
Practices and Perceptions of Community Pharmacists in the Management of Atopic Dermatitis: A Systematic Review and Thematic Synthesis

Abstract
:1. Introduction
2. Method
2.1. Design
2.2. Search Strategy
2.3. Selection Process and Inclusion Criteria
2.4. Assessment of Methodological Quality
2.5. Data Extraction and Synthesis
2.6. Assessment of Confidence
2.7. Outcomes Assessed
3. Results
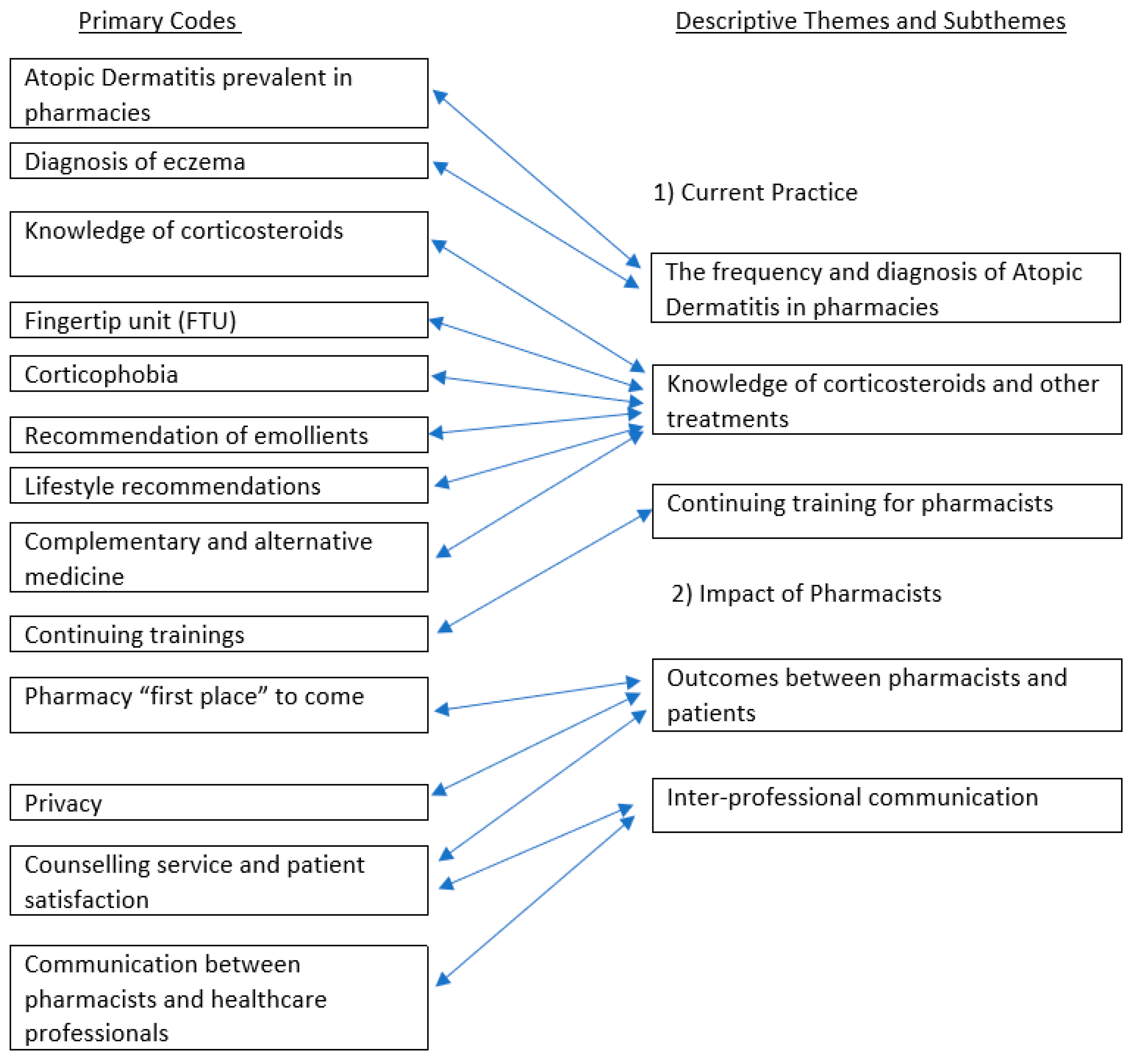
3.1. Descriptive Themes
3.1.1. Current Practice
- Knowledge of Corticosteroids and Other Treatments
- ii.
