reduction in infection. On the other hand, a successful reduction in infection can sometimes result in reduced psychiatric symptoms. Our current technological limitations prevent us from being sure that all pathogens have been eradicated. After stabilization, constant vigilance is needed to be alert to the possibility of a relapse that would require additional treatment.
3.7. Healthcare Delivery Issues
Adequately understanding the association between microbes and mental illness is one challenge, but using these insights to sufficiently impact the healthcare delivery system is an additional challenge. Our healthcare system is not structured to readily adapt to new approaches to emerging diseases. Super-specialization, a silo mentality, the rigidity of computerized medical electronic systems, insurance company criteria, and financial limitations impair our ability to adequately approach multisystem illness with complex infectious causes and psychiatric manifestations. The education of healthcare providers is a first step, with curricula addressing these issues in medical schools, residency programs, and allied healthcare programs. Multidisciplinary cooperation, especially between psychiatrists, psychoimmunologists, and infectious disease specialists, is needed [399].
3.8. Examples of Microbes Associated with Mental Illness
Five infectious diseases described as examples of microbes associated with mental illness are syphilis (a sexually transmitted spirochetal disease); toxoplasmosis (a zoonotic parasitic disease caused by Toxoplasma gondii); COVID-19 (a respiratory-transmitted viral disease); Lyme borreliosis and associated infections (zoonotic vector-borne disease); and group A beta hemolytic streptococcal infections and PANDAS/PANS (an autoimmune disease induced by infection and other provocations).
3.8.1. Syphilis
Syphilis is caused by Treponema pallidum and is a historical example of a sexually transmitted infection that can cause psychiatric disease. The spirochete can survive in a host for decades with gradually increasing and expanding general medical and psychiatric symptoms. Before the introduction of penicillin, there were many patients in psychiatric institutions diagnosed with general paresis of the insane, a form of late neurosyphilis. The mental symptoms caused by syphilis include a wide variety of psychiatric syndromes, including dementia and other cognitive impairments, psychosis, and mood disorders [400]. With proper diagnosis and antibiotic therapy in its early stages, syphilis is now readily treated, thereby preventing the development of late-stage complications [401]. Noguchi and Moore’s demonstration in 1913 of spirochetes in the brains of patients with general paresis provided proof of a psychiatric disease associated with chronic meningoencephalitis from a persistent smoldering syphilis infection in brain tissue [20,402]. The course of syphilis in its various stages is shaped by the host’s immune status and immune response to spirochetal infection. Indeed, much of the pathology of this disease is felt to be due to the host inflammatory reaction to the infection rather than direct damage by spirochetes [403,404]. While late-stage neurosyphilis is, fortunately, rare, there remains a lack of consensus on its long-term outcomes with antibiotic treatment [405,406,407,408]. An important consideration with the initiation of antibiotic therapy is the potential occurrence of a Jarisch–Herxheimer reaction, which is a temporary exacerbation of underlying symptoms attributed to the antimicrobial killing of the pathogen with the release of toxic and inflammatory mediators. Herxheimer reactions historically described in neurosyphilis patients include the exacerbation of psychosis, seizure development, and the development of suicidal and violent behavior [220,409].
The history of syphilis contains a lesson in medical ethics. Penicillin was discovered in 1928. The United States Public Health Service began the Tuskegee experiment in 1932, which studied the natural course of syphilis in the study participants. Penicillin was found to be effective in treating syphilis in the early 1940s, and its use expanded during the 1940s. Penicillin treatment was withheld from the study subjects until the 1970s, with subsequent severe syphilis-related neuropsychiatric and physical complications, as well as fatalities, in many of the study participants [410]. Better Institutional Review Board oversight exists over such experiments today. However, this experiment raises one of the ethical questions that scientists struggle with: how much intervention is ethically too little or too much? At one time, penicillin was an innovative and unproven treatment for syphilis: later, it became the standard of care. There are many proposed treatments for COVID-19, Lyme disease, and other infections with physical and psychiatric consequences that may be seen as innovative by some and unproven or disproven by others. Given the risks of long-term somatic and mental sequelae from the inadequate treatment of some infections, the consideration of the risk/benefit ratio is mandatory when evaluating interventions.
3.8.2. Toxoplasmosis
Toxoplasmosis is caused by Toxoplasma gondii and is a well-recognized parasitic zoonotic disease model for a parasite that can be found in the brain associated with mental illness. Some of these effects are possibly mediated by increased dopamine and decreased tryptophan. Toxoplasmosis is a disease in which a microbe completes different parts of the life cycle in different hosts. Based upon the Manipulation Hypothesis, Toxoplasma gondii manipulates the behavior of the host in a manner that makes the host (i.e., mouse) less fearful and more susceptible to predation by a larger mammal (i.e., the cat). This change increases the probability of transmission from an intermediate host to a definitive host [411]. Non-human mammals are the more common part of this microbe’s normal life cycle. However, humans may sometimes be accidental hosts in this zoonotic cycle. When these diseases are considered from the perspective of a zoonotic process, there may be adaptive value for the parasite to cause the host to become more aggressive, more sexually aggressive, more predatorial, and/or more susceptible to predation. As a zoonotic disease, latent Toxoplasma gondii infections are prevalent in humans throughout the world. Many infected individuals can have no or minimal symptoms, but the parasite can also result in psychopathology in humans [412]. The resultant psychopathology includes personality changes, mental illnesses, suicidal and homicidal behavior, schizophrenia, and auto and workplace accidents, which, collectively, can be indirectly responsible for hundreds of thousands of deaths [88,95,156,198,199,200,201,217,254,269,413,414,415].
Some studies have shown different personality changes in men vs. women. One study found that infected men were more likely to disregard rules and were more expedient, suspicious, jealous, and dogmatic, while infected women were more warm-hearted, outgoing, conscientious, persistent, and moralistic [416].
High titers of Toxoplasma gondii are associated with a greater propensity for suicidal behavior [417]. In a sample of 20 European nations, the prevalence of the brain parasite Toxoplasma gondii was positively associated with national suicide rates for men and women [418]. T. gondii seropositivity is also associated with a seven-fold greater risk of self-directed violence [419,420]. In a sample of 20 European nations, the prevalence of Toxoplasma gondii was positively associated with higher national homicide rates, which further amplified the research indicating a positive association of Toxoplasma gondii with suicide rates [421].
3.8.3. COVID-19 (Coronavirus Disease 2019)
COVID-19, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is a viral model of a microbe that, in some persons, plays an important role in the subsequent development of a mental illness. Since the identification of SARS-CoV-2 as the cause of an outbreak of pneumonia in Wuhan, China, in December 2019 and its subsequent rapid spread to other countries worldwide, information in this area has been rapidly evolving. In some, COVID-19 is a mild, at times subclinical infection, while in others, it can be severe or even fatal. Neuropsychiatric manifestations of acute infection include delirium, confusion, emotional disturbances, and psychosis [422]. A subset of patients experience residual sequelae after acute infection, including manifestations particularly relevant to psychiatry. Known as post-acute sequelae of COVID-19 (PASC) and also referred to as “long COVID”, these symptoms can resolve with the passage of time in some individuals while remaining chronic in others. In patients with chronic symptoms, there are similarities to other post-acute viral syndromes, such as Chronic Fatigue Syndrome/Myalgic Encephalomyelitis [423,424]. Symptoms can occur in multiple organ systems. Persistent symptoms may include fatigue, post-exertional malaise, and multiple emotional and cognitive impairments (memory impairment, attention deficits, cognitive difficulties, executive dysfunction) [422]. In addition to cognitive deficits, mental symptoms include anxiety, depression, mood swings, bipolar/manic episodes, obsessive–compulsive disorders, posttraumatic stress, new-onset psychosis, sleep disturbances, substance use disorders, suicidality, and symptom constellations consistent with pediatric acute-onset neuropsychiatric syndrome (PANS; see Section 3.8.5 for additional PANS information) [5,50,81,82,83,84,85,422,425,426,427,428,429,430,431,432]. One retrospective cohort study using electronic health record data comprising 81 million patients in healthcare organizations primarily in the US showed that the risk of common neuropsychiatric disorders (mood disorders, anxiety disorders) returned to baseline in 1–2 months, but there remained an elevated risk of psychotic disorders, cognitive deficit, dementia, and seizures at two years of follow-up [83]. In contrast, another study using data from the large US Veterans Health Administration national healthcare database showed, at one year of follow-up, an increased risk of an array of incident mental health disorders, including anxiety, depression, sleep disorders, stress and adjustment disorders, opioid and substance use disorders, and neurocognitive decline [426].
The proposed mechanisms for PASC [433,434,435,436,437,438] include persistent reservoirs of pathogens or pathogen remnants (e.g., SARS-CoV-2 structural proteins such as spike protein or spike protein fragments such as the S1 subunit); the development of autoimmunity due to molecular mimicry between pathogen and host proteins; the reactivation of other latent pathogens; dysbiosis from SARS-CoV-2–host-microbiome interactions; and resultant organ system or tissue damage from the infection and associated immunopathology, including vasculopathy, coagulopathy, and clotting issues. These potential contributors may act independently or in combination to cause persistent symptoms.
3.8.4. Lyme Borreliosis and Associated Diseases
Lyme borreliosis is a prime example of a vector-borne (tick) zoonotic infection that can have neuropsychiatric manifestations. An estimated 476,000 Americans yearly are diagnosed and treated for Lyme disease, making it the most common vector-borne disease in the US [439]. What is now commonly called Lyme disease was first described in Europe before World War I. In 1970, Dr. Rudolph Scrimenti in Wisconsin reported the first case in the United States, a patient with an erythema migrans rash at the site of a tick bite, accompanied by a low-grade fever, headache, and malaise, with symptoms responding to treatment with intramuscular penicillin [440]. The disease became more widely recognized following an epidemic of arthritis in children and adults in Lyme, Connecticut, which was described in multiple published reports by Dr. Allen Steere and colleagues [441,442,443]. Dr. Willy Burgdorfer discovered the causative organism, the bacterium Borrelia burgdorferi [444]. Like syphilis, Borrelia burgdorferi is a complex spirochetal illness. In contrast to syphilis, it has a much more complex genome that may give it greater adaptive capability to survive under different conditions in different hosts, namely, cold-blooded ticks versus warm-blooded vertebrates [445].
The nomenclature regarding Borrelia burgdorferi infection and Lyme disease is confusing and needs clarification. Lyme disease or Lyme borreliosis is the disease resulting from Borrelia burgdorferi sensu lato (Bbsl) infection. Included within Bbsl are three major Borrelia species that cause Lyme disease: Borrelia burgdorferi (also called Borrelia burgdorferi sensu stricto) causes the disease in the US, while Borrelia afzelii and Borrelia garinii are the predominant species causing Lyme borreliosis in Europe and Asia.
Similar to syphilis, Lyme disease is a complex illness with multi-symptom, multisystemic manifestations that are commonly described as presenting in stages. Early localized disease symptoms include a skin lesion (erythema migrans, or EM) that may or may not be accompanied by constitutional symptoms. Early disseminated disease includes multiple EM lesions and neurologic and cardiac manifestations. Late disseminated disease includes joint and neurologic manifestations. Some less common organ system manifestations, such as ocular involvement, can represent early or late disease. The psychiatric symptoms of Lyme disease are mostly late-stage symptoms [10].
Since many healthcare professionals are unaware of the full range of potential manifestations of Lyme disease, as well as the limited sensitivity of commonly used laboratory tests and interpretation criteria, many early cases are undiagnosed and untreated. These frequently avoidable errors can result in progression to late-stage disease with significant neuropsychiatric symptomatology [9,10].
Lyme borreliosis/tick-borne disease is associated with almost any psychiatric syndrome listed in the American Psychiatric Association DSM5-TR [9,164,312] (Supplementary S1). The neuropsychiatric symptoms seen with Lyme/tick-borne disease include developmental disorders, autism spectrum disorders, schizoaffective disorders, bipolar disorder, depression, anxiety disorders (panic disorder, social anxiety disorder, generalized anxiety disorder), posttraumatic stress disorder, eating disorders, sleep disorders, addiction, suicide, violence, anhedonia, depersonalization, dissociative episodes, derealization, hallucinations, intrusive symptoms, and vegetative functioning impairments. Possible cognitive impairments that can be precipitated include dementia and impairments in attention span, memory, processing, and executive functioning [9,10].
A large seroepidemiology survey in the Czech Republic reported Borrelia burgdorferi seropositivity in approximately 1/3 of psychiatric patients, a rate that was 1.7-fold higher than in matched healthy controls [446]. In the peer-reviewed medical literature, there are currently 501 references demonstrating an association between Lyme borreliosis/tick-borne disease and neuropsychiatric diseases and 88 demonstrating an association with dementia (in Supplementary S1, Peer-Reviewed Evidence of Lyme Borreliosis/Tick-Borne Disease Associated with Psychiatric Symptoms).
There are two broad postulated or demonstrated mechanisms by which late Lyme neuroborreliosis might lead to neuropsychiatric symptoms. First, there can be direct injury from CNS infection, i.e., Lyme encephalitis or meningoencephalitis. This is an infection within the parenchyma of the brain, associated in its infiltrative form with strong perivascular lymphoplasmacytic infiltrates, vasculitis, and microgliosis and in its atrophic form with cortical atrophy, gliosis, and dementia [402]. Second, infections outside the central nervous system (CNS), or perhaps a “smoldering” CNS infection, can have indirect immune and toxic effects upon the CNS through a variety of mechanisms, including molecular mimicry leading to autoantibody formation and cellular immune responses against host neuronal structures; altered metabolism of tryptophan resulting in the decreased production of serotonin and the increased production of neurotoxic and neuroexcitatory kynurenine metabolites; and consequent oxidative stress, neuronal excitotoxicity, changes in homocysteine metabolism, and mitochondrial dysfunction [12,357,358,363,365,366,372,374,447].
In 75% of chronic Lyme disease patients with neurocognitive and/or mood dysfunction that impaired their daily living activities, single-photon emission computed tomography brain imaging demonstrated perfusion deficits to various areas of the brain, most notably the frontal, temporal, and parietal lobes, Patients considered to be seropositive and those considered seronegative had similar rates and severity of perfusion defects. Antibiotic treatment, especially agents with intracellular-penetrating activity, resulted in the resolution or improvement of abnormalities in 70% of patients over a 1- to 2-year period [448].
Manifestations of Lyme disease that continue or recur for an extended period (more than 6 months) after commonly used antibiotic therapy are frequently referred to as either chronic Lyme disease [449,450] or post-treatment Lyme disease syndrome [451]. In their common historical use, these terms tend to connote different viewpoints on the likely etiology of persistent symptoms. “Chronic Lyme disease” commonly connotes that persistent symptoms could be due to an ongoing, active Borrelia infection [450]. As originally defined, “post-treatment Lyme disease syndrome” consists of persistent or recurrent symptoms of pain, fatigue, or cognitive issues lasting more than 6 months after treatment with a 2–4-week course of antibiotics and is considered to be of unknown etiology, although one postulated view is that the symptoms could be autoimmune in nature [338,451]. Importantly, these two explanations for persistent symptoms (ongoing, active infection vs. autoimmunity) need not be mutually exclusive. The latest US Tick-Borne Disease Working Group 2022 Report to Congress uses the term “persistent Lyme disease/chronic Lyme disease” [452] while neutrally recognizing the existence of divergent views on the cause of persistent symptoms.
None of the three aforementioned terms address the potential presence of tick-borne or other coinfections impacting disease presentation. Many other pathogens may be introduced in the tick bite in addition to Borrelia. Evidence indicating the presence of different Bartonella spp. DNA in various types of tick species from diverse geographic locations has also been reported [453]. Common coinfections besides Borrelia that are particularly relevant to neuropsychiatric symptoms include different species of Babesia [91,105,106,207] and Bartonella [25,26,28,105,106,162,163,207,208,221,222,223,224].
While the vector competence of Ixodes scapularis ticks for Bartonella transmission to a human host has yet to be definitively demonstrated and requires further study, Bartonella transmission by Ixodes ricinus, the tick vector for Lyme disease in Europe, has been documented in mice [454]. Furthermore, multiple other insect vectors are known or suspected to transmit Bartonella to humans [453]. Overall, the recognition of coinfections and their potential role in complex cases of Lyme disease is an emerging field of research. Presently, there are many recognized and yet-to-be-recognized tick-borne microbes that may act as human pathogens [455,456,457,458,459].
Considerable confusion, controversy, and complexity surrounding Lyme disease testing contribute to many missed or late diagnoses of Lyme disease that then can manifest with significant late-stage neuropsychiatric symptomatology [9,10,460], and hence, some clarification is in order. Most Lyme disease testing today is indirect testing that detects IgM and/or IgG antibodies produced in response to Borrelia infection, rather than direct testing for the organism itself. The CDC recommends two-tier serologic testing, typically consisting of a first-tier enzyme immunoassay (EIA) that, if positive or indeterminate, is followed by a more specific, second-tier Western blot or immunoblot assay [461]. More recently, the CDC updated their Lyme testing recommendations to allow the use of an EIA other than a Western immunoblot assay as an alternative second-tier test [462]. However, for complex cases, as commonly occurs in patients with neuropsychiatric manifestations, Western immunoblot testing may provide valuable information by demonstrating separate highly Borrelia-specific antibodies, as well as the degree of expansion of the Lyme antibody response, which may provide better support for a clinical diagnosis and help delineate duration of illness [463]. The commonly used interpretation criteria for a positive IgM or IgG immunoblot, which have been widely used since the mid-1990s [461], have been critiqued as being overly restrictive [449,460,464,465]. Notably, the IgG immunoblot criteria for the diagnosis of disseminated/late Lyme disease are based on a single study that reported an overall sensitivity of 83% for their proposed criteria, with substantially lower sensitivity for the subset of patients with neurologic disease compared to those with arthritis (72% vs. 96%, respectively; these figures are calculable from study data presented in their Table 4) [466]. Similarly low or even lower sensitivity of commonly used two-tiered testing—in one study, 43% [467] and, in another study, ranging from 44 to 74% [468]—was reported by two independent research groups, both using a CDC reference panel of serum samples and the CDC-recommended test interpretation criteria. Several subsequent and oft-cited studies reported high sensitivity (97–100%) of commonly used two-tier testing and interpretation criteria in late Lyme disease [469,470,471,472], but the problematic selection bias inherent in their study design deserves commentary. Specifically, the inclusion criteria in these studies required late-disease patients to have lab confirmation, either as defined in CDC surveillance criteria at the time or even as shown by positive two-tier serology. Additionally, in the studies that specified separate numbers for arthritis vs. neurologic disease cases, there were few cases of the latter—in one study, just 11 patients with late neurologic disease [469], and in another study, only 2 patients [470]. Furthermore, in each of these two studies, half or more of the few patients with neurologic disease also had current or previously treated arthritis. Attention to such details is warranted since, as previously noted, the sensitivity of the commonly used IgG immunoblot interpretation criteria for disseminated/late Lyme disease was substantially higher in patients with arthritis compared to neurologic disease in the single study that forms the basis for those criteria [466].
A final point that deserves emphasis is that lab testing cannot be relied on alone to diagnose or exclude Lyme disease and, instead, must always be considered in the context of the whole clinical picture. Clinicians must be familiar with the full array of clinical manifestations of Lyme borreliosis, as, ultimately, Lyme disease must be diagnosed clinically on the basis of clinical history and exam findings, with lab testing regarded as supportive or not of the clinical diagnosis [473,474]. The possibility of false-negative serologic tests in early disease is well recognized, as it takes time for the immune system to respond to infection with Borrelia-specific antibody production. In late Lyme disease, false-negative serologies can also occur due to a variety of reasons [475,476]. Indeed, seronegativity is well documented in patients with late Lyme borreliosis, including PCR- or culture-confirmed disease [477,478,479,480]. Conversely, false positives can be seen due to cross-reactivity in patients with other spirochetal diseases or clinical conditions, such as autoimmune diseases [475]. Additionally, in some Lyme-endemic areas in the US or Europe, background seropositivity rates as high as 11–20% have been reported in healthy blood donors or general outpatients not being seen for tick-borne disease testing [481,482,483,484,485]. In summary, laboratory testing alone cannot be the sole basis for determining whether any infection did or did not play a role in the development of any particular psychiatric symptom or syndrome. Instead, there must be reliance on the total clinical assessment [7,8,9,10].
3.8.5. Group A Streptococcal Infections, PANDAS, and PANS
An area of active investigation for more than two decades that helps demonstrate a connection between microbes and mental illness is the field of pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS). The illness follows a group A streptococcal (GAS) infection, such as pharyngitis, scarlet fever, or an anal streptococcal infection. Subsequently, the individual experiences a sudden onset of obsessive–compulsive symptoms, a tic disorder, or both [486]. Accompanying the psychiatric symptoms are new-onset neurologic abnormalities, such as physical hyperactivity or unusual, jerky involuntary movements. In addition, there are a variety of associated symptoms, including mood changes, increased irritability, sleep difficulties, separation anxiety symptoms, increased day or nighttime urination, joint pains, and motor skill changes, such as a decrement in handwriting [487].
The proposed etiological mechanisms for PANDAS include molecular mimicry and the development of autoimmunity. These processes play an important role in the development of cardiac valvular disease and Sydenham’s chorea, which can occur in individuals suffering from post-Streptococcal Rheumatic Fever [488]. In PANDAS, the proposed mechanism of causation involves antibodies that react to components of the strep bacteria and subsequently cross-react with similar molecules located in the child’s basal ganglia [489]. Experiments using mouse models have found that group A streptococcus infection induces a strong Th17 immune response in the nasal-associated lymphoid tissue (NALT), the murine equivalent of human palatine tonsils [490]. GAS-specific Th17 cells have also been shown to exist in the tonsils of people naturally exposed to group A strep [490]. In a mouse model, multiple GAS challenges promote the migration and persistence of GAS-specific Th17 cells to the brain, leading to blood–brain barrier breakdown and autoantibody access to the CNS [490].
