
Latent Subtype of Cognitive Frailty among Multimorbidity Older Adults and Their Association with Social Relationships
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Measures
2.3.1. Cognitive Frailty Indicators
2.3.2. Social Relationships
2.3.3. Covariables
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. World Population Ageing 2019: Highlights. 2019. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf (accessed on 28 March 2022).
- World Health Organization. Multimorbidity: Technical Series on Safer Primary Care; WHO: Geneva, Switzerland, 2016; Available online: https://apps.who.int/iris/bitstream/handle/10665/252275/9789241511650-eng.pdf (accessed on 14 September 2020).
- Fortin, M.; Haggerty, J.; Almirall, J.; Bouhali, T.; Sasseville, M.; Lemieux, M. Lifestyle factors and multimorbidity: A cross sectional study. BMC Public Health 2014, 14, 686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiao, D.; Watanabe, K.; Sawada, Y.; Tanaka, E.; Watanabe, T.; Tomisaki, E.; Ito, S.; Okumura, R.; Kawasaki, Y.; Anme, T. Multimorbidity and functional limitation: The role of social relationships. Arch. Gerontol. Geriatr. 2021, 92, 104249. [Google Scholar] [CrossRef]
- Lange-Maia, B.S.; Karvonen-Gutierrez, C.A.; Kazlauskaite, R.; Strotmeyer, E.S.; Karavolos, K.; Appelhans, B.M.; Janssen, I.; Avery, E.F.; Dugan, S.A.; Kravitz, H.M. Impact of Chronic Medical Condition Development on Longitudinal Physical Function from Mid- to Early Late-Life: The Study of Women’s Health Across the Nation. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1411–1417. [Google Scholar] [CrossRef] [PubMed]
- Quiñones, A.R.; Markwardt, S.; Botoseneanu, A. Multimorbidity combinations and disability in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 823–830. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, T.P.; Wagner, K.J.P.; Schneider, I.J.C.; Danielewicz, A.L. Multimorbidity patterns and functional disability in elderly Brazilians: A cross-sectional study with data from the Brazilian National Health Survey. Cad. Saúde Pública 2020, 36, e00241619. [Google Scholar] [CrossRef]
- Williams, J.S.; Egede, L.E. The association between multimorbidity and quality of life, health status and functional disability. Am. J. Med. Sci. 2016, 352, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.; Wu, Y.T.; Dregan, A.; Vitoratou, S.; Chua, K.C.; Prina, A.M. Multimorbidity patterns, all-cause mortality and healthy aging in older English adults: Results from the English Longitudinal Study of Aging. Geriatr. Gerontol. Int. 2020, 20, 1126–1132. [Google Scholar] [CrossRef]
- Wei, M.Y.; Levine, D.A.; Zahodne, L.B.; Kabeto, M.U.; Langa, K.M. Multimorbidity and cognitive decline over 14 years in older Americans. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1206–1213. [Google Scholar] [CrossRef]
