
A Nutritional Supplement as Adjuvant of Gabapentinoids for Adults with Neuropathic Pain following Spinal Cord Injury and Stroke: Preliminary Results
 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
1.1. Neuropathic Pain from Stroke Outcomes or Spinal Cord Injury
1.2. The Management of Neuropathic Pain from Stroke or Spinal Cord Injury Outcomes: The Role of Gabapentinoids and Pregabalin
1.3. Difficulties in the Use of Gabapentinoids and Pregabalin in Patients with NP
1.4. The Role of Nutraceuticals as Adjuvants in the Treatment of NP
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Intervention
2.4. Measures
2.5. Data Analyses
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Treede, R.D.; Jensen, T.S.; Campbell, J.N.; Cruccu, G.; Dostrovsky, J.O.; Griffin, J.W.; Hansson, P.; Hughes, R.; Nurmikko, T.; Serra, J. Neuropathic pain: Redefinition and a grading system for clinical and research purposes. Neurology 2008, 70, 1630–1635. [Google Scholar] [CrossRef] [PubMed]
- Bouhassira, D.; Lantéri-Minet, M.; Attal, N.; Laurent, B.; Touboul, C. Prevalence of chronic pain with neuropathic characteristics in the general population. Pain 2008, 136, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Raffaeli, W.; Minella, C.E.; Magnani, F.; Sarti, D. Population-based study of central post-stroke pain in Rimini district, Italy. J. Pain Res. 2013, 6, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Magrinelli, F.; Zanette, G.; Tamburin, S. Neuropathic pain: Diagnosis and treatment. Pract. Neurol. 2013, 13, 292–307. [Google Scholar] [CrossRef]
- Fornasari, D. Pharmacotherapy for neuropathic pain: A review. Pain Ther. 2017, 6, 25–33. [Google Scholar] [CrossRef]
- Liampas, A.; Velidakis, N.; Georgiou, T.; Vadalouca, A.; Varrassi, G.; Hadjigeorgiou, G.M.; Tsivgoulis, G.; Zis, P. Prevalence and management challenges in central post-stroke neuropathic pain: A systematic review and meta-analysis. Adv. Ther. 2020, 37, 3278–3291. [Google Scholar] [CrossRef]
- Burke, D.; Fullen, B.M.; Stokes, D.; Lennon, O. Neuropathic pain prevalence following spinal cord injury: A systematic review and meta-analysis. Eur. J. Pain 2017, 21, 29–44. [Google Scholar] [CrossRef]
