
Comparative Analysis of Fall Risk Assessment Features in Community-Elderly and Stroke Survivors: Insights from Sensor-Based Data

Abstract
:1. Introduction
2. Materials and Methods
2.1. General Approach
2.2. Subjects
2.2.1. Community-Dwelling Elderly
2.2.2. Stroke Survivors
2.3. Clinical Tests
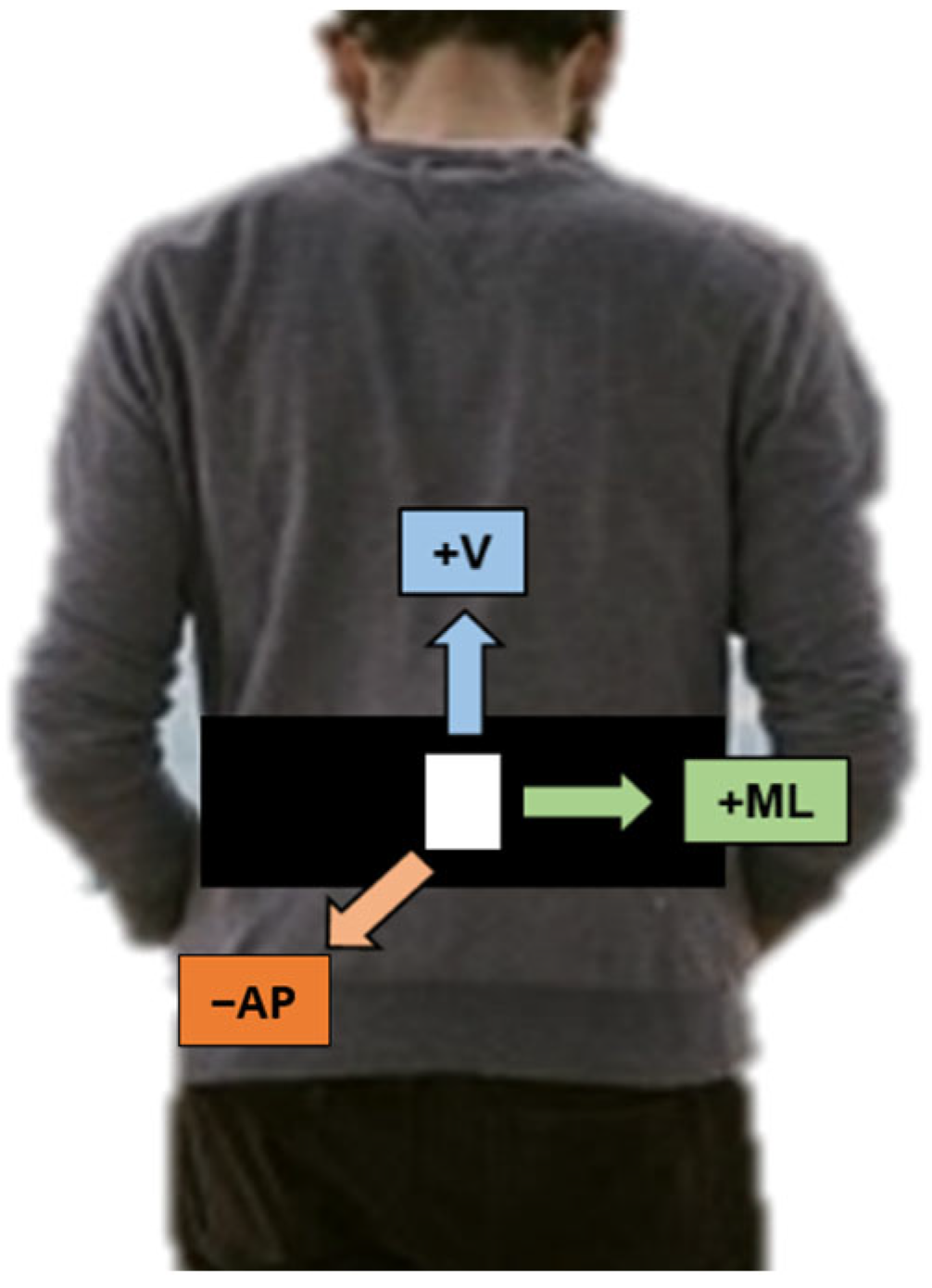
2.4. Wearable Accelerometer
2.5. Data Analysis
2.5.1. Feature Extraction
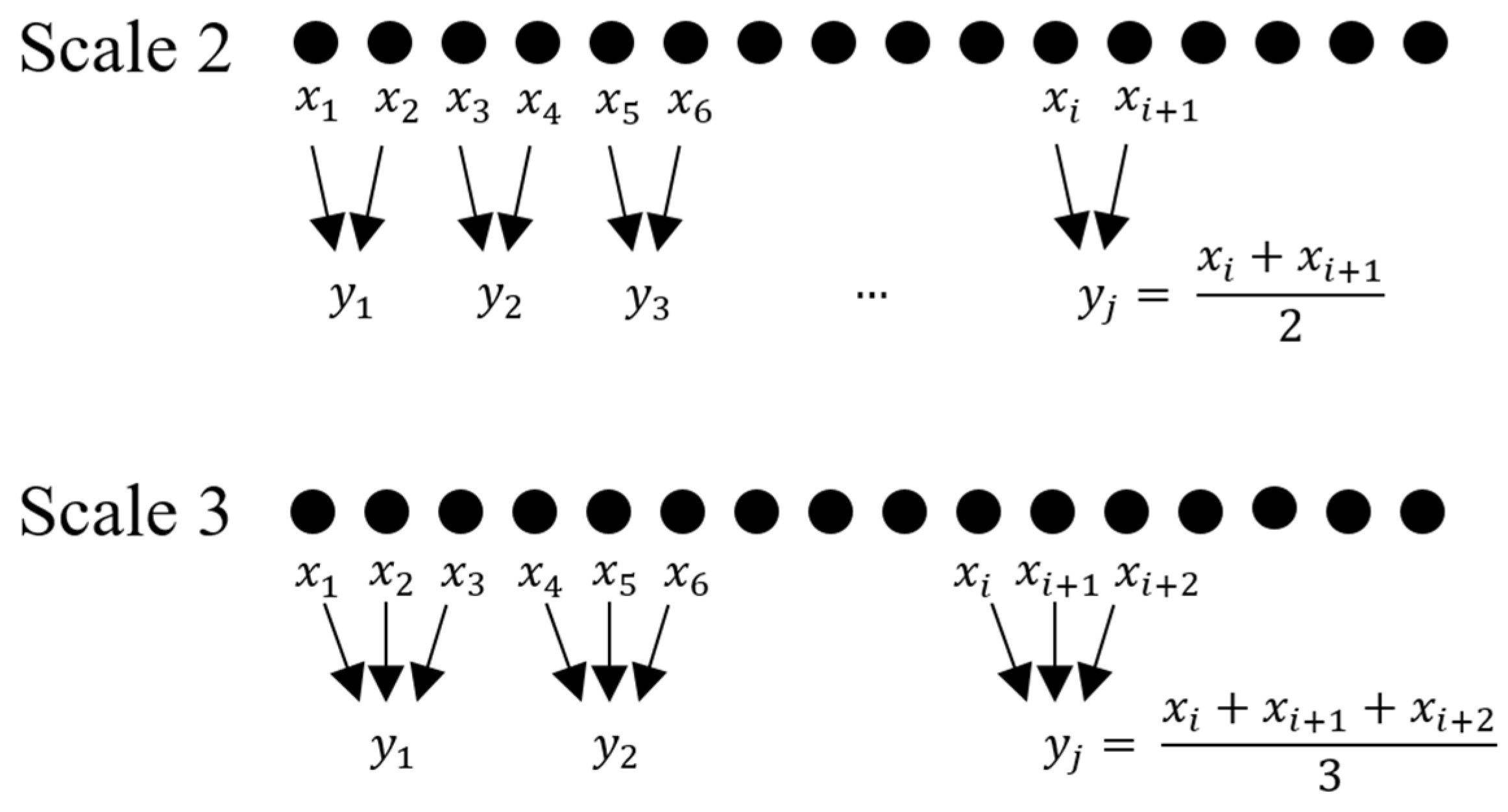
2.5.2. Multiscale Entropy (MSE) Analysis
2.5.3. Permutation Entropy (PE)
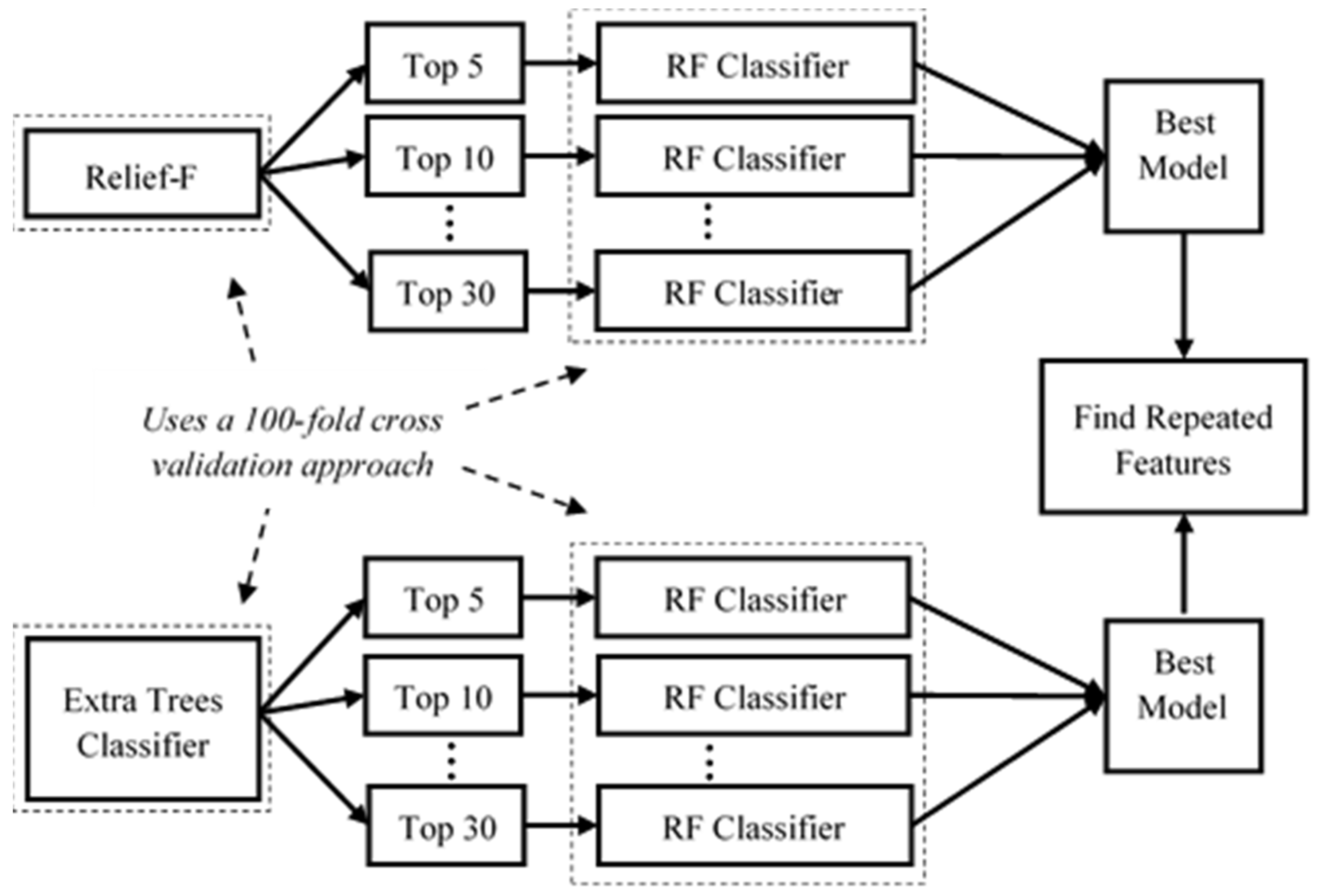
2.6. Feature Importance and Classification
2.6.1. Relief-F
2.6.2. Extra Trees Classifier (ETC)
3. Results and Discussion
3.1. Top Features Selected by Both Feature Selection Algorithms for Each Subject Group
3.2. Best-Performing Models for Each Clinical Test, Feature Selection Mechanism, and Subject Group
3.3. Most Important Features for the Community-Dwelling Elderly and Stroke Survivors
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Olson, M.; Lockhart, T. Predicting fall risk through automatic wearable monitoring: A systematic review. Int. J. Progn. Health Manag. 2021, 12, 1–15. [Google Scholar] [CrossRef]
- Day, L.; Finch, C.F.; Hill, K.D.; Haines, T.P.; Clemson, L.; Thomas, M.; Thompson, C. A protocol for evidence-based targeting and evaluation of statewide strategies for preventing falls among community-dwelling older people in Victoria, Australia. INJ Prev. 2011, 17, e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stenhagen, M.; Nordell, E.; Elmståhl, S. Falls in elderly people: A multifactorial analysis of risk markers using data from the Swedish general population study ‘Good Ageing in Skåne’. Aging Clin. Exp. Res. 2013, 25, 59–67. [Google Scholar] [CrossRef] [PubMed]
- NICE. Falls in Older People: Assessing Risk and Prevention. 2013. Available online: https://www.nice.org.uk/guidance/cg161/resources/falls-in-older-people-assessing-risk-and-prevention-35109686728645 (accessed on 25 September 2022).