- The Frequency and Diagnosis of Atopic Dermatitis in Pharmacies
- iii.
- Continuing Training for Pharmacists
3.1.2. Impact of Pharmacists
- Outcomes between Pharmacists and Patients
- ii.
- Inter-professional Communication
3.2. Analytical Themes
3.2.1. Misleading Position
“Pharmacists should be the first port of call for patients with a skin problem”.[37] Quote 1
“In terms of formulations, over 60% did not know how many topical corticosteroid potency categories exist”.[36] Quote 2
“Of course, you have those fingertip units. Well, I must confess that we don’t really work with it to indicate how much you have to apply. We just say: apply thin. It is still a hormone cream”.[42] Quote 3 (Pharmacist)
“When directing the amount of TCS to be applied, 54% reported informing the patient that TCS should be used sparingly…”[41] Quote 4
“A more detailed history would have been helpful and may have supported making the diagnosis”.[38] Quote 5 (Dermatology Specialists)
“Maybe they weren’t told about the emollient at the GP. And then you give the advice to use a moisturizer…”[42] Quote 6 (Pharmacist)
3.2.2. Perceptions of Education and Training
“Of those (pharmacists) surveyed, 92% stated they would advise TCS be used until the eczema is clear, compared to 27% prior to education (p < 0.0001)”.[41] Quote 7
“Knowledge about eczema and treatment among pharmacy staff increased from baseline to follow-up 7.3 ± 1.7 to 8.4 ± 1.5 (p = 0.052)”.[43] Quote 8
“Also, parents were, in general, positive about the counseling session in the pharmacy […] 45.8% mentioned they started using the treatment differently afterwards (e.g., more frequent use of emollients and increased application of TCS, based on FTU)”.[43] Quote 9
4. Discussion
4.1. Summary of Findings
4.2. Implications for Practice and Policy
4.3. Strengths and Limitations of the Study
4.4. Further Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Author and Year | Country | Study Design | Methods of Data Collection | Participants | Number of Participants | Aim | Key Findings | Further Recommendations |
|---|---|---|---|---|---|---|---|---|
| Abed et al. [56], 2021 | Iraq | Cross-sectional | Questionnaire | Customers who asked for topical corticosteroids (TCs) without prescription | 212 customers | To assess the patients’ knowledge of TC use and education provided by pharmacists |
|
|
| Carr et al. [34], 2009 | England | Pre-post educational intervention | Questionnaire | Patients and their parents | 50 children and their parents | To identify the effects of community pharmacists’ interventions on the use of emollients in children with eczema |
|
|
| Cowdell et al. [35], 2019 | England | Qualitative study | Field notes and interviews | Community pharmacists and other health professionals | 2 community pharmacists | To create positive atopic dermatitis (AD)-related mindsets among healthcare practitioners to improve management of the condition |
|
|
| Giua et al. [52], 2021 | Italy | Cross-sectional | Questionnaire | Community pharmacists | 154 community pharmacists | (1) To obtain information about pharmacists’ counseling activity regarding dermatological conditions; (2) to gain information about corticophobia among pharmacists; (3) to research the educational needs of pharmacists |
|
|
| Hammarstrom et al. [44], 1995 | Sweden | Pre-post educational intervention | Questionnaire and drug sale statistics | Community pharmacies | 900 community pharmacies | To improve treatment management in patients with skin disorders |
|
|
| Issa et al. [54], 2016 | Jordan | Cross-sectional | Questionnaire | Community pharmacists | 100 community pharmacists | To evaluate the disagreements in TCs prescription patterns and practice advices among different health workers and determine underlying causes |
|
|