Th17 memory cells help control extracellular bacterial infections and fungi at mucosal surfaces by recruiting and activating myeloid cells (neutrophils) [491] but also play a role in the generation of the immunopathology characteristic of autoimmune conditions such as rheumatoid arthritis and multiple sclerosis [492,493]. In a murine model of PANDAS, evidence supports the action of Th17 cells releasing the cytokine IL-17A, which is thought to play an important role in the entry of immune system cells into the CNS [494]. There, it leads to the disruption of healthy brain cells, eventually resulting in the development of neuropsychiatric symptoms. One hypothesis is that the olfactory bulb’s proximity to the nasal mucosa makes it a susceptible target for insult and infection of the brain [495]. Studies in the literature support the use of the olfactory route by many viruses and bacteria to create an infection within the brain [496]. However, in the case of PANDAS, there is no evidence of streptococcal entry across the blood–brain barrier and into the brain [490]. Recent work reported in preprint form by Agalliu and colleagues demonstrates that two Th17 effector cytokines, IL-17A and GM-CSF, differentially promote blood–brain barrier dysfunction and the microbial expression of interferon-response and chemokine genes in a murine model of intranasal GAS infections [497]. The brain microglia release a variety of chemokines that might act as potential biomarkers of the illness. Collectively, the evidence supports the idea that PANDAS is a form of infection-induced immune-mediated encephalitis.
Since the original description of PANDAS, it has subsequently become recognized as part of a broader category called pediatric acute-onset neuropsychiatric syndrome (PANS) [243,498]. Unlike PANDAS, the name PANS recognizes that the neuropsychiatric and other manifestations of this syndrome can be triggered by not just streptococcal infections but also a variety of other infections [243,499] (e.g., Mycoplasma [263], Borrelia (Lyme disease) [500], Bartonella [162], SARS-CoV-2 [82,425,437]), as well as, potentially, non-infectious triggers, such as environmental exposure to toxins or other inducers of inflammatory reactions [498,501]. As originally defined, the primary symptoms of PANS are the sudden onset of obsessive–compulsive symptoms or restricted eating behaviors. Additional symptoms of PANDAS and PANS include a variety of neuropsychiatric as well as somatic symptoms, including depression, anxiety, emotional lability, irritability, aggression, behavioral regression, ADHD-like symptoms, cognitive changes, sleep disturbances, and urinary frequency or enuresis [243,498,502].
4. Discussion
The microbial impact upon human mental functioning is more extensive than generally appreciated. Historically, there have been, and continue to be, many models to attempt to explain the causes of and contributors to mental illnesses. The increasing recognition that microbes may contribute to mental illness is expanding as clinical observations and newer technologies provide greater evidence.
A considerable amount of the literature recognizes that psychiatric conditions may be associated with infectious contributors. This is demonstrated in Table 1 and Table 2. There are multiple pathophysiological mechanisms explaining this association. The review of the five infection-associated diseases further supports the association between microbes and mental illness.
As a result, clinicians need to consider the possibility of infectious diseases in formulating a pathophysiological explanation and a differential diagnosis. Considering the complexity and interactive nature of the pathogen and host in illness, treatments including anti-infective and/or immune interventions become potential treatment options. This consideration may be of particular significance with treatment-resistant psychiatric illness.
It is important to look at the five examples of microbes associated with mental illnesses discussed in this article from a historical perspective. The effective treatment of neurosyphilis was not fully implemented for many years after the discovery of penicillin. The other four infection-associated diseases are surrounded by controversy. Will current technology facilitate more effective progress toward understanding and treating these illnesses?
There are many obstacles preventing forward progress in recognizing the association between microbes and mental illness. These include difficulties appreciating the potential role of infections in chronic illness, failure to recognize complex disease models, the difficulty developing disease models when there are multiple variables with susceptibility and infection, pathophysiology and manifestations, failure to appreciate the role of chronic relapsing infections and complex interactive infections with psychiatric illness, a silo mentality, paradigm blindness, investments in outdated belief systems, current clinical assessment limitations, laboratory limitations, the limitations of antimicrobial and other treatments, educational limitations, and healthcare system limitations.
Potential solutions include the following: (1) expanded research into the association between microbes and mental illness; (2) a reexamination of existing paradigms to identify and correct gaps and inconsistencies; (3) improved multidisciplinary collaboration; and (4) expanded clinician and public education.
Future Directions
Investigation and collaboration among multiple specialists are needed to further clarify and expand all of the topics that have been reviewed in this article. Table 1 can be expanded, and Table 2 can be expanded to include additional diagnostic categories. Additional research and education addressing the association between microbes and mental illness are needed. In addition, the education of healthcare providers, with curricula addressing microbes and mental illness in medical schools, residency programs, and allied healthcare programs, and multidisciplinary cooperation, especially between psychiatrists, psychoimmunologists, and infectious disease specialists, will help advance progress toward a better understanding of the etiology of mental illnesses.
5. Conclusions
The findings of this review support the concept that infectious diseases may have an important role in psychiatric diagnosis and treatment. Indirect mechanisms of infection, such as inflammation, neuroinflammation, autoimmunity, and other neurophysiological changes, have been implicated in the development and/or progression of some mental illnesses. The persistence of these processes may result in chronic effects on brain structure and function. A combination of these indirect actions, with direct pathophysiologic effects from infectious agents, has the potential to result in a broad spectrum of mental symptoms and illnesses. Further investigation into the association between infectious/immune processes and mental disorders may lead to greater use of antimicrobial and immune-modulating agents in the treatment of psychiatric conditions. This may prevent and reduce mental illness morbidity, disability, and mortality.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/healthcare12010083/s1: Supplementary S1: Peer-Reviewed Evidence of Lyme/Tick-Borne Disease Associated with Psychiatric Symptoms; Supplementary S2: Lyme Disease Screening Assessment; Supplementary S3: Coinfection Screen.
Author Contributions
R.C.B. performed data curation; formal analysis; methodology; project administration; visualization; writing of original draft; and writing, review, and editing of subsequent drafts. R.G. wrote original drafts of the Abstract, the Infections Early in Life with Later Consequences section, the Total Load Theory section, most of the History section, the Streptococcus section, and the Discussion and performed multiple revisions of the full manuscript. C.M. performed multiple reviews and revisions of the manuscript, with particular attention on Table 1 and Table 2; Syphilis; COVID; Lyme Borreliosis and Associated Diseases; Group A Streptococcal Infection, PANDAS, and PANS; and expanded references in the final draft. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable for studies not involving humans or animals.
Informed Consent Statement
Not applicable for studies not involving humans.
Data Availability Statement
Data are contained within the article and Supplementary Materials.
Acknowledgments
The authors recognize and appreciate the contributions of the thousands of members of the Microbes and Mental Illness Listserv over the past 25 years, Team GOAT, and our patients, all of whom have taught us a great deal.
Conflicts of Interest
R.C.B. has been an expert witness in cases involving neuropsychiatric manifestations in Lyme borreliosis patients. R.G. has participated in legal activities related to physician medical practices. C.M. declares no conflicts of interest.
References
- Human Microbiome Data Portal Project. Available online: https://portal.hmpdacc.org (accessed on 22 August 2022).
- O’Connor, S.M.; Taylor, C.E.; Hughes, J.M. Emerging infectious determinants of chronic diseases. Emerg. Infect. Dis. 2006, 12, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Knobler, S.L.; O’Connor, S.; Lemon, S.M.; Najafi, M. (Eds.) The Infectious Etiology of Chronic Diseases: Defining the Relationship, Enhancing the Research, and Mitigating the Effects: Workshop Summary; National Academies Press: Washington, DC, USA, 2004.
- Munjal, S.; Ferrando, S.J.; Freyberg, Z. Neuropsychiatric Aspects of Infectious Diseases: An Update. Crit. Care Clin. 2017, 33, 681–712. [Google Scholar] [CrossRef] [PubMed]
- Huarcaya-Victoria, J.; Alarcon-Ruiz, C.A.; Barzola-Farfán, W.; Cruzalegui-Bazán, C.; Cabrejos-Espinoza, M.; Aspilcueta-Montoya, G.; Cornero-Quispe, F.; Salazar-Bellido, J.; Villarreal, B. One-year follow-up of depression, anxiety, and quality of life of Peruvian patients who survived COVID-19. Qual. Life Res. 2023, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lantos, P.M.; Rumbaugh, J.; Bockenstedt, L.K.; Falck-Ytter, Y.T.; Aguero-Rosenfeld, M.E.; Auwaerter, P.G.; Baldwin, K.; Bannuru, R.R.; Belani, K.K.; Bowie, W.R.; et al. Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 Guidelines for the Prevention, Diagnosis and Treatment of Lyme Disease. Clin. Infect. Dis. 2021, 72, e1–e48. [Google Scholar] [CrossRef] [PubMed]
- Bransfield, R.C.; Cook, M.J.; Bransfield, D.R. Proposed Lyme Disease Guidelines and Psychiatric Illnesses. Healthcare 2019, 7, 105. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, S.P.; Brooks, C.; McNeely, C.L.; Thomas, K.C. Neurological Pain, Psychological Symptoms, and Diagnostic Struggles among Patients with Tick-Borne Diseases. Healthcare 2022, 10, 1178. [Google Scholar] [CrossRef] [PubMed]
- Bransfield, R.C. Neuropsychiatric Lyme Borreliosis: An Overview with a Focus on a Specialty Psychiatrist’s Clinical Practice. Healthcare 2018, 6, 104. [Google Scholar] [CrossRef] [PubMed]
- Bransfield, R.C.; Aidlen, D.M.; Cook, M.J.; Javia, S. A Clinical Diagnostic System for Late-Stage Neuropsychiatric Lyme Borreliosis Based upon an Analysis of 100 Patients. Healthcare 2020, 8, 13. [Google Scholar] [CrossRef]
- Fallon, B.A.; Madsen, T.; Erlangsen, A.; Benros, M.E. Lyme Borreliosis and Associations with Mental Disorders and Suicidal Behavior: A Nationwide Danish Cohort Study. Am. J. Psychiatry 2021, 178, 921–931. [Google Scholar] [CrossRef]
- Bransfield, R.C. The psychoimmunology of lyme/tick-borne diseases and its association with neuropsychiatric symptoms. Open Neurol. J. 2012, 6, 88–93. [Google Scholar] [CrossRef]
- Fallon, B.A.; Nields, J.A.; Burrascano, J.J.; Liegner, K.; DelBene, D.; Liebowitz, M.R. The neuropsychiatric manifestations of Lyme borreliosis. Psychiatr. Q. 1992, 63, 95–117. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Pachner, A.R.; Steere, A.C. CNS manifestations of third stage Lyme disease. Zentralblatt Bakteriol. Mikrobiol. Hyg. Ser. A Med. Microbiol. Infect. Dis. Virol. Parasitol. 1987, 263, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Pachner, A.R.; Duray, P.; Steere, A.C. Central nervous system manifestations of Lyme disease. Arch. Neurol. 1989, 46, 790–795. [Google Scholar] [CrossRef] [PubMed]
- Kohler, J. Die Lyme-Borreliose in Neurologie und Psychiatrie. Fortschr. Med. 1990, 108, 191–193. (In German) [Google Scholar] [PubMed]
- Southern, P.M.; Sanford, J.P. Relapsing Fever: A Clinical and Microbiological Review. Medicine 1969, 48, 129–150. [Google Scholar] [CrossRef]
- Semiz, U.B.; Turhan, V.; Basoglu, C.; Oner, O.; Ebrinc, S.; Cetin, M. Leptospirosis presenting with mania and psychosis: Four consecutive cases seen in a military hospital in Turkey. Int. J. Psychiatry Med. 2005, 35, 299–305. [Google Scholar] [CrossRef]
- Noguchi, H.; Moore, J.W. A demonstration of Treponema pallidum in the brain in cases of general paralysis. J. Exp. Med. 1913, 17, 232–238. [Google Scholar] [CrossRef]
- McBride, J.H. Mental symptoms of cerebral syphilis. JAMA 1901, 36, 297–302. [Google Scholar] [CrossRef]
- Dieterle, R.R. Spirochetosis of the central nervous system in general paralysis. Am. J. Psychiatry 1928, 84, 547–560. [Google Scholar] [CrossRef]
- Lin, L.R.; Zhang, H.L.; Huang, S.J.; Zeng, Y.L.; Xi, Y.; Guo, X.J.; Liu, G.L.; Tong, M.L.; Zheng, W.H.; Liu, L.L.; et al. Psychiatric manifestations as primary symptom of neurosyphilis among HIV-negative patients. J. Neuropsychiatry Clin. Neurosci. 2014, 26, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Bettoni, L.; Gabrielli, M.; Lechi, A.; Tedeschi, F.; Trabattoni, G. Cerebral mycosis: Clinico-pathological report of four cases observed in fifteen months. Ital. J. Neurol. Sci. 1984, 5, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Harvey, R.A.; Misselbeck, W.J.; Uphold, R.E. Cat-scratch disease: An unusual cause of combative behavior. Am. J. Emerg. Med. 1991, 9, 52–53. [Google Scholar] [CrossRef] [PubMed]
- Carithers, H.A.; Margileth, A.M. Cat-scratch disease. Acute encephalopathy and other neurologic manifestations. Am. J. Dis. Child. 1991, 145, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Breitschwerdt, E.B.; Mascarelli, P.E.; Schweickert, L.A.; Maggi, R.G.; Hegarty, B.C.; Bradley, J.M.; Woods, C.W. Hallucinations, sensory neuropathy, and peripheral visual deficits in a young woman infected with Bartonella koehlerae. J. Clin. Microbiol. 2011, 49, 3415–3417. [Google Scholar] [CrossRef] [PubMed]
- Breitschwerdt, E.B.; Sontakke, S.; Hopkins, S. Neurological Manifestations of Bartonellosis in Immunocompetent Patients: A composite of reports from 2005–2012. J. Neuroparasitol. 2013, 3, 1–15. [Google Scholar] [CrossRef]
- Shah, I.A.; Kawoos, Y.; Sanai, B.A.; Rabyang, S.; Banday, D. Neurobrucellosis Presenting as Acute Psychosis. J. Neurosci. Rural Pract. 2018, 9, 644–646. [Google Scholar] [CrossRef] [PubMed]
- Kalayci, F.; Ozdemir, A.; Saribas, S.; Yuksel, P.; Ergin, S.; Kuskucu, A.M.; Poyraz, C.A.; Balcioglu, I.; Alpay, N.; Kurt, A.; et al. The relationship of Chlamydophila pneumoniae with schizophrenia: The role of brain-derived neurotrophic factor (BDNF) and neurotrophin-3 (NT-3) in this relationship. Rev. Argent. Microbiol. 2017, 49, 39–49. [Google Scholar] [CrossRef]
- Fellerhoff, B.; Laumbacher, B.; Wank, R. High risk of schizophrenia and other mental disorders associated with chlamydial infections: Hypothesis to combine drug treatment and adoptive immunotherapy. Med. Hypotheses 2005, 65, 243–252. [Google Scholar] [CrossRef]
- Morroy, G.; Peters, J.B.; van Nieuwenhof, M.; Bor, H.H.; Hautvast, J.L.; van der Hoek, W.; Wijkmans, C.J.; Vercoulen, J.H. The health status of Q-fever patients after long-term follow-up. BMC Infect. Dis. 2011, 11, 97. [Google Scholar] [CrossRef]
- Olano, J.P.; Hogrefe, W.; Seaton, B.; Walker, D.H. Clinical manifestations, epidemiology, and laboratory diagnosis of human monocytotropic ehrlichiosis in a commercial laboratory setting. Clin. Diagn. Lab. Immunol. 2003, 10, 891–896. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, A.M.; Bertagnolli, J.F.; Shadiack, E.; De Antonio, S.M. An Unusual Case of Transient Psychosis from Ehrlichia Infection. Osteopath. Fam. 2012, 4, 124–127. [Google Scholar] [CrossRef]
- Al Quraan, A.M.; Beriwal, N.; Sangay, P.; Namgyal, T. The Psychotic Impact of Helicobacter pylori Gastritis and Functional Dyspepsia on Depression: A Systematic Review. Cureus 2019, 11, e5956. [Google Scholar] [CrossRef] [PubMed]
- Nicolson, G.L.; Nasralla, M.Y.; Berns, P.; Haier, J. Chronic Mycoplasmal Infections in Autism Patients. In Proceedings of the International Mind of a Child Conference, Sydney, Australia, 4–6 April 2002; Available online: https://www.researchgate.net/publication/228478817_Chronic_Mycoplasmal_Infections_in_Autism_Patients (accessed on 20 January 2023).