- Rubenstein, L.Z.; Robbins, A.S.; Schulman, B.L.; Rosado, J.; Osterweil, D.; Josephson, K.R. Falls and instability in the elderly. J. Am. Geriatr. Soc. 1988, 36, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Perry, B.C. Falls Among the Elderly. J. Am. Geriatr. Soc. 1982, 30, 788. [Google Scholar] [CrossRef]
- Sharif, R.S.; Al-Daour, D.S. Falls in the elderly: Assessment of prevalence and risk factors. Pharm. Pract. 2018, 16, 1–7. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6207352/pdf/pharmpract-16-1206.pdf (accessed on 26 September 2022). [CrossRef] [Green Version]
- Cuevas-Trisan, R. Balance Problems and Fall Risks in the Elderly. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 727–737. [Google Scholar] [CrossRef]
- Campbell, G.B.; Matthews, J.T. An integrative review of factors associated with falls during post-stroke rehabilitation. J. Nurs. Sch. 2010, 42, 395–404. [Google Scholar] [CrossRef] [Green Version]
- Thoker, A. Post Stroke Risk Factors of Fall during Rehabilitation in Elderly Patients. J. Physiother. Phys. Rehabil. 2021, 6, 1–5. [Google Scholar]
- Xu, T.; Clemson, L.; O’Loughlin, K.; Lannin, N.A.; Dean, C.; Koh, G. Risk Factors for Falls in Community Stroke Survivors: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2018, 99, 563–573.e5. [Google Scholar] [CrossRef]
- Belgen, B.; Beninato, M.; Sullivan, P.E.; Narielwalla, K. The association of balance capacity and falls self-efficacy with history of falling in community-dwelling people with chronic stroke. Arch. Phys. Med. Rehabil. 2006, 87, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.E.; De Silva, D.A.; Chang, H.M.; Yao, J.; Matchar, D.B.; Young, S.H.Y.; See, S.J.; Lim, G.H.; Wong, T.H.; Venketasubramanian, N. Post-stroke patients with moderate function have the greatest risk of falls: A National Cohort Study. BMC Geriatr. 2019, 19, 373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howcroft, J.; Kofman, J.; Lemaire, E.D. Review of fall risk assessment in geriatric populations using inertial sensors. J. Neuroeng. Rehabil. 2013, 10, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wüest, S.; Massé, F.; Aminian, K.; Gonzenbach, R.; De Bruin, E.D. Reliability and validity of the inertial sensor-based Timed “Up and Go” test in individuals affected by stroke. J. Rehabil. Res. Dev. 2016, 53, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Salarian, A.; Horak, F.B.; Zampieri, C.; Carlson-Kuhta, P.; Nutt, J.G.; Aminian, K. iTUG, a sensitive and reliable measure of mobility. IEEE Trans. Neural Syst. Rehabil. Eng. 2010, 18, 303–310. [Google Scholar] [CrossRef] [Green Version]
- van Lummel, R.C.; Walgaard, S.; Hobert, M.A.; Maetzler, W.; van Dieën, J.H.; Galindo-Garre, F.; Terwee, C.B. Intra-rater, inter-rater and test-retest reliability of an instrumented timed up and go (itug) test in patients with Parkinson’s disease. PLoS ONE 2016, 11, e0151881. [Google Scholar] [CrossRef] [Green Version]
- Patel, M.; Pavic, A.; Goodwin, V.A. Wearable inertial sensors to measure gait and posture characteristic differences in older adult fallers and non-fallers: A scoping review. Gait Posture 2019, 76, 110–121. [Google Scholar] [CrossRef]
- Mannini, A.; Trojaniello, D.; Cereatti, A.; Sabatini, A.M. A machine learning framework for gait classification using inertial sensors: Application to elderly, post-stroke and Huntington’s disease patients. Sensors 2016, 16, 134. [Google Scholar] [CrossRef] [Green Version]
- Shahzad, A.; Ko, S.; Lee, S.; Lee, J.-A.; Kim, K. Quantitative Assessment of Balance Impairment for Fall-Risk Estimation Using Wearable Triaxial Accelerometer. IEEE Sens. J. 2017, 17, 6743–6751. [Google Scholar] [CrossRef]
- Palumbo, P.; Palmerini, L.; Bandinelli, S.; Chiari, L. Fall risk assessment tools for elderly living in the community: Can we do better? PLoS ONE 2015, 10, e0146247. [Google Scholar] [CrossRef] [Green Version]
- Cella, A.; De Luca, A.; Squeri, V.; Parodi, S.; Vallone, F.; Giorgeschi, A.; Senesi, B.; Zigoura, E.; Guerrero, K.L.Q.; Siri, G.; et al. Development and validation of a robotic multifactorial fall-risk predictive model: A one-year prospective study in community-dwelling older adults. PLoS ONE 2020, 15, e0234904. [Google Scholar] [CrossRef]
- Alexandre, T.S.; Meira, D.M.; Rico, N.C.; Mizuta, S.K. Accuracy of Timed Up and Go Test for screening risk of falls among community-dwelling elderly. Braz. J. Phys. Ther. 2012, 16, 381–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Podsiadlo, S.; Richardson, D. The Timed Up and Go: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Saber-Sheikh, K.; Bryant, E.C.; Glazzard, C.; Hamel, A.; Lee, R.Y. Feasibility of using inertial sensors to assess human movement. Man. Ther. 2010, 15, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Menz, H.B.; Lord, S.R.; Fitzpatrick, R.C. A structural equation model relating impaired sensorimotor function, fear of falling and gait patterns in older people. Gait Posture 2007, 25, 243–249. [Google Scholar] [CrossRef]
- Kavanagh, J.; Barrett, R.; Morrison, S. Upper body accelerations during walking in healthy young and elderly men. Gait Posture 2004, 20, 291–298. [Google Scholar] [CrossRef]
- Winter, D.A. Book Review the Biomechanics and Motor Control of Human Gait: Normal, Elderly, and Pathological; University of Waterloo Press: Waterloo, ON, Canada, 1992. [Google Scholar]