| Jairoun et al. [53], 2020 | United Arab Emirates | Cross-sectional | Questionnaire | Community pharmacists | 772 community pharmacists | To find out pharmacist knowledge, attitude, and practice in use of corticosteroids |
|
|
| Kaneko et al. [46], 2014 | Japan | Cross-sectional | Questionnaire | Community and hospital pharmacists | 372 community, 109 hospital pharmacists | To investigate pharmacist practices regarding applying topical medications in the management of AD |
| To effectively counsel eczema patients, pharmacists should be aware of treatment guidelines for AD and are urged to follow these guidelines. |
| Koster et al. [42], 2019 | Netherlands | Qualitative study | Interviews | Parents of children with AD, community pharmacists, and pharmacy technicians | 29 parents, 6 community pharmacists, and 12 pharmacy technicians | To explore the perspectives of both pharmacy staff and parents regarding the treatment of children with AD in the Netherlands |
|
|
| Koster et al. [43], 2021 | Netherlands | Pre- and post-education interventions | Questionnaire | Parents of children with AD, community pharmacists, and pharmacy technicians | 48 parents, 6 community pharmacists, and 13 pharmacy technicians | To study the effects of pharmacy intervention on corticophobia among both pharmacy staff and parents of young AD patients |
|
|
| Lambrechts et al. [51], 2019 | Belgium | Cross-sectional | Questionnaire | Pharmacists, paediatricians, GPs, dermatologists | 118 pharmacists, 100 paediatricians, 81 GPs, and 92 dermatologists. | To determine the frequency of corticophobia among pharmacists and other health professionals |
|
|
| Lau et al. [36], 2017 | England | Mixed-methods | Interviews and questionnaire | Community pharmacists | 5 community pharmacists were interviewed and 105 community pharmacists filled out the questionnaire. | To investigate the knowledge of community pharmacists regarding corticosteroid use in the treatment of AD, as well as their information supply, attitudes, and patient counseling behavior |
|
|
| Lindblad et al. [45], 2006 | Sweden | Qualitative | Focus groups | Patients and health providers (community pharmacists, dermatology nurses, and dermatologists) | 12 patients and 12 health providers (the number of pharmacists was not applicable) | To determine the views of health providers and patients regarding the role of providers in the management of dermatological conditions |
|
|
| Manahan et al. [40], 2011 | Australia | Cross-sectional | Questionnaire | Community pharmacists and pharmacy interns | 17 community pharmacists and 3 pharmacy interns | To identify community pharmacists’ roles in the management of skin conditions and assess their opinions of teledermatology services |
|
|
| Oishi et al. [47], 2019 | Japan | Cross-sectional | Questionnaire | Community pharmacists | 300 community pharmacists | To investigate the effectiveness of community pharmacists’ instructions regarding the use of FTU and the effects of following practice guidelines on treatment |
|
|
| Raffin et al. [49], 2016 | France | Cross-sectional | Questionnaire | Community pharmacists, technicians and students | 176 community pharmacists, 10 pharmacy technicians, and 5 pharmacy students | To evaluate corticophobia among pharmacists in relation to AD in children |
|
|
| Salzmann et al. [50], 2020 | Germany | Cross-sectional | Questionnaire | Community pharmacists and dermatologists | 351 community pharmacists and 53 dermatologists | To acquire data about daily prescription habits related to compounded preparations (CPs) in dermatology and compare them using standardized questionnaires, as well as to overcome the lack of interdisciplinary collaboration |
| Future studies should concentrate on CPs to increase the quality of prescriptions. |
