
Physical Activity, Readiness, and Cardiovascular Risk Stratification in the Polytechnics Communities of the Northern Region of Portugal Integrated in Mobility as a Service Concept


Abstract
:1. Introduction
2. Materials and Methods
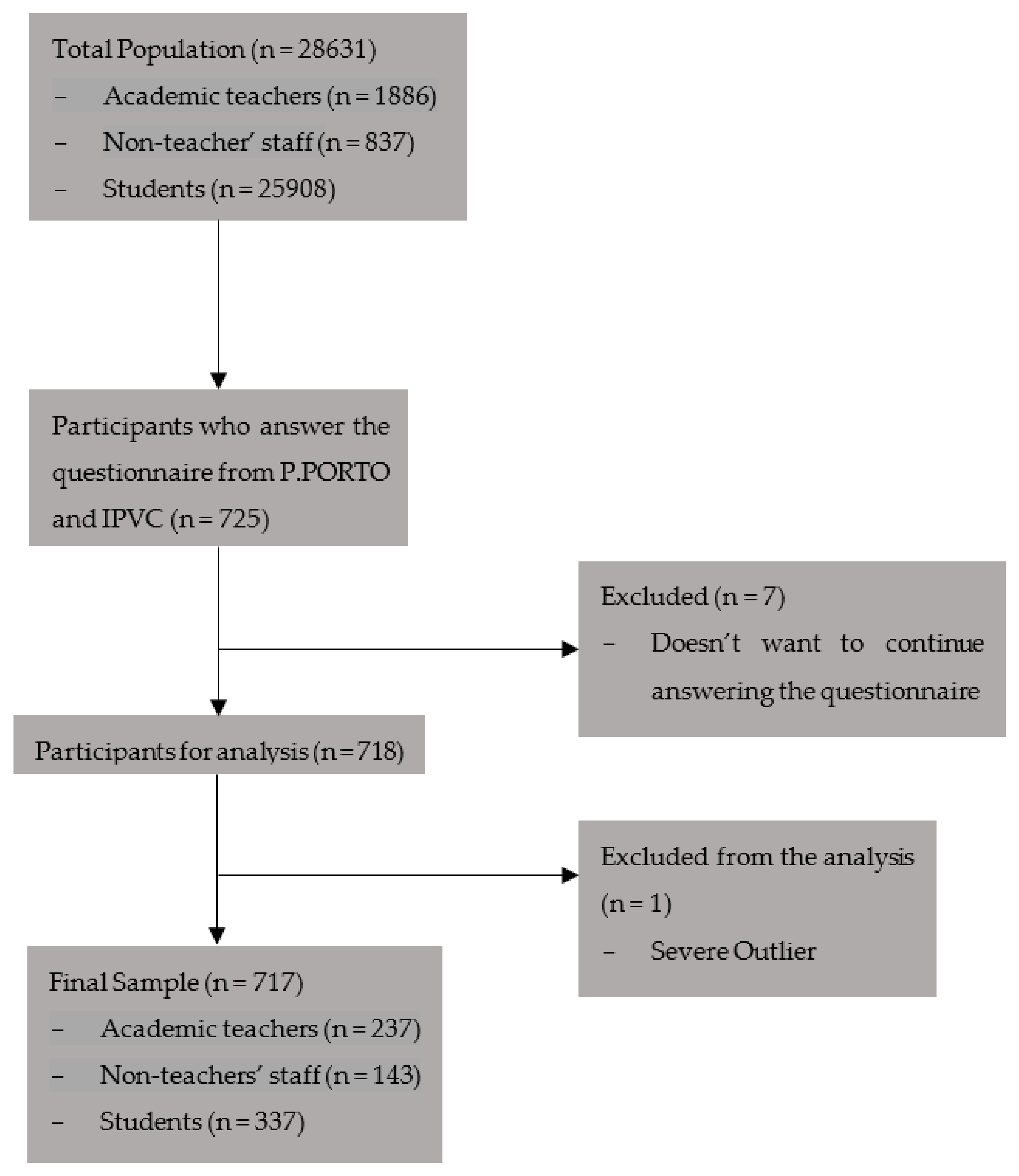
2.1. Participants
2.2. Instruments and Procedures
2.2.1. Characterization Data
2.2.2. PA Level Assessment
2.2.3. PA Readiness
2.2.4. Cardiovascular Risk Stratification
2.3. Statistical Analysis
3. Results
3.1. PA Level
3.2. PA Readiness
3.3. Cardiovascular Risk Stratification
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Status Report on Physical Activity; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- American College of Sports Medicine. ACSM’S Guidelines for Exercise Testing and Prescription, 8th ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2010. [Google Scholar]
- Kondamudi, N.; Mehta, A.; Thangada, N.D.; Pandey, A. Physical Activity and Cardiorespiratory Fitness: Vital Signs for Cardiovascular Risk Assessment. Curr. Cardiol. Rep. 2021, 23, 172. [Google Scholar] [CrossRef] [PubMed]
- Peluso, M.; Andrade, L. Phisical Activity and Mental Health: The Association Between Exercise and Mood. Clinics 2005, 60, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Alves, R.F.; Precioso, J.A.G. Exercício físico, sedentarismo e bem-estar dos/as estudantes universitários/as portugueses/as. Rev. Contexto Saúde 2022, 22, e13371. [Google Scholar] [CrossRef]
- Carballo-Fazanes, A.; Rico-Díaz, J.; Barcala-Furelos, R.; Rey, E.; Rodríguez-Fernández, J.E.; Varela-Casal, C.; Abelairas-Gómez, C. Physical Activity Habits and Determinants, Sedentary Behaviour and Lifestyle in University Students. Int. J. Environ. Res. Public Health 2020, 17, 3272. [Google Scholar] [CrossRef] [PubMed]