- Matsumoto, H.; Makabe, T.; Morita, T.; Ikuhara, K.; Kajigase, A.; Okamoto, Y.; Ashikawa, E.; Kobayashi, E.; Hagino, H. Accelerometry-based gait analysis predicts falls among patients with a recent fracture who are ambulatory: A 1-year prospective study. Int. J. Rehabil. Res. 2015, 38, 131–136. [Google Scholar] [CrossRef]
- Nishiguchi, S.; Yamada, M.; Nagai, K.; Mori, S.; Kajiwara, Y.; Sonoda, T.; Yoshimura, K.; Yoshitomi, H.; Ito, H.; Okamoto, K.; et al. Reliability and validity of gait analysis by android-based smartphone. Telemed. e-Health 2012, 18, 292–296. [Google Scholar] [CrossRef] [Green Version]
- Yamada, M.; Aoyama, T.; Mori, S.; Nishiguchi, S.; Okamoto, K.; Ito, T.; Muto, S.; Ishihara, T.; Yoshitomi, H.; Ito, H. Objective assessment of abnormal gait in patients with rheumatoid arthritis using a smartphone. Rheumatol. Int. 2012, 32, 3869–3874. [Google Scholar] [CrossRef]
- Schot, S.H. Jerk: The time rate of change of acceleration. Am. J. Phys. 1978, 46, 1090–1094. [Google Scholar] [CrossRef]
- Pozaic, T.; Lindemann, U.; Grebe, A.-K.; Stork, W. Sit-to-Stand Transition Reveals Acute Fall Risk in Activities of Daily Living. IEEE J. Transl. Eng. Health Med. 2016, 4, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ejupi, A.; Brodie, M.; Lord, S.R.; Annegarn, J.; Redmond, S.J.; Delbaere, K. Wavelet-Based Sit-To-Stand Detection and Assessment of Fall Risk in Older People Using a Wearable Pendant Device. IEEE Trans. Biomed. Eng. 2016, 64, 1602–1607. [Google Scholar] [CrossRef] [PubMed]
- Yack, H.J.; Berger, R.C. Dynamic stability in the elderly: Identifying a possible measure. J. Gerontol. 1993, 48, M225–M230. [Google Scholar] [CrossRef] [PubMed]
- Cho, C.-Y.; Kamen, G. Detecting balance deficits in frequent fallers using clinical and quantitative evaluation tools. J. Am. Geriatr. Soc. 1998, 46, 426–430. [Google Scholar] [CrossRef]
- Weiss, A.; Herman, T.; Plotnik, M.; Brozgol, M.; Giladi, N.; Hausdorff, J.M. An instrumented timed up and go: The added value of an accelerometer for identifying fall risk in idiopathic fallers. Physiol. Meas. 2011, 32, 2003–2018. [Google Scholar] [CrossRef]
- Terrier, P.; Reynard, F. Effect of age on the variability and stability of gait: A cross-sectional treadmill study in healthy individuals between 20 and 69 years of age. Gait Posture 2015, 41, 170–174. [Google Scholar] [CrossRef] [Green Version]
- Isho, T.; Tashiro, H.; Usuda, S. Accelerometry-based gait characteristics evaluated using a smartphone and their association with fall risk in people with chronic stroke. J. Stroke Cerebrovasc. Dis. 2015, 24, 1305–1311. [Google Scholar] [CrossRef] [PubMed]
- Mohler, J.M.; Wendel, C.S.; Taylor-Piliae, R.E.; Toosizadeh, N.; Najafi, B. Motor performance and physical activity as predictors of prospective falls in community-dwelling, older adults by frailty level: Application of wearable technology. Gerontology 2017, 176, 139–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razjouyan, J.; Grewal, G.S.; Rishel, C.; Parthasarathy, S.; Mohler, J.; Najafi, B. Activity monitoring and heart rate variability as indicators of fall risk: Proof-of-concept for application of wearable sensors in the acute care setting. J. Gerontol. Nurs. 2017, 43, 53–62. [Google Scholar] [CrossRef]
- Schwenk, M.; Hauer, K.; Zieschang, T.; Englert, S.; Mohler, J.; Najafi, B. Sensor-derived physical activity parameters can predict future falls in people with dementia. Gerontology 2014, 60, 483–492. [Google Scholar] [CrossRef] [Green Version]
- van Schooten, K.S.; Pijnappels, M.; Rispens, S.M.; Elders, P.J.M.; Lips, P.; van Dieën, J.H. Ambulatory Fall-Risk Assessment: Amount and Quality of Daily-Life Gait Predict Falls in Older Adults. J. Gerontol. Ser. A 2015, 70, 608–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mbourou, G.A.; Lajoie, Y.; Teasdale, N. Step length variability at gait initiation in elderly fallers and non-fallers, and young adults. Gerontology 2003, 49, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Lindemann, U.; Lundin-Olsson, L.; Hauer, K.; Wengert, M.; Becker, C.; Pfeiffer, K. Maximum step length as a potential screening tool for falls in non-disabled older adults living in the community. Aging Clin. Exp. Res. 2008, 20, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Kirkwood, R.N.; Moreira, B.d.S.; Vallone, M.L.; Mingoti, S.A.; Dias, R.C.; Sampaio, R.F. Step length appears to be a strong discriminant gait parameter for elderly females highly concerned about falls: A cross-sectional observational study. Physiotherapy 2011, 97, 126–131. [Google Scholar] [CrossRef]
- van Schooten, K.S.; Pijnappels, M.; Rispens, S.M.; Elders, P.J.M.; Lips, P.; Daffertshofer, A.; Beek, P.J.; van Dieën, J.H. Daily-life gait quality as predictor of falls in older people: A 1-year prospective cohort study. PLoS ONE 2016, 11, e0158623. [Google Scholar] [CrossRef] [Green Version]
- Weiss, A.; Brozgol, M.; Dorfman, M.; Herman, T.; Shema, S.; Giladi, N.; Hausdorff, J.M. Does the evaluation of gait quality during daily life provide insight into fall risk? A novel approach using 3-day accelerometer recordings. Neurorehabilit. Neural Repair 2013, 27, 742–752. [Google Scholar] [CrossRef]