- Kim, Y.; Ko, T.S.; Yum, M.S.; Jung, A.Y.; Kim, H.W. Obsessive-Compulsive Disorder Related to Mycoplasma-Associated Autoimmune Encephalopathy with Basal Ganglia Involvement. J. Child Adolesc. Psychopharmacol. 2016, 26, 400–402. [Google Scholar] [CrossRef] [PubMed]
- Ercan, T.E.; Ercan, G.; Severge, B.; Arpaozu, M.; Karasu, G. Mycoplasma pneumoniae infection and obsessive-compulsive disease: A case report. J. Child Neurol. 2008, 23, 338–340. [Google Scholar] [CrossRef] [PubMed]
- Gorman, R.J.; Saxon, S.; Snead, O.C., 3rd. Neurologic sequelae of Rocky Mountain spotted fever. Pediatrics 1981, 67, 354–357. [Google Scholar] [CrossRef] [PubMed]
- Harrell, G.T. Rickettsial involvement of the nervous system. Med. Clin. N. Am. 1953, 37, 395–422. [Google Scholar] [CrossRef]
- Ripley, H.S. Neuropsychiatric observation on tsutsugamushi fever (scrub typhus). Arch. Neurol. Psychiatry 1946, 56, 42–54. [Google Scholar] [CrossRef]
- Mahajan, S.K.; Mahajan, S.K. Neuropsychiatric Manifestations of Scrub Typhus. J. Neurosci. Rural. Pract. 2017, 8, 421–426. [Google Scholar] [CrossRef]
- Jackson, Y.; Chappuis, F.; Loutan, L. African tick-bite fever: Four cases among Swiss travelers returning from South Africa. J. Travel Med. 2004, 11, 225–228. [Google Scholar] [CrossRef]
- Swedo, S.E.; Grant, P.J. Annotation: PANDAS: A model for human autoimmune disease. J. Child Psychol. Psychiatry 2005, 46, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Duprez, T.P.; Grandin, C.B.; Bonnier, C.; Thauvoy, C.W.; Gadisseux, J.F.; Dutrieux, J.L.; Evrard, P. Whipple disease confined to the central nervous system in childhood. AJNR Am. J. Neuroradiol. 1996, 17, 1589–1591. [Google Scholar] [PubMed]
- Mohamed, W.; Neil, E.; Kupsky, W.J.; Juhász, C.; Mittal, S.; Santhakumar, S. Isolated intracranial Whipple’s disease—Report of a rare case and review of the literature. J. Neurol. Sci. 2011, 308, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, D.E.; Bode, L.; Spannhuth, C.W.; Hecker, H.; Ludwig, H.; Emrich, H.M. Antiviral treatment perspective against Borna disease virus 1 infection in major depression: A double-blind placebo-controlled randomized clinical trial. BMC Pharmacol. Toxicol. 2020, 21, 12. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, M.S.; Gautam, P.; Jhanjee, A. Psychiatric Morbidity in Patients with Chikungunya Fever: First Report from India. J. Clin. Diagn. Res. 2015, 9, VC01–VC03. [Google Scholar] [CrossRef] [PubMed]
- Severance, E.G.; Dickerson, F.B.; Viscidi, R.P.; Bossis, I.; Stallings, C.R.; Origoni, A.E.; Sullens, A.; Yolken, R.H. Coronavirus immunoreactivity in individuals with a recent onset of psychotic symptoms. Schizophr. Bull. 2011, 37, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]
- Lam, M.H.; Wing, Y.K.; Yu, M.W.; Leung, C.M.; Ma, R.C.; Kong, A.P.; So, W.Y.; Fong, S.Y.; Lam, S.P. Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors: Long-term follow-up. Arch. Intern. Med. 2009, 169, 2142–2147. [Google Scholar] [CrossRef]
- Liao, Y.T.; Hsieh, M.H.; Yang, Y.H.; Wang, Y.C.; Tsai, C.S.; Chen, V.C.; Gossop, M. Association between depression and enterovirus infection: A nationwide population-based cohort study. Medicine 2017, 96, e5983. [Google Scholar] [CrossRef]
- Marques, F.; Brito, M.J.; Conde, M.; Pinto, M.; Moreira, A. Autism spectrum disorder secondary to enterovirus encephalitis. J. Child Neurol. 2014, 29, 708–714. [Google Scholar] [CrossRef]
- Lin, H.Y.; Chen, Y.L.; Chou, P.H.; Gau, S.S.; Chang, L.Y. Long-term psychiatric outcomes in youth with enterovirus A71 central nervous system involvement. Brain Behav. Immun. Health 2022, 23, 100479. [Google Scholar] [CrossRef] [PubMed]
- Ford, B.N.; Yolken, R.H.; Aupperle, R.L.; Teague, T.K.; Irwin, M.R.; Paulus, M.P.; Savitz, J. Association of Early-Life Stress with Cytomegalovirus Infection in Adults with Major Depressive Disorder. JAMA Psychiatry 2019, 76, 545–547. [Google Scholar] [CrossRef]
- Burgdorf, K.S.; Trabjerg, B.B.; Pedersen, M.G.; Nissen, J.; Banasik, K.; Pedersen, O.B.; Sørensen, E.; Nielsen, K.R.; Larsen, M.H.; Erikstrup, C.; et al. Large-scale study of Toxoplasma and Cytomegalovirus shows an association between infection and serious psychiatric disorders. Brain Behav. Immun. 2019, 79, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Webster, M.J.; Weickert, C.S.; Beasley, C.L.; Paulus, M.P.; Yolken, R.H.; Savitz, J. Cytomegalovirus antibodies are associated with mood disorders, suicide, markers of neuroinflammation, and microglia activation in postmortem brain samples. Mol. Psychiatry 2023. [Google Scholar] [CrossRef] [PubMed]
- Khandaker, G.M.; Stochl, J.; Zammit, S.; Lewis, G.; Jones, P.B. Childhood Epstein-Barr Virus infection and subsequent risk of psychotic experiences in adolescence: A population-based prospective serological study. Schizophr. Res. 2014, 158, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Jones-Brando, L.; Dickerson, F.; Ford, G.; Stallings, C.; Origoni, A.; Katsafanas, E.; Sweeney, K.; Squire, A.; Khushalani, S.; Yolken, R. Atypical immune response to Epstein-Barr virus in major depressive disorder. J. Affect. Disord. 2020, 264, 221–226. [Google Scholar] [CrossRef]
- Brown, J.S., Jr. Geographic correlation of schizophrenia to ticks and tick-borne encephalitis. Schizophr. Bull. 1994, 20, 755–775. [Google Scholar] [CrossRef]
- Faccioli, J.; Nardelli, S.; Gioia, S.; Riggio, O.; Ridola, L. Neurological and psychiatric effects of hepatitis C virus infection. World J. Gastroenterol. 2021, 27, 4846–4861. [Google Scholar] [CrossRef]
- Pawlowski, T.; Radkowski, M.; Małyszczak, K.; Inglot, M.; Zalewska, M.; Jablonska, J.; Laskus, T. Depression and neuroticism in patients with chronic hepatitis C: Correlation with peripheral blood mononuclear cells activation. J. Clin. Virol. 2014, 60, 105–111. [Google Scholar] [CrossRef]
- Adinolfi, L.E.; Nevola, R.; Lus, G.; Restivo, L.; Guerrera, B.; Romano, C.; Zampino, R.; Rinaldi, L.; Sellitto, A.; Giordano, M.; et al. Chronic hepatitis C virus infection and neurological and psychiatric disorders: An overview. World J. Gastroenterol. 2015, 21, 2269–2280. [Google Scholar] [CrossRef]
- Huang, W.; Li, S.; Hu, Y.; Yu, H.; Luo, F.; Zhang, Q.; Zhu, F. Implication of the env gene of the human endogenous retrovirus W family in the expression of BDNF and DRD3 and development of recent-onset schizophrenia. Schizophr. Bull. 2011, 37, 988–1000. [Google Scholar] [CrossRef]
- Yan, Q.; Wu, X.; Zhou, P.; Zhou, Y.; Li, X.; Liu, Z.; Tan, H.; Yao, W.; Xia, Y.; Zhu, F. HERV-W Envelope Triggers Abnormal Dopaminergic Neuron Process through DRD2/PP2A/AKT1/GSK3 for Schizophrenia Risk. Viruses 2022, 14, 145. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Huang, J.; Zhu, F. Human Endogenous Retroviral Envelope Protein Syncytin-1 and Inflammatory Abnormalities in Neuropsychological Diseases. Front. Psychiatry 2018, 9, 422. [Google Scholar] [CrossRef] [PubMed]
- Johansson, E.M.; Bouchet, D.; Tamouza, R.; Ellul, P.; Morr, A.S.; Avignone, E.; Germi, R.; Leboyer, M.; Perron, H.; Groc, L. Human endogenous retroviral protein triggers deficit in glutamate synapse maturation and behaviors associated with psychosis. Sci. Adv. 2020, 6, eabc0708. [Google Scholar] [CrossRef] [PubMed]
- Owe-Larsson, B.; Säll, L.; Salamon, E.; Allgulander, C. HIV infection and psychiatric illness. Afr. J. Psychiatry 2009, 12, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Rocha-Filho, P.A.S.; Goncalves, L.R. Depression and anxiety disorders among patients with human T-cell lymphotropic virus type-1: A cross-sectional study with a comparison group. Rev. Soc. Bras. Med. Trop. 2018, 51, 357–360. [Google Scholar] [CrossRef] [PubMed]
- Honigsbaum, M. “An inexpressible dread”: Psychoses of influenza at fin-de-siècle. Lancet 2013, 381, 988–989. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, F.; Stallings, C.; Origoni, A.; Copp, C.; Khushalani, S.; Yolken, R. Antibodies to measles in individuals with recent onset psychosis. Schizophr. Res. 2010, 119, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Caplan, R.; Tanguay, P.E.; Szekely, A.G. Subacute sclerosing panencephalitis presenting as childhood psychosis. J. Am. Acad. Child Adolesc. Psychiatry 1987, 26, 440–443. [Google Scholar] [CrossRef]
- Duncalf, C.M.; Kent, J.N.; Harbord, M.; Hicks, E.P. Subacute sclerosing panencephalitis presenting as schizophreniform psychosis. Br. J. Psychiatry 1989, 155, 557–559. [Google Scholar] [CrossRef]
- Parmar, A.; Ranjan, R.; Sagar, R. Subacute Sclerosing Panencephalitis Presenting with Isolated Positive Psychotic and Catatonic Symptoms. Indian J. Psychol. Med. 2017, 39, 534–536. [Google Scholar] [CrossRef] [PubMed]
- Reddy, B.; Das, S.; Guruprasad, S. Primary Psychiatric Manifestations of Subacute Sclerosing Panencephalitis: A Case Report and Literature Review. Psychosomatics 2018, 59, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Jolly, A.J.; Suhas, S.; Arasappa, R.; Kamble, N.; Pal, P.K.; Varambally, S. Subacute Sclerosing Panencephalitis Masquerading as Schizophrenia: An Example of Diagnostic Overshadowing in NeuroPsychiatry. Prim. Care Companion CNS Disord. 2022, 24, 40943. [Google Scholar] [CrossRef] [PubMed]
- Kerr, J.R.; Barah, F.; Chiswick, M.L.; McDonnell, G.V.; Smith, J.; Chapman, M.D.; Bingham, J.B.; Kelleher, P.; Sheppard, M.N. Evidence for the role of demyelination, HLA-DR alleles, and cytokines in the pathogenesis of parvovirus B19 meningoencephalitis and its sequelae. J. Neurol. Neurosurg. Psychiatry 2002, 73, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Hammond, C.J.; Hobbs, J.A. Parvovirus B19 infection of brain: Possible role of gender in determining mental illness and autoimmune thyroid disorders. Med. Hypotheses 2007, 69, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Suvisaari, J.; Haukka, J.; Tanskanen, A.; Hovi, T.; Lönnqvist, J. Association between prenatal exposure to poliovirus infection and adult schizophrenia. Am. J. Psychiatry 1999, 156, 1100–1102. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, N.; Sen, M.S.; Jhanda, S.; Grover, S. Psychiatric manifestations of congenital rubella syndrome: A case report and review of literature. J. Pediatr. Neurosci. 2016, 11, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Bartley, C.M.; Johns, C.; Ngo, T.T.; Dandekar, R.; Loudermilk, R.L.; Alvarenga, B.D.; Hawes, I.A.; Zamecnik, C.R.; Zorn, K.C.; Alexander, J.R.; et al. Anti-SARS-CoV-2 and Autoantibody Profiles in the Cerebrospinal Fluid of 3 Teenaged Patients with COVID-19 and Subacute Neuropsychiatric Symptoms. JAMA Neurol. 2021, 78, 1503–1509. [Google Scholar] [CrossRef]
- Pavone, P.; Ceccarelli, M.; Marino, S.; Caruso, D.; Falsaperla, R.; Berretta, M.; Rullo, E.V.; Nunnari, G. SARS-CoV-2 related paediatric acute-onset neuropsychiatric syndrome. Lancet Child Adolesc. Health 2021, 5, e19–e21. [Google Scholar] [CrossRef]
- Taquet, M.; Sillett, R.; Zhu, L.; Mendel, J.; Camplisson, I.; Dercon, Q.; Harrison, P.J. Neurological and psychiatric risk trajectories after SARS-CoV-2 infection: An analysis of 2-year retrospective cohort studies including 1,284,437 patients. Lancet Psychiatry 2022, 9, 815–827. [Google Scholar] [CrossRef]
- Badenoch, J.B.; Rengasamy, E.R.; Watson, C.; Jansen, K.; Chakraborty, S.; Sundaram, R.D.; Hafeez, D.; Burchill, E.; Saini, A.; Thomas, L.; et al. Persistent neuropsychiatric symptoms after COVID-19: A systematic review and meta-analysis. Brain Commun. 2021, 4, fcab297. [Google Scholar] [CrossRef] [PubMed]
- Ferrando, S.J.; Klepacz, L.; Lynch, S.; Tavakkoli, M.; Dornbush, R.; Baharani, R.; Smolin, Y.; Bartell, A. COVID-19 Psychosis: A Potential New Neuropsychiatric Condition Triggered by Novel Coronavirus Infection and the Inflammatory Response? Psychosomatics 2020, 61, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Nolan, M.S.; Hause, A.M.; Murray, K.O. Findings of long-term depression up to 8 years post infection from West Nile virus. J. Clin. Psychol. 2012, 68, 801–808. [Google Scholar] [CrossRef] [PubMed]
- Lino, A.; Erickson, T.A.; Nolan, M.S.; Murray, K.O.; Ronca, S.E. A Preliminary Study of Proinflammatory Cytokines and Depression Following West Nile Virus Infection. Pathogens 2022, 11, 650. [Google Scholar] [CrossRef] [PubMed]
- Weiss, M.G. Parasitic diseases and psychiatric illness. Can. J. Psychiatry 1994, 39, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Nevin, R.L.; Croft, A.M. Psychiatric effects of malaria and anti-malarial drugs: Historical and modern perspectives. Malar. J. 2016, 5, 332. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.; Othieno, C.; Ongeri, L.; Ongecha, M.; Sifuna, P.; Omollo, R.; Ogutu, B. Malaria and mental disorder: A population study in an area endemic for malaria in Kenya. World Psychiatry 2017, 16, 324–325. [Google Scholar] [CrossRef]
- Sherr, V.T. Human babesiosis—An unrecorded reality. Absence of formal registry undermines its detection, diagnosis and treatment, suggesting need for immediate mandatory reporting. Med. Hypotheses 2004, 63, 609–615. [Google Scholar] [CrossRef]
- Hamdani, N.; Doukhan, R.; Picard, A.; Tamouza, R.; Leboyer, M. A bipolar disorder patient becoming asymptomatic after adjunctive anti-filiarasis treatment: A case report. BMC Psychiatry 2013, 13, 81. [Google Scholar] [CrossRef]
- Kenney, M.; Hewitt, R. Psychoneurotic disturbances in filariasis, and their relief by removal of adult worms or treatment with hetrazan. Am. J. Trop. Med. Hyg. 1950, 30, 895–899. [Google Scholar] [CrossRef]
- Pires, M.; Wright, B.; Kaye, P.M.; da Conceição, V.; Churchill, R.C. The impact of leishmaniasis on mental health and psychosocial well-being: A systematic review. PLoS ONE 2019, 14, e0223313. [Google Scholar] [CrossRef] [PubMed]
- Torrey, E.F.; Yolken, R.H. Toxoplasma gondii and schizophrenia. Emerg. Infect. Dis. 2003, 9, 1375–1380. [Google Scholar] [CrossRef] [PubMed]
- El-Kady, A.M.; Allemailem, K.S.; Almatroudi, A.; Abler, B.; Elsayed, M. Psychiatric Disorders of Neurocysticercosis: Narrative Review. Neuropsychiatr. Dis. Treat. 2021, 17, 1599–1610. [Google Scholar] [CrossRef] [PubMed]
- MacArthur, W.P. Cysticercosis as seen in British army with special reference to production of epilepsy. J. R. Army Med. Corps 1934, 62, 241–259. [Google Scholar]
- Forlenza, O.V.; Filho, A.H.; Nobrega, J.P.; dos Ramos Machado, L.; de Barros, N.G.; de Camargo, C.H.; da Silva, M.F. Psychiatric manifestations of neurocysticercosis: A study of 38 patients from a neurology clinic in Brazil. J. Neurol. Neurosurg. Psychiatry 1997, 62, 612–616. [Google Scholar] [CrossRef] [PubMed]
- Walters, J. Points of clinical importance in amoebiasis, leishmaniasis and trypanosomiasis. Trans. R. Soc. Trop. Med. Hyg. 1970, 64, 220–222. [Google Scholar] [CrossRef] [PubMed]
- Dembowitz, N. Psychiatry amongst West African troops. J. R. Army Med. Corps 1945, 84, 70–74. [Google Scholar]
- Severance, E.G.; Gressitt, K.L.; Stallings, C.R.; Katsafanas, E.; Schweinfurth, L.A.; Savage, C.L.; Adamos, M.B.; Sweeney, K.M.; Origoni, A.E.; Khushalani, S.; et al. Candida albicans exposures, sex specificity and cognitive deficits in schizophrenia and bipolar disorder. NPJ Schizophr. 2016, 2, 16018. [Google Scholar] [CrossRef]
- Severance, E.G.; Gressitt, K.L.; Stallings, C.R.; Katsafanas, E.; Schweinfurth, L.A.; Savage, C.L.G.; Adamos, M.B.; Sweeney, K.M.; Origoni, A.E.; Khushalani, S.; et al. Probiotic normalization of Candida albicans in schizophrenia: A randomized, placebo-controlled, longitudinal pilot study. Brain Behav. Immun. 2017, 62, 41–45. [Google Scholar] [CrossRef]
- Kim, J.; Hartzell, G.; Rezaii, N.; Gensler, L.; Baer, W.; Young, R.; Schwartz, A.C. Psychosis Due to Disseminated Cryptococcal Infection and Delirium in an Immunocompetent Patient: A Case Report and Review of the Literature. Psychosomatics 2018, 59, 394–399. [Google Scholar] [CrossRef]
- Prakash, P.Y.; Sugandhi, R.P. Neuropsychiatric manifestation of confusional psychosis due to Cryptococcus neoformans var. grubii in an apparently immunocompetent host: A case report. Cases J. 2009, 2, 9084. [Google Scholar] [CrossRef] [PubMed]
- Bransfield, R.C. Preventable cases of autism: Relationship between chronic infectious diseases and neurological outcome. Pediatr. Health 2009, 3, 125–140. [Google Scholar] [CrossRef]
- Bransfield, R.C.; Wulfman, J.S.; Harvey, W.T.; Usman, A.I. The association between tick-borne infections, Lyme borreliosis and autism spectrum disorders. Med. Hypotheses 2008, 70, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Pletnikov, M.V.; Moran, T.H.; Carbone, K.M. Borna disease virus infection of the neonatal rat: Developmental brain injury model of autism spectrum disorders. Front. Biosci. 2002, 7, 593–607. [Google Scholar] [CrossRef]
- Pletnikov, M.V.; Rubin, S.A.; Vasudevan, K.; Moran, T.H.; Carbone, K.M. Developmental brain injury associated with abnormal play behavior in neonatally Borna disease virus-infected Lewis rats: A model of autism. Behav. Brain Res. 1999, 100, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Hornig, M.; Weissenböck, H.; Horscroft, N.; Lipkin, W.I. An infection-based model of neurodevelopmental damage. Proc. Natl. Acad. Sci. USA 1999, 96, 12102–12107. [Google Scholar] [CrossRef] [PubMed]
- Lancaster, K.; Dietz, D.M.; Moran, T.H.; Pletnikov, M.V. Abnormal social behaviors in young and adult rats neonatally infected with Borna disease virus. Behav. Brain Res. 2007, 176, 141–148. [Google Scholar] [CrossRef]
- Kuhn, M.; Bransfield, R. Divergent opinions of proper Lyme disease diagnosis and implications for children co-morbid with autism spectrum disorder. Med. Hypotheses 2014, 83, 321–325. [Google Scholar] [CrossRef]
- Kuhn, M.; Grave, S.; Bransfield, R.; Harris, S. Long term antibiotic therapy may be an effective treatment for children co-morbid with Lyme disease and autism spectrum disorder. Med. Hypotheses 2012, 78, 606–615. [Google Scholar] [CrossRef]
- Planche, P.; Botbol, M. Lyme disease, Autism Spectrum Disorder and antibiotic therapy: A case report. Ann. Med. Psychol. 2013, 171, 711–715. [Google Scholar] [CrossRef]
- Kucharska, M. Borreliosis and co-infection as underlying factor in autism. In Proceedings of the 20th Annual ILADS Scientific Conference, Boston, MA, USA, 31 October–3 November 2019. [Google Scholar]
- Kucharska, M. Child with autism, mother with Lyme—Congenital Borreliosis? In Proceedings of the 18th Annual ILADS Scientific Conference, Boston, MA, USA, 9–12 November 2017. [Google Scholar]
- Alonso, L.; Raymond, P. Complex chronic infections in autistic children. In Proceedings of the ILADS 2017 European Conference, Paris, France, 19 May 2017. [Google Scholar]
- Nicolson, G.L. Chronic Bacterial and Viral Infections in Neurodegenerative and Neurobehavioral Diseases. Lab. Med. 2008, 39, 291–299. [Google Scholar] [CrossRef]
- Nicolson, G.L.; Gan, R.; Nicolson, N.L.; Haier, J. Evidence for Mycoplasma ssp., Chlamydia pneunomiae, and human herpes virus-6 coinfections in the blood of patients with autistic spectrum disorders. J. Neurosci. Res. 2007, 85, 1143–1148. [Google Scholar] [CrossRef] [PubMed]
- Contini, C.; Seraceni, S.; Cultrera, R.; Castellazzi, M.; Granieri, E.; Fainardi, E. Chlamydophila pneumoniae Infection and Its Role in Neurological Disorders. Interdiscip. Perspect. Infect. Dis. 2010, 2010, 273573. [Google Scholar] [CrossRef] [PubMed]
- Markowitz, P.I. Autism in a child with congenital cytomegalovirus infection. J. Autism Dev. Disord. 1983, 13, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, E.G.; Ash, E.; Williams, C.P. Autism and congenital cytomegalovirus. J. Autism Dev. Disord. 1984, 14, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Gentile, I.; Zappulo, E.; Riccio, M.P.; Binda, S.; Bubba, L.; Pellegrinelli, L.; Scognamiglio, D.; Operto, F.; Margari, L.; Borgia, G.; et al. Prevalence of Congenital Cytomegalovirus Infection Assessed through Viral Genome Detection in Dried Blood Spots in Children with Autism Spectrum Disorders. In Vivo 2017, 31, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.; Fujimoto, C.; Nakajima, E.; Isagai, T.; Matsuishi, T. Possible association between congenital cytomegalovirus infection and autistic disorder. J. Autism Dev. Disord. 2003, 33, 455–459. [Google Scholar] [CrossRef]
- Sweeten, T.L.; Posey, D.J.; McDougle, C.J. Brief report: Autistic disorder in three children with cytomegalovirus infection. J. Autism Dev. Disord. 2004, 34, 583–586. [Google Scholar] [CrossRef]
- Baker, S.; Shaw, W. Case Study: Rapid Complete Recovery from an Autism Spectrum Disorder after Treatment of Aspergillus with the Antifungal Drugs Itraconazole and Sporanox. Integr. Med. 2020, 19, 20–27. [Google Scholar]