- Gerber, M.; Brand, S.; Herrmann, C.; Colledge, F.; Holsboer-Trachsler, E.; Pühse, U. Increased objectively assessed vigorous-intensity exercise is associated with reduced stress, increased mental health and good objective and subjective sleep in young adults. Physiol. Behav. 2014, 135, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Redondo-Flórez, L.; Tornero-Aguilera, J.F.; Ramos-Campo, D.J.; Clemente-Suárez, V.J. Gender Differences in Stress- and Burnout-Related Factors of University Professors. BioMed Res. Int. 2020, 2020, 6687358. [Google Scholar] [CrossRef] [PubMed]
- Rimmele, U.; Seiler, R.; Marti, B.; Wirtz, P.H.; Ehlert, U.; Heinrichs, M. The level of physical activity affects adrenal and cardiovascular reactivity to psychosocial stress. Psychoneuroendocrinology 2009, 34, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Schultchen, D.; Reichenberger, J.; Mittl, T.; Weh, T.R.M.; Smyth, J.M.; Blechert, J.; Pollatos, O. Bidirectional relationship of stress and affect with physical activity and healthy eating. Br. J. Health Psychol. 2019, 24, 315–333. [Google Scholar] [CrossRef]
- European Commission; Directorate General for Education, Youth, Sport and Culture. Sport and Physical Activity: Full Report; Publications Office of the European Union: Luxembourg, 2022; Available online: https://data.europa.eu/doi/10.2766/356346 (accessed on 5 September 2023).
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018; 101p, Available online: https://apps.who.int/iris/handle/10665/272722 (accessed on 5 September 2023).
