
Self-Management Interventions for Adults Living with Type II Diabetes to Improve Patient-Important Outcomes: An Evidence Map

 , , , , , , , , , , , , , and add
Show full author list
, , , , , , , , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Screening and Selection Process
2.3. Data Extraction and Collection
2.4. Data Analysis
3. Results
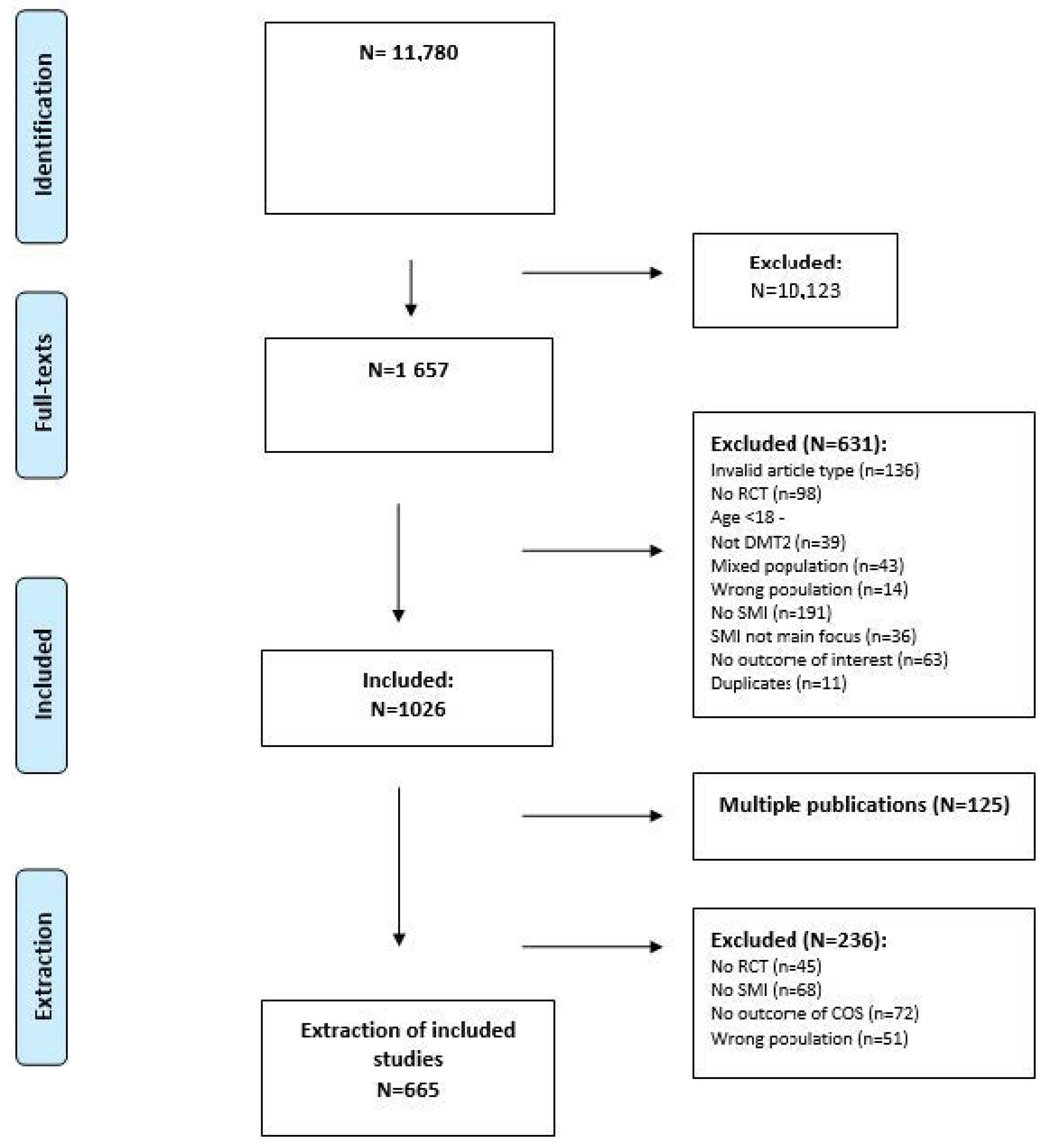
3.1. Search Results
3.2. Key Characteristics of Included RCTs
3.3. Characteristics of the Participants
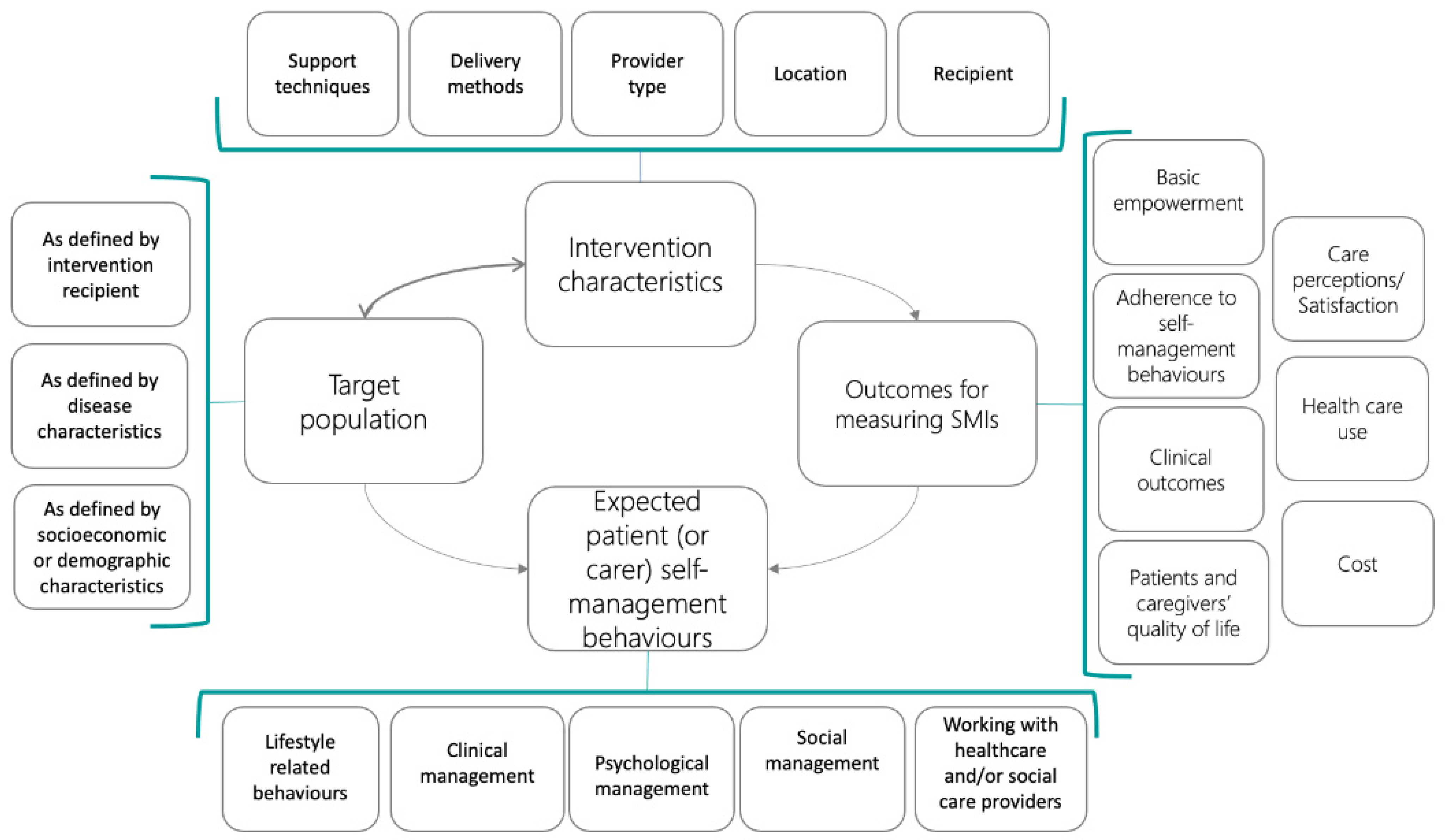
3.4. Characteristics of the SMIs Reported
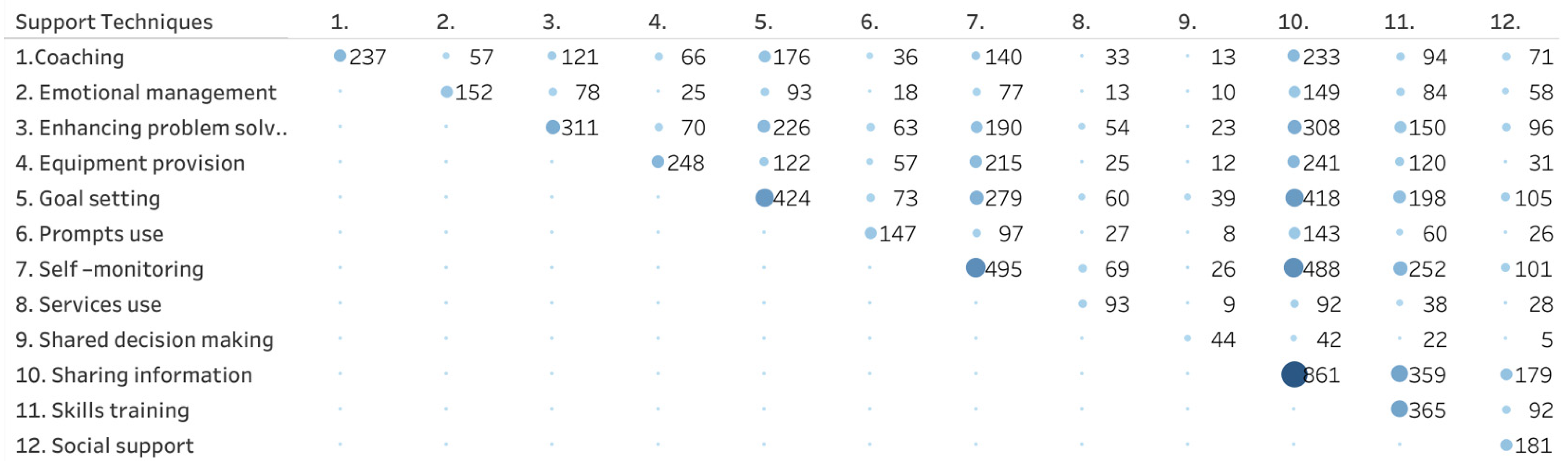
3.4.1. Self-Management Support Techniques
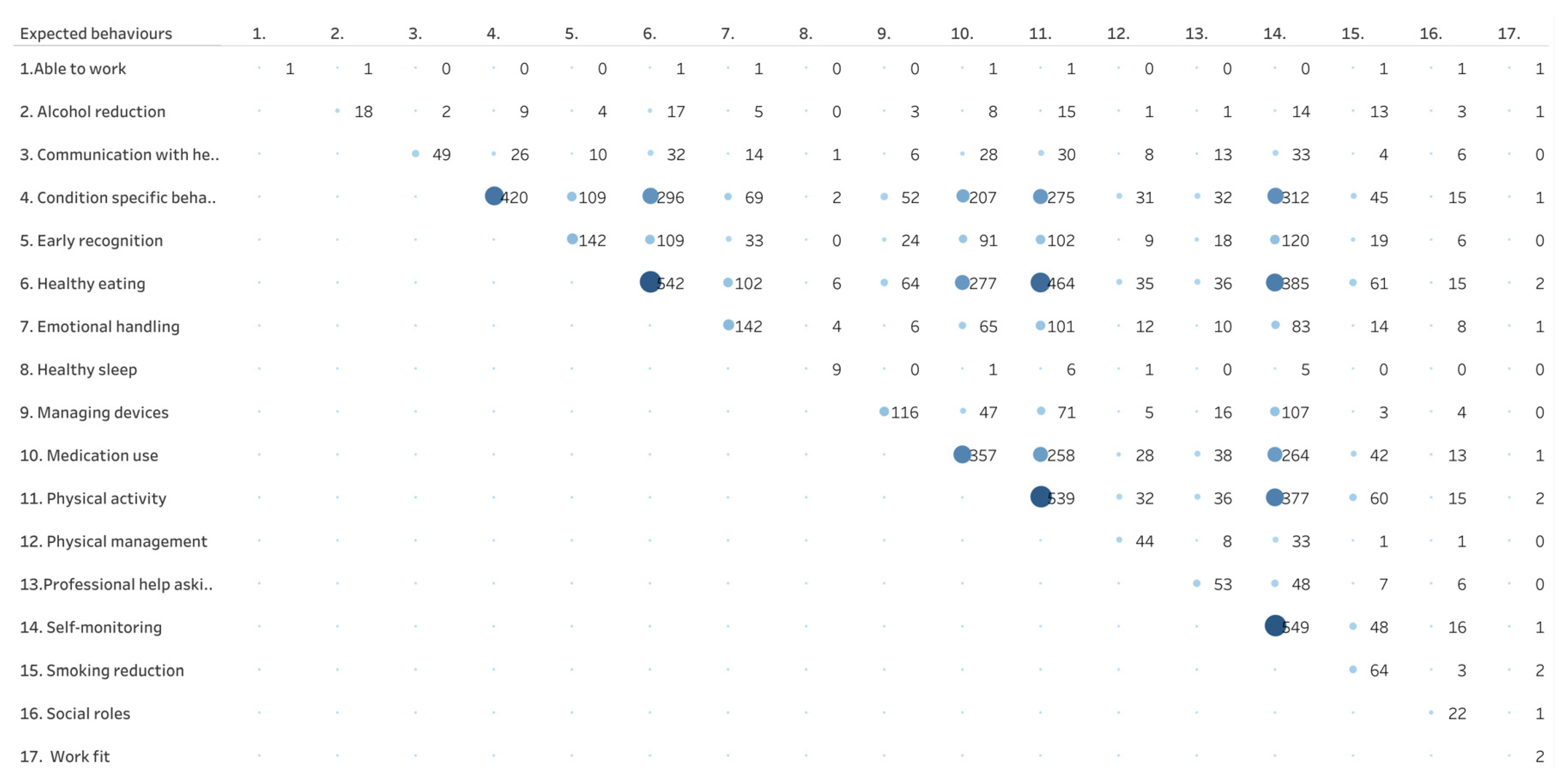
3.4.2. Expected Self-Management Behaviors
3.4.3. Mode of Delivery
3.5. Outcomes Reported in the Included RCTs
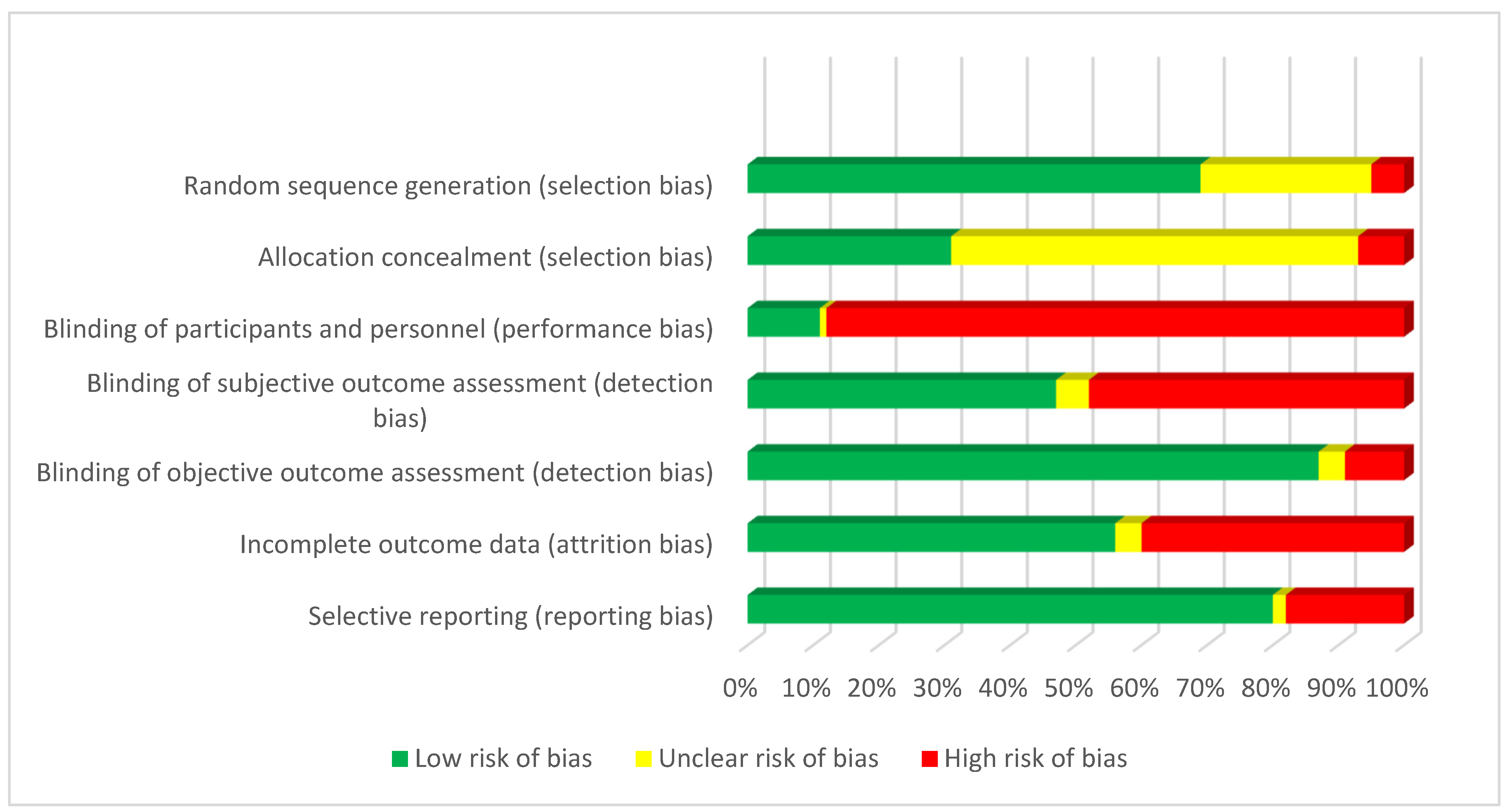
3.6. Risk of Bias of the Included Studies
4. Discussion
4.1. Main Findings
4.2. Study Findings in the Context of Other Research