- Watson, J.C.; Sandroni, P. Central neuropathic pain syndromes. Mayo. Clin. Proc. 2016, 91, 372–385. [Google Scholar] [CrossRef]
- Balzani, E.; Fanelli, A.; Malafoglia, V.; Tenti, M.; Ilari, S.; Corraro, A.; Muscoli, C.; Raffaeli, W. A Review of the Clinical and Therapeutic Implications of Neuropathic Pain. Biomedicines 2021, 9, 1239. [Google Scholar] [CrossRef]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef]
- Derry, S.; Bell, R.F.; Straube, S.; Wiffen, P.J.; Aldington, D.; Moore, R.A. Pregabalin for neuropathic pain in adults. Cochrane Database Syst. Rev. 2019, 1, CD007076. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; O’Connor, A.B.; Backonja, M.; Farrar, J.T.; Finnerup, N.B.; Jensen, T.S.; Kalso, E.A.; Loeser, J.D.; Finnerup, N.B.; Jensen, T.S.; et al. Pharmacologic management of neuropathic pain: Evidence-based recommendations. Pain 2007, 132, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Goodman, C.W.; Brett, A.S. Gabapentin and pregabalin for pain—Is increased prescribing a cause for concern? N. Engl. J. Med. 2017, 377, 411–414. [Google Scholar] [CrossRef] [PubMed]
- Evoy, K.E.; Sadrameli, S.; Contreras, J.; Covvey, J.R.; Peckham, A.M.; Morrison, M.D. Abuse and Misuse of Pregabalin and Gabapentin: A Systematic Review Update. Drugs 2021, 81, 125–156. [Google Scholar] [CrossRef]
- Marchesi, N.; Govoni, S.; Allegri, M. Non-drug pain relievers active on non-opioid pain mechanisms. Pain Pract. 2022, 22, 255–275. [Google Scholar] [CrossRef]
- Geller, M.; Oliveira, L.; Nigri, R.; Mezitis, S.G.; Goncalves Ribeiro, M.; de Souza da Fonseca, A.; Guimaraes, O.R.; Kaufman, R.; Wajnsztajn, F. B Vitamins for Neuropathy and Neuropathic Pain. Vitam Min. 2017, 6, 1000161. [Google Scholar] [CrossRef]
- Calderón-Ospina, C.A.; Nava-Mesa, M.O. B Vitamins in the nervous system: Current knowledge of the biochemical modes of action and synergies of thiamine, pyridoxine, and cobalamin. CNS Neurosci. Ther. 2020, 26, 5–13. [Google Scholar] [CrossRef]
- Jurna, I. Analgesic and analgesia-potentiating action of B vitamins. Schmerz 1998, 12, 136–141. [Google Scholar] [CrossRef]