- Markova, N. Dysbiotic microbiota in autistic children and their mothers: Persistence of fungal and bacterial wall-deficient L-form variants in blood. Sci. Rep. 2019, 9, 13401. [Google Scholar] [CrossRef]
- Herman, A.; Herman, A.P. Could Candida Overgrowth Be Involved in the Pathophysiology of Autism? J. Clin. Med. 2022, 11, 442. [Google Scholar] [CrossRef] [PubMed]
- Kantarcioglu, A.S.; Kiraz, N.; Aydin, A. Microbiota-Gut-Brain Axis: Yeast Species Isolated from Stool Samples of Children with Suspected or Diagnosed Autism Spectrum Disorders and In Vitro Susceptibility against Nystatin and Fluconazole. Mycopathologia 2016, 181, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Iovene, M.R.; Bombace, F.; Maresca, R.; Sapone, A.; Iardino, P.; Picardi, A.; Marotta, R.; Schiraldi, C.; Siniscalco, D.; Serra, N.; et al. Intestinal Dysbiosis and Yeast Isolation in Stool of Subjects with Autism Spectrum Disorders. Mycopathologia 2017, 182, 349–363. [Google Scholar] [CrossRef] [PubMed]
- De Long, G.R.; Bean, S.C.; Brown, F.R., 3rd. Acquired reversible autistic syndrome in acute encephalopathic illness in children. Arch. Neurol. 1981, 38, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Gillberg, C. Onset at age 14 of a typical autistic syndrome. A case report of a girl with herpes simplex encephalitis. J. Autism Dev. Disord. 1986, 16, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Gillberg, I.C. Autistic syndrome with onset at age 31 years: Herpes encephalitis as a possible model for childhood autism. Dev. Med. Child Neurol. 1991, 33, 920–924. [Google Scholar] [CrossRef] [PubMed]
- Ghaziuddin, M.; Tsai, L.Y.; Eilers, L.; Ghaziuddin, N. Brief report: Autism and herpes simplex encephalitis. J. Autism Dev. Disord. 1992, 22, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Ghaziuddin, M.; Al-Khouri, I.; Ghaziuddin, N. Autistic symptoms following herpes encephalitis. Eur. Child Adolesc. Psychiatry 2002, 11, 142–146. [Google Scholar] [CrossRef]
- Singh, V.K.; Lin, S.X.; Yang, V.C. Serological association of measles virus and human herpesvirus-6 with brain autoantibodies in autism. Clin. Immunol. Immunopathol. 1998, 89, 105–108. [Google Scholar] [CrossRef]
- Sabourin, K.R.; Reynolds, A.; Schendel, D.; Rosenberg, S.; Croen, L.A.; Pinto-Martin, J.A.; Schieve, L.A.; Newschaffer, C.; Lee, L.C.; Di Guiseppi, C. Infections in children with autism spectrum disorder: Study to Explore Early Development (SEED). Autism Res. 2019, 12, 136–146. [Google Scholar] [CrossRef]
- Debost, J.P.G.; Thorsteinsson, E.; Trabjerg, B.; Benros, M.E.; Albiñana, C.; Vilhjalmsson, B.J.; Børglum, A.; Mors, O.; Werge, T.; Mortensen, P.B.; et al. Genetic and psychosocial influence on the association between early childhood infections and later psychiatric disorders. Acta Psychiatr. Scand. 2022, 146, 406–419. [Google Scholar] [CrossRef] [PubMed]
- Morton, J.T.; Jin, D.M.; Mills, R.H.; Shao, Y.; Rahman, G.; McDonald, D.; Zhu, Q.; Balaban, M.; Jiang, Y.; Cantrell, K.; et al. Multi-level analysis of the gut-brain axis shows autism spectrum disorder-associated molecular and microbial profiles. Nat. Neurosci. 2023, 26, 1208–1217. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, A.; Van de Water, J. The Role of the Immune System in Autism Spectrum Disorder. Neuropsychopharmacology 2017, 42, 284–298. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.K.; Magnusson, C.; Gardner, R.M.; Blomström, Å.; Newschaffer, C.J.; Burstyn, I.; Karlsson, H.; Dalman, C. Maternal hospitalization with infection during pregnancy and risk of autism spectrum disorders. Brain Behav. Immun. 2015, 44, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Atladóttir, H.O.; Thorsen, P.; Østergaard, L.; Schendel, D.E.; Lemcke, S.; Abdallah, M.; Parner, E.T. Maternal infection requiring hospitalization during pregnancy and autism spectrum disorders. J. Autism Dev. Disord. 2010, 40, 1423–1430. [Google Scholar] [CrossRef]
- Zerbo, O.; Qian, Y.; Yoshida, C.; Grether, J.K.; Van de Water, J.; Croen, L.A. Maternal Infection During Pregnancy and Autism Spectrum Disorders. J. Autism Dev. Disord. 2015, 45, 4015–4025. [Google Scholar] [CrossRef] [PubMed]
- Patterson, P.H. Maternal infection and immune involvement in autism. Trends Mol. Med. 2011, 17, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Choi, G.B.; Yim, Y.S.; Wong, H.; Kim, S.; Kim, H.; Kim, S.V.; Hoeffer, C.A.; Littman, D.R.; Huh, J.R. The maternal interleukin-17a pathway in mice promotes autism-like phenotypes in offspring. Science 2016, 351, 933–939. [Google Scholar] [CrossRef]
- Kim, S.; Kim, H.; Yim, Y.S.; Ha, S.; Atarashi, K.; Tan, T.G.; Longman, R.S.; Honda, K.; Littman, D.R.; Choi, G.B.; et al. Maternal gut bacteria promote neurodevelopmental abnormalities in mouse offspring. Nature 2017, 549, 528–532. [Google Scholar] [CrossRef]
- Singh, V.K.; Jensen, R.L. Elevated levels of measles antibodies in children with autism. Pediatr. Neurol. 2003, 28, 292–294. [Google Scholar] [CrossRef]
- Mankoski, R.E.; Collins, M.; Ndosi, N.K.; Mgalla, E.H.; Sarwatt, V.V.; Folstein, S.E. Etiologies of autism in a case-series from Tanzania. J. Autism Dev. Disord. 2006, 36, 1039–1051. [Google Scholar] [CrossRef] [PubMed]
- Milner, E.M.; Kariger, P.; Pickering, A.J.; Stewart, C.P.; Byrd, K.; Lin, A.; Rao, G.; Achando, B.; Dentz, H.N.; Null, C.; et al. Association between Malaria Infection and Early Childhood Development Mediated by Anemia in Rural Kenya. Int. J. Environ. Res. Public Health 2020, 17, 902. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.A.; Lees, J.A.; Gona, J.K.; Murira, G.; Rimba, K.; Neville, B.G.; Newton, C.R. Severe falciparum malaria and acquired childhood language disorder. Dev. Med. Child Neurol. 2006, 48, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Samia, P.; Kanana, M.; King, J.; Donald, K.A.; Newton, C.R.; Denckla, C. Childhood autism spectrum disorder: Insights from a tertiary hospital cohort in Kenya. Afr. J. Health Sci. 2020, 33, 12–21. [Google Scholar] [PubMed]
- Desmond, M.M.; Montgomery, J.R.; Melnick, J.L.; Cochran, G.G.; Verniaud, W. Congenital rubella encephalitis. Effects on growth and early development. Am. J. Dis. Child. 1969, 118, 30–31. [Google Scholar] [CrossRef] [PubMed]
- Chess, S. Autism in children with congenital rubella. J. Autism Child. Schizophr. 1971, 1, 33–47. [Google Scholar] [CrossRef]
- Chess, S. Follow-up report on autism in congenital rubella. J. Autism Child. Schizophr. 1977, 7, 69–81. [Google Scholar] [CrossRef] [PubMed]
- Chess, S.; Fernandez, P.; Korn, S. Behavioral consequences of congenital rubella. J. Pediatr. 1978, 93, 699–703. [Google Scholar] [CrossRef]
- Hutton, J. Does Rubella Cause Autism: A 2015 Reappraisal? Front. Hum. Neurosci. 2016, 10, 25. [Google Scholar] [CrossRef]
- Al Malki, J.S.; Hussien, N.A.; Al Malki, F. Maternal toxoplasmosis and the risk of childhood autism: Serological and molecular small-scale studies. BMC Pediatr. 2021, 21, 133. [Google Scholar] [CrossRef]
- Gentile, I.; Zappulo, E.; Bonavolta, R.; Maresca, R.; Riccio, M.P.; Buonomo, A.R.; Portella, G.; Settimi, A.; Pascotto, A.; Borgia, G.; et al. Exposure to Varicella Zoster Virus is higher in children with autism spectrum disorder than in healthy controls. Results from a case-control study. In Vivo 2014, 28, 627–631. [Google Scholar]
- Shuid, A.N.; Jayusman, P.A.; Shuid, N.; Ismail, J.; Kamal Nor, N.; Mohamed, I.N. Association between Viral Infections and Risk of Autistic Disorder: An Overview. Int. J. Environ. Res. Public Health 2021, 18, 2817. [Google Scholar] [CrossRef] [PubMed]
- Libbey, J.E.; Sweeten, T.L.; McMahon, W.M.; Fujinami, R.S. Autistic disorder and viral infections. J. Neurovirol. 2005, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Martin, W.J. Stealth virus isolated from an autistic child. J. Autism Dev. Disord. 1995, 25, 223–224. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, H.J.; Mortensen, E.L.; Reinisch, J.M.; Mednick, S.A. Association between prenatal exposure to bacterial infection and risk of schizophrenia. Schizophr. Bull. 2009, 35, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Breitschwerdt, E.B.; Greenberg, R.; Maggi, R.G.; Mozayeni, B.R.; Lewis, A.; Bradley, J.M. Bartonella henselae Bloodstream Infection in a Boy with Pediatric Acute-Onset Neuropsychiatric Syndrome. J. Cent. Nerv. Syst. Dis. 2019, 11, 1179573519832014. [Google Scholar] [CrossRef] [PubMed]
- Lashnits, E.; Maggi, R.; Jarskog, F.; Bradley, J.; Breitschwerdt, E.; Frohlich, F. Schizophrenia and Bartonella spp. Infection: A Pilot Case-Control Study. Vector Borne Zoonotic Dis. 2021, 21, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Fallon, B.A.; Nields, J.A. Lyme disease: A neuropsychiatric illness. Am. J. Psychiatry 1994, 151, 1571–1583. [Google Scholar] [CrossRef] [PubMed]
- Mattingley, D.W.; Koola, M.M. Association of Lyme Disease and Schizoaffective Disorder, Bipolar Type: Is it Inflammation Mediated? Indian J. Psychol. Med. 2015, 37, 243–246. [Google Scholar] [CrossRef]
- Roelcke, U.; Barnett, W.; Wilder-Smith, E.; Sigmund, D.; Hacke, W. Untreated neuroborreliosis: Bannwarth’s syndrome evolving into acute schizophrenia-like psychosis. A case report. J. Neurol. 1992, 239, 129–131. [Google Scholar] [CrossRef]
- Hesslinger, B.; Walden, J.; Normann, C. Acute and long-term treatment of catatonia with risperidone. Pharmacopsychiatry 2001, 34, 25–26. [Google Scholar] [CrossRef]
- Bär, K.J.; Jochum, T.; Häger, F.; Meissner, W.; Sauer, H. Painful hallucinations and somatic delusions in a patient with the possible diagnosis of neuroborreliosis. Clin. J. Pain 2005, 21, 362–363. [Google Scholar] [CrossRef] [PubMed]
- Nagy, E.E.; Rácz, A.; Urbán, E.; Terhes, G.; Berki, T.; Horváth, E.; Georgescu, A.M.; Zaharia-Kézdi, I.E. Diagnostic pitfalls in a young Romanian ranger with an acute psychotic episode. Neuropsychiatr. Dis. Treat. 2016, 12, 961–967. [Google Scholar] [CrossRef] [PubMed]
- Barnett, W.; Sigmund, D.; Roelcke, U.; Mundt, C. Endomorphes paranoid-halluzinatorisches Syndrom durch Borrelienenzephalitis [Endogenous paranoid-hallucinatory syndrome caused by Borrelia encephalitis]. Nervenarzt 1991, 62, 445–447. (In German) [Google Scholar] [PubMed]
- Hess, A.; Buchmann, J.; Zettl, U.K.; Henschel, S.; Schlaefke, D.; Grau, G.; Benecke, R. Borrelia burgdorferi central nervous system infection presenting as an organic schizophrenialike disorder. Biol. Psychiatry 1999, 45, 795. [Google Scholar] [CrossRef] [PubMed]
- Arias, I.; Sorlozano, A.; Villegas, E.; de Dios Luna, J.; McKenney, K.; Cervilla, J.; Gutierrez, B.; Gutierrez, J. Infectious agents associated with schizophrenia: A meta-analysis. Schizophr. Res. 2012, 136, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Fellerhoff, B.; Laumbacher, B.; Mueller, N.; Gu, S.; Wank, R. Associations between Chlamydophila infections, schizophrenia and risk of HLA-A10. Mol. Psychiatry 2007, 12, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Fellerhoff, B.; Wank, R. Increased prevalence of Chlamydophila DNA in post-mortem brain frontal cortex from patients with schizophrenia. Schizophr. Res. 2011, 129, 191–195. [Google Scholar] [CrossRef]
- Gutiérrez-Fernández, J.; Luna Del Castillo Jde, D.; Mañanes-González, S.; Carrillo-Ávila, J.A.; Gutiérrez, B.; Cervilla, J.A.; Sorlózano-Puerto, A. Different presence of Chlamydia pneumoniae, herpes simplex virus type 1, human herpes virus 6, and Toxoplasma gondii in schizophrenia: Meta-analysis and analytical study. Neuropsychiatr. Dis. Treat. 2015, 11, 843–852. [Google Scholar] [CrossRef]
- Tedla, Y.; Shibre, T.; Ali, O.; Tadele, G.; Woldeamanuel, Y.; Asrat, D.; Aseffa, A.; Mihret, W.; Abebe, M.; Alem, A.; et al. Serum antibodies to Toxoplasma gondii and Herpesvidae family viruses in individuals with schizophrenia and bipolar disorder: A case-control study. Ethiop. Med. J. 2011, 49, 211–220. [Google Scholar]
- Runge, K.; Balla, A.; Fiebich, B.L.; Maier, S.J.; Pankratz, B.; Schlump, A.; Nickel, K.; Dersch, R.; Domschke, K.; Tebartz van Elst, L.; et al. Antibody indices of infectious pathogens from serum and cerebrospinal fluid in patients with schizophrenia spectrum disorders. Fluids Barriers CNS 2022, 19, 61. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, F.; Jones-Brando, L.; Ford, G.; Genovese, G.; Stallings, C.; Origoni, A.; O’Dushlaine, C.; Katsafanas, E.; Sweeney, K.; Khushalani, S.; et al. Schizophrenia is Associated with an Aberrant Immune Response to Epstein-Barr Virus. Schizophr. Bull. 2019, 45, 1112–1119. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, F.; Katsafanas, E.; Origoni, A.; Squire, A.; Khushalani, S.; Newman, T.; Rowe, K.; Stallings, C.; Savage, C.L.G.; Sweeney, K.; et al. Exposure to Epstein Barr virus and cognitive functioning in individuals with schizophrenia. Schizophr. Res. 2021, 228, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Buka, S.L.; Cannon, T.D.; Torrey, E.F.; Yolken, R.H.; Collaborative Study Group on the Perinatal Origins of Severe Psychiatric Disorders. Maternal exposure to herpes simplex virus and risk of psychosis among adult offspring. Biol. Psychiatry 2008, 63, 809–815. [Google Scholar] [CrossRef] [PubMed]
- De Tiège, X.; Rozenberg, F.; Héron, B. The spectrum of herpes simplex encephalitis in children. Eur. J. Paediatr. Neurol. 2008, 12, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Schröder, J.; Nellåker, C.; Bottmer, C.; Bachmann, S.; Yolken, R.H.; Karlsson, H. Elevated levels of human endogenous retrovirus-W transcripts in blood cells from patients with first episode schizophrenia. Genes. Brain Behav. 2008, 7, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Leboyer, M.; Tamouza, R.; Charron, D.; Faucard, R.; Perron, H. Human endogenous retrovirus type W (HERV-W) in schizophrenia: A new avenue of research at the gene-environment interface. World J. Biol. Psychiatry 2013, 14, 80–90. [Google Scholar] [CrossRef]
- Yolken, R.H.; Karlsson, H.; Yee, F.; Johnston-Wilson, N.L.; Torrey, E.F. Endogenous retroviruses and schizophrenia. Brain Res. Rev. 2000, 31, 193–199. [Google Scholar] [CrossRef]
- Buka, S.L.; Tsuang, M.T.; Torrey, E.F.; Klebanoff, M.A.; Bernstein, D.; Yolken, R.H. Maternal infections and subsequent psychosis among offspring. Arch. Gen. Psychiatry 2001, 58, 1032–1037. [Google Scholar] [CrossRef]
- Mednick, S.A.; Machon, R.A.; Huttunen, M.O.; Bonett, D. Adult schizophrenia following prenatal exposure to an influenza epidemic. Arch. Gen. Psychiatry 1988, 45, 189–192. [Google Scholar] [CrossRef]
- Brown, A.S.; Begg, M.D.; Gravenstein, S.; Schaefer, C.A.; Wyatt, R.J.; Bresnahan, M.; Babulas, V.P.; Susser, E.S. Serologic evidence of prenatal influenza in the etiology of schizophrenia. Arch. Gen. Psychiatry 2004, 61, 774–780. [Google Scholar] [CrossRef]
- Gilmore, J.; Fredrik Jarskog, L.; Vadlamudi, S.; Lauder, J.M. Prenatal Infection and Risk for Schizophrenia: IL-1β, IL-6, and TNFα Inhibit Cortical Neuron Dendrite Development. Neuropsychopharmacology 2004, 29, 1221–1229. [Google Scholar] [CrossRef]
- Barr, C.E.; Mednick, S.A.; Munk-Jorgensen, P. Exposure to influenza epidemics during gestation and adult schizophrenia. A 40-year study. Arch. Gen. Psychiatry 1990, 47, 869–874. [Google Scholar] [CrossRef]
- O’Callaghan, E.; Sham, P.; Takei, N.; Glover, G.; Murray, R.M. Schizophrenia after prenatal exposure to 1957 A2 influenza epidemic. Lancet 1991, 337, 1248–1250. [Google Scholar] [CrossRef]
- Sham, P.C.; O’Callaghan, E.; Takei, N.; Murray, G.K.; Hare, E.H.; Murray, R.M. Schizophrenia following pre-natal exposure to influenza epidemics between 1939 and 1960. Br. J. Psychiatry 1992, 160, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Kępińska, A.P.; Iyegbe, C.O.; Vernon, A.C.; Yolken, R.; Murray, R.M.; Pollak, T.A. Schizophrenia and Influenza at the Centenary of the 1918-1919 Spanish Influenza Pandemic: Mechanisms of Psychosis Risk. Front. Psychiatry 2020, 11, 72. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, P.B.; Nørgaard-Pedersen, B.; Waltoft, B.L.; Sørensen, T.L.; Hougaard, D.; Torrey, E.F.; Yolken, R.H. Toxoplasma gondii as a risk factor for early-onset schizophrenia: Analysis of filter paper blood samples obtained at birth. Biol. Psychiatry 2007, 61, 688–693. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.S.; Cohen, P.; Greenwald, S.; Susser, E. Nonaffective psychosis after prenatal exposure to rubella. Am. J. Psychiatry 2000, 157, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Kotsiri, I.; Resta, P.; Spyrantis, A.; Panotopoulos, C.; Chaniotis, D.; Beloukas, A.; Magiorkinis, E. Viral Infections and Schizophrenia: A Comprehensive Review. Viruses 2023, 15, 1345. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.S.; Cohen, P.; Harkavy-Friedman, J.; Babulas, V.; Malaspina, D.; Gorman, J.M.; Susser, E.S.A.E. Bennett Research Award. Prenatal rubella, premorbid abnormalities, and adult schizophrenia. Biol. Psychiatry 2001, 49, 473–486. [Google Scholar] [CrossRef]
- Niebuhr, D.W.; Millikan, A.M.; Cowan, D.N.; Yolken, R.; Li, Y.; Weber, N.S. Selected infectious agents and risk of schizophrenia among U.S. military personnel. Am. J. Psychiatry 2008, 165, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.S.; Schaefer, C.A.; Quesenberry, C.P., Jr.; Liu, L.; Babulas, V.P.; Susser, E.S. Maternal exposure to toxoplasmosis and risk of schizophrenia in adult offspring. Am. J. Psychiatry 2005, 162, 767–773. [Google Scholar] [CrossRef] [PubMed]
- Torrey, E.F.; Bartko, J.J.; Yolken, R.H. Toxoplasma gondii and other risk factors for schizophrenia: An update. Schizophr. Bull. 2012, 38, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Rantala, M.J.; Luoto, S.; Borráz-León, J.I.; Krams, I. Schizophrenia: The new etiological synthesis. Neurosci. Biobehav. Rev. 2022, 142, 104894. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Buka, S.L.; Cannon, T.D.; Suzuki, Y.; Viscidi, R.P.; Torrey, E.F.; Yolken, R.H. Serological pattern consistent with infection with type I Toxoplasma gondii in mothers and risk of psychosis among adult offspring. Microbes Infect. 2009, 11, 1011–1018. [Google Scholar] [CrossRef] [PubMed]
- Nutile, L.M. Neurosyphilis with psychosis as the primary presentation. Am. J. Psychiatry Resid. J. 2021, 16, 6–8. [Google Scholar] [CrossRef]
- Das, S.; Kalyan, A.; Garg, K.; Thirthalli, J.; Math, S.B. A case of very early neurosyphilis presented as schizophrenia-like psychosis. Asian J. Psychiatr. 2018, 31, 92–93. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.S.; Bai, Y.M.; Hsu, J.W.; Huang, K.L.; Ko, N.Y.; Chu, H.T.; Yeh, T.C.; Tsai, S.J.; Chen, T.J.; Chen, M.H. The Risk of Sexually Transmitted Infections Following First-Episode Schizophrenia Among Adolescents and Young Adults: A Cohort Study of 220 545 Subjects. Schizophr. Bull. 2020, 46, 795–803. [Google Scholar] [CrossRef]
- Yanhua, W.; Haishan, S.; Le, H.; Xiaomei, Z.; Xinru, C.; Ling, L.; Zhangying, W.; Dong, Z.; Yuefen, Z.; Yan, T.; et al. Clinical and neuropsychological characteristics of general paresis misdiagnosed as primary psychiatric disease. BMC Psychiatry 2016, 16, 230. [Google Scholar] [CrossRef]
- Maluki, A.; Breitschwerdt, E.; Bemis, L.; Greenberg, R.; Mozayeni, B.R.; Dencklau, J.; Ericson, M. Imaging analysis of Bartonella species in the skin using single-photon and multi-photon (second harmonic generation) laser scanning microscopy. Clin. Case Rep. 2020, 8, 1564–1570. [Google Scholar] [CrossRef]
- Greenberg, R. Infections and childhood psychiatric disorders: Tick-borne illness and bipolar disorder in youth. Bipolar Disord. 2017, 3, 113. [Google Scholar] [CrossRef]
- Greenberg, R. The Role of Infection and Immune Responsiveness in a Case of Treatment-Resistant Pediatric Bipolar Disorder. Front. Psychiatry 2017, 8, 78. [Google Scholar] [CrossRef] [PubMed]
- Fallon, B.A.; Schwartzberg, M.; Bransfield, R.; Zimmerman, B.; Scotti, A.; Weber, C.A.; Liebowitz, M.R. Late-stage neuropsychiatric Lyme borreliosis. Differential diagnosis and treatment. Psychosomatics 1995, 36, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Pasareanu, A.R.; Mygland, Å.; Kristensen, Ø. A woman in her 50s with manic psychosis. Tidsskr. Nor. Legeforening 2012, 132, 537–539. (In Norwegian) [Google Scholar] [CrossRef] [PubMed]
- Fallon, B.A.; Nields, J.A.; Parsons, B.; Liebowitz, M.R.; Klein, D.F. Psychiatric manifestations of Lyme borreliosis. J. Clin. Psychiatry 1993, 54, 263–268. [Google Scholar] [PubMed]
- Frank, O.; Giehl, M.; Zheng, C.; Hehlmann, R.; Leib-Mösch, C.; Seifarth, W. Human endogenous retrovirus expression profiles in samples from brains of patients with schizophrenia and bipolar disorders. J. Virol. 2005, 79, 10890–10901. [Google Scholar] [CrossRef] [PubMed]
