A Feasibility Study of AlzLife 40 Hz Sensory Therapy in Patients with MCI and Early AD

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
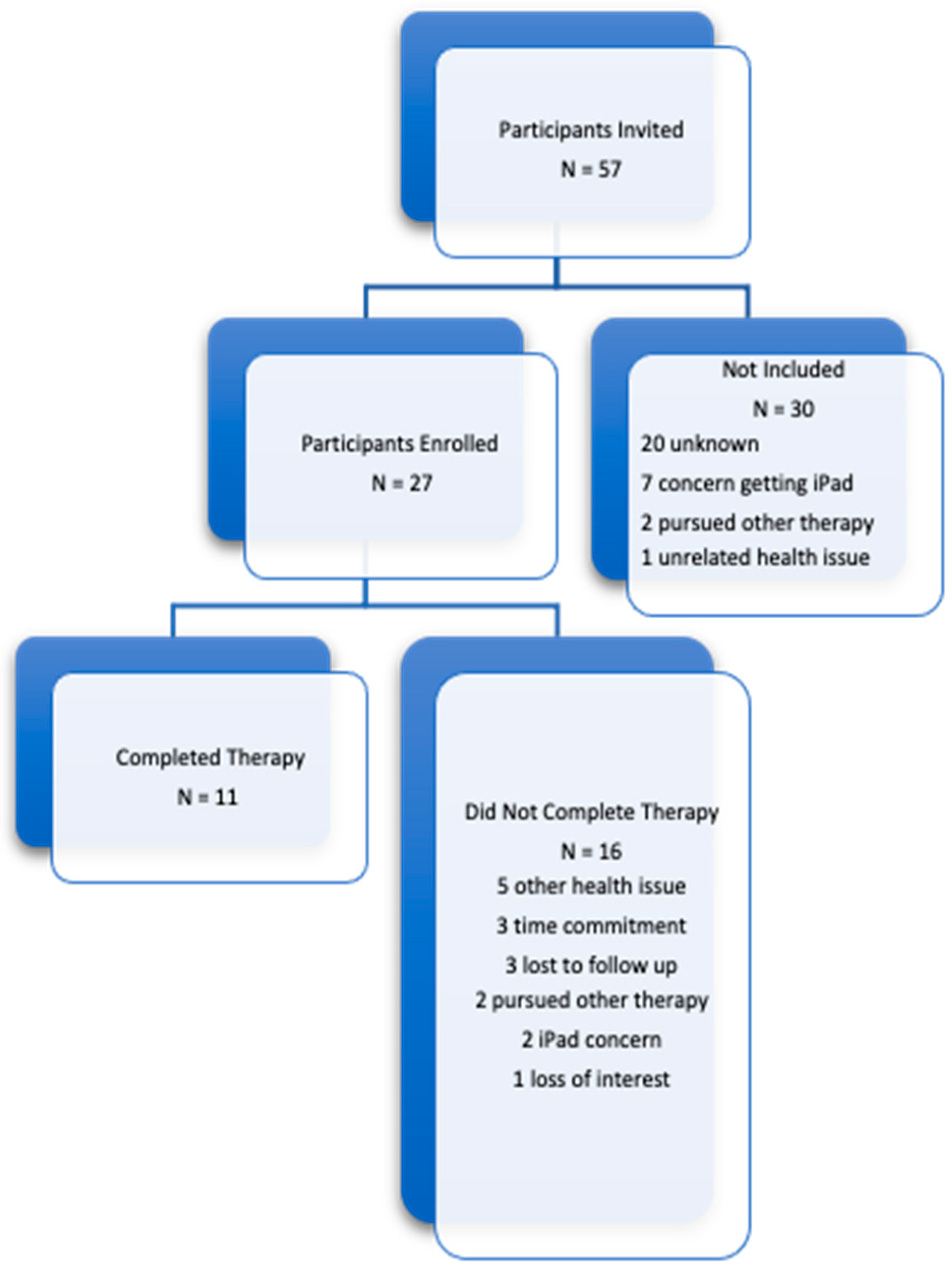
2.1. Participants
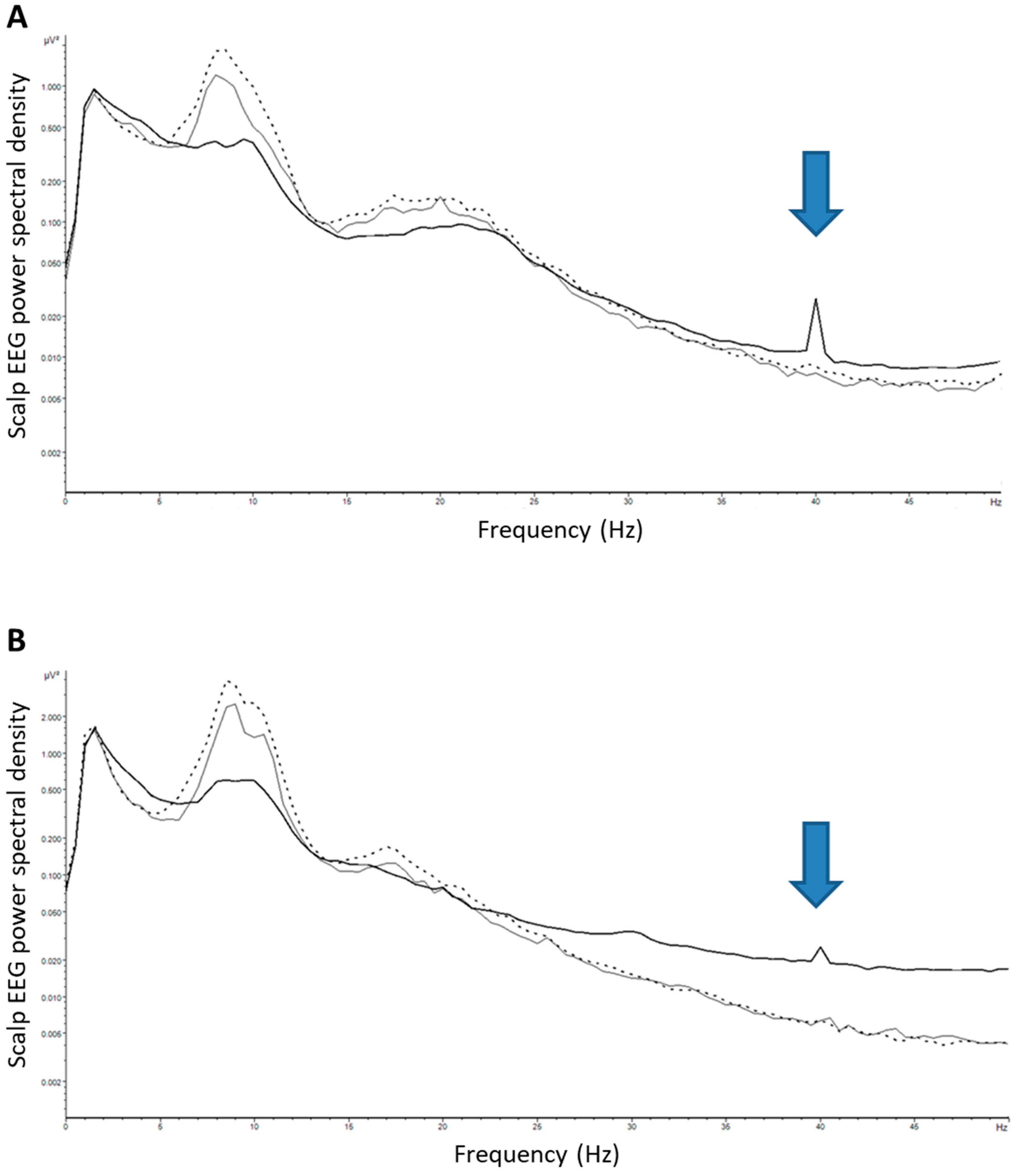
2.2. Evaluation of Induced Entrainment Using Scalp EEG Recording with Sensory Stimulation
3. Results
- P001 (enrolled with subjective cognitive complaints): “Well I mean I can’t say it was like a lightning strike or something, but I sort of feel like it may have helped, maybe a little bit focusing, I don’t know how to describe it, just attention.”