| Smith et al. [41], 2016 | Australia | Pre-post educational intervention | Survey | Pharmacists (including community pharmacists) | 292 pharmacists | To evaluate pharmacists’ beliefs and knowledge regarding the use of topical corticosteroids in paediatric eczema |
| Pharmacist education throughout initial education and pharmacy journals should be supported by dermatology specialists to enhance pharmacists’ knowledge of the use of TCs in AD. |
| Teixeira et al. [48], 2021 | Portugal | Cross-sectional | Questionnaire | Community pharmacists and patients | 149 community pharmacists, 44 patients | To find the association between pharmacists’ knowledge and their conveyance of information to patients with dermatoses and create a proper guide for patients about dosage instructions |
| Proper guidelines must be prepared to enhance communication of dosage instructions to patients. Moreover, continued training courses should be implemented to help pharmacists to solve problems. |
| Thandar et al. [55], 2019 | South Africa | Cross-sectional | Questionnaire | Community pharmacists | 82 community pharmacists | To identify community pharmacists’ attitudes and practices regarding the use of complementary and alternative therapies in patients with AD |
| It was revealed that pharmacists had insufficienct knowledge of CAMs, meaning that they needed further ongoing education. |
| Tucker et al. [37], 2012 | England and Wales | Cross-sectional | Questionnaire | Community Pharmacists | 870 community pharmacists | To find out which types of skin diseases pharmacists come across in pharmacies and which training sessions they attend to gain more knowledge of dermatological diseases |
| Use of pharmacists’ advice in the management of skin conditions should be studied in future studies. |
| Tucker et al. [39], 2013 | England and Wales | Cross-sectional | Questionnaire | Community Pharmacists | 870 community pharmacists | To identify pharmacists’ roles in medicine use review (MUR) and evaluate pharmacists’ understanding of long-term skin diseases |
| Further studies should be conducted to identify whether these reviews contribute to better disease-related outcomes. |
| Tucker et al. [38], 2017 | England | Mixed methods | Questionnaire- and assessment-based feedback | Patients, dermatology specialists, and community pharmacists | 40 patients, 3 dermatology specialists, and 9 community pharmacists | To assess the clinical convenience of pharmacists’ diagnoses and management of dermatitis and acne, as well as to obtain patients’ self-reported perceptions regarding the effectiveness of pharmacy intervention |
| Patient assessment-related education for pharmacists should be considered, with particuar focus on dermatology. |
References
- Weidinger, S.; Beck, L.A.; Bieber, T.; Kabashima, K.; Irvine, A.D. Atopic dermatitis. Nat. Rev. Dis. Primers 2018, 4, 1–20. [Google Scholar] [CrossRef]
- Bekić, S.; Martinek, V.; Talapko, J.; Majnarić, L.; Vasilj Mihaljević, M.; Škrlec, I. Atopic Dermatitis and Comorbidity. Healthcare 2020, 8, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kay, J.; Gawkrodger, D.J.; Mortimer, M.J.; Jaron, A.G. The prevalence of childhood atopic eczema in a general population. J. Am. Acad. Dermatol. 1994, 30, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Ellis, C.N.; Mancini, A.J.; Paller, A.S.; Simpson, E.L.; Eichenfield, L.F. Understanding and managing atopic dermatitis in adult patients. Semin. Cutan. Med. Surg. 2012, 31, S18–S22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girolomoni, G.; de Bruin-Weller, M.; Aoki, V.; Kabashima, K.; Deleuran, M.; Puig, L.; Bansal, A.; Rossi, A.B. Nomenclature and clinical phenotypes of atopic dermatitis. Ther. Adv. Chronic Dis. 2021, 12, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Eichenfield, L.F.; Tom, W.L.; Chamlin, S.L.; Feldman, S.R.; Hanifin, J.M.; Simpson, E.L.; Berger, T.G.; Bergman, J.N.; Cohen, D.E.; Cooper, K.D. Guidelines of care for the management of atopic dermatitis: Section 1. Diagnosis and assessment of atopic dermatitis. J. Am. Acad. Dermatol. 2014, 70, 338–351. [Google Scholar] [CrossRef] [Green Version]