- Koyanagi, A.; Smith, L.; Shin, J.I.; Oh, H.; Kostev, K.; Jacob, L.; Abduljabbar, A.S.; Haro, J.M. Multimorbidity and Subjective Cognitive Complaints: Findings from 48 Low- and Middle-Income Countries of the World Health Survey 2002–2004. J. Alzheimer’s Dis. 2021, 81, 1737–1747. [Google Scholar] [CrossRef]
- Kao, S.L.; Wang, J.H.; Chen, S.C.; Li, Y.Y.; Yang, Y.L.; Lo, R.Y. Impact of Comorbidity Burden on Cognitive Decline: A Prospective Cohort Study of Older Adults with Dementia. Dement. Geriatr. Cogn. Disord. 2021, 50, 43–50. [Google Scholar] [CrossRef]
- Lee, Y.; Cho, C.C. Examining the effects of multiple chronic conditions on cognitive decline and potential moderators among older Koreans: Findings from the Korean Longitudinal Study of Ageing 2006–2016. Arch. Gerontol. Geriatr. 2021, 95, 104424. [Google Scholar] [CrossRef] [PubMed]
- Jacob, L.; Haro, J.M.; Koyanagi, A. Physical Multimorbidity and Subjective Cognitive Complaints among Adults in the United Kingdom: A Cross-sectional Community-based Study. Sci Rep. 2019, 9, 12417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, N.L.; Bhargava, S.; Brown, M.J.; Kim, H.; Bhang, I.; Mullin, K.; Phillips, K.; Mogle, J. Cognitive complaints in age-related chronic conditions: A systematic review. PLoS ONE 2021, 16, e0253795. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Morris, J.C.; Berg-Weger, M.; Borson, S.; Carpenter, B.D.; Del Campo, N.; Dubois, B.; Fargo, K.; Fitten, L.J.; Flaherty, J.H.; et al. Brain health: The importance of recognizing cognitive impairment: An IAGG consensus conference. J. Am. Med. Dir. Assoc. 2015, 16, 731–739. [Google Scholar] [CrossRef] [Green Version]
- Sugimoto, T.; Arai, H.; Sakurai, T. An update on cognitive frailty: Its definition, impact, associated factors and underlying mechanisms, and interventions. Geriatr. Gerontol. Int. 2021, 22, 99–109. [Google Scholar] [CrossRef]
- Das, S. Cognitive frailty among community-dwelling rural elderly population of West Bengal in India. Asian J. Psychiatry 2022, 70, 103025. [Google Scholar] [CrossRef]
- Qiu, Y.; Li, G.; Wang, X.; Zheng, L.; Wang, C.; Wang, C.; Chen, L. Prevalence of cognitive frailty among community-dwelling older adults: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2022, 125, 104112. [Google Scholar] [CrossRef]
- Tsutsumimoto, K.; Doi, T.; Makizako, H.; Hotta, R.; Nakakubo, S.; Makino, K.; Suzuki, T.; Shimada, H. Cognitive frailty is associated with fall-related fracture among older people. J. Nutr. Health Aging 2018, 22, 1216–1220. [Google Scholar] [CrossRef]