- P002 (enrolled with subjective cognitive complaints): “I don’t have to search as long for words. [...] I find that I have regular conversations with people and I’m not caught in the middle of a sentence stumbling. I feel that that is better.”
- P013 (AD): “[The therapy] Improved my thinking. Could answer questions I couldn’t before in general conversation.”
- P020: (AD) Has noticed “Feeling more in control, not so frustrated”.
- P002: Has noticed she “doesn’t get stuck in the middle of trying to find her words” like the “desk drawer is open”.
- P003 (enrolled with subjective cognitive complaints): “My impression is that there hasn’t been any deterioration.”
- P023 (AD): “During the first 3 months using the AlzLife app I thought she was showing improvement, I’m not sure now.”
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feigin, V.L.; Nichols, E.; Alam, T.; Bannick, M.S.; Beghi, E.; Blake, N.; Fischer, F. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stites, S.D.; Harkins, K.; Rubright, J.D.; Karlawish, J. Relationships between Cognitive Complaints and Quality of Life in Older Adults with Mild Cognitive Impairment, Mild Alzheimer’s Disease Dementia, and Normal Cognition. Alzheimer Dis. Assoc. Disord. 2018, 32, 276. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.L.; Morstorf, T.; Zhong, K. Alzheimer’s disease drug-development pipeline: Few candidates, frequent failures. Alzheimer’s Res. Ther. 2014, 6, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardy, J.; Selkoe, D.J. The amyloid hypothesis of Alzheimer’s disease: Progress and problems on the road to therapeutics. Science 2002, 297, 353–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy, D.S.; Arons, A.; Mitchell, T.I.; Pignatelli, M.; Ryan, T.J.; Tonegawa, S. Memory retrieval by activating engram cells in mouse models of early Alzheimer’s disease. Nature 2016, 531, 508–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iaccarino, H.F.; Singer, A.C.; Martorell, A.J.; Rudenko, A.; Gao, F.; Gillingham, T.Z.; Tsai, L.H.; Mathys, H.; Seo, J.; Kritskiy, O.; et al. Gamma frequency entrainment attenuates amyloid load and modifies microglia. Nature 2016, 540, 230–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martorell, A.J.; Paulson, A.L.; Suk, H.J.; Abdurrob, F.; Drummond, G.T.; Guan, W.; Tsai, L.H.; Young, J.Z.; Kim, D.N.-W.; Kritskiy, O.; et al. Multi-sensory gamma stimulation ameliorates Alzheimer’s-associated pathology and improves cognition. Cell 2019, 177, 256–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, Q.; Colon-Motas, K.M.; Pybus, A.F.; Piendel, L.; Seppa, J.K.; Walker, M.L.; Singer, A.C. A feasibility trial of gamma sensory flicker for patients with prodromal Alzheimer’s disease. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2021, 7, e12178. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.; Suk, H.-J.; Jackson, B.L.; Milman, N.P.; Stark, D.; Klerman, E.B.; Kitchener, E.; Fernandez Avalos, V.S.; de Weck, G.; Banerjee, A.; et al. Gamma frequency sensory stimulation in mild probable Alzheimer’s dementia patients: Results of feasibility and pilot studies. PLoS ONE 2022, 17, e0278412. [Google Scholar] [CrossRef]