- Sun, J.; Chen, F.; Braun, C.; Zhou, Y.Q.; Rittner, H.; Tian, Y.K.; Cai, X.Y.; Ye, D.W. Role of curcumin in the management of pathological pain. Phytomedicine 2018, 48, 129–140. [Google Scholar] [CrossRef]
- Malek, N.; Pajak, A.; Kolosowska, N.; Kucharczyk, M.; Starowicz, K. The importance of TRPV1-sensitisation factors for the development of neuropathic pain. Mol. Cell. Neurosci. 2015, 65, 1–10. [Google Scholar] [CrossRef]
- Marrone, M.C.; Morabito, A.; Giustizieri, M.; Chiurchiu, V.; Leuti, A.; Mattioli, M.; Marinelli, S.; Riganti, L.; Lombardi, M.; Murana, E.; et al. TRPV1 channels are critical brain inflammation detectors and neuropathic pain biomarkers in mice. Nat. Commun. 2017, 8, 15292. [Google Scholar] [CrossRef] [PubMed]
- Naik, G.G.; Uniyal, A.; Chouhan, D.; Tiwari, V.; Sahu, A.N. Natural Products and some Semi-synthetic Analogues as Potential TRPV1 Ligands for Attenuating Neuropathic Pain. Curr. Pharm. Biotechno. 2022, 23, 766–786. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Xu, L.; Deng, X.; Jiang, C.; Pan, C.; Chen, L.; Han, Y.; Dai, W.; Hu, L.; Zhang, G.; et al. N-acetyl-cysteine attenuates neuropathic pain by suppressing matrix metalloproteinases. Pain 2016, 157, 1711–1723. [Google Scholar] [CrossRef] [PubMed]
- Truini, A.; Piroso, S.; Pasquale, E.; Notartomaso, S.; Stefano, G.D.; Lattanzi, R.; Battaglia, G.; Nicoletti, F.; Cruccu, G. N-acetyl-cysteine, a drug that enhances the endogenous activation of group-II metabotropic glutamate receptors, inhibits nociceptive transmission in humans. Mol. Pain 2015, 11, s12990-015. [Google Scholar] [CrossRef] [PubMed]
- Heidari, N.; Sajedi, F.; Mohammadi, Y.; Mirjalili, M.; Mehrpooya, M. Ameliorative Effects Of N-Acetylcysteine as Adjunct Therapy on Symptoms of Painful Diabetic Neuropathy. J. Pain Res. 2019, 12, 3147–3159. [Google Scholar] [CrossRef]
- Mbiantcha, M.; Khalid, R.; Atsamo, D.A.; Njoku, I.S.; Mehreen, A.; Ateufack, G.; Hamza, D.; Nana, W.Y.; Naeem, R.U.; Izhar, A.; et al. Anti-hypernociceptive effects of methanol extract of Boswellia dalzielii on STZ-induced diabetic neuropathic pain. Adv. Tradit. Med. 2020, 20, 405–417. [Google Scholar] [CrossRef]