- Becker, M.A.; Cannon, J.; Certa, K. A Case of Mycoplasma Pneumoniae Encephalopathy Presenting as Mania. J. Acad. Consult. Liaison Psychiatry 2021, 62, 150–154. [Google Scholar] [CrossRef] [PubMed]
- D’Imperio, A.; Lo, J.; Bettini, L.; Prada, P.; Guido, B. Bipolar type I diagnosis after a manic episode secondary to SARS-CoV-2 infection: A case report. Medicine 2022, 101, e29633. [Google Scholar] [CrossRef]
- Park, J.H.; Kummerlowe, M.; Gardea Resendez, M.; Nuñez, N.A.; Almorsy, A.; Frye, M.A. First manic episode following COVID-19 infection. Bipolar Disord. 2021, 23, 847–849. [Google Scholar] [CrossRef]
- Greenberg, R. Support for a Connection Between Pediatric Bipolar Disorder and Tick-Borne Infections. J. Affect. Disord. 2023, 12, 100543. [Google Scholar] [CrossRef]
- de Barros, J.L.V.M.; Barbosa, I.G.; Salem, H.; Rocha, N.P.; Kummer, A.; Okusaga, O.O.; Soares, J.C.; Teixeira, A.L. Is there any association between Toxoplasma gondii infection and bipolar disorder? A systematic review and meta-analysis. J. Affect. Disord. 2017, 209, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Dewhurst, K. The neurosyphilitic psychoses today. A survey of 91 cases. Br. J. Psychiatry 1969, 115, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Patkar, A.A.; Pradhan, P.V.; Shah, L.P.; Lokhandwala, Y. Tertiary syphilis presenting as manic depressive psychosis. Indian J. Psychiatry 1989, 31, 261–263. [Google Scholar] [PubMed]
- Hahn, R.D.; Webster, B.; Weickhardt, G.; Thomas, E.; Timberlake, W.; Solomon, H.; Stokes, J.H.; Moore, J.E.; Heyman, A.; GAMMON, G.; et al. Penicillin treatment of general paresis (dementia paralytica): Results of treatment in 1086 patients the majority of whom were followed for more than five years. AMA Arch. Neurol. Psychiatry 1959, 81, 557–590. [Google Scholar] [CrossRef] [PubMed]
- Schaller, J.L.; Burkland, G.A.; Langhoff, P.J. Do bartonella infections cause agitation, panic disorder, and treatment-resistant depression? MedGenMed 2007, 9, 54. [Google Scholar] [PubMed]
- Flegr, J.; Preiss, M.; Balátová, P. Depressiveness and Neuroticism in Bartonella Seropositive and Seronegative Subjects-Preregistered Case-Controls Study. Front. Psychiatry 2018, 9, 314. [Google Scholar] [CrossRef] [PubMed]
- Lantos, P.M.; Maggi, R.G.; Ferguson, B.; Varkey, J.; Park, L.P.; Breitschwerdt, E.B.; Woods, C.W. Detection of Bartonella species in the blood of veterinarians and veterinary technicians: A newly recognized occupational hazard? Vector-Borne Zoonotic Dis. 2014, 14, 563–570. [Google Scholar] [CrossRef]
- Breitschwerdt, E.B.; Bradley, J.M.; Maggi, R.G.; Lashnits, E.; Reicherter, P. Bartonella Associated Cutaneous Lesions (BACL) in People with Neuropsychiatric Symptoms. Pathogens 2020, 9, 1023. [Google Scholar] [CrossRef]
- Logigian, E.L.; Kaplan, R.F.; Steere, A.C. Chronic neurologic manifestations of Lyme disease. N. Engl. J. Med. 1990, 323, 1438–1444. [Google Scholar] [CrossRef]
- Hündersen, F.; Forst, S.; Kasten, E. Neuropsychiatric and Psychological Symptoms in Patients with Lyme Disease: A Study of 252 Patients. Healthcare 2021, 9, 733. [Google Scholar] [CrossRef]
- Omasits, M.; Seiser, A.; Brainin, M. Zur rezidivierenden und schubhaft verlaufenden Borreliose des Nervensystems [Recurrent and relapsing course of borreliosis of the nervous system]. Wien. Klin. Wochenschr. 1990, 102, 4–12. (In German) [Google Scholar] [PubMed]
- Garakani, A.; Mitton, A.G. New-onset panic, depression with suicidal thoughts, and somatic symptoms in a patient with a history of lyme disease. Case Rep. Psychiatry 2015, 2015, 457947. [Google Scholar] [CrossRef] [PubMed]
- Blum, K.; Modestino, E.J.; Febo, M.; Steinberg, B.; McLaughlin, T.; Fried, L.; Baron, D.; Siwicki, D.; Badgaiyan, R.D. Lyme and Dopaminergic Function: Hypothesizing Reduced Reward Deficiency Symptomatology by Regulating Dopamine Transmission. J. Syst. Integr. Neurosci. 2017, 3. [Google Scholar] [CrossRef] [PubMed]
- Reik, L.; Steere, A.C.; Bartenhagen, N.H.; Shope, R.E.; Malawista, S.E. Neurologic abnormalities of Lyme disease. Medicine 1979, 58, 281–294. [Google Scholar] [CrossRef] [PubMed]
- Doshi, S.; Keilp, J.G.; Strobino, B.; McElhiney, M.; Rabkin, J.; Fallon, B.A. Depressive Symptoms and Suicidal Ideation Among Symptomatic Patients with a History of Lyme Disease vs Two Comparison Groups. Psychosomatics 2018, 59, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Del Guerra, F.B.; Fonseca, J.L.; Figueiredo, V.M.; Ziff, E.B.; Konkiewitz, E.C. Human immunodeficiency virus-associated depression: Contributions of immuno-inflammatory, monoaminergic, neurodegenerative, and neurotrophic pathways. J. Neurovirol. 2013, 19, 314–327. [Google Scholar] [CrossRef] [PubMed]
- Gopinathan, V.P.; Thampi, U.R.; Ganguly, S.B. Neuropsychiatric manifestations of falciparum malaria. J. Indian Med. Assoc. 1982, 78, 155–157. [Google Scholar]
- Prakash, M.V.; Stein, G. Malaria presenting as atypical depression. Br. J. Psychiatry 1990, 156, 594–595. [Google Scholar] [CrossRef]
- Mazza, M.G.; De Lorenzo, R.; Conte, C.; Poletti, S.; Vai, B.; Bollettini, I.; Melloni, E.M.T.; Furlan, R.; Ciceri, F.; Rovere-Querini, P.; et al. Anxiety and depression in COVID-19 survivors: Role of inflammatory and clinical predictors. Brain Behav. Immun. 2020, 89, 594–600. [Google Scholar] [CrossRef]
- Murray, K.O.; Resnick, M.; Miller, V. Depression after infection with West Nile virus. Emerg. Infect. Dis. 2007, 13, 479–481. [Google Scholar] [CrossRef]
- Sherr, V.T. Panic attacks may reveal previously unsuspected chronic disseminated Lyme disease. J. Psychiatr. Pract. 2000, 6, 352–356. [Google Scholar] [CrossRef] [PubMed]
- Johnco, C.; Kugler, B.B.; Murphy, T.K.; Storch, E.A. Obsessive-compulsive symptoms in adults with Lyme disease. Gen. Hosp. Psychiatry 2018, 51, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Fagundes, C.P.; Jaremka, L.M.; Glaser, R.; Alfano, C.M.; Povoski, S.P.; Lipari, A.M.; Agnese, D.M.; Yee, L.D.; Carson, W.E., 3rd; Farrar, W.B.; et al. Attachment anxiety is related to Epstein-Barr virus latency. Brain Behav. Immun. 2014, 41, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Murphy, T.K.; Patel, P.D.; McGuire, J.F.; Kennel, A.; Mutch, P.J.; Parker-Athill, E.C.; Hanks, C.E.; Lewin, A.B.; Storch, E.A.; Toufexis, M.D.; et al. Characterization of the pediatric acute-onset neuropsychiatric syndrome phenotype. J. Child Adolesc. Psychopharmacol. 2015, 25, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Frankovich, J.; Thienemann, M.; Rana, S.; Chang, K. Five youth with pediatric acute-onset neuropsychiatric syndrome of differing etiologies. J. Child Adolesc. Psychopharmacol. 2015, 25, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Saltzman, L.Y.; Longo, M.; Hansel, T.C. Long-COVID stress symptoms: Mental health, anxiety, depression, or posttraumatic stress. Psychol. Trauma Theory Res. Pract. Policy 2023. Epub ahad of print. [Google Scholar] [CrossRef]
- Chang, K.; Frankovich, J.; Cooperstock, M.; Cunningham, M.W.; Latimer, M.E.; Murphy, T.K.; Pasternack, M.; Thienemann, M.; Williams, K.; Walter, J.; et al. Clinical evaluation of youth with pediatric acute-onset neuropsychiatric syndrome (PANS): Recommendations from the 2013 PANS Consensus Conference. J. Child Adolesc. Psychopharmacol. 2015, 25, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Lund-Sørensen, H.; Benros, M.E.; Madsen, T.; Sørensen, H.J.; Eaton, W.W.; Postolache, T.T.; Nordentoft, M.; Erlangsen, A. A nationwide cohort study of the association between hospitalization with infection and risk of death by suicide. JAMA Psychiatry 2016, 73, 912–919. [Google Scholar] [CrossRef] [PubMed]
- Bransfield, R.C. Suicide and Lyme and associated diseases. Neuropsychiatr. Dis. Treat. 2017, 13, 1575–1587. [Google Scholar] [CrossRef]
- Bransfield, R.C.; Embers, M.E.; Dwork, A.J. A Fatal Case of Late Stage Lyme Borreliosis and Substance Abuse. 2023 Psychoimmunology Experts Meeting abstract. J. Affect. Disord. 2023, 12, 100525. [Google Scholar] [CrossRef]
- Lucaciu, L.A.; Dumitrascu, D.L. Depression and suicide ideation in chronic hepatitis C patients untreated and treated with interferon: Prevalence, prevention, and treatment. Ann. Gastroenterol. 2015, 28, 440–447. [Google Scholar]
- Nissen, J.; Trabjerg, B.; Pedersen, M.G.; Banasik, K.; Pedersen, O.B.; Sørensen, E.; Nielsen, K.R.; Erikstrup, C.; Petersen, M.S.; Paarup, H.M.; et al. Herpes Simplex Virus Type 1 infection is associated with suicidal behavior and first registered psychiatric diagnosis in a healthy population. Psychoneuroendocrinology 2019, 108, 150–154. [Google Scholar] [CrossRef]
- Pelton, M.; Ciarletta, M.; Wisnousky, H.; Lazzara, N.; Manglani, M.; Ba, D.M.; Chinchillli, V.M.; Du, P.; Ssentongo, A.E.; Ssentongo, P. Rates and risk factors for suicidal ideation, suicide attempts and suicide deaths in persons with HIV: A systematic review and meta-analysis. Gen. Psychiatr. 2021, 34, e100247. [Google Scholar] [CrossRef] [PubMed]
- Okusaga, O.; Yolken, R.H.; Langenberg, P.; Lapidus, M.; Arling, T.A.; Dickerson, F.B.; Scrandis, D.A.; Severance, E.; Cabassa, J.A.; Balis, T.; et al. Association of seropositivity for influenza and coronaviruses with history of mood disorders and suicide attempts. J. Affect. Disord. 2011, 130, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Y.; Du, X. Trends and prevalence of suicide 2017–2021 and its association with COVID-19: Interrupted time series analysis of a national sample of college students in the United States. Psychiatry Res. 2022, 14, 114796. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.J.; Yang, J.W.; Lee, S.; Kim, J.Y.; Oh, J.W.; Lee, J.; Stubbs, B.; Lee, K.H.; Koyanagi, A.; Hong, S.H.; et al. Suicide associated with COVID-19 infection: An immunological point of view. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 6397–6407. [Google Scholar] [CrossRef] [PubMed]
- Latimer, M.E.; L’Etoile, N.; Seidlitz, J.; Swedo, S.E. Therapeutic plasma apheresis as a treatment for 35 severely ill children and adolescents with pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections. J. Child Adolesc. Psychopharmacol. 2015, 25, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Kamal, A.M.; Kamal, A.M.; Abd El-Fatah, A.S.; Rizk, M.M.; Hassan, E.E. Latent Toxoplasmosis is Associated with Depression and Suicidal Behavior. Arch. Suicide Res. 2022, 26, 819–830. [Google Scholar] [CrossRef] [PubMed]
- Bransfield, R.C. Aggressiveness, violence, homicidality, homicide, and Lyme disease. Neuropsychiatr. Dis. Treat. 2018, 14, 693–713. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, R. Aggressiveness, violence, homicidality, homicide, and Lyme disease. Neuropsychiatr. Dis. Treat. 2018, 14, 1253–1254. [Google Scholar] [CrossRef]
- Auden, G.A. Behaviour changes supervening upon encephalitis in children. Lancet 1922, 200, 901–904. [Google Scholar] [CrossRef]
- Ruiz, V. ‘A disease that makes criminals’: Encephalitis lethargica (EL) in children, mental deficiency, and the 1927 Mental Deficiency Act. Endeavour 2015, 39, 44–51. [Google Scholar] [CrossRef]
- Cottu, A.; Kante, A.; Megherbi, A.; Lhomme, S.; Maisonneuve, L.; Santoli, F. A frantic confusion: Beyond rabies and anti-N-methyl-D-aspartate encephalitis. J. Neurovirol. 2023, 29, 358–363. [Google Scholar] [CrossRef]
- Greenwood, R.; Bhalla, A.; Gordon, A.; Roberts, J. Behaviour disturbances during recovery from herpes simplex encephalitis. J. Neurol. Neurosurg. Psychiatry 1983, 46, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Shannon, T.E.; Griffin, S.L. Managing aggression in global amnesia following herpes simplex virus encephalitis: The case of E.B. Brain Inj. 2015, 29, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Blomström, Å.; Kosidou, K.; Kristiansson, M.; Masterman, T. Infection during childhood and the risk of violent criminal behavior in adulthood. Brain Behav. Immun. 2020, 86, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Piras, C.; Pintus, R.; Pruna, D.; Dessì, A.; Atzori, L.; Fanos, V. Pediatric Acute-onset Neuropsychiatric Syndrome and Mycoplasma Pneumoniae Infection: A Case Report Analysis with a Metabolomics Approach. Curr. Pediatr. Rev. 2020, 16, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Ssenkusu, J.M.; Hodges, J.S.; Opoka, R.O.; Idro, R.; Shapiro, E.; John, C.C.; Bangirana, P. Long-term Behavioral Problems in Children with Severe Malaria. Pediatrics 2016, 138, e20161965, Erratum in Pediatrics 2017, 140, e20172709. [Google Scholar] [CrossRef] [PubMed]
- Chipman, M.; Cadigan, F.C., Jr.; Benjapongse, W. Involvement of the nervous system in malaria in Thailand. Trop. Geogr. Med. 1967, 19, 8–14. [Google Scholar] [PubMed]
- Jackson, A.C. Diabolical effects of rabies encephalitis. J. Neurovirol. 2016, 22, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Dimaano, E.M.; Scholand, S.J.; Alera, M.T.; Belandres, D.B. Clinical and epidemiological features of human rabies cases in the Philippines: A review from 1987 to 2006. Int. J. Infect. Dis. 2011, 15, e495–e499. [Google Scholar] [CrossRef]
- Duarte, N.F.H.; Pires Neto, R.D.J.; Viana, V.F.; Feijão, L.X.; Alencar, C.H.; Heukelbach, J. Clinical aspects of human rabies in the state of Ceará, Brazil: An overview of 63 cases. Rev. Soc. Bras. Med. Trop. 2021, 54, e01042021. [Google Scholar] [CrossRef] [PubMed]
- Coccaro, E.F.; Lee, R.; Groer, M.W.; Can, A.; Coussons-Read, M.; Postolache, T.T. Toxoplasma gondii infection: Relationship with aggression in psychiatric subjects. J. Clin. Psychiatry 2016, 77, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Saini, H.S.; Sayre, M.; Saini, I.; Elsharkawy, N. Neurosyphilis Presenting as Intermittent Explosive Disorder and Acute Psychosis. Cureus 2019, 11, e6337. [Google Scholar] [CrossRef] [PubMed]
- Taki El-Din, Z.; Iqbal, H.; Sharma, A. Neurosyphilis-Induced Psychosis: A Unique Presentation of Syphilis with a Primary Psychiatric Manifestation. Cureus 2023, 15, e36080. [Google Scholar] [CrossRef] [PubMed]
- Deka, K.; Bhuyan, D.; Chaudhury, P.K. Conduct disorder-A sequelae of viral encephalitis. Indian J. Psychiatry 2006, 48, 258–259. [Google Scholar] [CrossRef] [PubMed]
- Goswani, N. Tour of Duty Ends for Dog. Bennington Banner. 2006. Available online: http://www.benningtonbanner.com/stories/tour-of-duty-ends-for-dog,257240 (accessed on 27 January 2023).
- Bishop, B.L.; Cherry, N.A.; Hegarty, B.C.; Breitschwerdt, E.B. Enrichment blood culture isolation of Bartonella henselae from horses with chronic circulatory, musculoskeletal and/or neurologic deficits. Adv. Biotechnol. Microbiol. 2017, 4, 555646. [Google Scholar]
- CBSNews CBS/AP. Chimp Shot Dead after Attacking Woman. 2009. Available online: www.cbsnews.com/news/chimp-shot-dead-after-attacking-woman (accessed on 27 January 2023).
- Christoffersen, J.; Easton Robb, P. Huge Chimp Shot Dead after Mauling Woman. Associated Press. Available online: https://www.nhregister.com/news/article/Huge-chimp-shot-dead-after-mauling-woman-11635518.php (accessed on 27 January 2023).
- Kirchoff, N.S.; Udell, M.A.R.; Sharpton, T.J. The gut microbiome correlates with conspecific aggression in a small population of rescued dogs (Canis familiaris). PeerJ 2019, 7, e6103. [Google Scholar] [CrossRef]
- Mach, N.; Ruet, A.; Clark, A.; Bars-Cortina, D.; Ramayo-Caldas, Y.; Crisci, E.; Pennarun, S.; Dhorne-Pollet, S.; Foury, A.; Moisan, M.P.; et al. Priming for welfare: Gut microbiota is associated with equitation conditions and behavior in horse athletes. Sci. Rep. 2020, 10, 8311. [Google Scholar] [CrossRef]
- Winkler, W.G.; Schneider, N.J.; Jennings, W.L. Experimental rabies infection in wild rodents. J. Wildl. Dis. 1972, 8, 99–103. [Google Scholar] [CrossRef]
- Rabhi, N.; Thibodeau, A.; Côté, J.C.; Devillers, N.; Laplante, B.; Fravalo, P.; Larivière-Gauthier, G.; Thériault, W.P.; Faucitano, L.; Beauchamp, G.; et al. Association Between Tail-Biting and Intestinal Microbiota Composition in Pigs. Front. Vet. Sci. 2020, 7, 563762. [Google Scholar] [CrossRef]
- Homer, B.; Judd, J.; Mohammadi Dehcheshmeh, M.; Ebrahimie, E.; Trott, D.J. Gut Microbiota and Behavioural Issues in Production, Performance, and Companion Animals: A Systematic Review. Animals 2023, 13, 1458. [Google Scholar] [CrossRef] [PubMed]
- Mondo, E.; Barone, M.; Soverini, M.; D’Amico, F.; Cocchi, M.; Petrulli, C.; Mattioli, M.; Marliani, G.; Candela, M.; Accorsi, P.A. Gut microbiome structure and adrenocortical activity in dogs with aggressive and phobic behavioral disorders. Heliyon 2020, 6, e03311. [Google Scholar] [CrossRef] [PubMed]
- Craddock, H.A.; Godneva, A.; Rothschild, D.; Motro, Y.; Grinstein, D.; Lotem-Michaeli, Y.; Narkiss, T.; Segal, E.; Moran-Gilad, J. Phenotypic correlates of the working dog microbiome. NPJ Biofilms Microbiomes 2022, 8, 66. [Google Scholar] [CrossRef] [PubMed]
- Faria, M.A., Jr. Violence, mental illness, and the brain—A brief history of psychosurgery: Part 1—From trephination to lobotomy. Surg. Neurol. Int. 2013, 4, 49. [Google Scholar] [CrossRef] [PubMed]
- The History of Schizophrenia. Schizophrenia.com. Available online: http://schizophrenia.com/history.htm (accessed on 22 August 2022).
- Beck, J. Diagnosing Metal illness in ancient Greece and Rome. The Atlantic. 2014. Available online: https://www.theatlantic.com/health/archive/2014/01/diagnosing-mental-illness-in-ancient-greece-and-rome/282856/ (accessed on 26 August 2022).
- Szasz, T.S. The myth of mental illness. Am. Psychol. 1960, 15, 113–118. [Google Scholar] [CrossRef]
- Schoeneman, T.J. The role of mental illness in the European witch hunts of the sixteenth and seventeenth centuries: An assessment. J. Hist. Behav. Sci. 1977, 13, 337–351. [Google Scholar] [CrossRef] [PubMed]
- Zilboorg, G.; Henry, G.W. A History of Medical Psychology; W.W. Norton & Company Inc.: New York, NY, USA, 1941. [Google Scholar]
- Montague, J. Can an Auto-Immune Illness Explain the Salem Witch Trials? 2019. Available online: https://www.bbc.com/future/article/20181221-can-an-auto-immune-illness-explain-the-salem-witch-trials (accessed on 26 August 2022).
- Tam, J.; Zandi, M.S. The witchcraft of encephalitis in Salem. J. Neurol. 2017, 264, 1529–1531. [Google Scholar] [CrossRef]
- Drymon, M.M. Disguised as the Devil: How Lyme Disease Created Witches and Changed History; Wythe Avenue Press: New York, NY, USA, 2008. [Google Scholar]
- Arens, K.; Griesinger, W. Psychiatry between Philosophy and Praxis. Project MUSE. Philos. Psychiatry Psychol. 1996, 3, 147–163. [Google Scholar] [CrossRef]
- Parry, M.S. Dorothea Dix (1802–1887). Am. J. Public Health 2006, 96, 624–625. [Google Scholar] [CrossRef]
- Scull, A. Madhouse in Civilization; Princeton University Press: Princeton, NJ, USA, 2016. [Google Scholar]
- Schildkraut, J.J. The Catecholamine Hypothesis of Affective Disorders: A Review of Supporting Evidence. Am. J. Psychiatry 1965, 122, 509–522. [Google Scholar] [CrossRef]
- Williams, G.; Nesse, R. The dawn of Darwinian medicine. Q. Rev. Biol. 1991, 66, 1–22. [Google Scholar] [CrossRef] [PubMed]
- CDC. What Is Epigenetics? Available online: https://www.cdc.gov/genomics/disease/epigenetics.htm (accessed on 18 December 2022).
- Ewald, P.W. Evolution of virulence. Infect. Dis. Clin. N. Am. 2004, 18, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Sines, G.; Sakellarakis, Y.A. Lenses in antiquity. Am. J. Archaeol. 1987, 91, 191–196. [Google Scholar] [CrossRef]
- Da Vinci, L. Design for a Machine for Grinding Convex Lenses. Available online: https://www.leonardo-da-vinci.net/design-for-a-machine-for-grinding-convex-lenses (accessed on 8 January 2023).
- Gest, H. The discovery of microorganisms by Robert Hooke and Antoni Van Leeuwenhoek, fellows of the Royal Society. Notes Rec. R. Soc. Lond. 2004, 58, 187–201. [Google Scholar] [CrossRef] [PubMed]
- Schultz, M. Rudolf Virchow. Emerg. Infect. Dis. 2008, 14, 1480–1481. [Google Scholar] [CrossRef]
- Health and the People: Germ Theory. Available online: https://healthandthepeople.ncl.ac.uk/germ-theory/ (accessed on 8 January 2023).
- Wagner, M. Infected with Insanity. Sci. Am. Mind 2008, 19, 40–47. [Google Scholar] [CrossRef]
- Sefton, A.M. The Great Pox that was… syphilis. J. Appl. Microbiol. 2001, 91, 592–596. [Google Scholar] [CrossRef]
- The Stanley Neurovirology Laboratory of the Johns Hopkins University School of Medicine. Available online: https://www.stanleylab.org/ (accessed on 27 November 2022).
- PubMed Search Microbes + [Mental Illness]. Available online: https://www.ncbi.nlm.nih.gov/pmc/?term=microbes+%2B+%5Bmental+illness%5D (accessed on 22 April 2023).