- Balasubramanian, C.K.; Neptune, R.R.; Kautz, S.A. Variability in spatiotemporal step characteristics and its relationship to walking performance post-stroke. Gait Posture 2009, 29, 408–414. [Google Scholar] [CrossRef] [Green Version]
- Balaban, B.; Tok, F. Gait Disturbances in Patients with Stroke. PM&R 2014, 6, 635–642. [Google Scholar] [CrossRef]
- Sterke, C.S.; van Beeck, E.F.; Looman, C.W.; Kressig, R.W.; van der Cammen, T.J. An electronic walkway can predict short-term fall risk in nursing home residents with dementia. Gait Posture 2012, 36, 95–101. [Google Scholar] [CrossRef]
- Greene, B.R.; O’Donovan, A.; Romero-Ortuno, R.; Cogan, L.; Ni Scanaill, C.; Kenny, R.A. Quantitative Falls Risk Assessment Using the Timed Up and Go Test. IEEE Trans. Biomed. Eng. 2010, 57, 2918–2926. [Google Scholar] [CrossRef]
- Doheny, E.P.; Greene, B.R.; Foran, T.; Cunningham, C.; Fan, C.W.; Kenny, R.A. Diurnal variations in the outcomes of instrumented gait and quiet standing balance assessments and their association with falls history. Physiol. Meas. 2012, 33, 361–373. [Google Scholar] [CrossRef] [PubMed]
- Ganea, R.; Paraschiv-Ionescu, A.; Büla, C.; Rochat, S.; Aminian, K. Multi-parametric evaluation of sit-to-stand and stand-to-sit transitions in elderly people. Med. Eng. Phys. 2011, 33, 1086–1093. [Google Scholar] [CrossRef] [PubMed]
- Millor, N.; Lecumberri, P.; Gomez, M.; Martinez-Ramirez, A.; Izquierdo, M. Kinematic parameters to evaluate functional performance of sit-to-stand and stand-to-sit transitions using motion sensor devices: A systematic review. IEEE Trans. Neural Syst. Rehabilitation Eng. 2014, 22, 926–936. [Google Scholar] [CrossRef]
- Doheny, E.P.; Walsh, C.; Foran, T.; Greene, B.R.; Fan, C.W.; Cunningham, C.; Kenny, R.A. Falls classification using tri-axial accelerometers during the five-times-sit-to-stand test. Gait Posture 2013, 38, 1021–1025. [Google Scholar] [CrossRef]
- Cheng, P.-T.; Liaw, M.-Y.; Wong, M.-K.; Tang, F.-T.; Lee, M.-Y. The Sit-to-Stand Movement in Stroke Patients and Its Correlation With Falling. Am. Congr. Rehabil. Med. 1998, 79, 1043–1046. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.; Goldberger, A.; Peng, C.-K. Multiscale entropy to distinguish physiologic and synthetic RR time series. Comput. Cardiol. 2002, 29, 137–140. [Google Scholar] [CrossRef]
- American Geriatrics Society; British Geriatrics Society; American Academy of Orthopaedic Surgeons Panel on Falls Preventiont. Guideline for the prevention of falls in older persons. J. Am. Geriatr. Soc. 2001, 49, 664–672. [Google Scholar] [CrossRef]
- Daines, K.J.F.; Baddour, N.; Burger, H.; Bavec, A.; Lemaire, E.D. Fall risk classification for people with lower extremity amputations using random forests and smartphone sensor features from a 6-minute walk test. PLoS ONE 2021, 16, e0247574. [Google Scholar] [CrossRef]
- Wong, T.-T. Performance evaluation of classification algorithms by k-fold and leave-one-out cross validation. Pattern Recognit. 2015, 48, 2839–2846. [Google Scholar] [CrossRef]
- Drover, D.; Howcroft, J.; Kofman, J.; Lemaire, E.D. Faller classification in older adults using wearable sensors based on turn and straight-walking accelerometer-based features. Sensors 2017, 17, 1321. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, N.F.; Santos, C.P. Two fall-related and kinematic data-based approaches for an instrumented conventional cane. IEEE Trans. Hum.-Mach. Syst. 2021, 51, 554–563. [Google Scholar] [CrossRef]
- Urbanowicz, R.J.; Meeker, M.; La Cava, W.; Olson, R.S.; Moore, J.H. Relief-based feature selection: Introduction and review. J. Biomed. Inform. 2018, 85, 189–203. [Google Scholar] [CrossRef]
- Song, Y.; Si, W.; Dai, F.; Yang, G. Weighted Relief with threshold constraints of feature selection for imbalanced data classification. Concurr. Comput. Pract. Exp. 2020, 32, e5691. [Google Scholar] [CrossRef]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Dentamaro, V.; Impedovo, D.; Pirlo, G. Fall detection by human pose estimation and kinematic theory. In Proceedings of the International Conference on Pattern Recognition, Milan, Italy, 10 January 2020; pp. 2328–2335. [Google Scholar] [CrossRef]
- Mathew, T.E. An optimized extremely randomized tree model for breast cancer classification. J. Theor. Appl. Inf. Technol. 2022, 31, 5234–5246. Available online: http://www.jatit.org (accessed on 14 February 2023).
- Geurts, P.; Ernst, D.; Wehenkel, L. Extremely randomized trees. Mach. Learn. 2006, 63, 3–42. [Google Scholar] [CrossRef] [Green Version]
- Hsu, Y.-C.; Zhao, Y.; Huang, K.-H.; Wu, Y.-T.; Cabrera, J.; Sun, T.-L.; Tsui, K.-L. A Novel Approach for Fall Risk Prediction Using the Inertial Sensor Data from the Timed-Up-and-Go Test in a Community Setting. IEEE Sens. J. 2020, 20, 9339–9350. [Google Scholar] [CrossRef]
- Montesinos, L.; Castaldo, R.; Pecchia, L. Wearable inertial sensors for fall risk assessment and prediction in older adults: A systematic review and meta-analysis. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 573–582. [Google Scholar] [CrossRef] [Green Version]
- Brauer, S.G.; Burns, Y.R.; Galley, P. A prospective study of laboratory and clinical measures of postural stability to predict community-dwelling fallers. J. Gerontol. Ser. A 2000, 55, M469–M476. [Google Scholar] [CrossRef] [Green Version]