- Kulkarni, R.R.; Patki, P.S.; Jog, V.P.; Gandage, S.G.; Patwardhan, B. Treatment of osteoarthritis with a herbomineral formulation: A double-blind, placebo-controlled, cross-over study. J. Ethnopharmacol. 1991, 33, 91–95. [Google Scholar] [CrossRef]
- Bates, D.; Schultheis, B.C.; Hanes, M.C.; Jolly, S.M.; Chakravarthy, K.V.; Deer, T.R.; Levy, R.M.; Hunter, C.W. A comprehensive algorithm for management of neuropathic pain. Pain Med. 2019, 20 (Suppl. S1), S2–S12. [Google Scholar] [CrossRef]
- Chou, R.; Loeser, J.D.; Owens, D.K.; Rosenquist, R.W.; Atlas, S.J.; Baisden, J.; Carragee, E.J.; Grabois, M.; Murphy, D.R.; Resnick, D.K.; et al. Interventional therapies, surgery, and interdisciplinary rehabilitation for low back pain: An evidence-based clinical practice guideline from the American Pain Society. Spine 2009, 34, 1066–1077. [Google Scholar] [CrossRef]
- Safikhani, S.; Gries, K.S.; Trudeau, J.J.; Reasner, D.; Rüdell, K.; Coons, S.J.; Bush, E.N.; Hanlon, J.; Abraham, L.; Vernon, M. Response scale selection in adult pain measures: Results from a literature review. J. Patient Rep. Outcomes 2018, 2, 40. [Google Scholar] [CrossRef]
- Padua, L.; Briani, C.; Jann, S.; Nobile-Orazio, E.; Pazzaglia, C.; Morini, A.; Mondelli, M.; Ciaramitaro, P.; Cavaletti, G.; Cocito, D.; et al. Validation of the Italian version of the Neuropathic Pain Symptom Inventory in peripheral nervous system diseases. Neurol. Sci. 2009, 30, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Kodraliu, G.; Mosconi, P.; Groth, N.; Carmosino, G.; Perilli, A.; Gianicolo, E.A.; Rossi, C.; Apolone, G. Subjective health status assessment: Evaluation of the Italian version of the SF-12 Health Survey. Results from the MiOS Project. J. Epidemiol. Biostat. 2001, 6, 305–316. [Google Scholar] [CrossRef] [PubMed]
- Ilari, S.; Proietti, S.; Russo, P.; Malafoglia, V.; Gliozzi, M.; Maiuolo, J.; Oppedisano, F.; Palma, E.; Tomino, C.; Fini, M.; et al. A Systematic Review and Meta-Analysis on the Role of Nutraceuticals in the Management of Neuropathic Pain in In Vivo Studies. Antioxidants 2022, 11, 2361. [Google Scholar] [CrossRef] [PubMed]