- Schallreuter, K.; Levenig, C.; Berger, J.; Umbert, J.; Winkelmann, R.; Wegener, L.; Correia, O.; Chosidow, O.; Saiag, P.; Bastuji-Garin, S. Severity scoring of atopic dermatitis: The SCORAD index. Dermatology 1993, 186, 23–31. [Google Scholar]
- Ng, M.S.; Tan, S.; Chan, N.H.; Foong, A.Y.; Koh, M.J. Effect of atopic dermatitis on quality of life and its psychosocial impact in Asian adolescents. Australas. J. Dermatol. 2018, 59, e114–e117. [Google Scholar] [CrossRef]
- Maliyar, K.; Sibbald, C.; Pope, E.; Sibbald, R.G. Diagnosis and management of atopic dermatitis: A review. Adv. Ski. Wound Care 2018, 31, 538–550. [Google Scholar] [CrossRef]
- Chovatiya, R.; Paller, A.S. JAK inhibitors in the treatment of atopic dermatitis. J. Allergy Clin. Immunol. 2021, 148, 927–940. [Google Scholar] [CrossRef]
- Holm, J.G.; Clausen, M.-L.; Agner, T.; Thomsen, S.F. Use of complementary and alternative therapies in outpatients with atopic dermatitis from a dermatological university department. Dermatology 2019, 235, 189–195. [Google Scholar] [CrossRef]
- Dattola, A.; Bennardo, L.; Silvestri, M.; Nisticò, S.P. What’s new in the treatment of atopic dermatitis? Dermatol. Ther. 2019, 32, e12787. [Google Scholar] [CrossRef]
- McAleer, M.; Flohr, C.; Irvine, A. Management of difficult and severe eczema in childhood. BMJ 2012, 345, e4770. [Google Scholar] [CrossRef]
- Patel, N.U.; D’Ambra, V.; Feldman, S.R. Increasing adherence with topical agents for atopic dermatitis. Am. J. Clin. Dermatol. 2017, 18, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Ference, J.D.; Last, A.R. Choosing topical corticosteroids. Am. Fam. Physician 2009, 79, 135–140. [Google Scholar]
- Fischer, G. Compliance problems in paediatric atopic eczema. Australas. J. Dermatol. 1996, 37, S10–S13. [Google Scholar] [CrossRef] [PubMed]
- Charman, C.; Williams, H. The use of corticosteroids and corticosteroid phobia in atopic dermatitis. Clin. Dermatol. 2003, 21, 193–200. [Google Scholar] [CrossRef]
- Niculet, E.; Bobeica, C.; Tatu, A.L. Glucocorticoid-induced skin atrophy: The old and the new. Clin. Cosmet. Investig. Dermatol. 2020, 13, 1041–1050. [Google Scholar] [CrossRef]
- Kijima, T.; Shimada, N.; Ishida, N.; Yamagata, S.; Makiishi, T. Adrenal Insufficiency Following Prolonged Administration of Ultra-High Topical Steroid: A Case of Refractory Dermatitis. Cureus 2023, 15, e37967. [Google Scholar] [CrossRef] [PubMed]
- Roque, F.; Soares, S.; Breitenfeld, L.; López-Durán, A.; Figueiras, A.; Herdeiro, M.T. Attitudes of community pharmacists to antibiotic dispensing and microbial resistance: A qualitative study in Portugal. Int. J. Clin. Pharm. 2013, 35, 417–424. [Google Scholar] [CrossRef]
- Murray, E.; Bieniek, K.; Del Aguila, M.; Egodage, S.; Litzinger, S.; Mazouz, A.; Mills, H.; Liska, J. Impact of pharmacy intervention on influenza vaccination acceptance: A systematic literature review and meta-analysis. Int. J. Clin. Pharm. 2021, 43, 1163–1172. [Google Scholar] [CrossRef]
- Wong, I.T.; Tsuyuki, R.T.; Cresswell-Melville, A.; Doiron, P.; Drucker, A.M. Guidelines for the management of atopic dermatitis (eczema) for pharmacists. Can. Pharm. J./Rev. Des. Pharm. Du Can. 2017, 150, 285–297. [Google Scholar] [CrossRef]
- Atopic Eczema in Under 12s: Diagnosis and Management. National Institute for Health Care Excellence (NICE) Clinical Guideline [CG57]. Available online: https://www.nice.org.uk/guidance/cg57 (accessed on 15 July 2023).