- Hietanen, S. Mobility as a Service’—The new transport model? ITS Transp. Manag. Suppl. 2014, 12, 1–4. [Google Scholar]
- Jittrapirom, P.; Caiati, V.; Feneri, A.M.; Ebrahimigharehbaghi, S.; González, M.J.A.; Narayan, J. Mobility as a Service: A Critical Review of Definitions, Assessments of Schemes, and Key Challenges. Urban Plan. 2017, 2, 13–25. [Google Scholar] [CrossRef]
- Cruz-Rodríguez, J.; Luque-Sendra, A.; Heras, A.D.L.; Zamora-Polo, F. Analysis of Interurban Mobility in University Students: Motivation and Ecological Impact. Int. J. Environ. Res. Public Health 2020, 17, 9348. [Google Scholar] [CrossRef] [PubMed]
- Fissi, S.; Romolini, A.; Gori, E.; Contri, M. The path toward a sustainable green university: The case of the University of Florence. J. Clean. Prod. 2021, 279, 123655. [Google Scholar] [CrossRef]
- Silva, J.P.D.; Fischer, F.M. Understudied school teachers’ work/life balance and everyday life typologies. Chronobiol. Int. 2020, 37, 1513–1515. [Google Scholar] [CrossRef] [PubMed]
- Pace, F.; D’Urso, G.; Zappulla, C.; Pace, U. The relation between workload and personal well-being among university professors. Curr. Psychol. 2021, 40, 3417–3424. [Google Scholar] [CrossRef]
- American College of Sports Medicine. Health Care Providers Action Guide: Exercise is Medicine; American College of Sports Medicine: Indianapolis, IN, USA, 2021. [Google Scholar]
- Thompson, W.R.; Sallis, R.; Joy, E.; Jaworski, C.A.; Stuhr, R.M.; Trilk, J.L. Exercise Is Medicine. Am. J. Lifestyle Med. 2020, 14, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Campaniço, H. Validade Simultânea do Questionário Internacional de Actividade Física Através da Medição Objectiva da Actividade Física por Actigrafia Proporcional. Master’s Thesis, Faculdade de Motricidade Humana, Universidade de Lisboa, Lisbon, Portugal, 2016. [Google Scholar]
- Fan, M.; Lyu, J.; He, P. Guidelines for data processing and analysis of the International Physical Activity Questionnaire (IPAQ). Zhonghua Liu Xing Bing Xue Za Zhi Zhonghua Liuxingbingxue Zazhi 2014, 35, 961–964. [Google Scholar] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Meh, K.; Jurak, G.; Sorić, M.; Rocha, P.; Sember, V. Validity and Reliability of IPAQ-SF and GPAQ for Assessing Sedentary Behaviour in Adults in the European Union: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4602. [Google Scholar] [CrossRef]
- Schwartz, J.; Oh, P.; Takito, M.Y.; Saunders, B.; Dolan, E.; Franchini, E.; Rhodes, R.E.; Bredin, S.S.D.; Coelho, J.P.; dos Santos, P.; et al. Translation, Cultural Adaptation, and Reproducibility of the Physical Activity Readiness Questionnaire for Everyone (PAR-Q+): The Brazilian Portuguese Version. Front. Cardiovasc. Med. 2021, 8, 712696. [Google Scholar] [CrossRef]
- Fahim, N.K.; Negida, A. Sample Size Calculation Guide—Part 1: How to Calculate the Sample Size Based on the Prevalence Rate. Adv. J. Emerg. Med. 2018, 2, e50. [Google Scholar]
- Sedgwick, P. Questionnaire surveys: Sources of bias. BMJ 2013, 347, f5265. [Google Scholar] [CrossRef]
- Alves, R.; Gomes Precioso, J.A.; Becoña Iglesias, E. Physical activity among Portuguese university students and its relation to knowledge and perceived barriers. Sport. Sci. J. Sch. Sport Phys. Educ. Psychomot. 2021, 7, 25–42. [Google Scholar] [CrossRef]
- Clemente, F.M.; Nikolaidis, P.T.; Martins, F.M.L.; Mendes, R.S. Physical Activity Patterns in University Students: Do They Follow the Public Health Guidelines? PLoS ONE 2016, 11, e0152516. [Google Scholar] [CrossRef] [PubMed]