4.3. Limitations and Strengths of This Study
4.4. Implication for Practice and Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy for Diabetes
| PubMed Search | Query | Items Found |
| #3 | #1 AND #2 AND #3 Filters: Publication date from 1 January 2010 | 6988 |
| #3 | (“Clinical Trials as Topic”[Mesh] OR “Randomized Controlled Trial”[pt] OR “Controlled Clinical Trial”[pt] OR randomized[tiab] OR randomly[tiab] OR placebo[tiab] OR trial[ti]) NOT (animals[mh] NOT humans[mh]) | 1,166,396 |
| #2 | “Self Care”[Mesh] OR “Self-Management”[Mesh] OR “Power (Psychology)”[Mesh] OR “Health Education”[Mesh] OR “Patient Participation”[Mesh] OR “Decision Making”[Mesh] OR “Telemedicine”[Mesh] OR self-administration*[tiab] OR self-care[tiab] OR self efficac*[tiab] OR self-manag*[tiab] OR selfmanag*[tiab] OR self-monitor*[tiab] OR selfmonitor*[tiab] OR self-diagnos*[tiab] OR selfdiagnos*[tiab] OR self-assess*[tiab] OR selfassess*[tiab] OR self-direct*[tiab] OR selfdirect*[tiab] OR self-help*[tiab] OR empower*[tiab] OR enablement[tiab] OR health education[tiab] OR patient education[tiab] OR patient participation[tiab] OR coach*[tiab] OR health promot*[tiab] OR ((community[tiab] OR peer[tiab]) AND (support*[tiab] OR advice*[tiab] OR monitor*[tiab] OR train*[tiab] OR instruction*[tiab] OR intervention*[tiab] OR consult*[tiab] OR assist*[tiab] OR educat*[tiab] OR information*[tiab] OR skill*[tiab])) OR group support*[tiab] OR group intervention*[tiab] OR group advice*[tiab] OR group monitor*[tiab] OR group train*[tiab] OR training group*[tiab] OR group instruct*[tiab] OR group assist*[tiab] OR group educat*[tiab] OR group inform*[tiab] OR group skill*[tiab] OR ((patient[tiab] OR patients[tiab]) AND (centered[tiab] OR centred[tiab] OR focus*[tiab] of directed[tiab] OR coach*[tiab] OR engage*[tiab] OR involve*[tiab] OR orient*[tiab] OR participat*[tiab])) OR ((patient[tiab] OR patients[tiab]) AND (educat*[tiab] OR train*[tiab] OR instruct*[tiab] OR