- Song, X.J. Analgesic and Neuroprotective Effects of B Vitamins. In Nutritional Modulators of Pain in the Aging Population, 1st ed.; Watson, R.R., Zibadi, S., Eds.; Academic Press: New York, NY, USA, 2017; pp. 151–170. ISBN 9780128053362. [Google Scholar]
- Bernatoniene, J.; Sciupokas, A.; Kopustinskiene, D.M.; Petrikonis, K. Novel Drug Targets and Emerging Pharmacotherapies in Neuropathic Pain. Pharmaceutics 2023, 15, 1799. [Google Scholar] [CrossRef]
- Caillaud, M.; Aung Myo, Y.P.; McKiver, B.D.; Osinska Warncke, U.; Thompson, D.; Mann, J.; Del Fabbro, E.; Desmoulière, A.; Billet, F.; Damaj, M.I. Key Developments in the Potential of Curcumin for the Treatment of Peripheral Neuropathies. Antioxidants 2020, 9, 950. [Google Scholar] [CrossRef]
- Cao, H.; Zheng, J.W.; Li, J.J.; Meng, B.; Li, J.; Ge, R.S. Effects of curcumin on pain threshold and on the expression of nuclear factor κ B and CX3C receptor 1 after sciatic nerve chronic constrictive injury in rats. Chin. J. Integr. Med. 2014, 20, 850–856. [Google Scholar] [CrossRef]
- Mbiantcha, M.; Ngouonpe Wembe, A.; Dawe, A.; Yousseu Nana, W.; Ateufack, G. Antinociceptive Activities of the Methanolic Extract of the Stem Bark of Boswellia dalzielii Hutch. (Burseraceae) in Rats Are NO/cGMP/ATP-Sensitive-K+ Channel Activation Dependent. Evid. Based Complement Altern. Med. 2017, 2017, 6374907. [Google Scholar] [CrossRef]
- Wang, Y.; Xiong, Z.L.; Ma, X.L.; Zhou, C.; Huo, M.H.; Jiang, X.W.; Yu, W.H. Acetyl-11-keto-beta-boswellic acid promotes sciatic nerve repair after injury: Molecular mechanism. Neural Regen Res. 2022, 17, 2778–2784. [Google Scholar] [CrossRef]
- Hakim, M.; Kurniani, N.; Pinzon, R.T.; Tugasworo, D.; Basuki, M.; Haddani, H.; Pambudi, P.; Fithrie, A.; Wuysang, A.D. Management of peripheral neuropathy symptoms with a fixed dose combination of high-dose vitamin B1, B6 and B12: A 12-week prospective non-interventional study in Indonesia. Asian J. Med. Sci. 2018, 9, 32–40. [Google Scholar] [CrossRef]
- Rizvi, A.M.N.A.; Ahmad, A.M.N.A.; Rizvi, Z.A.I.N.A.B. Efficacy of combination of vitamin B1, B6 and B12 in management of diabetic peripheral neuropathy. Pak. J. Med. Health Sci. 2013, 7, 801–804. [Google Scholar]