- Lamb, S.; Ferrucci, L.; Volapto, S.; Fried, L.; Guralnik, J. Risk factors for falling in home-dwelling older women with stroke: The women’s health and aging study. Stroke 2003, 34, 494–501. [Google Scholar] [CrossRef] [Green Version]
- Patterson, K.K.; Gage, W.H.; Brooks, D.; Black, S.E.; McIlroy, W.E. Evaluation of gait symmetry after stroke: A comparison of current methods and recommendations for standardization. Gait Posture 2010, 31, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Ryerson, S.; Byl, N.N.; Brown, D.A.; Wong, R.A.; Hidler, J.M. Altered trunk position sense and its relation to balance functions in people post-stroke. J. Neurol. Phys. Ther. 2008, 32, 14–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najafi, B.; Armstrong, D.G.; Mohler, J. Novel wearable technology for assessing spontaneous daily physical activity and risk of falling in older adults with diabetes. J. Diabetes Sci. Technol. 2013, 7, 1147–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marschollek, D.; Nemitz, G.; Gietzelt, M.; Wolf, K.H.; Schwabedissen, H.M.Z.; Haux, R. Prädiktion von Stürzen stationärer Patienten in einer geriatrischen Klinik: Eine klinische Studie zur Kombination von Assessmentdaten und einfachen, sensorisch erfassten Gangparametern. Z. Gerontol. Geriatr. 2009, 42, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Zhang, B.; Wei, D. The elderly fall risk assessment and prediction based on gait analysis. In Proceedings of the 2011 IEEE 11th International Conference on Computer and Information Technology, Paphos, Cyprus, 31 August–2 September 2011; pp. 176–180. [Google Scholar]
- Zhao, G.; Chen, L.; Ning, H. Sensor-Based Fall Risk Assessment: A Survey. Healthcare 2021, 9, 1448. [Google Scholar] [CrossRef]
- Tmaura, T.; Zakaria, N.A.; Kuwae, Y.; Sekine, M.; Minato, K.; Yoshida, M. Quantitative analysis of the fall-risk assessment test with wearable inertia sensors. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Osaka, Japan, 3–7 July 2013; Volume 2013, pp. 7217–7220. [Google Scholar] [CrossRef]
- Reider, N.; Gaul, C. Fall risk screening in the elderly: A comparison of the minimal chair height standing ability test and 5-repetition sit-to-stand test. Arch. Gerontol. Geriatr. 2016, 65, 133–139. [Google Scholar] [CrossRef]
- Hyndman, D.; Ashburn, A.; Stack, E. Fall events among people with stroke living in the community: Circumstances of falls and characteristics of fallers. Arch. Phys. Med. Rehabil. 2002, 83, 165–170. [Google Scholar] [CrossRef]
- White, H.C. Post-stroke hip fractures. Arch. Orthop. Trauma Surg. 1988, 107, 345–347. [Google Scholar] [CrossRef]
- Nyberg, L.; Gustafson, Y. Patient falls in stroke rehabilitation. A challenge to rehabilitation strategies. Stroke 1995, 26, 838–842. [Google Scholar] [CrossRef]
- Chou, S.-W.; Wong, A.M.K.; Leong, C.-P.; Hong, W.-S.; Tang, F.-T.; Lin, T.-H. Postural control during sit-to stand and gait in stroke patients. Am. J. Phys. Med. Rehabil. 2003, 82, 42–47. [Google Scholar] [CrossRef]
- Lecours, J.; Nadeau, S.; Gravel, D.; Teixera-Salmela, L. Interactions between foot placement, trunk frontal position, weight-bearing and knee moment asymmetry at seat-off during rising from a chair in healthy controls and persons with hemiparesis. Acta Derm. Venereol. 2008, 40, 200–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunt, D.; Greenberg, B.; Wankadia, S.; Trimble, M.A.; Shechtman, O. The effect of foot placement on sit to stand in healthy young subjects and patients with hemiplegia. Arch. Phys. Med. Rehabil. 2002, 83, 924–929. [Google Scholar] [CrossRef] [PubMed]
- Mackintosh, S.; Hill, K.; Dodd, K.; Goldie, P.; Culham, E. Falls and injury prevention should be part of every stroke rehabilitation plan. Clin. Rehabil. 2005, 19, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Lamontagne, A.; Fung, J. Gaze and postural reorientation in the control of locomotor steering after stroke. Neurorehabilit. Neural Repair 2009, 23, 256–266. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Subject Group | Description | Value | Number of Participants | Age (Mean ± STD) |
|---|---|---|---|---|
| Community-dwelling Elderly | Gender | Female | 49 | 77 ± 6.60 |
| Male | 16 | 73 ± 6.00 | ||
| Age | 65–70 | 12 | 69 ± 1.72 | |
| 71–75 | 25 | 73 ± 1.53 | ||
| 76–80 | 12 | 78 ± 1.48 | ||
| >80 | 16 | 85 ± 4.60 | ||
| Situation (SFBBS) | Healthy | 61 | 72.64 ± 9.29 | |
| Fall-Risk | 13 | 78.5 ± 7.5 | ||
| Situation (TUG) | Healthy | 61 | 71.91 ± 8.81 | |
| Fall-Risk | 13 | 81.61 ± 6.46 | ||
| Stroke Survivors | Gender | Female | 22 | 61 ± 11.78 |
| Male | 13 | 61 ± 11.41 | ||
| Age | 15–20 | 1 | 18 ± 0 | |
| 21–30 | 0 | 0 | ||
| 31–40 | 4 | 34.5 ± 1.5 | ||
| 41–50 | 2 | 46.5 ± 2.5 | ||
| Situation (SFBBS) | 51–60 | 11 | 56 ± 3.23 | |
| 61–70 | 12 | 64 ± 1.32 | ||
| Situation (TUG) | 71–80 | 4 | 73 ± 1.51 | |
| >80 | 1 | 84 ± 0 |
| Feature Name (Feature Number) | |||
|---|---|---|---|
| Full TUG Features | |||
| MSE Mean (1–3) | MSE Standard Dev. (4–6) | MSE Complexity Idx. (7–9) | Permutation Ent. (10–12) |
| Sit to Stand (SiSt) Features | |||
| Stand Duration (13) | Range (14–16) | Maximum Value (17–19) | Root Mean Square (20–22) |
| Maximum Jerk (23–25) | Minimum Value (26–28) | Mean Jerk (29–31) | Standard Dev. (32–34) |