- Chen, C.; Park, J.; Wu, C.; Xue, Q.; Agogo, G.; Han, L.; Hoogendijk, E.O.; Liu, Z.; Wu, Z. Cognitive frailty in relation to adverse health outcomes independent of multimorbidity: Results from the China health and retirement longitudinal study. Aging 2020, 12, 23129–23145. [Google Scholar] [CrossRef]
- Lee, W.J.; Peng, L.N.; Liang, C.K.; Loh, C.H.; Chen, L.K. Cognitive frailty predicting all-cause mortality among community-living older adults in Taiwan: A 4-year nationwide population-based cohort study. PLoS ONE 2018, 13, e0200447. [Google Scholar] [CrossRef] [Green Version]
- Malek Rivan, N.F.; Shahar, S.; Rajab, N.F.; Singh, D.K.A.; Din, N.C.; Hazlina, M.; Hamid, T.A.T.A. Cognitive frailty among Malaysian older adults: Baseline findings from the LRGS TUA cohort study. Clin. Interv. Aging 2019, 14, 1343–1352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, W.M.; Tange, C.; Nishita, Y.; Tomida, M.; Shimokata, H.; Otsuka, R.; Lee, M.C.; Arai, H. Effect of different types of social support on physical frailty development among community-dwelling older adults in Japan: Evidence from a 10-year population-based cohort study. Arch. Gerontol. Geriatr. 2023, 108, 104928. [Google Scholar] [CrossRef] [PubMed]
- Ye, B.; Chen, H.; Huang, L.; Ruan, Y.; Qi, S.; Guo, Y.; Huang, Z.; Sun, S.; Chen, X.; Shi, Y.; et al. Changes in frailty among community-dwelling Chinese older adults and its predictors: Evidence from a two-year longitudinal study. BMC Geriatr. 2020, 20, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.; Shin, H.E.; Kim, M.; Won, C.W.; Song, Y.M. Longitudinal association between eating alone and deterioration in frailty status: The Korean Frailty and Aging Cohort Study. Exp. Gerontol. 2023, 172, 112078. [Google Scholar] [CrossRef]
- Wang, Y.; Li, J.; Fu, P.; Jing, Z.; Zhao, D.; Zhou, C. Social support and subsequent cognitive frailty during a 1-year follow-up of older people: The mediating role of psychological distress. BMC Geriatr. 2022, 22, 162. [Google Scholar] [CrossRef]
- Muthén, B.; Muthén, L.K. Integrating person-centered and variable-centered analyses: Growth mixture modeling with latent trajectory classes. Alcohol Clin. Exp. Res. 2000, 24, 882–891. [Google Scholar] [CrossRef]
- Majnarić, L.T.; Bekić, S.; Babič, F.; Pusztová, Ľ.; Paralič, J. Cluster analysis of the associations among physical frailty, cognitive impairment and mental disorders. Med. Sci. Monit. 2020, 26, e924281. [Google Scholar] [CrossRef]
- Fukutomi, E.; Okumiya, K.; Wada, T.; Sakamoto, R.; Ishimoto, Y.; Kimura, Y.; Kasahara, Y.; Chen, W.L.; Imai, H.; Fujisawa, M.; et al. Importance of cognitive assessment as part of the “Kihon Checklist” developed by the Japanese Ministry of Health, Labor and Welfare for prediction of frailty at a 2-year follow up. Geriatr. Gerontol. Int. 2013, 13, 654–662. [Google Scholar] [CrossRef]