- Huber, M.; Knottnerus, J.A.; Green, L.; van der Horst, H.; Jadad, A.R.; Kromhout, D.; Leonard, B.; Lorig, K.; Loureiro, M.I.; van der Meer, J.W.; et al. How should we define health? BMJ 2011, 343, d4163. [Google Scholar] [CrossRef]
- Kleinman, A.; Eisenberg, L.; Good, B. Culture, illness and care. Clinical lessons from anthropologic and cross-cultural research. Ann. Intern. Med. 1978, 88, 251–258. [Google Scholar] [CrossRef]
- Kleinman, A. The meaning of symptoms and disorders. In The Illness Narratives; Basic Books: New York, NY, USA, 1988 1988; p. 3. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; Text Revision; American Psychiatric Publishing: Arlington, VA, USA, 2022. [Google Scholar]
- Galderisi, S.; Heinz, A.; Kastrup, M.; Beezhold, J.; Sartorius, N. Toward a new definition of mental health. World Psychiatry 2015, 14, 231–233. [Google Scholar] [CrossRef]
- CDC. Centers for Disease Control and Prevention, National Center for Chronic Diseases and Health Promotion (NCCDPHP). About Chronic Diseases. Available online: https://www.cdc.gov/chronicdisease/about/index.htm (accessed on 26 August 2022).
- Bransfield, R.C. Systems Theory. Presented at Sheppard and Enoch Pratt Scientific Day, 1974, Baltimore, MD, USA. Available online: https://www.mentalhealthandillness.com/system_theory.html (accessed on 26 August 2022).
- Nesse, R.M. Darwinian Medicine. Encyclopedia Britannica. 2019. Available online: https://www.britannica.com/science/Darwinian-medicine (accessed on 13 August 2022).
- Ewald, P.W. The evolution of virulence and emerging diseases. J. Urban Health 1998, 75, 480–491. [Google Scholar] [CrossRef]
- Robinson-Agramonte, M.d.l.A.; Noris García, E.; Fraga Guerra, J.; Vega Hurtado, Y.; Antonucci, N.; Semprún-Hernández, N.; Schultz, S.; Siniscalco, D. Immune Dysregulation in Autism Spectrum Disorder: What Do We Know about It? Int. J. Mol. Sci. 2022, 23, 3033. [Google Scholar] [CrossRef]
- Khandaker, G.M.; Cousins, L.; Deakin, J.; Lennox, B.R.; Yolken, R.; Jones, P.B. Inflammation and immunity in schizophrenia: Implications for pathophysiology and treatment. Lancet Psychiatry 2015, 2, 258–270. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, F.; Severance, E.; Yolken, R. The microbiome, immunity, and schizophrenia and bipolar disorder. Brain Behav. Immun. 2017, 62, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Marrie, R.A.; Walld, R.; Bolton, J.M.; Sareen, J.; Walker, J.R.; Patten, S.B.; Singer, A.; Lix, L.M.; Hitchon, C.A.; El-Gabalawy, R.; et al. Increased incidence of psychiatric disorders in immune-mediated inflammatory disease. J. Psychosom. Res. 2017, 101, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Müller, N.; Schwarz, M.J. The immune-mediated alteration of serotonin and glutamate: Towards an integrated view of depression. Mol. Psychiatry 2007, 12, 988–1000. [Google Scholar] [CrossRef] [PubMed]
- Furtado, M.; Katzman, M.A. Neuroinflammatory pathways in anxiety, posttraumatic stress, and obsessive compulsive disorders. Psychiatry Res. 2015, 229, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Jansson, S.; Malham, M.; Wewer, V.; Rask, C.U. Psychiatric comorbidity in childhood onset immune-mediated diseases—A systematic review and meta-analysis. Acta Paediatr. 2022, 111, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Najjar, S.; Pearlman, D.M.; Alper, K.; Najjar, A.; Devinsky, O. Neuroinflammation and psychiatric illness. J. Neuroinflamm. 2013, 10, 816. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.M.; Boyle, M.F. Delirium. BMJ 2002, 325, 644–647. [Google Scholar] [CrossRef]
- Loewenstein, R.J.; Sharfstein, S.S. Neuropsychiatric aspects of acquired immune deficiency syndrome. Int. J. Psychiatry Med. 1984, 13, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Anthony, S.J.; Epstein, J.H.; Murray, K.A.; Navarrete-Macias, I.; Zambrana-Torrelio, C.M.; Solovyov, A.; Ojeda-Flores, R.; Arrigo, N.C.; Islam, A.; Ali Khan, S.; et al. A strategy to estimate unknown viral diversity in mammals. mBio 2013, 4, e00598-13. [Google Scholar] [CrossRef] [PubMed]
- Short, E.E.; Caminade, C.; Thomas, B.N. Climate Change Contribution to the Emergence or Re-Emergence of Parasitic Diseases. Infect. Dis. 2017, 10, 1178633617732296. [Google Scholar] [CrossRef] [PubMed]
- Bransfield, R.C. Did Infections Caused by World War I Contribute to Causing World War II? ContagionLive. 5 January 2018. Available online: https://www.contagionlive.com/view/did-infections-caused-by-world-war-i-contribute-to-causing-world-war-ii (accessed on 18 December 2022).
- Kuodi, P.; Gorelik, Y.; Edelstein, M. Characterisation of the long-term physical and mental health consequences of SARS-CoV-2 infection: A systematic review and meta-analysis protocol. PLoS ONE 2022, 17, e0266232. [Google Scholar] [CrossRef] [PubMed]
- Embers, M.E.; Ramamoorthy, R.; Philipp, M.T. Survival strategies of Borrelia burgdorferi, the etiologic agent of Lyme disease. Microbes Infect. 2004, 6, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Rogovskyy, A.S.; Gillis, D.C.; Ionov, Y.; Gerasimov, E.; Zelikovsky, A. Antibody Response to Lyme Disease Spirochetes in the Context of VlsE-Mediated Immune Evasion. Infect. Immun. 2016, 85, e00890-16. [Google Scholar] [CrossRef] [PubMed]
- Berndtson, K. Review of evidence for immune evasion and persistent infection in Lyme disease. Int. J. Gen. Med. 2013, 6, 291–306. [Google Scholar] [CrossRef]
- Elsner, R.A.; Hastey, C.J.; Olsen, K.J.; Baumgarth, N. Suppression of Long-Lived Humoral Immunity Following Borrelia burgdorferi Infection. PLoS Pathog. 2015, 11, e1004976. [Google Scholar] [CrossRef]
- Ford, L.; Tufts, D.M. Lyme Neuroborreliosis: Mechanisms of B. burgdorferi Infection of the Nervous System. Brain Sci. 2021, 11, 789. [Google Scholar] [CrossRef]
- Cabello, F.C.; Godfrey, H.P.; Newman, S.A. Hidden in plain sight: Borrelia burgdorferi and the extracellular matrix. Trends Microbiol. 2007, 15, 350–354. [Google Scholar] [CrossRef]
- Wormser, G.P.; Dattwyler, R.J.; Shapiro, E.D.; Halperin, J.J.; Steere, A.C.; Klempner, M.S.; Krause, P.J.; Bakken, J.S.; Strle, F.; Stanek, G.; et al. The clinical assessment, treatment, and prevention of lyme disease, human granulocytic anaplasmosis, and babesiosis: Clinical practice guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2006, 43, 1089–1134. [Google Scholar] [CrossRef]
- Virolainen, S.J.; VonHandorf, A.; Viel, K.C.; Weirauch, M.T.; Kottyan, L.C. Gene–environment interactions and their impact on human health. Genes. Immun. 2023, 24, 1–11. [Google Scholar] [CrossRef]
- Yolken, R.; Torrey, E.F.; Dickerson, F. Neuropsychiatric Consequences of Viral Infections-Focus on SARS2 and Other Coronaviruses. Available online: https://neuroimmune.org/wp-content/uploads/2022/05/yolken.pdf (accessed on 26 August 2022).
- Sanchez-Vicente, S.; Tagliafierro, T.; Coleman, J.L.; Benach, J.L.; Tokarz, R. Polymicrobial Nature of Tick-Borne Diseases. mBio 2019, 10, e02055-19. [Google Scholar] [CrossRef] [PubMed]
- Berghoff, W. Chronic Lyme Disease and Co-infections: Differential Diagnosis. Open Neurol. J. 2012, 6, 158–178. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Oertle, J.; Warren, D.; Prato, D. Chronic Lyme Disease Complex and Its Commonly Undiagnosed Primary and Secondary Co-Infections. Open J. Med. Microbiol. 2015, 5, 143–158. [Google Scholar] [CrossRef]
- Nicolson Nicolson Haier Chronic fatigue syndrome patients subsequently diagnosed with Lyme disease Borrelia burgdorferi: Evidence for Mycoplasma species coinfections. J. Chronic Fatigue Syndr. 2008, 14, 5–17. [CrossRef]
- Grab, D.J.; Nyarko, E.; Barat, N.C.; Nikolskaia, O.V.; Dumler, J.S. Anaplasma phagocytophilum-Borrelia burgdorferi coinfection enhances chemokine, cytokine, and matrix metalloprotease expression by human brain microvascular endothelial cells. Clin. Vaccine Immunol. 2007, 14, 1420–1424. [Google Scholar] [CrossRef] [PubMed]
- Jarefors, S.; Karlsson, M.; Forsberg, P.; Eliasson, I.; Ernerudh, J.; Ekerfelt, C. Reduced number of interleukin-12 secreting cells in patients with Lyme borreliosis previously exposed to Anaplasma phagocytophilum. Clin. Exp. Immunol. 2006, 143, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Djokic, V.; Akoolo, L.; Primus, S.; Schlachter, S.; Kelly, K.; Bhanot, P.; Parveen, N. Protozoan Parasite Babesia microti Subverts Adaptive Immunity and Enhances Lyme Disease Severity. Front. Microbiol. 2019, 10, 1596. [Google Scholar] [CrossRef]
- Bransfield, R.C. A Tale of Two Pandemics: Lyme and COVID-19. In Proceedings of the 2021 ILADS Scientific Conference, Orlando, FL, USA, 16 October 2021. [Google Scholar]
- Szewczyk-Dąbrowska, A.; Budziar, W.; Harhala, M.; Baniecki, K.; Pikies, A.; Jędruchniewicz, N.; Kaźmierczak, Z.; Gembara, K.; Klimek, T.; Witkiewicz, W.; et al. Correlation between COVID-19 severity and previous exposure of patients to Borrelia spp. Sci. Rep. 2022, 12, 15944. [Google Scholar] [CrossRef] [PubMed]
- Goswami, A.; Wendt, F.R.; Pathak, G.A.; Tylee, D.S.; De Angelis, F.; De Lillo, A.; Polimanti, R. Role of microbes in the pathogenesis of neuropsychiatric disorders. Front. Neuroendocrinol. 2021, 62, 100917. [Google Scholar] [CrossRef]
- Bull, M.J.; Plummer, N.T. Part 1: The Human Gut Microbiome in Health and Disease. Integr. Med. 2014, 13, 17–22. [Google Scholar]
- Imai, D.M.; Feng, S.; Hodzic, E.; Barthold, S.W. Dynamics of connective-tissue localization during chronic Borrelia burgdorferi infection. Lab. Investig. 2013, 93, 900–910. [Google Scholar] [CrossRef] [PubMed]
- Bockenstedt, L.K.; Gonzalez, D.G.; Haberman, A.M.; Belperron, A.A. Spirochete antigens persist near cartilage after murine Lyme borreliosis therapy. J. Clin. Investig. 2012, 122, 2652–2660. [Google Scholar] [CrossRef] [PubMed]
- Eisenstein, M. The skin microbiome and its relationship with the human body explained. Nature 2020, 588, S210–S211. [Google Scholar] [CrossRef] [PubMed]
- Scholthof, K.B. The disease triangle: Pathogens, the environment and society. Nat. Rev. Microbiol. 2007, 5, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Dorfman, K. The Total Load Theory: Why So Many Children Have Developmental Problems. Available online: https://epidemicanswers.org/total-load-theory-why-so-many-children-have-developmental-problems/ (accessed on 18 December 2022).
- Bransfield, R.C. Relationship of Inflammation and Autoimmunity to Psychiatric Sequelae in Lyme Disease. Psychiatr. Ann. 2012, 42, 337–341. [Google Scholar] [CrossRef]
- Fallon, B.A.; Levin, E.S.; Schweitzer, P.J.; Hardesty, D. Inflammation and central nervous system Lyme disease. Neurobiol. Dis. 2010, 37, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, T.; Kawai, T. Toll-like receptor signaling pathways. Front. Immunol. 2014, 5, 461. [Google Scholar] [CrossRef]
- Pizzino, G.; Irrera, N.; Cucinotta, M.; Pallio, G.; Mannino, F.; Arcoraci, V.; Squadrito, F.; Altavilla, D.; Bitto, A. Oxidative Stress: Harms and Benefits for Human Health. Oxid. Med. Cell Longev. 2017, 2017, 8416763. [Google Scholar] [CrossRef]
- Burke, H.M.; Davis, M.C.; Otte, C.; Mohr, D.C. Depression and cortisol responses to psychological stress: A meta-analysis. Psychoneuroendocrinology 2005, 30, 846–856. [Google Scholar] [CrossRef]
- Somani, A.; Singh, A.K.; Gupta, B.; Nagarkoti, S.; Dalal, P.K.; Dikshit, M. Oxidative and Nitrosative Stress in Major Depressive Disorder: A Case Control Study. Brain Sci. 2022, 12, 144. [Google Scholar] [CrossRef] [PubMed]
- Halperin, J.J.; Heyes, M.P. Neuroactive kynurenines in Lyme borreliosis. Neurology 1992, 42, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Gasse, T.; Murr, C.; Meyersbach, P.; Schmutzhard, E.; Wachter, H.; Fuchs, D. Neopterin production and tryptophan degradation in acute Lyme neuroborreliosis versus late Lyme encephalopathy. Eur. J. Clin. Chem. Clin. Biochem. 1994, 32, 685–689. [Google Scholar] [CrossRef] [PubMed]
- Gasse, T.; Widner, B.; Baier-Bitterlich, G.; Sperner-Unterweger, B.; Leblhuber, F.; Wachter, H.; Fuchs, D. Abnormal tryptophan metabolism, neurologic/psychiatric disturbances and its relationship to immune activation. In Neurochemical Markers of Degenerative Nervous Diseases and Drug Addiction, Progress in HPLC-HPCE, 7th ed.; Qureshi, G.A., Parvez, H., Caudy, P., Parvez, S., Eds.; Ridderprint BV: Ridderkerk, The Netherlands, 1998. [Google Scholar]
- Wirleitner, B.; Neurauter, G.; Schröcksnadel, K.; Frick, B.; Fuchs, D. Interferon-gamma-induced conversion of tryptophan: Immunologic and neuropsychiatric aspects. Curr. Med. Chem. 2003, 10, 1581–1591. [Google Scholar] [CrossRef] [PubMed]
- Myint, A.M. Kynurenines: From the perspective of major psychiatric disorders. FEBS J. 2012, 279, 1375–1385. [Google Scholar] [CrossRef] [PubMed]
- Iliff, J.J.; Wang, M.; Liao, Y.; Plogg, B.A.; Peng, W.; Gundersen, G.A.; Benveniste, H.; Vates, G.E.; Deane, R.; Goldman, S.A.; et al. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid β. Sci. Transl. Med. 2012, 4, 147ra111. [Google Scholar] [CrossRef] [PubMed]
- Nedergaard, M. Neuroscience. Garbage truck of the brain. Science 2013, 340, 1529–1530. [Google Scholar] [CrossRef]
- Ibarra-Coronado, E.G.; Pantaleón-Martínez, A.M.; Velazquéz-Moctezuma, J.; Prospéro-García, O.; Méndez-Díaz, M.; Pérez-Tapia, M.; Pavón, L.; Morales-Montor, J. The Bidirectional Relationship between Sleep and Immunity against Infections. J. Immunol. Res. 2015, 2015, 678164. [Google Scholar] [CrossRef]
- Xie, L.; Kang, H.; Xu, Q.; Chen, M.J.; Liao, Y.; Thiyagarajan, M.; O’Donnell, J.; Christensen, D.J.; Nicholson, C.; Iliff, J.J.; et al. Sleep drives metabolite clearance from the adult brain. Science 2013, 342, 373–377. [Google Scholar] [CrossRef]
- Hemmer, B.; Gran, B.; Zhao, Y.; Marques, A.; Pascal, J.; Tzou, A.; Kondo, T.; Cortese, I.; Bielekova, B.; Straus, S.E.; et al. Identification of candidate T-cell epitopes and molecular mimics in chronic Lyme disease. Nat. Med. 1999, 5, 1375–1382. [Google Scholar] [CrossRef] [PubMed]
- Soulas, P.; Woods, A.; Jaulhac, B.; Knapp, A.M.; Pasquali, J.L.; Martin, T.; Korganow, A.S. Autoantigen, innate immunity, and T cells cooperate to break B cell tolerance during bacterial infection. J. Clin. Investig. 2005, 115, 2257–2267. [Google Scholar] [CrossRef] [PubMed]
- Sigal, L.H. Immunologic mechanisms in Lyme neuroborreliosis: The potential role of autoimmunity and molecular mimicry. Semin. Neurol. 1997, 17, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Kreye, J.; Reincke, S.M.; Prüss, H. Do cross-reactive antibodies cause neuropathology in COVID-19? Nat. Rev. Immunol. 2020, 20, 645–646. [Google Scholar] [CrossRef] [PubMed]
- Sherbet, S.G.S. Bacterial Infections and the Pathogenesis of Autoimmune Conditions. Br. J. Med. Pract. 2009, 2, 6–13. [Google Scholar]
- Tausk, F.; Elenkov, I.; Moynihan, J. Psychoneuroimmunology. Dermatol. Ther. 2008, 21, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Pan, W.; Stone, K.P.; Hsuchou, H.; Manda, V.K.; Zhang, Y.; Kastin, A.J. Cytokine signaling modulates blood-brain barrier function. Curr. Pharm. Des. 2011, 17, 3729–3740. [Google Scholar] [CrossRef] [PubMed]
- Klein, H.C.; de Witte, L.; Bransfield, R.; De Deyn, P.P. PET and SPECT in Neurology; Dierckx, R.A.J.O., Otte, A., de Vries, E.F.J., van Waarde, A., Leenders, K.L., Eds.; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Wichers, M.C.; Koek, G.H.; Robaeys, G.; Verkerk, R.; Scharpé, S.; Maes, M. IDO and interferon-alpha-induced depressive symptoms: A shift in hypothesis from tryptophan depletion to neurotoxicity. Mol. Psychiatry 2005, 10, 538–544. [Google Scholar] [CrossRef]
- Saikarthik, J.; Saraswathi, I.; Alarifi, A.; Al-Atram, A.A.; Mickeymaray, S.; Paramasivam, A.; Shaikh, S.; Jeraud, M.; Alothaim, A.S. Role of neuroinflammation mediated potential alterations in adult neurogenesis as a factor for neuropsychiatric symptoms in Post-Acute COVID-19 syndrome-A narrative review. PeerJ 2022, 10, e14227. [Google Scholar] [CrossRef]
- Casey, B.J.; Heller, A.S.; Gee, D.G.; Cohen, A.O. Development of the emotional brain. Neurosci. Lett. 2019, 693, 29–34. [Google Scholar] [CrossRef]
- Cattarinussi, G.; Miola, A.; Trevisan, N.; Valeggia, S.; Tramarin, E.; Mucignat, C.; Morra, F.; Minerva, M.; Librizzi, G.; Bordin, A.; et al. Altered brain regional homogeneity is associated with depressive symptoms in COVID-19. J. Affect. Disord. 2022, 313, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, X.; Zhan, B.; Jia, Y.; Li, C.; Wu, N.; Zhao, M.; Chen, N.; Guo, Y.; Du, Y.; Zhang, Y.; et al. IL-33 in the basolateral amygdala integrates neuroinflammation into anxiogenic circuits via modulating BDNF expression. Brain Behav. Immun. 2022, 102, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Prell, T.; Dirks, M.; Arvanitis, D.; Braun, D.; Peschel, T.; Worthmann, H.; Schuppner, R.; Raab, P.; Grosskreutz, J.; Weissenborn, K. Cerebral patterns of neuropsychological disturbances in hepatitis C patients. J. Neurovirol. 2019, 25, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Denton, A.R.; Samaranayake, S.A.; Kirchner, K.N.; Roscoe, R.F., Jr.; Berger, S.N.; Harrod, S.B.; Mactutus, C.F.; Hashemi, P.; Booze, R.M. Selective monoaminergic and histaminergic circuit dysregulation following long-term HIV-1 protein exposure. J. Neurovirol. 2019, 25, 540–550. [Google Scholar] [CrossRef] [PubMed]
- Kamat, R.; Brown, G.G.; Bolden, K.; Fennema-Notestein, C.; Archibald, S.; Marcotte, T.D.; Letendre, S.L.; Ellis, R.J.; Woods, S.P.; Grant, I.; et al. Apathy is associated with white matter abnormalities in anterior, medial brain regions in persons with HIV infection. J. Clin. Exp. Neuropsychol. 2014, 36, 854–866. [Google Scholar] [CrossRef] [PubMed]
- Green, M.J.; Watkeys, O.J.; Whitten, T.; Thomas, C.; Karluki, M.; Dean, K.; Laurens, K.R.; Harris, F.; Carr, V.J. Increased incidence of childhood mental disorders following exposure to early life infection. Brain Behav. Immun. 2021, 97, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Petersen, L.; Gasse, C.; Mortensen, P.B.; Dalsgaard, S.; Yolken, R.H.; Mors, O.; Benros, M.E. A Nationwide Study in Denmark of the Association Between Treated Infections and the Subsequent Risk of Treated Mental Disorders in Children and Adolescents. JAMA Psychiatry 2019, 76, 271–279. [Google Scholar] [CrossRef]
- Boyd, C.M.; Darer, J.; Boult, C.; Fried, L.P.; Boult, L.; Wu, A.W. Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: Implications for pay for performance. JAMA 2005, 294, 716–724. [Google Scholar] [CrossRef]
- Bransfield, R.C.; Friedman, K.J. Differentiating Psychosomatic, Somatopsychic, Multisystem Illnesses, and Medical Uncertainty. Healthcare 2019, 7, 114. [Google Scholar] [CrossRef]
- Citera, M.; Freeman, P.R.; Horowitz, R.I. Empirical validation of the Horowitz Multiple Systemic Infectious Disease Syndrome Questionnaire for suspected Lyme disease. Int. J. Gen. Med. 2017, 10, 249–273. [Google Scholar] [CrossRef]
- Shroff, G.; Hopf-Seidel, P. A Novel Scoring System Approach to Assess Patients with Lyme Disease (Nutech Functional Score). J. Glob. Infect. Dis. 2018, 10, 3–6. [Google Scholar] [CrossRef]
- Fallon, B.A.; Zubcevik, N.; Bennett, C.; Doshi, S.; Rebman, A.W.; Kishon, R.; Moeller, J.R.; Octavien, N.R.; Aucott, J.N. The General Symptom Questionnaire-30 (GSQ-30): A Brief Measure of Multi-System Symptom Burden in Lyme Disease. Front. Med. 2019, 6, 283. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. National Healthcare Safety Network: Surveillance vs. Clinical. Frequently Asked Questions (FAQs) Frequently Asked Questions (FAQs). Available online: https://www.cdc.gov/nhsn/faqs/faqs-miscellaneous.html (accessed on 7 June 2023).