- Mably, A.J.; Colgin, L.L. Gamma oscillations in cognitive disorders. Curr. Opin. Neurobiol. 2018, 52, 182–187. [Google Scholar] [CrossRef]
- Colgin, L.L.; Denninger, T.; Fyhn, M.; Hafting, T.; Bonnevie, T.; Jensen, O.; Moser, E.I. Frequency of gamma oscillations routes flow of information in the hippocampus. Nature 2009, 462, 353–357. [Google Scholar] [CrossRef]
- Abeysinghe, A.A.D.T.; Deshapriya, R.D.U.S.; Udawatte, C. Alzheimer’s disease; a review of the pathophysiological basis and therapeutic interventions. Life Sci. 2020, 256, 117996. [Google Scholar] [CrossRef] [PubMed]
- Marucci, G.; Buccioni, M.; Dal Ben, D.; Lambertucci, C.; Volpini, R.; Amenta, F. Efficacy of acetylcholinesterase inhibitors in Alzheimer’s disease. Neuropharmacology 2021, 190, 108352. [Google Scholar] [CrossRef] [PubMed]
- Sevigny, J.; Chiao, P.; Bussière, T.; Weinreb, P.H.; Williams, L.; Maier, M.; Sandrock, A. The antibody aducanumab reduces Aβ plaques in Alzheimer’s disease. Nature 2016, 537, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Hershey, L.A.; Tarawneh, R. Clinical efficacy, drug safety, and surrogate endpoints: Has aducanumab met all of its expectations? Neurology 2021, 97, 517–518. [Google Scholar] [CrossRef] [PubMed]
- Larner, A.J. Screening utility of the Montreal Cognitive Assessment (MoCA): In place of—Or as well as—The MMSE? Int. Psychogeriatr. 2012, 24, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Vyshedskiy, A.; Netson, R.; Fridberg, E.; Jagadeesan, P.; Arnold, M.; Barnett, S.; Gondalia, A.; Maslova, V.; de Torres, L.; Ostrovsky, S.; et al. Boston cognitive assessment (BOCA)—A comprehensive self-administered smartphone- and computer-based at-home test for longitudinal tracking of cognitive performance. BMC Neurol. 2022, 22, 92. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sex | Age | Diagnosis | MOCA Base Line | MOCA 3 Months | MOCA 6 Months | MOCA 3 Months Change from Baseline | MOCA 6 Months Change from Baseline | MOCA Improvement | |
|---|---|---|---|---|---|---|---|---|---|
| P001 | F | 72 | Subjective cognitive complaints, family hx of AD | 29 | 29 | 30 | 0 | 1 | Y |
| P002 | F | 69 | Subjective cognitive complaints, APOE4++ status | 27 | 30 | 29 | 3 | 2 | Y |
| P003 | F | 75 | AD | 23 | 21 | 24 | −2 | 1 | Y |
| P004 | F | 67 | Subjective cognitive complaints, family hx of AD, APOE4+ status | 30 | 29 | 28 | −1 | −2 | N |
| P005 | F | 87 | AD | 22 | - | 23 | - | 1 | Y |
| P009 | F | 75 | Subjective cognitive complaints | 26 | 25 | 25 | −1 | −1 | N |
| P0013 | M | 95 | AD | 19 | 19 | 19 | 0 | 0 | N |
| P0014 | M | 77 | MCI | 23 | 21 | 25 | −2 | 2 | Y |
| P020 | F | 82 | AD | - | 26 | 26 | 0 | - | - |
| P023 | F | 89 | AD | 23 | 17 | 18 | −6 | −5 | N |
| P024 | F | 89 | AD | 0 | 0 | 0 | 0 | 0 | N |
| Mean | −0.9 | −0.1 | |||||||
| SD | 2.2 | 2.0 |
| Sex | Age | Diagnosis | MOCA-MIS Baseline | MOCA-MIS 3 Months | MOCA-MIS 6 Months | MOCA-MIS 3 Months Change from Baseline | MOCA-MIS 6 Months Change from Baseline | MOCA-MIS Improvement from Baseline | |
|---|---|---|---|---|---|---|---|---|---|
| P001 | F | 72 | Subjective cognitive complaints, family hx of AD | 14 | 14 | 15 | 0 | 1 | Y |