- Ravis, S.M.; Eaglstein, W.H. Topical hydrocortisone from prescription to over-the-counter sale: A past controversy: A cautionary tale. Arch. Dermatol. 2007, 143, 413–415. [Google Scholar] [CrossRef]
- Pluye, P.; Hong, Q.N. Combining the power of stories and the power of numbers: Mixed methods research and mixed studies reviews. Annu. Rev. Public Health 2014, 35, 29–45. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B. Mixed Methods Appraisal Tool (MMAT); Version 2018; Registration of Copyright Canadian Intellectual Property Office, Industry Canada: Gatineau, QC, Canada, 2018. [Google Scholar]
- Pace, R.; Pluye, P.; Bartlett, G.; Macaulay, A.C.; Salsberg, J.; Jagosh, J.; Seller, R. Testing the reliability and efficiency of the pilot Mixed Methods Appraisal Tool (MMAT) for systematic mixed studies review. Int. J. Nurs. Stud. 2012, 49, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8, 45. [Google Scholar] [CrossRef] [Green Version]
- Sandelowski, M. Combining qualitative and quantitative sampling, data collection, and analysis techniques in mixed-method studies. Res. Nurs. Health 2000, 23, 246–255. [Google Scholar] [CrossRef]
- Hong, Q.N.; Pluye, P.; Bujold, M.; Wassef, M. Convergent and sequential synthesis designs: Implications for conducting and reporting systematic reviews of qualitative and quantitative evidence. Syst. Rev. 2017, 6, 61. [Google Scholar] [CrossRef] [Green Version]
- Lewin, S.; Glenton, C.; Munthe-Kaas, H.; Carlsen, B.; Colvin, C.J.; Gülmezoglu, M.; Noyes, J.; Booth, A.; Garside, R.; Rashidian, A. Using qualitative evidence in decision making for health and social interventions: An approach to assess confidence in findings from qualitative evidence syntheses (GRADE-CERQual). PLoS Med. 2015, 12, e1001895. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Carr, A.; Patel, R.; Jones, M.; Suleman, A. A pilot study of a community pharmacist intervention to promote the effective use of emollients in childhood eczema. Pharm. J. 2007, 278, 319–322. [Google Scholar]
- Cowdell, F. Knowledge mobilisation: An ethnographic study of the influence of practitioner mindlines on atopic eczema self-management in primary care in the UK. BMJ Open 2019, 9, e025220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, W.M.; Donyai, P. Knowledge, Attitude and Advice-Giving Behaviour of Community Pharmacists Regarding Topical Corticosteroids. Pharmacy 2017, 5, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, R. Community pharmacists’ perceptions of the skin conditions they encounter and how they view their role in dermatological care. Int. J. Pharm. Pract. 2012, 20, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Tucker, R.P.; MacLure, K.; Paudyal, V.; Layton, A.M.; Bewley, A.; Stewart, D. An exploratory study of community pharmacist diagnosis and management of dermatitis and acne. Selfcare 2017, 8, 1–10. [Google Scholar]
- Tucker, R. The medicines use review in patients with chronic skin diseases: Are pharmacists doing them and how confident are they? Int. J. Pharm. Pract. 2013, 21, 202–204. [Google Scholar] [CrossRef] [PubMed]
- Manahan, M.N.; Soyer, H.P.; Nissen, L.M. Teledermatology in pharmacies: A pilot study. J. Telemed. Telecare 2011, 17, 392–396. [Google Scholar] [CrossRef]
- Smith, S.D.; Lee, A.; Blaszczynski, A.; Fischer, G. Pharmacists’ knowledge about use of topical corticosteroids in atopic dermatitis: Pre and post continuing professional development education. Australas. J. Dermatol. 2016, 57, 199–204. [Google Scholar] [CrossRef]
- Koster, E.S.; Philbert, D.; Wagelaar, K.R.; Galle, S.; Bouvy, M.L. Optimizing pharmaceutical care for pediatric patients with dermatitis: Perspectives of parents and pharmacy staff. Int. J. Clin. Pharm. 2019, 41, 711–718. [Google Scholar] [CrossRef] [Green Version]