- Anme, T. Evaluation of environmental stimulation and its relation to physical deterioration in the elderly after 3 years--A health-social longitudinal study. Nihon Koshu Eisei Zasshi 1997, 44, 159–166. [Google Scholar]
- Muthén, B.; Asparouhov, T. Latent variable analysis with categorical outcomes: Multiple-group and growth modeling in Mplus. Mplus Web Notes 2002, 4, 1–22. [Google Scholar]
- Cheng, G.H.L.; Sung, P.; Chan, A.; Ma, S.; Malhotra, R. Transitions between social network profiles and their relation with all-cause mortality among older adults. Soc. Sci. Med. 2022, 292, 114617. [Google Scholar] [CrossRef] [PubMed]
- Collins, L.M.; Lanza, S.T. Latent Class and Latent Transition Analysis: With Applications in the Social, Behavioral, and Health Sciences; John Wiley and Sons Inc.: New York, NY, USA, 2010. [Google Scholar] [CrossRef]
- Shen, Z.; Ruan, Q.; Yu, Z.; Sun, Z. Chronic kidney disease-related physical frailty and cognitive impairment: A systemic review. Geriatr. Gerontol. Int. 2016, 17, 529–544. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Yamasaki, S.; Higuchi, S.; Kamiya, K.; Saito, H.; Saito, K.; Ogasahara, Y.; Maekawa, E.; Konishi, M.; Kitai, T.; et al. Prevalence and prognostic impact of cognitive frailty in elderly patients with heart failure: Sub-analysis of FRAGILE-HF. ESC Heart Fail. 2022, 9, 1574–1583. [Google Scholar] [CrossRef]
- Kim, H.; Awata, S.; Watanabe, Y.; Kojima, N.; Osuka, Y.; Motokawa, K.; Sakuma, N.; Inagaki, H.; Edahiro, A.; Hosoi, E.; et al. Cognitive frailty in community-dwelling older Japanese people: Prevalence and its association with falls. Geriatr. Gerontol. Int. 2019, 19, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Xie, B.; Ma, C.; Chen, Y.; Wang, J. Prevalence and risk factors of the co-occurrence of physical frailty and cognitive impairment in Chinese community-dwelling older adults. Health Soc. Care Community 2021, 29, 294–303. [Google Scholar] [CrossRef]
- Bekić, S.; Babič, F.; Pavlišková, V.; Paralič, J.; Wittlinger, T.; Majnarić, L.T. Clusters of physical frailty and cognitive impairment and their associated comorbidities in older primary care patients. Healthcare 2021, 9, 891. [Google Scholar] [CrossRef]
- Kelly, M.E.; Duff, H.; Kelly, S.; McHugh Power, J.E.; Brennan, S.; Lawlor, B.A.; Loughrey, D.G. The impact of social activities, social networks, social support and social relationships on the cognitive functioning of healthy older adults: A systematic review. Syst. Rev. 2017, 6, 259. [Google Scholar] [CrossRef]
- Wang, C.; Zhang, J.; Hu, C.; Wang, Y. Prevalence and Risk Factors for Cognitive Frailty in Aging Hypertensive Patients in China. Brain Sci. 2021, 11, 1018. [Google Scholar] [CrossRef]