| Walk Features | |||
| Walk Duration (35) | Cadence (36) | Step Length (37) | Gait Speed (38) |
| Step Time (39) | Stride Time (40) | CV Step Time (41) | CV Stride Time (42) |
| Root Mean Square (43–45) | |||
| Turn Features | |||
| CV (46–48) | Median (49–51) | Range (52–54) | Root Mean Square (55–57) |
| Stand to Sit Features | |||
| Sit Duration (58) | Range (59–61) | Root Mean Square (62–64) | Minimum (65–67) |
| Maximum (68–70) | Maximum Jerk (71–73) | Mean Jerk (74–76) | Standard Deviation (77–79) |
| Feature Name | ||||||
|---|---|---|---|---|---|---|
| Top | Relief-F | ETC | ||||
| y = SFBBS | y = TUG | y = SFBBS + TUG | y = SFBBS | y = TUG | y = SFBBS + TUG | |
| 1 | Stand Duration | Stand Duration | Median Turn (ML) | Step Length | Gait Speed | Gait Speed |
| 2 | Gait Speed | RMS Turn (AP) | Range Turn (ML) | Gait Speed | Walk Duration | Walk Duration |
| 3 | Step Length | Min Stand (ML) | Stand Duration | Min Sit (ML) | Stand Duration | RMS Stand (ML) |
| 4 | Walk Duration | MSE Mean (AP) | Max Stand (AP) | RMS Walk (V) | Cadence | Std Stand (ML) |
| 5 | Std Stand (ML) | Jerk Stand (AP) | Range Sit (ML) | Walk Duration | RMS Walk (V) | Stand Duration |
| 6 | RMS Stand (ML) | RMS Stand (AP) | Min Sit (ML) | RMS Walk (ML) | Step Length | MSE Mean (AP) |
| 7 | MSE CI (ML) | Min Sit (V) | Gait Speed | MSE Mean (ML) | RMS Walk (ML) | Min Sit (ML) |
| 8 | MSE Mean (ML) | Max Stand (ML) | Median Turn (V) | MSE CI (ML) | Sit Duration | MSE CI (AP) |
| 9 | MaxJerk Stand V | MSE CI (AP) | Jerk Stand (AP) | RMS Stand (ML) | Step Time | RMS Walk (ML) |
| 10 | Stand Duration | Stand Duration | Median Turn (ML) | Step Length | Gait Speed | Gait Speed |
| 11 | CV Stride Time | PE (V) | Min Std (AP) | Std Stand (ML) | Stride Time | MSE Mean (ML) |
| 12 | CV Step Time | Median Turn (AP) | MaxJerk Stand AP | Stand Duration | RMS Stand (ML) | Step Length |
| 13 | Min Sit (ML) | Range Stand (V) | Std Sit (V) | MSE Std (AP) | Std Stand (ML) | MSE CI (ML) |
| 14 | MSE CI (V) | Std Stand (ML) | Jerk Stand (ML) | Min Stand (AP) | Std Sit (V) | Cadence |
| 15 | MSE Mean (V) | RMS Walk (V) | MaxJerk Sit (ML) | MSE CI (AP) | RMS Sit (V) | RMS Walk (V) |
| 16 | Median Turn (V) | RMS Walk (AP) | RMS Turn (V) | MSE CI (V) | MSE CI (ML) | PE (AP) |
| 17 | RMS Turn (V) | Std Stand (V) | MeanJerk Sit (ML) | MSE Mean (V) | MSE Mean (ML) | Step Time |
| 18 | RMS Walk (ML) | CV Turn (ML) | Max Stand (ML) | MSE Mean (AP) | Min Sit (ML) | Std Sit (V) |
| 19 | Max Stand (V) | MSE Mean (ML) | Range Turn (V) | Max Sit (V) | Range Sit (V) | RMS Sit (ML) |
| 20 | CV Turn (AP) | Range Sit (AP) | Max Stand (ML) | CV Turn (ML) | Std Sit (ML) | Std Sit (ML) |
| 21 | Median Turn (AP) | Gait Speed | RMS Walk (ML) | MaxJerk Stand AP | Median Turn (V) | RMS Sit (V) |
| 22 | PE (ML) | Min Stand (V) | CV Turn (AP) | Max Sit (V) | Min Stand (AP) | Sit Duration |
| 23 | Range Stand (ML) | MeanJerk Sit (AP) | RMS Sit (AP) | Range Stand (AP) | CV Stride Time | Stride Time |
| 24 | RMS Walk (V) | RMS Turn (V) | MSE CI (ML) | RMS Turn (AP) | Min Sit (V) | MaxJerk Stand AP |
| 25 | CV Turn (ML) | PE (AP) | PE (AP) | Range Stand (ML) | Range Stand AP | Range Stand ML |
| 26 | Max Stand (ML) | Step Time | Range Stand (ML) | MSE Std (ML) | CV Step Time | MSE Mean (V) |
| 27 | PE (V) | Min Std (AP) | Range Sit (V) | Range Sit (AP) | Range Stand ML | MSE CI (V) |
| 28 | Min Stand (ML) | Median Turn (ML) | Jerk Stand (V) | Jerk Stand (ML) | MSE Std (V) | Range Sit (AP) |
| 29 | Max Stand (ML) | RMS Sit (AP) | Range Stand (AP) | Jerk Stand (V) | Min Stand (ML) | Min Std (AP) |
| 30 | RMS Turn (AP) | Range Turn (ML) | Max Sit (V) | Median Turn (V) | Range Sit (ML) | MSE Std (AP) |
| Feature Name | ||||||
|---|---|---|---|---|---|---|
| Top | Relief-F | ETC | ||||
| y = SFBBS | y = TUG | y = SFBBS + TUG | y = SFBBS | y = TUG | y = SFBBS + TUG | |
| 1 | Walk Duration | MSE Mean (V) | Std Stand (ML) | Step Length | Gait Speed | Step Length |
| 2 | Gait Speed | RMS Sit (V) | Std Sit (AP) | Gait Speed | Step Length | Gait Speed |
| 3 | Step Length | MSE Std (ML) | Median Turn (AP) | Walk Duration | Walk Duration | Walk Duration |
| 4 | CV Step Time | Min Std (AP) | Min Sit (V) | CV Step Time | Cadence | MSE Std (ML) |
| 5 | CV Stride Time | RMS Walk (ML) | Range Stand (ML) | RMS Walk (ML) | MSE Std (ML) | RMS Walk ML |
| 6 | RMS Walk (ML) | CV Step Time | MSE Std (V) | CV Stride Time | MaxJerk Stand AP | Sit Duration |
| 7 | Sit Duration | PE_V | RMS Turn (AP) | MSE Std (ML) | Step Time | CV Step Time |
| 8 | Cadence | Stand Duration | Max Sit (AP) | Sit Duration | Min Stand (AP) | Cadence |
| 9 | Std Sit (AP) | Std Sit (V) | RMS Turn (V) | RMS Turn (V) | RMS Stand (ML) | Std Sit (AP) |
| 10 | Median Turn (AP) | Min Std (AP) | MSE Mean (V) | CV Turn (AP) | Jerk Sit (ML) | Stand Duration |
| 11 | Step Time | Range Sit (ML) | Max Sit (V) | Std Sit (AP) | Stride Time | CV Stride Time |
| 12 | Stride Time | MSE CI (V) | RMS Stand (V) | MaxJerk Sit (AP) | Stand Duration | Stride Time |
| 13 | Stand Duration | Min Stand (AP) | CV Turn (V) | RMS Walk (AP) | RMS Stand (AP) | Step Time |
| 14 | MaxJerk Sit (AP) | MaxJerk Sit (ML) | Gait Speed | Cadence | Range Stand (AP) | MSE Std (V) |
| 15 | RMS Turn (V) | Range Sit (V) | RMS Stand (ML) | Std Sit (V) | Std Stand (AP) | RMS Turn (V) |