- Koster, E.S.; Philbert, D.; Zheng, X.; Moradi, N.; de Vries, T.W.; Bouvy, M.L. Reducing corticosteroid phobia in pharmacy staff and parents of children with atopic dermatitis. Int. J. Clin. Pharm. 2021, 43, 1237–1244. [Google Scholar] [CrossRef]
- Hammarström, B.; Wessling, A.; Nilsson, J.L. Pharmaceutical care for patients with skin diseases: A campaign year at Swedish pharmacies. J. Clin. Pharm. Ther. 1995, 20, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Lindblad, A.K.; Kjelgren, K.I.; Ring, L.; Maroti, M.; Serup, J. The role of dermatologists, nurses and pharmacists in chronic dermatological treatment: Patient and provider views and experiences. Acta Derm. Venereol. 2006, 86, 202–208. [Google Scholar] [CrossRef] [Green Version]
- Kaneko, S.; Kakamu, T.; Matsuo, H.; Naora, K.; Morita, E. Questionnaire-based study on the key to the guidance to the patients with atopic dermatitis by pharmacist. Jpn. J. Allergol. 2014, 63, 1250–1257. [Google Scholar]
- Oishi, N.; Iwata, H.; Kobayashi, N.; Fujimoto, K.; Yamaura, K. A survey on awareness of the "finger-tip unit" and medication guidance for the use of topical steroids among community pharmacists. Drug Discov. Ther. 2019, 13, 128–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teixeira, A.; Teixeira, M.; Herdeiro, M.T.; Vasconcelos, V.; Correia, R.; Bahia, M.F.; Almeida, I.F.; Vidal, D.G.; Sousa, H.F.P.E.; Dinis, M.A.P. Knowledge and practices of community pharmacists in topical dermatological treatments. Int. J. Environ. Res. Public Health 2021, 18, 2928. [Google Scholar] [CrossRef]
- Raffin, D.; Giraudeau, B.; Samimi, M.; Machet, L.; Pourrat, X.; Maruani, A. Corticosteroid phobia among pharmacists regarding atopic dermatitis in children: A national French survey. Acta Derm. Venereol. 2016, 96, 177–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salzmann, S.; Salzmann, M.; Staubach, P. Compounded preparations in dermatology-analysis of prescribing habits in everyday clinical practice in Germany. J. Dtsch. Dermatol. Ges. 2020, 18, 334–340. [Google Scholar] [CrossRef]
- Lambrechts, L.; Gilissen, L.; Morren, M.-A. Topical Corticosteroid Phobia Among Healthcare Professionals Using the TOPICOP Score. Acta Derm. Venereol. 2019, 99, 1004–1008. [Google Scholar] [CrossRef] [Green Version]
- Giua, C.; Floris, N.P.; Schlich, M.; Keber, E.; Gelmetti, C. Dermatitis in community pharmacies: A survey on italian pharmacists’ management and implications on corticophobia. Pharmacia 2021, 68, 671–677. [Google Scholar] [CrossRef]
- Jairoun, A.A.; Al-Hemyari, S.S.; El-Dahiyat, F.; Shahwan, M. GAP analysis of pharmacy curriculum regarding topical corticosteroid use and safety. J Public Health 2021, 29, 1291–1299. [Google Scholar] [CrossRef]
- Issa, A.Y.; Farhaa, R.A.; Elayeha, E.; Bustanji, Y. Impact of medical specialty on the prescription patterns of topical corticosteroid among healthcare professionals. Jordan J. Pharm. Sci. 2016, 9, 103–114. [Google Scholar] [CrossRef]
- Thandar, Y.; Botha, J.; Mosam, A. Community pharmacists’ knowledge, attitude and practices towards the use of complementary and alternative medicines in Durban, South Africa. Health SA Gesondheid 2019, 24, 6. [Google Scholar] [CrossRef] [PubMed]
- Abed, A.S.; Hassan, J.K. Abuse of topical glucocorticoids among patients visiting community pharmacy in Basrah-Iraq. Indian. J. Forensic Med. Toxicol. 2021, 15, 623–632. [Google Scholar]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Mays, N.; Pope, C.; Popay, J. Systematically reviewing qualitative and quantitative evidence to inform management and policy-making in the health field. J. Health Serv. Res. Policy 2005, 10 (Suppl. S1), 6–20. [Google Scholar] [CrossRef] [PubMed]
- Corticosteroïden: Niet dun smeren, maar per FTU. Koninklijke Nederlandse Maatschappij Pharmacie (KNMP). Available online: https://maken.wikiwijs.nl/userfiles/b/b0c1c845c5840e083a8a5fd7d1166c8ebeb71bdd.pdf (accessed on 16 November 2022).