teach*[tiab])) OR (management*[tiab] AND (plan[tiab] OR program*[tiab] OR disease[tiab])) OR (symptom*[tiab] AND (management[tiab] OR directed[tiab] OR focus*[tiab])) OR ((personalized[tiab] OR personalized[tiab]) AND care[tiab]) OR telemedicine[tiab] OR eHealth[tiab] OR e-Health[tiab] OR mHealth[tiab] OR m-Health[tiab] OR shared decision*[tiab] OR sharing decision*[tiab] OR informed decision*[tiab] OR informed choice*[tiab] or decision aid*[tiab] OR ((share*[ti] OR sharing*[ti] OR informed*[ti]) AND (decision*[ti] OR deciding*[ti] OR choice*[ti])) | 1,902,834 |
| #1 | “Diabetes Mellitus”[Mesh] OR diabet*[tiab] | 626,033 |
Appendix B. Description Self-Management Support Techniques from Taxonomy (Source: Orrego, Health Expect. 2021)
This term refers to training techniques for watching, registering and/or encouraging and following up with a person to keep a record of specified behavior, symptoms or clinical data. It could include feedback from clinicians or from the technology of maintained records on a regular basis to encourage the continuation of monitoring, e.g., advising patients how to register symptoms and signs such as glycemia, physical activity, pain level, etc.
|

Appendix C. Description of Expected Behaviors in SMI from Taxonomy (Source: Orrego, Health Expect. 2021)
Lifestyle-related behaviors
Clinical management Referred to decisions and actions specifically related to the physical dimension of self-management. It could include self-monitoring of signs and symptoms, medication use, early recognition of symptoms or physical management of the chronic disease.
Psychological management This area is related to handling and managing emotions in different stages of the condition and using these skills to improve a great variety of situations.
Social management The ability to interact with other persons and to build relationships in different spaces of exchange with people, i.e., social communities, at work, etc.