- Kljajević, V.; Stanković, M.; Đorđević, D.; Trkulja-Petković, D.; Jovanović, R.; Plazibat, K.; Oršolić, M.; Čurić, M.; Sporiš, G. Physical Activity and Physical Fitness among University Students—A Systematic Review. Int. J. Environ. Res. Public Health 2021, 19, 158. [Google Scholar] [CrossRef] [PubMed]
- Almhdawi, K.A.; Obeidat, D.; Kanaan, S.F.; Hajela, N.; Bsoul, M.; Arabiat, A.; Alazrai, A.; Jaber, H.; Alrabbaie, H. University professors’ mental and physical well-being during the COVID-19 pandemic and distance teaching. Work 2021, 69, 1153–1161. [Google Scholar] [CrossRef] [PubMed]
- Santos, G.M.R.F.D.; Silva, M.E.D.; Belmonte, B.D.R. COVID-19: Emergency remote teaching and university professors’ mental health. Rev. Bras. Saúde Mater. Infant. 2021, 21 (Suppl. S1), 237–243. [Google Scholar] [CrossRef]
- Kwiecień-Jaguś, K.; Mędrzycka-Dąbrowska, W.; Kopeć, M.; Piotrkowska, R.; Czyż-Szypenbejl, K.; Hansdorfer-Korzon, R.; Lemska, M.; Jarzynkowski, P. Level and factors associated with physical activity among university teacher: An exploratory analysis. BMC Sports Sci. Med. Rehabil. 2021, 13, 114. [Google Scholar] [CrossRef] [PubMed]
- Güneş, F.E.; Bekiroglu, N.; Imeryuz, N.; Agirbasli, M. Awareness of cardiovascular risk factors among university students in Turkey. Prim. Health Care Res. Dev. 2019, 20, e127. [Google Scholar] [CrossRef]
- Cengel, A. Cardiovascular risk factors in women. Turk Kardiyol. Dern. Ars. Turk Kardiyol. Dern. Yayin Organidir 2010, 38 (Suppl. S1), 17–24. [Google Scholar]
- Hayman, L.L.; Williams, C.L.; Daniels, S.R.; Steinberger, J.; Paridon, S.; Dennison, B.A.; McCrindle, B.W. Cardiovascular Health Promotion in the Schools: A Statement for Health and Education Professionals and Child Health Advocates from the Committee on Atherosclerosis, Hypertension, and Obesity in Youth (AHOY) of the Council on Cardiovascular Disease in the Young, American Heart Association. Circulation 2004, 110, 2266–2275. [Google Scholar]
- Maas, B. Literature Review of Mobility as a Service. Sustainability 2022, 14, 8962. [Google Scholar] [CrossRef]


{kind=link}
| Study Participants | Academic Teachers (n = 237) | Non-Teacher Staff (n = 147) | Students (n = 337) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD (95% CI) | Min–Max | Mean ± SD (95% CI) | Min–Max | Mean ± SD (95% CI) | Min–Max | Z | p | ||
| Age (years) | 48.28 ± 10.40 (46.94–49.64) | 22–72 | 38.30 ± 14.03 (36.08–40.71) | 19–65 | 26.23 ± 8.63 (25.37–27.15) | 19–60 | 310.418 | <0.001 * | P vs. NP < 0.001 * P vs. S < 0.001 * S vs. NP < 0.001 * |
| Weight (kg) | 71.37 ± 15.10 (69.49–73.51) | 43–130 | 66.77 ± 12.94 (64.76–68.91) | 43–99 | 66.51 ± 13.10 (65.03–67.87) | 40–112 | 9.717 | <0.001 * | P vs. NP = 0.005 * P vs. S < 0.001 * S vs. NP = 1 |
| Height (cm) | 1.70 ± 0.10 (1.68–1.71) | 1.42–1.93 | 1.66 ± 0.09 (1.65–1.68) | 1.50–1.92 | 1.69 ± 0.09 (1.68–1.70) | 1.50–1.98 | 6.461 | 0.002 * | P vs. NP = 0.001 * P vs. S = 0.570 S vs. NP = 0.023 * |
| BMI (kg/m2) | 24.70 ± 4.02 (24.22–25.21) | 15.96–43.44 | 24.13 ± 3.76 (23.54–24.78) | 17.48–38.79 | 23.33 ± 3.90 (22.92–23.74) | 15.82–40.98 | 8.429 | <0.001 * | P vs. NP = 0.515 P vs. S < 0.001 * S vs. NP = 0.140 |
| n (%) | χ2 | p | |||||||
| Underweight (<18.5) | 5 (2.1) | 4 (2.8) | 23 (6.8) | 28.190 | 0.001 * | ||||
| Normal weight (18.5–24.9) | 136 (57.6) | 93 (65.5) | 221 (65.6) | ||||||
| Overweight (25.0–29.9) | 68 (28.8) | 39 (27.5) | 73 (21.7) | ||||||
| Grade I obesity (30.0–34.9) | 24 (10.2) | 3 (2.1) | 13 (3.9) | ||||||
| Grade II obesity—severe (35.0–39.9) | 2 (0.8) | 3 (2.1) | 6 (1.8) | ||||||