| P002 | F | 69 | Subjective cognitive complaints, APOE4++ status | 11 | 14 | 13 | 3 | 2 | Y |
| P003 | F | 75 | AD | 6 | 2 | 15 | −4 | 9 | Y |
| P004 | F | 67 | Subjective cognitive complaints, family hx of AD, APOE4+ status | 15 | 15 | 13 | 0 | −2 | N |
| P005 | F | 87 | AD | 8 | - | 8 | - | 0 | N |
| P009 | F | 75 | Subjective cognitive complaints | 11 | 11 | 5 | 0 | −6 | N |
| P0013 | M | 95 | AD | - | 3 | 4 | 3 | 4 | - |
| P0014 | M | 77 | MCI | 12 | 11 | 8 | −1 | −4 | N |
| P020 | F | 82 | AD | - | 13 | 13 | - | - | - |
| P023 | F | 89 | AD | 3 | 4 | 0 | 1 | −3 | N |
| P024 | F | 89 | AD | 0 | 0 | 0 | 0 | 0 | N |
| Mean | 0.2 | 0.1 | |||||||
| SD | 2.1 | 4.3 |
| Sex | Age | Diagnosis | BOCA Baseline | BOCA 3 Months | BOCA 6 Months | BOCA 3 Months Change from Baseline | BOCA 6 Months Change from Baseline | BOCA Improvement | |
|---|---|---|---|---|---|---|---|---|---|
| P001 | F | 72 | Subjective cognitive complaints, family hx of AD | 29 | 28 | 29 | −1 | 0 | N |
| P002 | F | 69 | Subjective cognitive complaints, APOE4++ status | 28 | 27 | 28 | −1 | 0 | N |
| P003 | F | 75 | AD | 16 | 18 | 21 | 2 | 5 | Y |
| P004 | F | 67 | Subjective cognitive complaints, family hx of AD, APOE4+ status | 28 | 25 | 29 | −3 | 1 | Y |
| P005 | F | 87 | AD | 21 | - | - | - | - | - |
| P009 | F | 75 | Subjective cognitive complaints | 25 | - | - | - | - | - |
| P0013 | M | 95 | AD | 15 | 22 | 30 | 7 | 15 | Y |
| P0014 | M | 77 | MCI | - | - | - | - | - | - |
| P020 | F | 82 | AD | 26 | 24 | 28 | −2 | 2 | Y |
| P023 | F | 89 | AD | 21 | 18 | - | - | - | - |
| P024 | F | 89 | AD | 0 | 0 | 0 | 0 | 0 | N |
| Mean | 0.3 | 3.3 | |||||||
| SD | 3.4 | 5.5 |
| Sex | Age | Diagnosis | Subjective Improvement (Participant) | Subjective Improvement (Caregiver) | |
|---|---|---|---|---|---|
| P001 | F | 72 | Subjective cognitive complaints, family hx of AD | Y | - |
| P002 | F | 69 | Subjective cognitive complaints, APOE4++ status | Y | - |
| P003 | F | 75 | AD | N | N |
| P004 | F | 67 | Subjective cognitive complaints, family hx of AD, APOE4+ status | - | - |
| P005 | F | 87 | AD | - | - |
| P009 | F | 75 | Subjective cognitive complaints | - | - |
| P0013 | M | 95 | AD | Y | Y |
| P0014 | M | 77 | MCI | N | Y |
| P020 | F | 82 | AD | Y | Y |
| P023 | F | 89 | AD | - | Y then N |
| P024 | F | 89 | AD | - | N |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McNett, S.D.; Vyshedskiy, A.; Savchenko, A.; Durakovic, D.; Heredia, G.; Cahn, R.; Kogan, M. A Feasibility Study of AlzLife 40 Hz Sensory Therapy in Patients with MCI and Early AD. Healthcare 2023, 11, 2040. https://doi.org/10.3390/healthcare11142040
McNett SD, Vyshedskiy A, Savchenko A, Durakovic D, Heredia G, Cahn R, Kogan M. A Feasibility Study of AlzLife 40 Hz Sensory Therapy in Patients with MCI and Early AD. Healthcare. 2023; 11(14):2040. https://doi.org/10.3390/healthcare11142040
Chicago/Turabian StyleMcNett, Sienna D., Andrey Vyshedskiy, Andrei Savchenko, Danijel Durakovic, George Heredia, Rael Cahn, and Mikhail Kogan. 2023. "A Feasibility Study of AlzLife 40 Hz Sensory Therapy in Patients with MCI and Early AD" Healthcare 11, no. 14: 2040. https://doi.org/10.3390/healthcare11142040