- Weinstein, E.R.; Rebman, A.W.; Aucott, J.N.; Johnson-Greene, D.; Bechtold, K.T. Sleep quality in well-defined Lyme disease: A clinical cohort study in Maryland. Sleep 2018, 41, zsy035. [Google Scholar] [CrossRef] [PubMed]
- Modolfsy, H. Sleep and the immune system. Int. J. Immunopharmacol. 1995, 17, 649–654. [Google Scholar]
- Kelley, K.W. The role of growth hormone in modulation of the immune response. Ann. N. Y. Acad. Sci. 1990, 594, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Bransfield, R.C. Building Bridges between Infectious Disease Physicians and Psychiatrists. Contagion Live. 2017. Available online: https://www.contagionlive.com/view/building-bridges-between-infectious-disease-physicians-and-psychiatrists (accessed on 22 August 2022).
- Hutto, B. Syphilis in Clinical Psychiatry: A Review. Psychosomatics 2001, 42, 453–460. [Google Scholar] [CrossRef] [PubMed]
- WHO Guidelines for the Treatment of Treponema pallidum (Syphilis). World Health Organization: Geneva, Switzerland, 2016; 4, Recommendations for the Treatment of Syphilis. Available online: https://www.ncbi.nlm.nih.gov/books/NBK384905/ (accessed on 26 August 2022).
- Miklossy, J. Chronic or late lyme neuroborreliosis: Analysis of evidence compared to chronic or late neurosyphilis. Open Neurol. J. 2012, 6, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Norris, S.J. Polypeptides of Treponema pallidum: Progress toward understanding their structural, functional, and immunologic roles. Treponema Pallidum Polypeptide Research Group. Microbiol. Rev. 1993, 57, 750–779, Erratum in Microbiol. Rev. 1994, 58, 291. [Google Scholar] [CrossRef]
- Carlson, J.A.; Dabiri, G.; Cribier, B.; Sell, S. The immunopathobiology of syphilis: The manifestations and course of syphilis are determined by the level of delayed-type hypersensitivity. Am. J. Dermatopathol. 2011, 33, 433–460. [Google Scholar] [CrossRef]
- Dawson-Butterworth, K.; Heathcote, P.R. Review of hospitalized cases of general paralysis of the insane. Br. J. Vener. Dis. 1970, 46, 295–302. [Google Scholar] [CrossRef]
- Yogeswari, L.; Chacko, C.W. Persistence of T. pallidum and its significance in penicillin-treated seropositive late syphilis. Br. J. Vener. Dis. 1971, 47, 339–347. [Google Scholar] [CrossRef]
- Whiteside, C.M. Persistence of neurosyphilis despite multiple treatment regimens. Am. J. Med. 1989, 87, 225–227. [Google Scholar] [CrossRef] [PubMed]
- Moulton, C.D.; Koychev, I. The effect of penicillin therapy on cognitive outcomes in neurosyphilis: A systematic review of the literature. Gen. Hosp. Psychiatry 2015, 37, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Stokes, J.H.; Beerman, H.; Ingraham, N.R. Modern Clinical Syphilology: Diagnosis, Treatment, Case Study, 3rd ed.; Saunders: Philadelphia, PA, USA, 1944; 1025p. [Google Scholar]
- Tuskegee Experiment: The Infamous Syphilis Study. Available online: https://www.history.com/news/the-infamous-40-year-tuskegee-study (accessed on 26 August 2022).
- Boillat, M.; Hammoudi, P.M.; Dogga, S.K.; Pagès, S.; Goubran, M.; Rodriguez, I.; Soldati-Favre, D. Neuroinflammation-Associated Aspecific Manipulation of Mouse Predator Fear by Toxoplasma gondii. Cell Rep. 2020, 30, 320–334. [Google Scholar] [CrossRef] [PubMed]
- Flegr, J. How and why Toxoplasma makes us crazy. Trends Parasitol. 2013, 29, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Flegr, J.; Hrdy, I. Influence of chronic toxoplasmosis on some human personality factors. Folia Parasitol. 1994, 42, 122–126. [Google Scholar]
- Flegr, J.; Zitkova, S.; Kodym, P.; Frynta, D. Induction of changes in human behavious by the parasitic protozoan Toxoplasma gondii. Parasitology 1996, 113 Pt 1, 49–54. [Google Scholar] [CrossRef]
- Piekarski, G. Behavioral alterations caused by parasitic infection in case of latent toxoplasma infection. Zentralbl. Bakteriol. Mikrobiol. Hyg. A Med. Mikrobiol. Infekt. Parasitol. 1981, 250, 403–406. [Google Scholar] [CrossRef] [PubMed]
- Flegr, J. Effects of toxoplasma on human behavior. Schizophr. Bull. 2007, 33, 757–760. [Google Scholar] [CrossRef] [PubMed]
- Coryell, W.; Yolken, R.; Butcher, B.; Burns, T.; Dindo, L.; Schlechte, J.; Calarge, C. Toxoplasmosis Titers and past Suicide Attempts Among Older Adolescents Initiating SSRI Treatment. Arch. Suicide Res. 2016, 20, 605–613. [Google Scholar] [CrossRef]
- Lester, D. Brain parasites and suicide. Psychol. Rep. 2010, 107, 424. [Google Scholar] [CrossRef]
- Zhang, Y.; Träskman-Bendz, L.; Janelidze, S.; Langenberg, P.; Saleh, A.; Constantine, N.; Okusaga, O.; Bay-Richter, C.; Brundin, L.; Postolache, T.T. Toxoplasma gondii immunoglobulin G antibodies and nonfatal suicidal self-directed violence. J. Clin. Psychiatry 2012, 73, 1069–1076. [Google Scholar] [CrossRef] [PubMed]
- Bak, J.; Shim, S.H.; Kwon, Y.J.; Lee, H.Y.; Kim, J.S.; Yoon, H.; Lee, Y.J. The Association between Suicide Attempts and Toxoplasma gondii Infection. Clin. Psychopharmacol. Neurosci. 2018, 16, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Lester, D. Toxoplasma gondii and homicide. Psychol. Rep. 2012, 111, 196–197. [Google Scholar] [CrossRef] [PubMed]
- Dix, E.; Roy, K. COVID-19: Brain Effects. Psychiatr. Clin. N. Am. 2022, 45, 625–637. [Google Scholar] [CrossRef] [PubMed]
- Espinosa Rodríguez, P.; Martínez Aguilar, A.; Ripoll Muñoz, M.P.; Rodríguez Navarro, M.Á. COVID persistente: ¿es en realidad una encefalomielitis miálgica? Revisión bibliográfica y consideraciones [Long COVID: Is it really myalgic encephalomyelitis? Bibliographic review and considerations]. Semergen 2022, 48, 63–69. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Bansal, R.; Gubbi, S.; Koch, C.A. COVID-19 and chronic fatigue syndrome: An endocrine perspective. J. Clin. Transl. Endocrinol. 2022, 27, 100284. [Google Scholar] [CrossRef] [PubMed]
- Berloffa, S.; Salvati, A.; Pantalone, G.; Falcioni, L.; Rizzi, M.M.; Naldini, F.; Masi, G.; Gagliano, A. Steroid treatment response to post SARS-CoV-2 PANS symptoms: Case series. Front. Neurol. 2023, 14, 1085948, Erratum in Front. Neurol. 2023, 14, 1178013. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Xu, E.; Al-Aly, Z. Risks of mental health outcomes in people with covid-19: Cohort study. BMJ 2022, 376, e068993. [Google Scholar] [CrossRef]
- Schou, T.M.; Joca, S.; Wegener, G.; Bay-Richter, C. Psychiatric and neuropsychiatric sequelae of COVID-19—A systematic review. Brain Behav. Immun. 2021, 97, 328–348. [Google Scholar] [CrossRef]
- Pandya, D.; Johnson, T.P. Chronic and delayed neurological manifestations of persistent infections. Curr. Opin. Neurol. 2023, 36, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Walitt, B.; Johnson, T.P. The pathogenesis of neurologic symptoms of the postacute sequelae of severe acute respiratory syndrome coronavirus 2 infection. Curr. Opin. Neurol. 2022, 35, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Roessler, M.; Tesch, F.; Batram, M.; Jacob, J.; Loser, F.; Weidinger, O.; Wende, D.; Vivirito, A.; Toepfner, N.; Ehm, F.; et al. Post-COVID-19-associated morbidity in children, adolescents, and adults: A matched cohort study including more than 157,000 individuals with COVID-19 in Germany. PLoS Med. 2022, 19, e1004122. [Google Scholar] [CrossRef] [PubMed]
- Păunescu, R.L.; Miclu Ia, I.V.; Verişezan, O.R.; Crecan-Suciu, B.D. Acute and longterm psychiatric symptoms associated with COVID19 (Review). Biomed. Rep. 2022, 18, 4. [Google Scholar] [CrossRef] [PubMed]
- Mat Hassan, N.; Salim, H.S.; Amaran, S.; Yunus, N.I.; Yusof, N.A.; Daud, N.; Fry, D. Prevalence of mental health problems among children with long COVID: A systematic review and meta-analysis. PLoS ONE 2023, 18, e0282538. [Google Scholar] [CrossRef] [PubMed]
- Proal, A.D.; VanElzakker, M.B. Long COVID or Post-acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms. Front. Microbiol. 2021, 12, 698169. [Google Scholar] [CrossRef] [PubMed]
- Choutka, J.; Jansari, V.; Hornig, M.; Iwasaki, A. Unexplained post-acute infection syndromes. Nat. Med. 2022, 28, 911–923. [Google Scholar] [CrossRef] [PubMed]
- Proal, A.D.; VanElzakker, M.B.; Aleman, S.; Bach, K.; Boribong, B.P.; Buggert, M.; Cherry, S.; Chertow, D.S.; Davies, H.E.; Dupont, C.L.; et al. SARS-CoV-2 reservoir in post-acute sequelae of COVID-19 (PASC). Nat. Immunol. 2023, 24, 1616–1627. [Google Scholar] [CrossRef]
- Schultheiß, C.; Willscher, E.; Paschold, L.; Gottschick, C.; Klee, B.; Bosurgi, L.; Dutzmann, J.; Sedding, D.; Frese, T.; Girndt, M.; et al. Liquid biomarkers of macrophage dysregulation and circulating spike protein illustrate the biological heterogeneity in patients with post-acute sequelae of COVID-19. J. Med. Virol. 2023, 95, e28364. [Google Scholar] [CrossRef]
- Pallanti, S.; Di Ponzio, M. PANDAS/PANS in the COVID-19 Age: Autoimmunity and Epstein-Barr Virus Reactivation as Trigger Agents? Children 2023, 10, 648. [Google Scholar] [CrossRef]
- Frank, M.G.; Fleshner, M.; Maier, S.F. Exploring the immunogenic properties of SARS-CoV-2 structural proteins: PAMP:TLR signaling in the mediation of the neuroinflammatory and neurologic sequelae of COVID-19. Brain Behav. Immun. 2023, 111, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Kugeler, K.J.; Schwartz, A.M.; Delorey, M.J.; Mead, P.S.; Hinckley, A.F. Estimating the Frequency of Lyme Disease Diagnoses, United States, 2010–2018. Emerg. Infect. Dis. 2021, 27, 616–619. [Google Scholar] [CrossRef] [PubMed]
- Scrimenti, R.J. Erythema Chronicum Migrans. Arch. Derm. 1970, 102, 104–105. [Google Scholar] [CrossRef] [PubMed]
- Steere, A.C.; Malawista, S.E.; Snydman, D.R.; Shope, R.E.; Andiman, W.A.; Ross, M.R.; Steele, F.M. Lyme arthritis: An epidemic of oligoarticular arthritis in children and adults in three connecticut communities. Arthritis Rheum. 1977, 20, 7–17. [Google Scholar] [CrossRef]
- Steere, A.C.; Malawista, S.E.; Bartenhagen, N.H.; Spieler, P.N.; Newman, J.H.; Rahn, D.W.; Hutchinson, G.J.; Green, J.; Snydman, D.R.; Taylor, E. The clinical spectrum and treatment of Lyme disease. Yale J. Biol. Med. 1984, 57, 453–461. [Google Scholar] [PubMed]
- Steere, A.C.; Malawista, S.E.; Hardin, J.A.; Ruddy, S.; Askenase, W.; Andiman, W.A. Erythema chronicum migrans and Lyme arthritis. The enlarging clinical spectrum. Ann. Intern. Med. 1977, 86, 685–698. [Google Scholar] [CrossRef] [PubMed]
- Burgdorfer, W.; Barbour, A.G.; Hayes, S.F.; Benach, J.L.; Grunwaldt, E.; Davis, J.P. Lyme disease-a tick-borne spirochetosis? Science 1982, 216, 1317–1319. [Google Scholar] [CrossRef] [PubMed]
- Porcella, S.F.; Schwan, T.G. Borrelia burgdorferi and Treponema pallidum: A comparison of functional genomics, environmental adaptations, and pathogenic mechanisms. J. Clin. Investig. 2001, 107, 651–656. [Google Scholar] [CrossRef]
- Hájek, T.; Pasková, B.; Janovská, D.; Bahbouh, R.; Hájek, P.; Libiger, J.; Höschl, C. Higher prevalence of antibodies to Borrelia burgdorferi in psychiatric patients than in healthy subjects. Am. J. Psychiatry 2002, 159, 297–301. [Google Scholar] [CrossRef]
- Back, T.; Grünig, S.; Winter, Y.; Bodechtel, U.; Guthke, K.; Khati, D.; von Kummer, R. Neuroborreliosis-associated cerebral vasculitis: Long-term outcome and health-related quality of life. J. Neurol. 2013, 260, 1569–1575. [Google Scholar] [CrossRef]
- Donta, S.T.; Noto, R.B.; Vento, J.A. SPECT brain imaging in chronic Lyme disease. Clin. Nucl. Med. 2012, 37, e219–e222. [Google Scholar] [CrossRef] [PubMed]
- Stricker, R.S.; Fesler, M.C. Chronic Lyme disease: A working case definition. Am. J. Infect. Dis. 2018, 14, 1–44. [Google Scholar] [CrossRef]
- Shor, S.; Green, C.; Szantyr, B.; Phillips, S.; Liegner, K.; Burrascano, J.J., Jr.; Bransfield, R.; Maloney, E.L. Chronic Lyme Disease: An Evidence-Based Definition by the ILADS Working Group. Antibiotics 2019, 8, 269. [Google Scholar] [CrossRef] [PubMed]
- CDC. Lyme Disease Syndrome (PTLDS). Available online: https://www.cdc.gov/lyme/postlds/index.html (accessed on 18 September 2023).
- Tick-Borne Disease Working Group 2022 Report to Congress. Available online: https://www.hhs.gov/sites/default/files/tbdwg-2022-report-to-congress.pdf?fbclid=IwAR3lYeRCwLcgxjK8HoIxcOARP9F0qZwiS-E_X55Pr5ArrGzK4x8v6roZEhk (accessed on 28 February 2023).
- Billeter, S.A.; Levy, M.G.; Chomel, B.B.; Breitschwerdt, E.B. Vector transmission of Bartonella species with emphasis on the potential for tick transmission. Med. Vet. Entomol. 2008, 22, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Reis, C.; Cote, M.; Le Rhun, D.; Lecuelle, B.; Levin, M.L.; Vayssier-Taussat, M.; Bonnet, S.I. Vector competence of the tick Ixodes ricinus for transmission of Bartonella birtlesii. PLoS Negl. Trop. Dis. 2011, 5, e1186. [Google Scholar] [CrossRef] [PubMed]
- Vayssier-Taussat, M.; Moutailler, S.; Michelet, L.; Devillers, E.; Bonnet, S.; Cheval, J.; Hébert, C.; Eloit, M. Next generation sequencing uncovers unexpected bacterial pathogens in ticks in western Europe. PLoS ONE 2013, 8, e81439. [Google Scholar] [CrossRef] [PubMed]
- Moutailler, S.; Valiente Moro, C.; Vaumourin, E.; Michelet, L.; Tran, F.H.; Devillers, E.; Cosson, J.F.; Gasqui, P.; Van, V.T.; Mavingui, P.; et al. Co-infection of Ticks: The Rule Rather Than the Exception. PLoS Negl. Trop. Dis. 2016, 10, e0004539. [Google Scholar] [CrossRef] [PubMed]
- Garg, K.; Meriläinen, L.; Franz, O.; Pirttinen, H.; Quevedo-Diaz, M.; Croucher, S.; Gilbert, L. Evaluating polymicrobial immune responses in patients suffering from tick-borne diseases. Sci. Rep. 2018, 8, 15932, Erratum in Sci. Rep. 2022, 12, 3211. [Google Scholar] [CrossRef]
- CDC. Tickborne Diseases of the United States, 6th ed.; 2022. Available online: https://www.cdc.gov/ticks/tickbornediseases/TickborneDiseases-P.pdf (accessed on 19 September 2023).