| Grade III obesity—morbid (≥40.0) | 1 (0.4) | - | 1 (0.3) | ||||||
| n (%) | χ2 | p | |||||||
| History of cardiovascular, respiratory, and/or metabolic disease | 28 (11.8) | 18 (12.6) | 42 (12.5) | 0.657 | 0.957 | ||||
| Family history of coronary disease | 34 (14.3) | 17 (11.9) | 30 (8.9) | 9.768 | 0.045 * | ||||
| High blood pressure | 35 (14.8) | 23 (16.1) | 31 (9.2) | 9.251 | 0.137 | ||||
| Diabetes or prediabetes | 6 (2.5) | 6 (4.2) | 8 (2.4) | 1.316 | 0.518 | ||||
| High cholesterol | 55 (23.2) | 28 (19.6) | 33 (9.8) | 23.219 | <0.001 * | ||||
| Smoker | 30 (12.7) | 13 (9.1) | 33 (9.8) | 1.635 | 0.441 | ||||
| Total number of participants | 237 (33.05) | 143 (19.94) | 337 (47.00) | ||||||
| Study Participants | Academic Teachers | Non-Teacher Staff | Students | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD (95% CI) | Min–Max | Mean ± SD (95% CI) | Min–Max | Mean ± SD (95% CI) | Min–Max | Z | p | ||
| IPAQ Score | 2729.04 ± 2734.76 (2379.07–3079.00) | 0–24,556.80 | 2104.46 ± 1955.07 (1781.27–2427.66) | 0–11,880.00 | 3094.60 ± 2666.21 (2808.91–3380.29) | 0–24,840.00 | 7.542 | <0.001 * | P vs. NP = 0.605 P vs. S = 0.279 S vs. NP = <0.001 * |
| n (%) | χ2 | p | |||||||
| Sedentary (<600 MET/week) | 48 (20.25) | 33 (23.08) | 47 (13.95) | 15.245 | 0.004 * | ||||
| Moderate PA (600–3000 MET/week) | 100 (42.19) | 75 (52.45) | 153 (45.40) | ||||||
| Vigorous PA (>3000 MET/week) | 89 (37.55) | 35 (24.48) | 137 (40.65) | ||||||
| Total number of participants | 237 (33.05) | 143 (19.94) | 337 (47.00) | ||||||
| Study Participants | Academic Teachers | Non-Teacher Staff | Students | ||
|---|---|---|---|---|---|
| n (%) | χ2 | p | |||
| Cleared for PA | 118 (49.79) | 49 (34.27) | 162 (48.07) | 13.589 | 0.009 * |
| Ready to become more physically active, preferably after consulting a qualified professional | 62 (26.16) | 37 (25.87) | 79 (23.44) | ||
| Should seek further information before becoming more physically active or engaging in a fitness appraisal | 57 (24.05) | 57 (39.86) | 96 (28.49) | ||
| Total number of participants | 237 (33.05) | 143 (19.94) | 337 (47.00) | ||
| Study Participants | Academic Teachers | Non-Teacher Staff | Students | ||
|---|---|---|---|---|---|
| n (%) | χ2 | p | |||
| Low cardiovascular risk | 107 (45.15) | 74 (51.75) | 219 (64.98) | 88.589 | <0.001 * |
| Moderate cardiovascular risk | 97 (40.93) | 33 (23.08) | 28 (8.31) | ||
| High cardiovascular risk | 33 (13.92) | 36 (25.17) | 90 (26.71) | ||
| Total number of participants | 237 (33.05) | 143 (19.94) | 337 (47.00) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sousa, A.S.P.; Guedes, D.C.; Félix, J.; Pereira, S.; Santos, R. Physical Activity, Readiness, and Cardiovascular Risk Stratification in the Polytechnics Communities of the Northern Region of Portugal Integrated in Mobility as a Service Concept. Healthcare 2023, 11, 3145. https://doi.org/10.3390/healthcare11243145
Sousa ASP, Guedes DC, Félix J, Pereira S, Santos R. Physical Activity, Readiness, and Cardiovascular Risk Stratification in the Polytechnics Communities of the Northern Region of Portugal Integrated in Mobility as a Service Concept. Healthcare. 2023; 11(24):3145. https://doi.org/10.3390/healthcare11243145
Chicago/Turabian StyleSousa, Andreia S. P., Diana C. Guedes, José Félix, Soraia Pereira, and Rubim Santos. 2023. "Physical Activity, Readiness, and Cardiovascular Risk Stratification in the Polytechnics Communities of the Northern Region of Portugal Integrated in Mobility as a Service Concept" Healthcare 11, no. 24: 3145. https://doi.org/10.3390/healthcare11243145