| 16 | MSE Std (ML) | Median Turn (ML) | Cadence | Step Time | MSE Std (V) | Jerk Sit (AP) |
| 17 | Median Turn (V) | Sit Duration | Stand Duration | PE (AP) | Std Stand (ML) | RMS Walk (AP) |
| 18 | Range Sit (ML) | Median Turn (V) | Min Sit (ML) | Jerk Sit (AP) | MaxJerk Stand V | Jerk Stand (V) |
| 19 | RMS Walk (AP) | Step Length | MaxJerk Sit (ML) | Stride Time | Jerk stand ML | Std Sit (V) |
| 20 | Min Sit (ML) | Stride Time | Max Stand (ML) | Stand Duration | Std Sit (AP) | MSE Mean (V) |
| 21 | Std Sit (V) | MaxJerk Stand AP | RMS Sit (V) | Median Turn (AP) | MaxJerk Sit (ML) | PE (AP) |
| 22 | MaxJerk Sit (ML) | RMS Walk (AP) | Jerk Stand V | Jerk Sit (V) | RMS Walk (ML) | MSE CI (V) |
| 23 | Range Sit (AP) | Range Turn (ML) | Min Stand (ML) | Max Sit (V) | Max Stand (AP) | CV Turn (AP) |
| 24 | CV Turn (AP) | RMS Turn (V) | Step Time | Median Turn (V) | Range Turn (V) | Median Turn AP |
| 25 | Jerk Stand ML | RMS Stand (ML) | CV Turn (AP) | MSE CI (V) | RMS Sit (AP) | Jerk Sit (ML) |
| 26 | RMS Sit (V) | Median Turn (AP) | Jerk Sit (V) | MSE Mean (V) | Max Stand (ML) | Std Sit (ML) |
| 27 | Median Turn (ML) | Std Stand (ML) | Max Stand (V) | Jerk Stand (V) | Max Sit (V) | Max Sit (V) |
| 28 | MSE CI (V) | Min Sit (V) | MaxJerk Sit (AP) | MSE Std (V) | CV Turn (AP) | RMS Walk (V) |
| 29 | MSE Mean (V) | Std Sit (AP) | Range Turn (ML) | Jerk Stand ML | Min Std (AP) | Median Turn V |
| 30 | RMS Sit (AP) | MSE Std (V) | Std Sit (ML) | MaxJerk Stand AP | MSE CI (AP) | Jerk Sit (V) |
| Subjects | y | Top 5 | Top 10 | Top 15 | Top 20 | Top 25 | Top 30 | |
|---|---|---|---|---|---|---|---|---|
| Relief-F | Stroke Survivors | SFBBS | 0.789 | 0.781 | 0.781 | 0.790 | 0.785 | 0.798 |
| TUG | 0.808 | 0.855 | 0.864 | 0.967 | 0.965 | 0.956 | ||
| SFBBS + TUG | 0.609 | 0.715 | 0.805 | 0.810 | 0.835 | 0.838 | ||
| Community Dwelling Elderly | SFBBS | 0.834 | 0.820 | 0.843 | 0.824 | 0.802 | 0.810 | |
| TUG | 0.869 | 0.870 | 0.919 | 0.983 | 0.986 | 0.987 | ||
| SFBBS + TUG | 0.829 | 0.945 | 0.949 | 0.941 | 0.941 | 0.940 | ||
| ETC | Stroke Survivors | SFBBS | 0.815 | 0.834 | 0.829 | 0.838 | 0.835 | 0.849 |
| TUG | 0.990 | 0.993 | 0.994 | 0.994 | 0.995 | 0.995 | ||
| SFBBS + TUG | 0.922 | 0.927 | 0.932 | 0.932 | 0.918 | 0.931 | ||
| Community Dwelling Elderly | SFBBS | 0.850 | 0.867 | 0.870 | 0.869 | 0.870 | 0.866 | |
| TUG | 0.991 | 0.995 | 0.995 | 0.993 | 0.994 | 0.994 | ||
| SFBBS + TUG | 0.962 | 0.975 | 0.970 | 0.965 | 0.954 | 0.962 |
| Subjects | y | AUC | Precision | Recall | F1-Score | |
|---|---|---|---|---|---|---|
| Relief-F | Stroke Survivors | SFBBS | 0.798 | 0.742 | 0.716 | 0.729 |
| TUG | 0.967 | 0.787 | 0.815 | 0.801 | ||
| SFBBS + TUG | 0.838 | 0.814 | 0.795 | 0.804 | ||
| Community Dwelling Elderly | SFBBS | 0.843 | 0.761 | 0.810 | 0.785 | |
| TUG | 0.987 | 0.949 | 0.944 | 0.946 | ||
| SFBBS + TUG | 0.949 | 0.841 | 0.912 | 0.875 | ||
| ETC | Stroke Survivors | SFBBS | 0.849 | 0.794 | 0.768 | 0.781 |
| TUG | 0.995 | 0.976 | 0.969 | 0.972 | ||
| SFBBS + TUG | 0.932 | 0.854 | 0.831 | 0.842 | ||
| Community Dwelling Elderly | SFBBS | 0.870 | 0.770 | 0.811 | 0.790 | |
| TUG | 0.995 | 0.989 | 0.987 | 0.988 | ||
| SFBBS + TUG | 0.975 | 0.890 | 0.923 | 0.906 |
| SFBBS | TUG | SFBBS + TUG |
|---|---|---|
| Walk Duration | Stand Duration * | Gait Speed |
| Gait Speed | Stand Duration * | |
| Step Length | ||
| Stand Duration * | ||
| MSE-V CI | ||
| MSE-V Mean |
| SFBBS | TUG | SFBBS + TUG |
|---|---|---|
| Walk duration | Stand duration * | Walk duration |
| Gait speed | Step Length * | Sit duration |
| Step length * | Stride time | |
| CV step time | Mean sit (V) | |
| RMS walk (ML) | Stand duration * | |
| CV stride time | CV stride time | |
| Sit duration | Step Length * | |
| Std sit (AP) | ||
| RMS turn (Y) | ||
| Jerk sit (AP) | ||
| Cadence | ||
| Median turn (AP) | ||
| Stand duration * | ||
| Step time | ||
| Stride time |
| SFBBS | TUG | SFBBS + TUG |
|---|---|---|
| Walk Duration | Stand Duration | Stand Duration |
| Gait Speed | ||
| Step Length | ||
| Stand Duration |
| Subjects | Situation | BBS Mean (SD) | TUG Mean (SD) | BBS + TUG Mean (SD) |
|---|---|---|---|---|
| Stroke Survivors | Fall Risk | 4.14 (1.76) | 3.59 (1.74) | 4.58 (2.08) |
| Healthy | 1.81 (0.85) | 1.27 (0.25) | 1.27 (0.82) | |
| Community Dwelling Elderly | Fall Risk | 1.37 (0.46) | 1.70 (0.37) | 1.66 (0.32) |
| Healthy | 1.07 (0.39) | 1.00 (0.30) | 0.99 (0.39) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.-H.; Mendoza, T.; Huang, C.-H.; Sun, T.-L. Comparative Analysis of Fall Risk Assessment Features in Community-Elderly and Stroke Survivors: Insights from Sensor-Based Data. Healthcare 2023, 11, 1938. https://doi.org/10.3390/healthcare11131938
Lee C-H, Mendoza T, Huang C-H, Sun T-L. Comparative Analysis of Fall Risk Assessment Features in Community-Elderly and Stroke Survivors: Insights from Sensor-Based Data. Healthcare. 2023; 11(13):1938. https://doi.org/10.3390/healthcare11131938
Chicago/Turabian StyleLee, Chia-Hsuan, Tomas Mendoza, Chien-Hua Huang, and Tien-Lung Sun. 2023. "Comparative Analysis of Fall Risk Assessment Features in Community-Elderly and Stroke Survivors: Insights from Sensor-Based Data" Healthcare 11, no. 13: 1938. https://doi.org/10.3390/healthcare11131938