Working with healthcare and/or social care providers This sub-domain involves the capacity and skills development of patients to work with healthcare providers as nurses or physicians and/or social care providers
|
References
- WHO. Global Action Plan for the Prevention and Control of NCDs 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Lin, X.; Xu, Y.; Pan, X.; Xu, J.; Ding, Y.; Sun, X. Global, regional, and national burden and trend of diabetes in 195 countries and territories: An analysis from 1990 to 2025. Sci. Rep. 2020, 10, 14790. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Eakin, E.G. Issues in Diabetes Self-Management. The Handbook of Health Behavior Change, 2nd ed.; Springer Publishing Company: New York, NY, USA, 1998; pp. 435–461. [Google Scholar]
- Peyrot, M.; Rubin, R.R.; Lauritzen, T.; Snoek, F.J.; Matthews, D.R.; Skovlund, S.E. Psychosocial problems and barriers to improved diabetes management: Results of the Cross-National Diabetes Attitudes, Wishes and Needs (DAWN) Study. Diabet. Med. 2005, 22, 1379–1385. [Google Scholar] [CrossRef] [PubMed]
- Effing, T.W.; Bourbeau, J.; Vercoulen, J.; Apter, A.J.; Coultas, D.; Meek, P.; Valk, P.V.; Partridge, M.R.; van Palen, J. Self-management programmes for COPD: Moving forward. Chron. Respir. Dis. 2012, 9, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, R.; DiChiacchio, T.; Barker, K. Interventions for self-management of type 2 diabetes: An integrative review. Int. J. Nurs. Sci. 2018, 14, 70–91. [Google Scholar] [CrossRef] [PubMed]
- Jonkman, N.H.; Schuurmans, M.J.; Jaarsma, T.; Shortridge-Baggett, L.M.; Hoes, A.W.; Trappenburg, J.C. Self-management interventions: Proposal and validation of a new operational definition. J. Clin. Epidemiol. 2016, 80, 34–42. [Google Scholar] [CrossRef]
- Captieux, M.; Pearce, G.; Parke, H.L.; Epiphaniou, E.; Wild, S.; Taylor, S.J.C. Supported self-management for people with type 2 diabetes: A meta-review of quantitative systematic reviews. BMJ Open 2018, 8, e024262. [Google Scholar] [CrossRef]
- Chrvala, C.A.; Sherr, D.; Lipman, R.D. Diabetes self-management education for adults with type 2 diabetes mellitus: A systematic review of the effect on glycemic control. Patient Educ. Couns. 2016, 99, 926–943. [Google Scholar] [CrossRef] [PubMed]
- Orrego, C.; Ballester, M.; Heymans, M.; Camus, E.; Groene, O.; Nino de Guzman, E.; Pardo-Hernandez, H.; Sunol, R.; COMPAR-EU Group. Talking the same language on patient empowerment: Development and content validation of a taxonomy of self-management interventions for chronic conditions. Health Expect. 2021, 24, 1626–1638. [Google Scholar] [CrossRef]
- Valli, C.; Suñol, R.; Orrego, C.; Niño de Guzmán, E.; Strammiello, V.; Adrion, N.; Immonen, K.; Ninov, L.; van der Gaag, M.; Ballester, M.; et al. The development of a core outcomes set for self-management interventions for patients living with obesity. Clin. Obes. 2022, 12, e12489. [Google Scholar] [CrossRef]
- Miake-Lye, I.M.; Hempel, S.; Shanman, R.; Shekelle, P.G. What is an evidence map? A systematic review of published evidence maps and their definitions, methods, and products. Syst. Rev. 2016, 10, 5–28. [Google Scholar] [CrossRef]
- Campbell, F.; Tricco, A.C.; Munn, Z.; Pollock, D.; Saran, A.; Sutton, A.; White, H.; Khalil, H. Mapping reviews, scoping reviews, and evidence and gap maps (EGMs): The same but different—The “Big Picture” review family. Syst. Rev. 2023, 12, 45. [Google Scholar] [CrossRef]
- Bragge, P.; Clavisi, O.; Turner, T.; Tavender, E.; Collie, A.; Gruen, R.L. The Global Evidence Mapping Initiative: Scoping research in broad topic areas. BMC Med. Res. Methodol. 2011, 11, 92. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Ballester, M.; Orrego, C.; Heijmans, M.; Alonso-Coello, P.; Versteegh, M.M.; Mavridis, D.; Groene, O.; Immonen, K.; Wagner, C.; Canelo-Aybar, C.; et al. Comparing the effectiveness and cost-effectiveness of self-management interventions in four high-priority chronic conditions in Europe (COMPAR-EU): A research protocol. BMJ Open. 2020, 10, e034680. [Google Scholar] [CrossRef] [PubMed]
- PRO-STEP Consortium. Promoting Self-Management for Chronic Diseases in the EU-PROSTEP Project. 2018. Available online: https://wwweu-patienteu/projects/completed-projects/prostep/ (accessed on 12 June 2023).