- Smith, S.D.; Hong, E.; Fearns, S.; Blaszczynski, A.; Fischer, G. Corticosteroid phobia and other confounders in the treatment of childhood atopic dermatitis explored using parent focus groups. Australas. J. Dermatol. 2010, 51, 168–174. [Google Scholar] [CrossRef]
- Stalder, J.F.; Aubert, H.; Anthoine, E.; Futamura, M.; Marcoux, D.; Morren, M.A.; Trzeciak, M.; Szalai, Z.; Veres, K.; Deleuran, M. Topical corticosteroid phobia in atopic dermatitis: International feasibility study of the TOPICOP score. Allergy 2017, 72, 1713–1719. [Google Scholar] [CrossRef]
- Nathan, A.D.; Shankar, P.R.; Sreeramareddy, C.T. Community pharmacists’ counseling practices and patient experiences about topical corticosteroids–an online survey in the Klang Valley, Malaysia. BMC Prim. Care 2022, 23, 263. [Google Scholar] [CrossRef]
- McMillan, S.S.; Thangarajah, T.; Anderson, C.; Kelly, F. Pharmacy student decision making in over-the-counter medicine supply: A critical incident study. Res. Soc. Adm. Pharm. 2018, 14, 749–757. [Google Scholar] [CrossRef] [Green Version]
- Chahine, B.; Cherfane, M.; Sakr, F.; Safwan, J.; Dabbous, M.; Akel, M.; Rahal, M. Community pharmacists’ perceptions and role in the management of common dermatological problems in Lebanon: A cross-sectional study. Int. J. Pharm. Pract. 2021, 29, 573–579. [Google Scholar] [CrossRef]
- Garreau, A.C.; Stalder, J.F.; Méry, S.; Bunouf, P.; Jean-Decoster, C.; Nosbaum, A.; Eczema Foundation, t.F.G.o.T.E.i.D. Impact of an e-learning programme on pharmacists’ management of atopic dermatitis. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e656–e659. [Google Scholar] [CrossRef]
- Fivenson, D. The effect of atopic dermatitis on total burden of illness and quality of life on adults and children in a large managed care organization. J. Manag. Care Pharm. 2002, 8, 333–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wollenberg, A.; Barbarot, S.; Bieber, T.; Christen-Zaech, S.; Deleuran, M.; Fink-Wagner, A.; Gieler, U.; Girolomoni, G.; Lau, S.; Muraro, A. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: Part I. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 657–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wollenberg, A.; Kinberger, M.; Arents, B.; Aszodi, N.; Avila Valle, G.; Barbarot, S.; Bieber, T.; Brough, H.; Calzavara Pinton, P.; Christen-Zäch, S. European guideline (EuroGuiDerm) on atopic eczema–part II: Non-systemic treatments and treatment recommendations for special AE patient populations. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1904–1926. [Google Scholar] [CrossRef] [PubMed]


| Population | Patients with atopic dermatitis (all ages) |
| Intervention | Practices and perceptions of community pharmacists in the management of atopic dermatitis |
| Control | None |
| Outcome | Main: Pharmacists’ knowledge, recommendations, attitudes, and experiences regarding the management of atopic dermatitis Secondary: Perspectives of others (healthcare providers, patients, and parents) regarding the practices of pharmacists |
| Study design | Qualitative, quantitative, and mixed methods studies |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cayci, A.B.; Rathbone, A.P.; Lindsey, L. Practices and Perceptions of Community Pharmacists in the Management of Atopic Dermatitis: A Systematic Review and Thematic Synthesis. Healthcare 2023, 11, 2159. https://doi.org/10.3390/healthcare11152159
Cayci AB, Rathbone AP, Lindsey L. Practices and Perceptions of Community Pharmacists in the Management of Atopic Dermatitis: A Systematic Review and Thematic Synthesis. Healthcare. 2023; 11(15):2159. https://doi.org/10.3390/healthcare11152159
Chicago/Turabian StyleCayci, Abdi Berk, Adam Pattison Rathbone, and Laura Lindsey. 2023. "Practices and Perceptions of Community Pharmacists in the Management of Atopic Dermatitis: A Systematic Review and Thematic Synthesis" Healthcare 11, no. 15: 2159. https://doi.org/10.3390/healthcare11152159