- Asadi, S.; Gholami, M.S.; Siassi, F.; Qorbani, M.; Khamoshian, K.; Sotoudeh, G. Nano curcumin supplementation reduced the severity of diabetic sensorimotor polyneuropathy in patients with type 2 diabetes mellitus: A randomized double-blind placebo- controlled clinical trial. Complement Ther. Med. 2019, 43, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Fotio, Y.; Aboufares El Alaoui, A.; Borruto, A.M.; Acciarini, S.; Giordano, A.; Ciccocioppo, R. Efficacy of a Combination of N-Palmitoylethanolamide, Beta-Caryophyllene, Carnosic Acid, and Myrrh Extract on Chronic Neuropathic Pain: A Preclinical Study. Front. Pharmacol. 2019, 10, 711. [Google Scholar] [CrossRef] [PubMed]
- Rowin, J. Integrative neuromuscular medicine: Neuropathy and neuropathic pain: Consider the alternatives. Muscle Nerve 2019, 60, 124–136. [Google Scholar] [CrossRef]
- Abdelrahman, K.M.; Hackshaw, K.V. Nutritional Supplements for the Treatment of Neuropathic Pain. Biomedicines 2021, 9, 674. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Singh, R.; Singh, K.; Lehl, S.S. Reversible dementia and gait disturbance as a result of polypharmacy. BMJ Case Rep. 2013, 2013, bcr2013008932. [Google Scholar] [CrossRef] [PubMed]
- Pereira, F.; Wernli, B.; von Gunten, A.; Carral, M.D.R.; Martins, M.M.; Verloo, H. Functional Status among Polymedicated Geriatric Inpatients at Discharge: A Population-Based Hospital Register Analysis. Geriatrics 2021, 6, 86. [Google Scholar] [CrossRef] [PubMed]
- Vranken, J.H.; Hollmann, M.W.; van der Vegt, M.H.; Kruis, M.R.; Heesen, M.; Vos, K.; Pijl, A.J.; Dijkgraaf, M.G.W. Duloxetine in patients with central neuropathic pain caused by spinal cord injury or stroke: A randomized, double-blind, placebo-controlled trial. Pain 2011, 152, 267–273. [Google Scholar] [CrossRef]
- Adams, M.; Weatherall, M.; Bell, E. A cohort study of the association between psychosocial factors and pain in patients with Spinal Cord Injury and Stroke. NeuroRehabilitation 2019, 45, 419–427. [Google Scholar] [CrossRef]