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.J.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Goodall, T.A.; Halford, W.K. Self-management of diabetes mellitus: A critical review. Health Psychol. 1991, 10, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Celik, A.; Forde, R.; Sturt, J. The impact of online self-management interventions on midlife adults with type 2 diabetes: A systematic review. Br. J. Nurs. 2020, 29, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Agyemang, C.; van der Linden, E.L.; Bennet, L. Type 2 diabetes burden among migrants in Europe: Unravelling the causalpathways. Diabetologia 2021, 64, 2665–2675. [Google Scholar] [CrossRef]
- Skovlund, S.E.; Troelsen, L.H.; Klim, L.; Jakobsen, P.E.; Ejskjaer, N. The participatory development of a national core set of person-centred diabetes outcome constructs for use in routine diabetes care across healthcare sectors. Res. Involv. Engagem. 2021, 7, 62. [Google Scholar] [CrossRef]
- Santana, M.J.; Manalili, K.; Jolley, R.J.; Zelinsky, S.; Lu, M. How to practice person-centred care: A conceptual framework. Health Expect. 2018, 21, 429–440. [Google Scholar] [CrossRef] [PubMed]
- Noordman, J.; Heijmans, M.; Poortvliet, R.; Groene, O.; Ballester, M.; Ninov, L.; Niño de Guzmán, E.; Alonso-Coello, P.; Orrego, C.; Suñol, R. Identifying most important contextual factors for the implementation of self-management interventions: A Delphi study. Patient Educ. Couns. 2023, 114, 107843. [Google Scholar] [CrossRef] [PubMed]
- Mikhael, E.M.; Hassali, M.A.; Hussain, S.A. Effectiveness of Diabetes Self-Management Educational Programs For Type 2 Diabetes Mellitus Patients In Middle East Countries: A Systematic Review. Diabetes Metab. Syndr. Obes. 2020, 13, 117–138. [Google Scholar] [CrossRef] [PubMed]
- Lambrinou, E.; Hansen, T.B.; Beulens, J.W. Lifestyle factors, self-management and patient empowerment in diabetes care. Eur. J. Prev. Cardiol. 2019, 26 (Suppl. S2), 55–63. [Google Scholar] [CrossRef]
- Heijmans, M.; Poortvliet, R.; Van der Gaag, M.; González-González, A.I.; Beltran Puerta, J.; Canelo-Aybar, C.; Valli, C.; Ballester, M.; Rocha, C.; Garcia, M.L.; et al. Using a taxonomy to systematically identify and describe self-management interventions components in randomized trials for COPD. Int. J. Environ. Res. Public Health 2022, 19, 12685. [Google Scholar] [CrossRef]
- Sunol, R.; González-González, A.I.; Valli, C.; Ballester, M.; Seils, L.; Heijmans, M.; Poortvliet, R.; van der Gaag, M.; Rocha, C.; León-García, M.; et al. Self-management interventions for adults living with obesity to improve patient-relevant outcomes: An evidence map. Patient Educ. Couns. 2023, 110, 107647. [Google Scholar] [CrossRef]
- Creber, A.; Leo, D.G.; Buckley, B.J.; Chowdhury, M.; Harrison, S.L.; Isanejad, M.; Lane, D.A.; TAILOR investigators. Use of telemonitoring in patient self-management of chronic disease: A qualitative meta-synthesis. BMC Cardiovasc. Disord. 2023, 23, 469. [Google Scholar] [CrossRef]
- Litchfield, I.; Barrett, T.; Hamilton-Shield, J.; Moore, T.; Narendran, P.; Redwood, S.; Searle, A.; Uday, S.; Wheeler, J.; Greenfield, S.; et al. Current evidence for designing self-management support for underserved populations: An integrative review using the example of diabetes. Int. J. Equity Health 2023, 22, 188. [Google Scholar] [CrossRef]
- Nowakowska, M.; Zghebi, S.S.; Ashcroft, D.M.; Buchan, I.; Chew-Graham, C.; Holt, T.; Mallen, C.; Van Marwijk, H.; Peek, N.; Perera-Salazar, R.; et al. The comorbidity burden of type 2 diabetes mellitus: Patterns, clusters and predictions from a large English primary care cohort. BMC Med. 2019, 17, 145. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics of Included RCTs | N (%) | |
|---|---|---|
| Country (Top 5) | US | 233 (35%) |
| Iraq | 47 (7%) | |
| United Kingdom | 41 (6%) | |
| China | 37 (6%) | |
| Korea | 30 (5%) | |
| Type of population | Patient | 655 (99%) |
| Caregiver | 1 (0%) | |
| Mixed | 8 (1%) | |
| Type of comparison | Head-to-head interventions | 135 (20%) |
| Intervention(s) vs usual care | 530 (80%) | |
| Type of usual care (n = 530) | Usual care | 367 (69%) |
| Usual care plus | 163 (31%) | |
| Number of arms across all interventions (n = 665) | 2 | 598 (90%) |
| 3 | 56 (8%) | |
| 4 | 10 (2%) | |
| 5 | 1 (0%) | |
| Unit of allocation | By individual | 612 (92%) |
| At population level | 53 (8%) | |
| Specific target population | T2DM with low SES | 72 (11%) |
| T2DM from minority groups | 89 (13%) | |
| T2DM with low Health Literacy | 29 (4%) | |