- Scott, J.D.; Sajid, M.S.; Pascoe, E.L.; Foley, J.E. Detection of Babesia odocoilei in Humans with Babesiosis Symptoms. Diagnostics 2021, 11, 947. [Google Scholar] [CrossRef]
- Fallon, B.A.; Kochevar, J.M.; Gaito, A.; Nields, J.A. The underdiagnosis of neuropsychiatric Lyme disease in children and adults. Psychiatr. Clin. N. Am. 1998, 21, 693–703. [Google Scholar] [CrossRef]
- CDC. Notice to Readers Recommendations for Test Performance and Interpretation from the Second National Conference on Serologic Diagnosis of Lyme Disease. Morb. Mortal. Wkly. Rep. 1995, 44, 590–591. [Google Scholar]
- Mead, P.; Petersen, J.; Hinckley, A. Updated CDC Recommendation for Serologic Diagnosis of Lyme Disease. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 703. [Google Scholar] [CrossRef]
- Branda, J.A.; Strle, K.; Nigrovic, L.E.; Lantos, P.M.; Lepore, T.J.; Damle, N.S.; Ferraro, M.J.; Steere, A.C. Evaluation of Modified 2-Tiered Serodiagnostic Testing Algorithms for Early Lyme Disease. Clin. Infect. Dis. 2017, 64, 1074–1080. [Google Scholar] [CrossRef]
- Hilton, E.; Devoti, J.; Sood, S. Recommendation to include OspA and OspB in the new immunoblotting criteria for serodiagnosis of Lyme disease. J. Clin. Microbiol. 1996, 34, 1353–1354, Erratum in J. Clin. Microbiol. 1997, 35, 2713. [Google Scholar] [CrossRef] [PubMed]
- Stricker, R.B.; Johnson, L. Lyme disease: Call for a “Manhattan Project” to combat the epidemic. PLoS Pathog. 2014, 10, e1003796. [Google Scholar] [CrossRef] [PubMed]
- Dressler, F.; Whalen, J.A.; Reinhardt, B.N.; Steere, A.C. Western blotting in the serodiagnosis of Lyme disease. J. Infect. Dis. 1993, 167, 392–400. [Google Scholar] [CrossRef] [PubMed]
- Ledue, T.B.; Collins, M.F.; Craig, W.Y. New laboratory guidelines for serologic diagnosis of Lyme disease: Evaluation of the two-test protocol. J. Clin. Microbiol. 1996, 34, 2343–2350. [Google Scholar] [CrossRef] [PubMed]
- Tilton, R.C.; Sand, M.N.; Manak, M. The western immunoblot for Lyme disease: Determination of sensitivity, specificity, and interpretive criteria with use of commercially available performance panels. Clin. Infect. Dis. 1997, 25 (Suppl. S1), S31–S34. [Google Scholar] [CrossRef] [PubMed]
- Bacon, R.M.; Biggerstaff, B.J.; Schriefer, M.E.; Gilmore, R.D., Jr.; Philipp, M.T.; Steere, A.C.; Wormser, G.P.; Marques, A.R.; Johnson, B.J. Serodiagnosis of Lyme disease by kinetic enzyme-linked immunosorbent assay using recombinant VlsE1 or peptide antigens of Borrelia burgdorferi compared with 2-tiered testing using whole-cell lysates. J. Infect. Dis. 2003, 187, 1187–1199. [Google Scholar] [CrossRef] [PubMed]
- Steere, A.C.; McHugh, G.; Damle, N.; Sikand, V.K. Prospective study of serologic tests for Lyme disease. Clin. Infect. Dis. 2008, 47, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Branda, J.A.; Aguero-Rosenfeld, M.E.; Ferraro, M.J.; Johnson, B.J.; Wormser, G.P.; Steere, A.C. 2-tiered antibody testing for early and late Lyme disease using only an immunoglobulin G blot with the addition of a VlsE band as the second-tier test. Clin. Infect. Dis. 2010, 50, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Branda, J.A.; Linskey, K.; Kim, Y.A.; Steere, A.C.; Ferraro, M.J. Two-tiered antibody testing for Lyme disease with use of 2 enzyme immunoassays, a whole-cell sonicate enzyme immunoassay followed by a VlsE C6 peptide enzyme immunoassay. Clin. Infect. Dis. 2011, 53, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Rahn, D.W.; Malawista, S.E. Lyme disease: Recommendations for diagnosis and treatment. Ann. Intern. Med. 1991, 114, 472–481. [Google Scholar] [CrossRef] [PubMed]
- Gardner, T. Lyme disease. In Infectious Diseases of the Fetus and Newborn Infant, 5th ed.; Remington, J.S., Klein, J.O., Eds.; WB Saunders Company: Philadelphia, PA, USA, 2001; 585p. [Google Scholar]
- Cutler, S. Pitfalls in the laboratory diagnosis of Lyme borreliosis. In 2nd European Symposium on Lyme Borreliosis. A NATO advanced research workshop. United Kingdom, 19–20 May 1993. Abstracts. Ann. Rheum. Dis. 1993, 52, 387–412. [Google Scholar] [CrossRef]
- Schutzer, S.E.; Schwartz, R.A. Diagnosing Lyme disease: Often simple, often difficult. Cutis 1991, 47, 229–230. [Google Scholar] [PubMed]
- Dattwyler, R.J.; Volkman, D.J.; Luft, B.J.; Halperin, J.J.; Thomas, J.; Golightly, M.G. Seronegative Lyme disease. Dissociation of specific T- and B-lymphocyte responses to Borrelia burgdorferi. N. Engl. J. Med. 1988, 319, 1441–1446. [Google Scholar] [CrossRef] [PubMed]
- Dressler, F.; Yoshinari, N.H.; Steere, A.C. The T-cell proliferative assay in the diagnosis of Lyme disease. Ann. Intern. Med. 1991, 115, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, C.; Lipton, R.B.; Lowy, F.D.; Coyle, P.K. Seronegative chronic relapsing neuroborreliosis. Eur. Neurol. 1995, 35, 113–117. [Google Scholar] [CrossRef]
- Oksi, J.; Uksila, J.; Marjamäki, M.; Nikoskelainen, J.; Viljanen, M.K. Antibodies against whole sonicated Borrelia burgdorferi spirochetes, 41-kilodalton flagellin, and P39 protein in patients with PCR- or culture-proven late Lyme borreliosis. J. Clin. Microbiol. 1995, 33, 2260–2264. [Google Scholar] [CrossRef]
- Smith, H.V.; Gray, J.S.; Mckenzie, G. A Lyme borreliosis human serosurvey of asymptomatic adults in Ireland. Zentralbl. Bakteriol. 1991, 275, 382–389. [Google Scholar] [CrossRef]
- Huycke, M.M.; D’Alessio, D.D.; Marx, J.J. Prevalence of antibody to Borrelia burgdorferi by indirect fluorescent antibody assay, ELISA, and western immunoblot in healthy adults in Wisconsin and Arizona. J. Infect. Dis. 1992, 165, 1133–1137. [Google Scholar] [CrossRef]
- Carlsson, S.A.; Granlund, H.; Nyman, D.; Wahlberg, P. IgG seroprevalence of Lyme borreliosis in the population of the Aland Islands in Finland. Scand. J. Infect. Dis. 1998, 30, 501–503. [Google Scholar] [CrossRef]
- Riesbeck, K.; Hammas, B. Comparison of an automated Borrelia indirect chemiluminescent immunoassay (CLIA) with a VlsE/C6 ELISA and Immunoblot. Eur. J. Clin. Microbiol. Infect. Dis. 2007, 26, 517–519. [Google Scholar] [CrossRef]
- Johnston, D.; Kelly, J.R.; Ledizet, M.; Lavoie, N.; Smith, R.P.; Parsonnet, J.; Schwab, J.; Stratidis, J.; Espich, S.; Lee, G.; et al. Frequency and Geographic Distribution of Borrelia miyamotoi, Borrelia burgdorferi, and Babesia microti Infections in New England Residents. Clin. Infect. Dis. 2022, ciac107. [Google Scholar] [CrossRef] [PubMed]
- Swedo, S.E.; Leonard, H.L.; Garvey, M.; Mittleman, B.; Allen, A.J.; Perlmutter, S.; Lougee, L.; Dow, S.; Zamkoff, J.; Dubbert, B.K. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections: Clinical description of the first 50 cases. Am. J. Psychiatry 1998, 155, 264–271, Erratum in Am. J. Psychiatry 1998, 155, 57. [Google Scholar] [CrossRef] [PubMed]
- Dop, D.; Marcu, I.R.; Padureanu, R.; Niculescu, C.E.; Padureanu, V. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (Review). Exp. Ther. Med. 2021, 21, 94. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.A.; Swedo, S.E. Post-infectious autoimmune disorders: Sydenham’s chorea, PANDAS and beyond. Brain Res. 2015, 1617, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Singer, H.S.; Loiselle, C.R.; Lee, O.; Minzer, K.; Swedo, S.; Grus, F.H. Anti-basal ganglia antibodies in PANDAS. Mov. Disord. 2004, 19, 406–415. [Google Scholar] [CrossRef]
- Dileepan, T.; Smith, E.D.; Knowland, D.; Hsu, M.; Platt, M.; Bittner-Eddy, P.; Cohen, B.; Southern, P.; Latimer, E.; Harley, E.; et al. Group A Streptococcus intranasal infection promotes CNS infiltration by streptococcal-specific Th17 cells. J. Clin. Investig. 2016, 126, 303–317. [Google Scholar] [CrossRef]
- Kolls, J.K.; Khader, S.A. The role of Th17 cytokines in primary mucosal immunity. Cytokine Growth Factor Rev. 2010, 21, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Maddur, M.S.; Miossec, P.; Kaveri, S.V.; Bayry, J. Th17 cells: Biology, pathogenesis of autoimmune and inflammatory diseases, and therapeutic strategies. Am. J. Pathol. 2012, 181, 8–18. [Google Scholar] [CrossRef]
- Paroli, M.; Caccavale, R.; Fiorillo, M.T.; Spadea, L.; Gumina, S.; Candela, V.; Paroli, M.P. The Double Game Played by Th17 Cells in Infection: Host Defense and Immunopathology. Pathogens 2022, 11, 1547. [Google Scholar] [CrossRef] [PubMed]
- Kebir, H.; Kreymborg, K.; Ifergan, I.; Dodelet-Devillers, A.; Cayrol, R.; Bernard, M.; Giuliani, F.; Arbour, N.; Becher, B.; Prat, A. Human TH17 lymphocytes promote blood-brain barrier disruption and central nervous system inflammation. Nat. Med. 2007, 13, 1173–1175. [Google Scholar] [CrossRef] [PubMed]
- Platt, M.P.; Agalliu, D.; Cutforth, T. Hello from the Other Side: How autoantibodies Circumvent the blood-brain barrier in autoimmune encephalitis. Front. Immunol. 2017, 8, 442. [Google Scholar] [CrossRef] [PubMed]
- Dando, S.J.; Mackay-Sim, A.; Norton, R.; Currie, B.J.; St John, J.A.; Ekberg, J.A.; Batzloff, M.; Ulett, G.C.; Beacham, I.R. Pathogens penetrating the central nervous system: Infection pathways and the cellular and molecular mechanisms of invasion. Clin. Microbiol. Rev. 2014, 27, 691–726. [Google Scholar] [CrossRef] [PubMed]
- Wayne, C.R.; Bremner, L.; Faust, T.E.; Durán-Laforet, V.; Ampatey, N.; Ho, S.J.; Feinberg, P.A.; Arvanitis, P.; Ciric, B.; Ruan, C.; et al. Distinct Th17 effector cytokines differentially promote microglial and blood-brain barrier inflammatory responses during post-infectious encephalitis. bioRxiv 2023. bioRxiv:9:2023.03.10.532135. [Google Scholar]
- Swedo, S.E.; Leckman, J.F.; Rose, N.R. From Research Subgroup to Clinical Syndrome: Modifying the PANDAS Criteria to Describe PANS (Pediatric Acute-onset Neuropsychiatric Syndrome). Pediatr. Therapeut. 2012, 2, 113. [Google Scholar] [CrossRef]
- Johns Hopkins All Children’s Hospital: What Is PANS? Available online: https://www.hopkinsallchildrens.org/Patients-Families/Health-Library/HealthDocNew/What-Is-PANS (accessed on 17 January 2023).
- Cross, A.; Bouboulis, D.; Shimasaki, C.; Jones, C.R. Case Report: PANDAS and Persistent Lyme Disease with Neuropsychiatric Symptoms: Treatment, Resolution, and Recovery. Front. Psychiatry 2021, 12, 505941. [Google Scholar] [CrossRef] [PubMed]
- Calaprice, D.; Tona, J.; Parker-Athill, E.C.; Murphy, T.K. A Survey of Pediatric Acute-Onset Neuropsychiatric Syndrome Characteristics and Course. J. Child Adolesc. Psychopharmacol. 2017, 27, 607–618. [Google Scholar] [CrossRef] [PubMed]
- Stanford Medicine. PANS: Pediatric Acute-Onset Neuropsychiatric Syndrome. Available online: https://med.stanford.edu/pans (accessed on 17 January 2023).
Figure 1.
Disease progression. Disease progression evolves over time. The unique path of evolution can create genetic vulnerabilities. Genetic and other vulnerabilities may then interact with pathogens and other disease contributors to begin a pathological process with regulatory dysfunction. The resulting pathological cascade may then lead to symptoms and syndromes (groups of symptoms). The symptoms, and syndromes (e.g., chronic stress, sleep deprivation, immune dysfunction) may further exacerbate disease progression.
Figure 1.
Disease progression. Disease progression evolves over time. The unique path of evolution can create genetic vulnerabilities. Genetic and other vulnerabilities may then interact with pathogens and other disease contributors to begin a pathological process with regulatory dysfunction. The resulting pathological cascade may then lead to symptoms and syndromes (groups of symptoms). The symptoms, and syndromes (e.g., chronic stress, sleep deprivation, immune dysfunction) may further exacerbate disease progression.


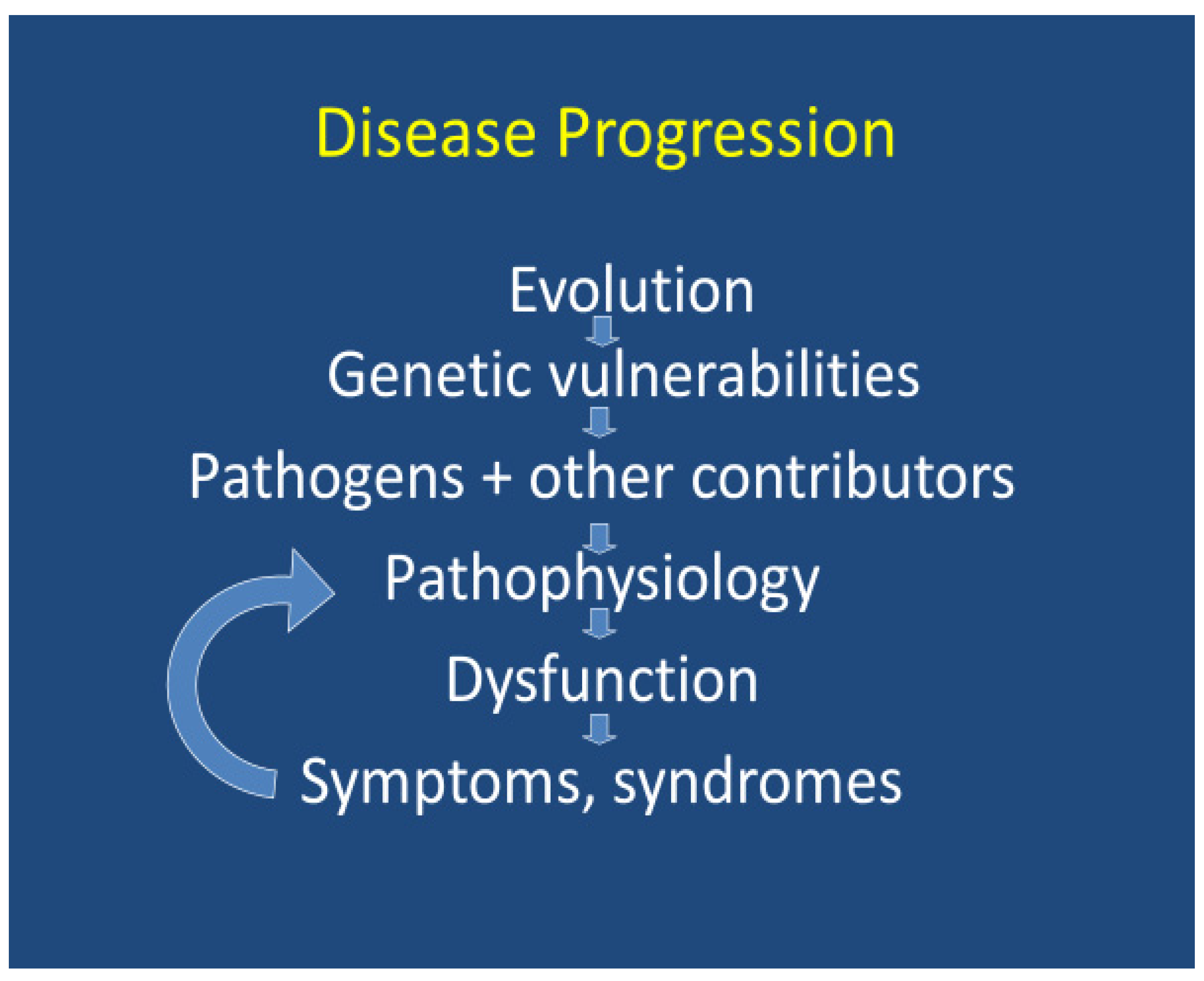{kind=link}
Table 1.
Infectious agents with potential psychiatric manifestations.
| Spirochetes |
| Borrelia burgdorferi sensu lato (new genus name Borreliella) [9,10,11,12,13,15,16,17] (Supplementary S1) |
| Borrelia burgdorferi sensu stricto (Lyme disease in USA, Europe) |
| Borrelia afzelii (Lyme disease mostly in Europe, Asia) |
| Borrelia garinii (Lyme disease mostly in Europe, Asia) |
| Relapsing fever group (also known as relapsing fever group Borrelia) [18] |
| Leptospira species (leptospirosis) [19] |
| Treponema pallidum (syphilis) [20,21,22,23] |
| Other bacteria |
| Actinomyces [24] |
| Bartonella henselae and other species (cat scratch disease, bartonellosis) [25,26,27,28] |
| Brucella species (brucellosis) [29] |
| Chlamydia species [30,31] |
| Coxiella burnetii (Q Fever and “Post-Q Fever Fatigue Syndrome”) [32] |
| Ehrlichia chaffeensis (human monocytic ehrlichiosis) [33,34] |
| Helicobacter pylori [35] |
| Mycoplasma pneumoniae and other species [36,37,38] |
| Rickettsia species (spotted fever, scrub typhus, African tick bite fever) [39,40,41,42,43] |
| Streptococcus pyogenes (group A beta hemolytic strep, PANDAS, Sydenham’s Chorea, St Vitus Dance) [44] |
| Tropheryma whipplei (Whipple’s disease) [45,46] |
| Viruses |
| Borna disease virus [47] |
| Chikungunya virus [48] |
| Coronaviruses (other than SARS-CoV-2) [49,50,51] |
| Enterovirus [52,53,54] |
| Cytomegalovirus [55,56,57] |
| Epstein–Barr virus [58,59] |
| Tick-borne encephalitis virus [60] |
| Hepatitis C virus [61,62,63] |
| Human endogenous retroviruses [64,65,66,67] H |
| Human immunodeficiency virus [68] |
| Human T-cell lymphotropic virus type 1 [69] |
| Influenza virus [70] |
| Measles virus [71,72,73,74,75,76] |
| Parvovirus B19 [77,78] |
| Poliovirus [79] |
| Rubella [80] |
| SARS-CoV-2 coronavirus [50,81,82,83,84,85] |
| West Nile virus [86,87] |
| Parasites [88] |
| Plasmodium species (malaria) [89,90] |
| Babesia species (B. microti, B. duncani, other Babesia species (Babesiosis)) [91] |
| Filaria (filariasis) [88,92,93] |
| Leishmania species (leishmaniasis) [94] |
| Toxoplasma gondii (toxoplasmosis) [95] |
| Taenia solium (neurocysticercosis or cysticercosis) [96,97,98] |
| Trypanosoma sp. (trypanosomiasis) [88,99,100] |
| Fungi |
| Aspergillus species [24] |
| Candida [101,102] |
| Cryptocococcus neoformans (cryptococcosis) [103,104] |
Table 2.
Examples of mental conditions potentially associated with infections.
| Mental Conditions | Infections | Citations |
|---|---|---|
| Autism spectrum disorders | Babesia | [105,106] |
| Bartonella | [105,106] | |
| Borna disease virus (animal models) | [107,108,109,110] | |
| Borrelia burgdorferi and other tick-borne diseases | [105,106,111,112,113,114,115,116,117] | |
| Chlamydia pneumoniae | [117,118,119] | |
| Cytomegalovirus | [120,121,122,123,124] | |
| Enterovirus | [53,54] | |
| Fungi (Aspergillus, Candida) | [125,126,127,128,129] | |
| Herpes simplex virus | [130,131,132,133,134] | |
| Human herpes virus-6 | [118,135] | |
| Infections in early childhood | [136,137] | |
| Intestinal microbiome composition changes | [138] | |
| Maternal infections or immune activation during pregnancy | [139,140,141,142,143,144,145] | |
| Mycoplasma: (M. fermentans, M. genitalium, M. hominis, M. pneumoniae) | [36,117,118] | |
| Measles virus (subacute sclerosing panencephalitis) | [135,146] | |
| Plasmodium (malaria) | [147,148,149,150] | |
| Rubella (congenital) | [80,151,152,153,154,155] | |
| Toxoplasma gondii (Toxoplasmosis) | [156] | |
| Varicella zoster virus | [157] | |
| Viral infections | [158,159,160] | |
| Schizophrenia | Aspergillus | [24] |
| Bacterial infections | [161] | |
| Bartonella | [25,162,163] | |
| Borrelia burgdorferi (Lyme disease) | [17,164,165,166,167,168,169,170,171] | |
| Borna disease virus | [172] | |
| Candida albicans | [101,102] | |
| Chlamydia, (C. psittaci, C. pneumoniae) | [31,172,173,174,175] | |
| Coronaviruses | [49] | |
| Cryptocococcus neoformans (cryptococcosis) | [103] | |
| Cytomegalovirus | [176] | |
| Epstein–Barr virus (EBV) | [58,177,178,179] | |
| Herpes simplex virus | [172,180,181] | |
| Human endogenous retroviruses | [64,65,172,182,183,184] | |
| Infections in early childhood | [137] | |
| Influenza virus | [185,186,187,188,189,190,191,192] | |
| Maternal infections or immune activation during pregnancy | [161,182,183,185,186,187,188,189,190,191,192,193,194,195] | |
| Measles virus (subacute sclerosing panencephalitis) | [71,72,73,74,75,76] | |
| Parvovirus | [78] | |
| Poliovirus | [79] | |
| Rubella | [194,196] | |
| Taenia solium (neurocysticercosis or cysticercosis) | [88,97] | |
| Toxoplasma gondii | [175,176,193,197,198,199,200,201] | |
| Treponema pallidum (syphilis) | [23,202,203,204,205] | |
| Bipolar disorders | Bartonella | [206,207,208] |
| Borrelia burgdorferi | [10,165,207,209,210,211] | |
| Cytomegalovirus | [57,176] | |
| Human endogenous retroviruses | [212] | |
| Mycoplasma | [207,213] | |
| Parvovirus B19 | [78] | |
| SARS-CoV-2 | [214,215] | |
| Tick-borne diseases | [216] | |
| Toxoplasma gondii | [176,217] | |
| Treponema pallidum (syphilis) | [205,218,219,220] | |
| Depressive disorders | Babesia | [91] |
| Bartonella | [27,28,162,208,221,222,223,224] | |
| Borrelia burgdorferi | [10,17,164,225,226,227,228,229,230,231] | |
| Borna disease virus | [47] | |
| Cytomegalovirus | [57] | |
| Enterovirus | [52] | |
| Hepatitis C virus | [61,62,63] | |
| Human immunodeficiency virus (HIV) | [68,232] | |
| Human T-cell lymphotropic virus type 1 (HTLV-1) | [69] | |
| Infections early in childhood | [137] | |
| Measles virus (subacute sclerosing panencephalitis) | [75] | |
| Plasmodium (malaria) | [233,234] | |
| SARS-CoV-2 and other coronaviruses: | [50,51,81,235] | |
| Taenia solium (neurocysticercosis or cysticercosis) | [96,97,98] | |
| Treponema pallidum (syphilis) | [23,205,218,220] | |
| West Nile virus | [86,87,236] | |
| Anxiety disorders | Bartonella | [27,206,207,221,224] |
| Borrelia burgdorferi | [10,164,211,229,237,238] | |
| Epstein–Barr virus | [239] | |
| Human T-cell lymphotropic virus type 1 | [69] | |
| Mycoplasma pneumoniae | [38,207,240,241] | |
| SARS-CoV-2 | [50,81,84,235,242] | |
| Streptococcus pyogenes (group A strep) | [240,243] | |
| Treponema pallidum (syphilis) | [205] | |
| Suicidality | All infections requiring hospitalization (including infections requiring hospitalization for COPD) | [244] |
| Bartonella | [162,206,208] | |
| Borrelia burgdorferi | [10,11,165,209,228,231,245,246] | |
| Cytomegalovirus | [57] | |
| Hepatitis C virus | [247] | |
| Herpes simplex virus type 1 (HSV-1) | [248] | |
| Human immunodeficiency virus (HIV) | [249] | |
| Influenza virus | [250] | |
| SARS-CoV-2 | [251,252] | |
| Streptococcus pyogenes (group A Strep) | [253] | |
| Toxoplasma gondii | [254] | |
| Aggressive or violent behavior | Babesia | [91] |
| Bartonella | [25,26,162,207,221] | |
| Borrelia burgdorferi | [10,16,209,211,246,255,256] | |
| Encephalitis lethargica agent | [257,258] | |
| Hepatitis E virus | [259] | |
| Herpes simplex virus | [260,261] | |
| Infection during childhood | [262] | |
| Measles virus (subacute sclerosing panencephalitis) | [75] | |
| Mycoplasma | [38,263] | |
| Parvovirus | [77] | |
| Plasmodium (Malaria) | [264,265] | |
| Rabies virus | [266,267,268] | |
| SARS-CoV-2 | [81] | |
| Streptococcus pyogenes (group A Strep) | [208,241] | |
| Toxoplasma gondii (toxoplasmosis) | [269] | |
| Treponema pallidum (syphilis) | [204,270,271] | |
| Viral encephalitis | [272] | |
| Animal models of infections associated with aggression include Borrelia burgdorferi in dogs, Bartonella henselae in dogs, B. henselae in horses, B. burgdorferi postulated in chimpanzee in lay news, rabies virus in multiple animal species, and gut microbiota in dogs, horses, and pigs. | [273,274,275,276,277,278,279,280,281,282,283] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Bransfield, R.C.; Mao, C.; Greenberg, R. Microbes and Mental Illness: Past, Present, and Future. Healthcare 2024, 12, 83. https://doi.org/10.3390/healthcare12010083
AMA Style
Bransfield RC, Mao C, Greenberg R. Microbes and Mental Illness: Past, Present, and Future. Healthcare. 2024; 12(1):83. https://doi.org/10.3390/healthcare12010083
Chicago/Turabian StyleBransfield, Robert C., Charlotte Mao, and Rosalie Greenberg. 2024. "Microbes and Mental Illness: Past, Present, and Future" Healthcare 12, no. 1: 83. https://doi.org/10.3390/healthcare12010083
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.