- Selingardi, P.M.L.; de Lima Rodrigues, A.L.; da Silva, V.A.; Fernandes, D.T.R.M.; Rosí, J., Jr.; Marcolin, M.A.; Yeng, L.T.; Brunoni, A.R.; Teixeira, M.J.; Galhardoni, R.; et al. Long-term deep-TMS does not negatively affect cognitive functions in stroke and spinal cord injury patients with central neuropathic pain. BMC Neurol. 2019, 19, 319. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Age, years | 63.67 ± 15.47 |
| Sex, male | 14 (58.3) |
| Education | |
| Primary to 3 years professional school | 16 (66.6) |
| High school | 6 (25) |
| University degree | 1 (4.2) |
| Postgraduate | 1 (4.2) |
| Occupation | |
| Employed | 11 (45.8) |
| Unemployed | 1 (4.2) |
| Housewife | 2 (8.3) |
| Retired | 10 (41.7) |
| SCI | 22 (91.7) |
| Stroke | 2 (8.3) |
| Onset of pain | |
| Coincident with the spinal injury or stroke | 24 (100) |
| Occurred months after the spinal injury or stroke | 0 (0) |
| Pain location * | |
| Pain at the injury site | 12 (52.2) |
| Pain at the injury site with irradiation to a single hemibody | 4 (17.4) |
| Pain at the injury site with bilateral sublesional irradiation | 7 (30.4) |
| Pain frequency | |
| Intermittent | 8 (33.3) |
| Continuous | 16 (66.7) |
| SCI-related surgeries * | |
| None | 6 (26.1) |
| One | 9 (39.1) |
| More than one | 8 (34.8) |
| Pharmacotherapy | |
| Pregabalin 25 mg one daily | 1 (4.2) |
| Pregabalin 50 mg 3 times daily | 1 (4.2) |
| Pregabalin 75 mg once daily | 4 (16.7) |
| Pregabalin 75 mg twice daily | 6 (25) |
| Pregabalin 75 mg 3 times daily | 2 (8.3) |
| Pregabalin 100 mg 3 times daily | 3 (12.5) |
| Pregabalin 100 mg 4 times daily | 1 (4.2) |
| Pregabalin 150 mg once daily | 1 (4.2) |
| Pregabalin 150 mg twice daily | 3 (12.5) |
| Gabapentin 100 mg twice daily | 2 (8.3) |
| Perceived efficacy of pharmacotherapy | 5.13 (2.14) |
| Variables | Mean (SD) |
|---|---|
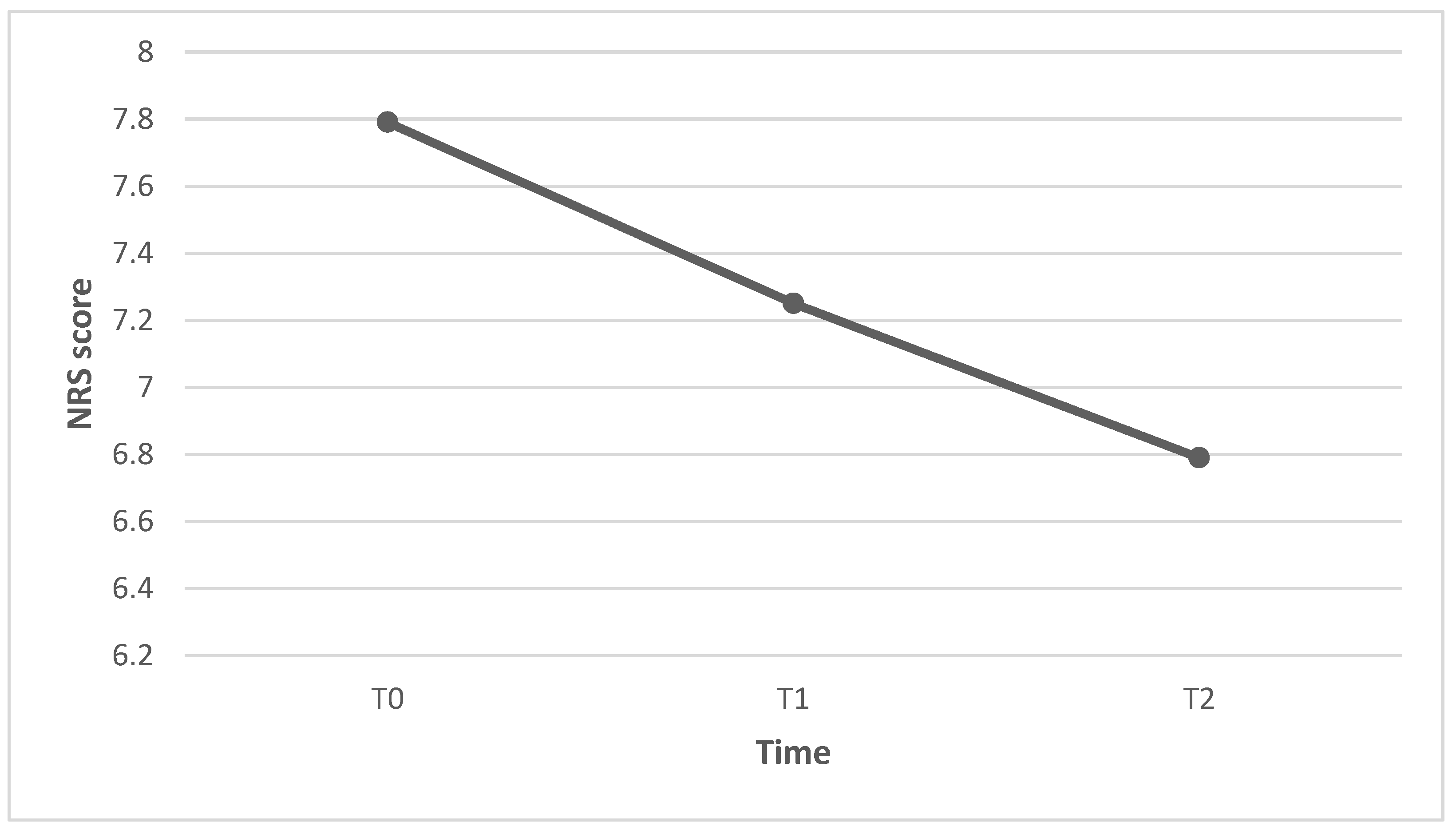
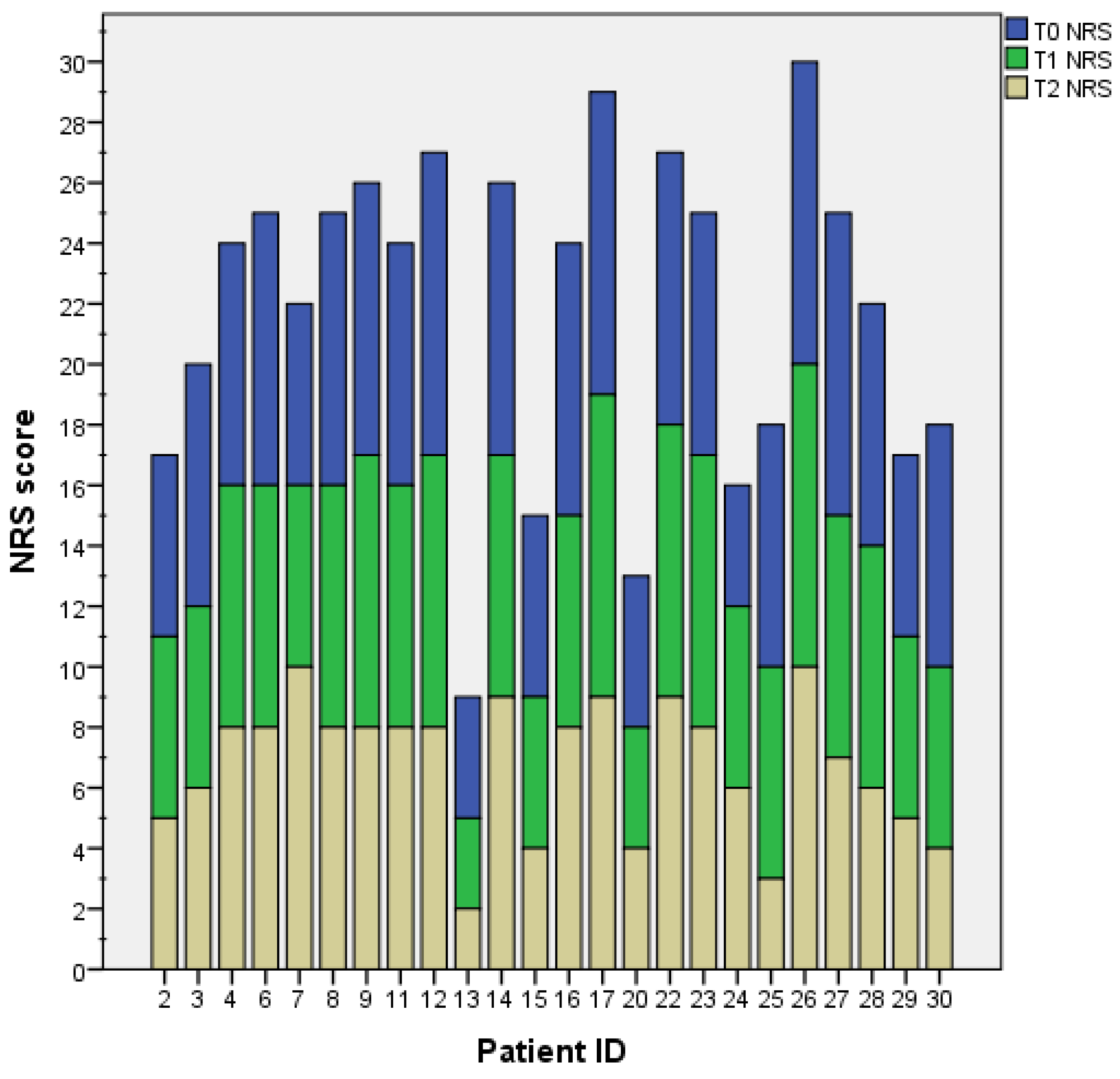
| T0 NRS | 7.79 (1.84) |
| T1 NRS | 7.25 (1.80) |
| T2 NRS | 6.79 (2.25) |
| T0 NPSI | |
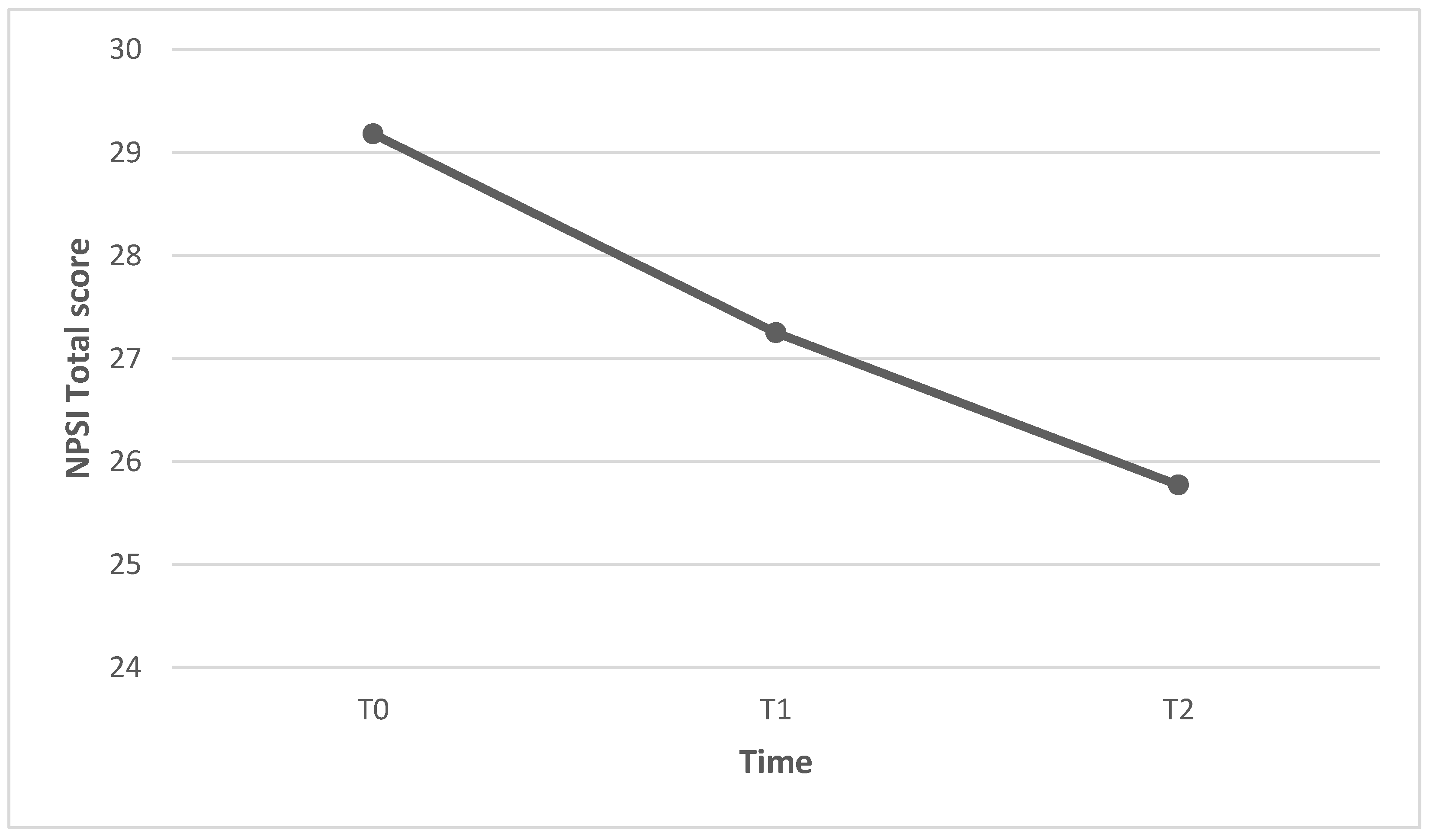
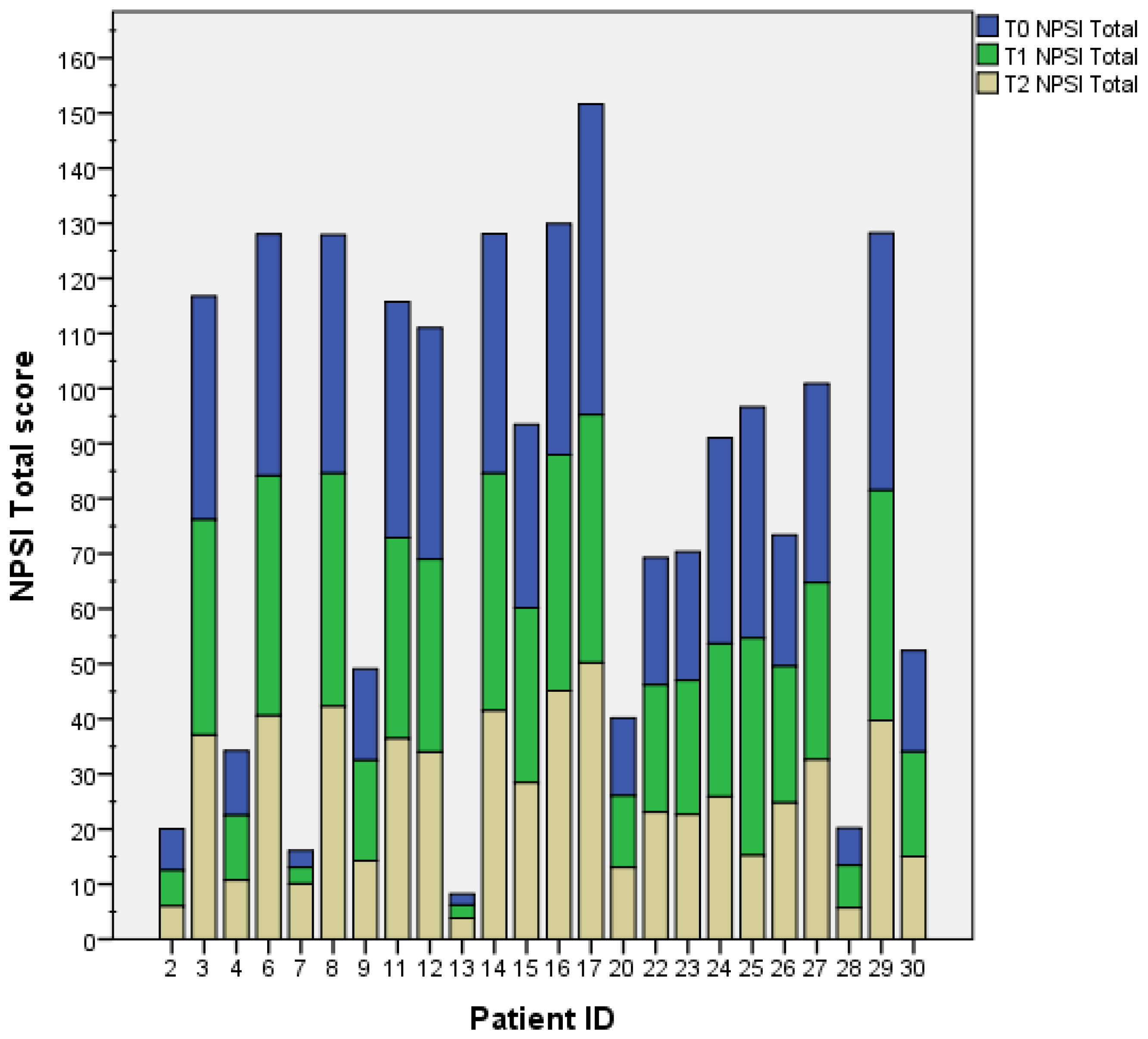
| Total intensity score | 29.18 (16.03) |
| Burning (superficial) spontaneous pain subscale | 3.46 (3.61) |
| Pressing (deep) spontaneous pain subscale | 6.13 (4.97) |
| Paroxysmal pain subscale | 7.15 (5.94) |