| T2DM with comorbidities | 88 (13%) | |
| Characteristics of the total population included across interventions | Mean (SD) | |
| % women Mean age | 57.0 (49.0–67.0) 57.6 (54.3–61.5) | |
| Mean number of years since diagnosis | 8.6 (6.6–10.8) | |
| Mean HbA1c | 8.2 (7.6–8.9) | |
| Support Techniques | Type | n | % |
|---|---|---|---|
| Educational | Sharing information | 861 | 98% |
| Skills training | 365 | 42% | |
| Monitoring | Self-monitoring | 495 | 56% |
| Prompt use | 147 | 17% | |
| Behavioral change-action based | Goal setting | 424 | 48% |
| Enhancing problem-solving | 311 | 35% | |
| Behavioral change-emotion based | Coaching | 237 | 27% |
| Emotional management | 152 | 17% | |
| Social support | Using social support | 181 | 21% |
| Shared Decision Making (SDM) | SDM | 44 | 5% |
| Use of external resources | Service use | 93 | 11% |
| Equipment provision | 248 | 28% | |
| Expected self-management behaviors | Type | n | % |
| Lifestyle-related | Healthy eating | 542 | 62% |
| Physical activity | 539 | 61% | |
| Smoking reduction | 64 | 7% | |
| Alcohol reduction | 18 | 2% | |
| Healthy sleep | 9 | 1% | |
| Clinical management | Self-monitoring (e.g., blood sugar) | 549 | 63% |
| Condition-specific behavior | 420 | 48% | |
| Medication use | 357 | 41% | |
| Early recognition of symptoms | 142 | 16% | |
| Managing devices | 116 | 13% | |
| Professional help-seeking | 53 | 6% | |
| Physical management | 55 | 5% | |
| Psychological management | Handling emotions | 142 | 16% |
| Social management | Fulfilling social roles | 22 | 3% |
| Able to work/being fit | 3 | 1% | |
| Experience with care | Communication with healthcare | 49 | 6% |
| Type of encounter | n | % | |
| Clinical visits | 85 | 10% | |
| Support sessions | 465 | 53% | |
| Self-guided | 98 | 11% | |
| Combination | 229 | 26% | |
| Way of delivery | n | % | |
| Face-to-face | 395 | 45% | |
| Remote | 181 | 21% | |
| Combination | 293 | 33% | |
| Location | n | % | |
| Outpatient care | 376 | 43% | |
| Homecare | 207 | 24% | |
| Community care | 134 | 15% | |
| Primary care | 143 | 16% | |
| Virtual/online | 142 | 16% | |
| Other (hospital, work, long-term care) | 1–11 | <2% each | |
| Type of provider | n | % | |
| Nurse | 309 | 35% | |
| Physician | 177 | 20% | |
| Educator | 258 | 29% | |
| Nutritionist | 162 | 18% | |
| Other | <9% | ||
| Intensity | n | % | |
| Low intensity (<10 h) | 592 | 67% | |
| High intensity (≥10 h) | 286 | 33% |
| Category of Outcomes | Type | n | % |
|---|---|---|---|
| Basic empowerment | Self-efficacy | 120 | 18% |
| Knowledge | 109 | 16% | |
| Patient activation | 11 | 2% | |
| Health literacy | 3 | 0% | |
| Adherence to | Physical activity | 153 | 23% |
| Dietary habits | 106 | 16% | |
| Self-management activities in general | 111 | 17% | |
| Medication | 92 | 14% | |
| Smoking cessation | 14 | 2% | |
| Self-monitoring | 63 | 10% | |
| Clinical | HbA1c | 550 | 83% |
| Weight | 353 | 53% | |
| Lipid profile | 296 | 45% | |
| Blood pressure | 281 | 42% | |
| Hypoglycemia | 28 | 4% | |
| Hyperglycemia | 13 | 2% | |
| Complications | 15 | 2% | |
| Life expectancy | 2 | 0% | |
| Quality of life | Quality of life | 180 | 27% |
| Care perceptions | Participation in decision-making | 4 | 1% |
| Experience/satisfaction with care | 34 | 5% | |
| Health care use | Unscheduled care | 26 | 4% |
| Scheduled care | 13 | 2% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, Y.; Beltran Puerta, J.; Medina-Aedo, M.; Canelo-Aybar, C.; Valli, C.; Ballester, M.; Rocha, C.; Garcia, M.L.; Salas-Gama, K.; Kaloteraki, C.; et al. Self-Management Interventions for Adults Living with Type II Diabetes to Improve Patient-Important Outcomes: An Evidence Map. Healthcare 2023, 11, 3156. https://doi.org/10.3390/healthcare11243156
Song Y, Beltran Puerta J, Medina-Aedo M, Canelo-Aybar C, Valli C, Ballester M, Rocha C, Garcia ML, Salas-Gama K, Kaloteraki C, et al. Self-Management Interventions for Adults Living with Type II Diabetes to Improve Patient-Important Outcomes: An Evidence Map. Healthcare. 2023; 11(24):3156. https://doi.org/10.3390/healthcare11243156
Chicago/Turabian StyleSong, Yang, Jessica Beltran Puerta, Melixa Medina-Aedo, Carlos Canelo-Aybar, Claudia Valli, Marta Ballester, Claudio Rocha, Montserrat León Garcia, Karla Salas-Gama, Chrysoula Kaloteraki, and et al. 2023. "Self-Management Interventions for Adults Living with Type II Diabetes to Improve Patient-Important Outcomes: An Evidence Map" Healthcare 11, no. 24: 3156. https://doi.org/10.3390/healthcare11243156