- Vetrano, D.L.; Palmer, K.; Marengoni, A.; Marzetti, E.; Lattanzio, F.; Roller-Wirnsberger, R.; Lopez Samaniego, L.; Rodríguez-Mañas, L.; Bernabei, R.; Onder, G.; et al. Frailty and multimorbidity: A systematic review and meta-analysis. J. Gerontol. Ser. A 2019, 74, 659–666. [Google Scholar] [CrossRef] [Green Version]
- Facal, D.; Maseda, A.; Pereiro, A.X.; Gandoy-Crego, M.; Lorenzo-López, L.; Yanguas, J.; Millán-Calenti, J.C. Cognitive frailty: A conceptual systematic review and an operational proposal for future research. Maturitas 2019, 121, 48–56. [Google Scholar] [CrossRef]
- Berkman, F.L.; Kawachi, I.; Glymour, M.M. Social Epidemiology, 2nd ed.; Oxford University Press: New York, NY, USA, 2014. [Google Scholar]
- Asparouhov, T.; Muthén, B. Auxiliary variables in mixture modeling: Three-step approaches using Mplus. Struct. Equ. Model. 2014, 21, 329–341. [Google Scholar] [CrossRef]


{kind=link}
| Items | Categories | n | % |
|---|---|---|---|
| Age | Mean (±SD) | 75.8 ± 7.3 | |
| Missing | 0 | 0.0 | |
| Sex | Male | 193 | 48.7 |
| Female | 203 | 51.3 | |
| Missing | 0 | 0.0 | |
| Living status | Alone | 23 | 5.8 |
| Not alone | 341 | 86.1 | |
| Missing | 32 | 8.1 | |
| Drinking/Smoking | Yes | 139 | 35.1 |
| No | 249 | 62.9 | |
| Missing | 8 | 2 | |
| Long term care | Need | 88 | 22.2 |
| No need | 308 | 77.8 | |
| Missing | 0 | 0.0 | |
| Exercise | Doing | 212 | 53.5 |
| Not doing | 150 | 37.9 | |
| Missing | 34 | 8.6 | |
| Chronic disease | Mean (±SD) | 2.6 ± 0.8 | |
| Missing | 0 | 0.0 | |
| ISI | Mean (±SD) | 16.3 (± 2.2) | |
| Missing | 29 | 7.3 | |
| Models | AIC | BIC | ABIC | Entropy | LMR | BLRT |
|---|---|---|---|---|---|---|
| Class 1 | 3451.665 | 3483.516 | 3458.132 | |||
| Class 2 | 3077.052 | 3144.737 | 3090.795 | 0.871 | <0.001 | <0.001 |
| Class 3 | 3029.740 | 3133.311 | 3050.812 | 0.683 | <0.001 | <0.001 |
| Class 4 | 3028.503 | 3167.852 | 3056.797 | 0.726 | 0.046 | 0.192 |
| Class 5 | 3024.62 | 3199.802 | 3060.190 | 0.765 | 0.121 | 0.136 |
| Class 6 | 3027.678 | 3238.693 | 3070.523 | 0.754 | 0.582 | 1.000 |
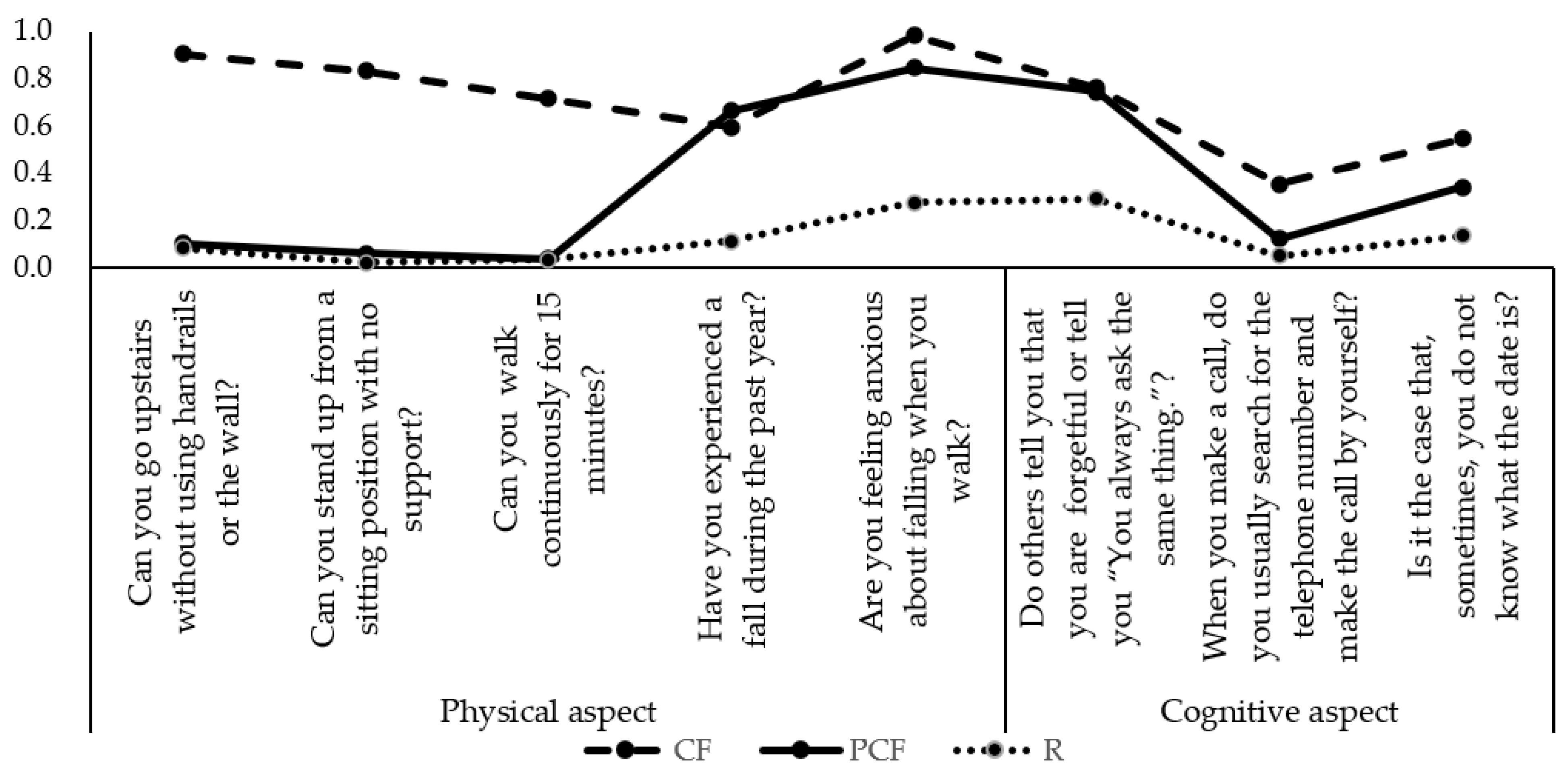
| Items | Class 1 CF | Class 2 PCF | Class 3 R |
|---|---|---|---|
| Can you go upstairs without using handrails or the wall? | 0.906 | 0.103 | 0.084 |
| Can you stand up from a sitting position with no support? | 0.835 | 0.061 | 0.022 |
| Can you walk continuously for 15 min? | 0.715 | 0.038 | 0.033 |
| Have you experienced a fall during the past year? | 0.594 | 0.663 | 0.114 |
| Are you feeling anxious about falling when you walk? | 0.983 | 0.848 | 0.275 |
| Do others tell you that you are forgetful or tell you that “You always ask the same thing”? | 0.763 | 0.745 | 0.292 |
| When you make a call, do you usually search for the telephone number and make the call by yourself? | 0.353 | 0.122 | 0.051 |
| Is it the case that, sometimes, you do not know what the date is? | 0.548 | 0.342 | 0.135 |