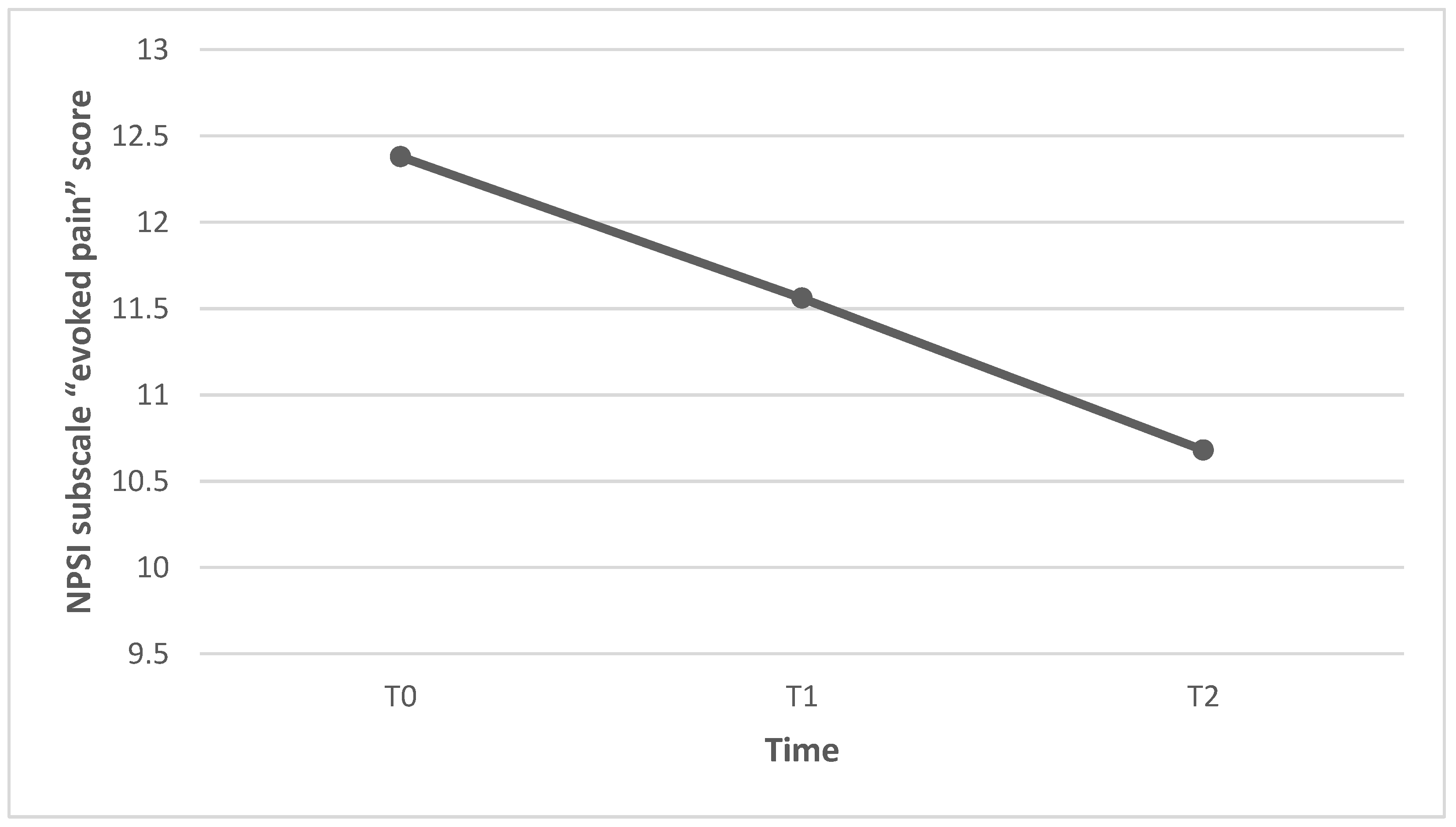
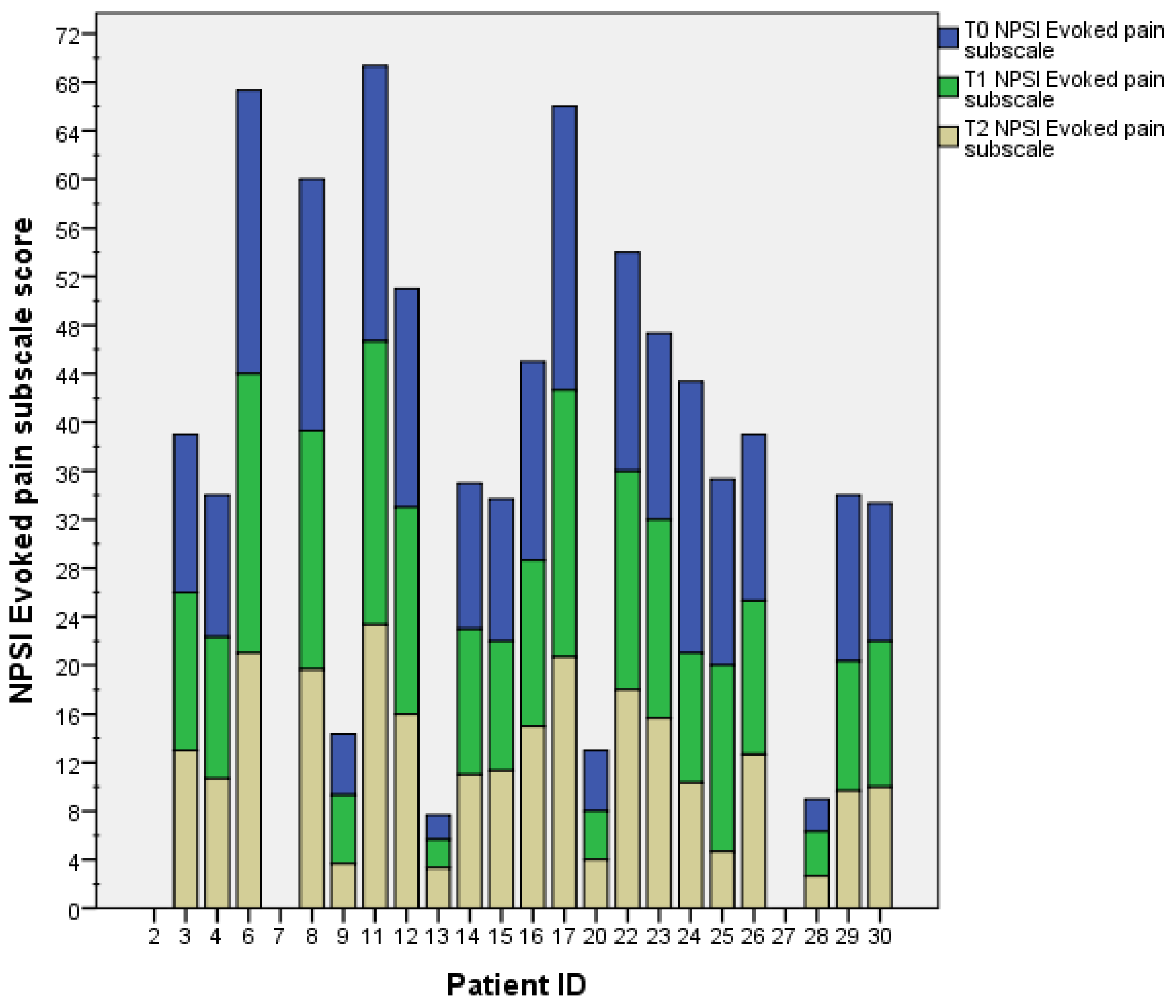
| Evoked pain subscale | 12.38 (7.76) |
| Paraesthesia/dysesthesia subscale | 7.33 (4.62) |
| T1 NPSI | |
| Total intensity score | 27.25 (14.18) |
| Burning (superficial) spontaneous pain subscale | 3.38 (3.50) |
| Pressing (deep) spontaneous pain subscale | 5.81 (4.59) |
| Paroxysmal pain subscale | 6.44 (5.24) |
| Evoked pain subscale | 11.56 (7.23) |
| Paraesthesia/dysesthesia subscale | (7.40 (4.32) |
| T2 NPSI | |
| Total intensity score | 25.77 (14.08) |
| Burning (superficial) spontaneous pain subscale | 3.17 (3.40) |
| Pressing (deep) spontaneous pain subscale | 5.29 (4.25) |
| Paroxysmal pain subscale | 6.56 (5.07) |
| Evoked pain subscale | 10.68 (7.15) |
| Paraesthesia/dysesthesia subscale | 6.63 (4.33) |
| T0 SF-12 | |
| Physical component summary | 33.84 (8.17) |
| Mental component summary | 47.73 (15.22) |
| T1 SF-12 | |
| Physical component summary | 34.20 (8.21) |
| Mental component summary | 48.36 (12.60) |
| T2 SF-12 | |
| Physical component summary | 33.89 (7.72) |
| Mental component summary | 49.45 (13.31) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raffaeli, W.; Felzani, G.; Tenti, M.; Greco, L.; D’Eramo, M.P.; Proietti, S.; Morone, G. A Nutritional Supplement as Adjuvant of Gabapentinoids for Adults with Neuropathic Pain following Spinal Cord Injury and Stroke: Preliminary Results. Healthcare 2023, 11, 2563. https://doi.org/10.3390/healthcare11182563
Raffaeli W, Felzani G, Tenti M, Greco L, D’Eramo MP, Proietti S, Morone G. A Nutritional Supplement as Adjuvant of Gabapentinoids for Adults with Neuropathic Pain following Spinal Cord Injury and Stroke: Preliminary Results. Healthcare. 2023; 11(18):2563. https://doi.org/10.3390/healthcare11182563
Chicago/Turabian StyleRaffaeli, William, Giorgio Felzani, Michael Tenti, Luca Greco, Maria Pia D’Eramo, Stefania Proietti, and Giovanni Morone. 2023. "A Nutritional Supplement as Adjuvant of Gabapentinoids for Adults with Neuropathic Pain following Spinal Cord Injury and Stroke: Preliminary Results" Healthcare 11, no. 18: 2563. https://doi.org/10.3390/healthcare11182563