| Items | Categories | Class 3: R (n = 166) | Class 2: PCF (n = 153) | Class 1: CF (n = 77) | z/χ² | p | |||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||||
| Age | Mean (±SD) | 73.0 (±6.1) | 75.5 (±7.4) | 82.9 (±7.2) | 68.573 | <0.001 | |||
| Sex | Male | 95 | 57.2 | 73 | 47.7 | 25 | 32.5 | 13.013 | <0.001 |
| Female | 71 | 42.8 | 80 | 52.3 | 52 | 67.5 | |||
| Drinking or Smoking | Yes | 71 | 43.3 | 59 | 39.9 | 9 | 11.8 | 24.042 | <0.001 |
| No | 93 | 56.7 | 89 | 60.1 | 67 | 88.2 | |||
| Long-term care need | Need | 10 | 6 | 29 | 19 | 49 | 63.6 | 102.554 | <0.001 |
| No need | 156 | 94 | 124 | 81 | 28 | 36.4 | |||
| Exercise | Doing | 109 | 70.3 | 80 | 57.6 | 23 | 33.8 | 26.042 | <0.001 |
| Not doing | 46 | 29.7 | 59 | 42.4 | 45 | 66.2 | |||
| Living status | Alone | 6 | 3.9 | 12 | 8.6 | 5 | 6.8 | 2.736 | 0.255 |
| Not alone | 146 | 96.1 | 127 | 91.4 | 68 | 93.2 | |||
| Chronic disease | Mean (±SD) | 2.4 (±0.7) | 2.6 (±0.8) | 2.8 (±1.0) | 13.848 | <0.001 | |||
| ISI | Mean (±SD) | 16.9 (±1.5) | 16.5 (±2.0) | 14.6 (±2.7) | 56.224 | <0.001 | |||
| Items | Category | Class 2: PCF | Class 3: R | ||||
|---|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | ||
| ISI | 1.28 | 1.08–1.57 | 0.004 | 1.40 | 1.15–1.70 | <0.001 | |
| Age | 0.93 | 0.88–0.95 | 0.020 | 0.89 | 0.83–0.94 | <0.001 | |
| Sex | Male | 3.34 | 1.40–7.98 | 0.007 | 6.11 | 2.41–15.45 | <0.001 |
| Female | Ref. | ||||||
| Drinking or Smoking | No | 0.36 | 0.12–1.04 | 0.059 | 0.28 | 0.07–1.19 | 0.086 |
| Yes | Ref. | ||||||
| Exercise | Do | 2.78 | 1.25–6.25 | 0.013 | 4.76 | 2.02–12.50 | <0.001 |
| Do not | Ref. | ||||||
| Long-term care | No need | 5.91 | 2.49–14.03 | <0.001 | 14.61 | 5.20–41.11 | <0.001 |
| Need | Ref. | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiao, D.; Li, X.; Zhu, Z.; Zhang, J.; Liu, Y.; Cui, M.; Matsumoto, M.; Banu, A.A.; Sawada, Y.; Watanabe, T.; et al. Latent Subtype of Cognitive Frailty among Multimorbidity Older Adults and Their Association with Social Relationships. Healthcare 2023, 11, 1933. https://doi.org/10.3390/healthcare11131933
Jiao D, Li X, Zhu Z, Zhang J, Liu Y, Cui M, Matsumoto M, Banu AA, Sawada Y, Watanabe T, et al. Latent Subtype of Cognitive Frailty among Multimorbidity Older Adults and Their Association with Social Relationships. Healthcare. 2023; 11(13):1933. https://doi.org/10.3390/healthcare11131933
Chicago/Turabian StyleJiao, Dandan, Xiang Li, Zhu Zhu, Jinrui Zhang, Yang Liu, Mingyu Cui, Munenori Matsumoto, Alpona Afsari Banu, Yuko Sawada, Taeko Watanabe, and et al. 2023. "Latent Subtype of Cognitive Frailty among Multimorbidity Older Adults and Their Association with Social Relationships" Healthcare 11, no. 13: 1933. https://doi.org/10.3390/healthcare11131933