
Type 2 Diabetes Patients’ Views of Local Pharmacists and Fulfilment with Pharmaceutical Diabetes Care in Syria’s Latakia Governorate: An Online Survey Research



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Survey
2.3. Development of the Questionnaire
2.4. Study Participants
2.5. Ethical Approval
2.6. Data Collection and Analysis
3. Results
3.1. Characteristics of the Respondents
3.2. Evaluation of Patients’ Adherence to Prescribed Medications
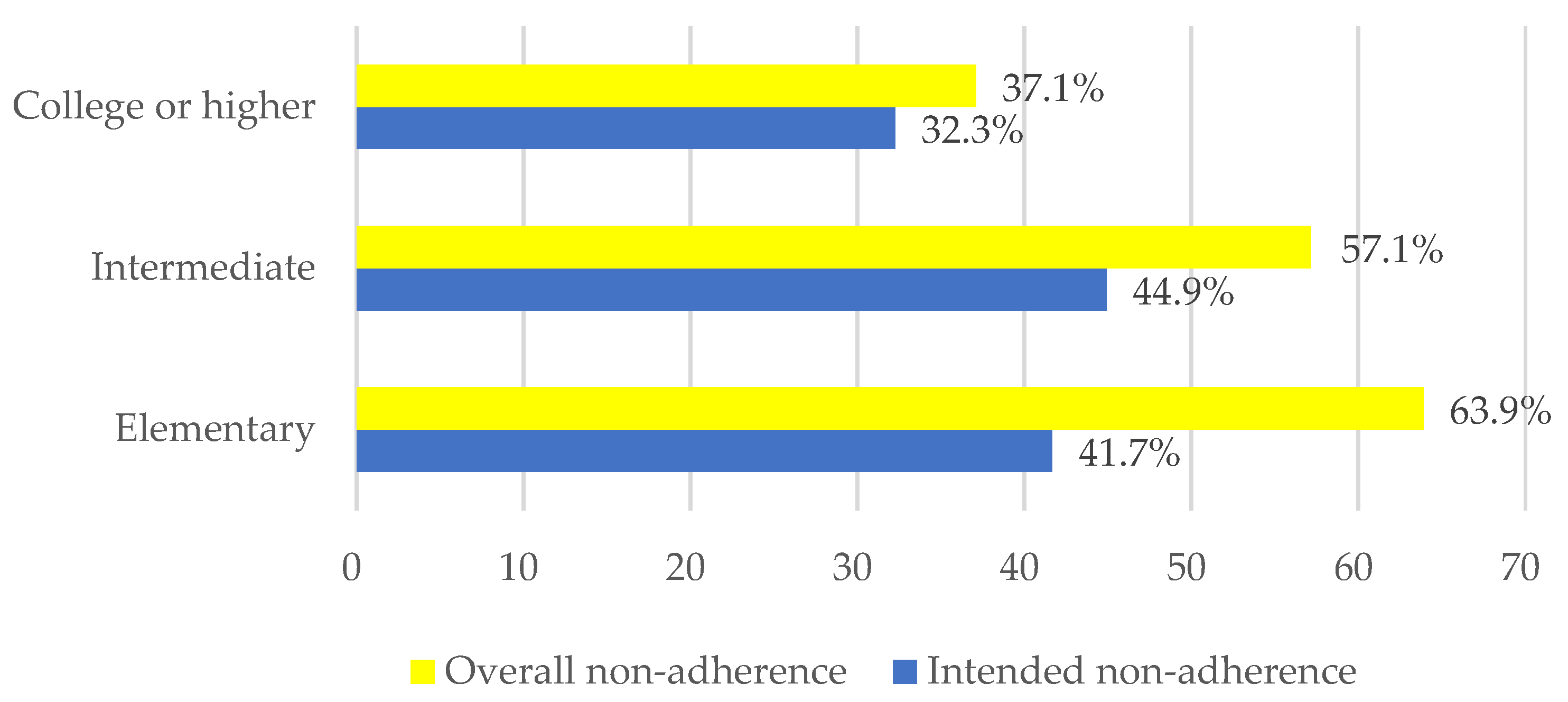
3.3. Percentage of Non-Adherent Patients Depends on Educational Level
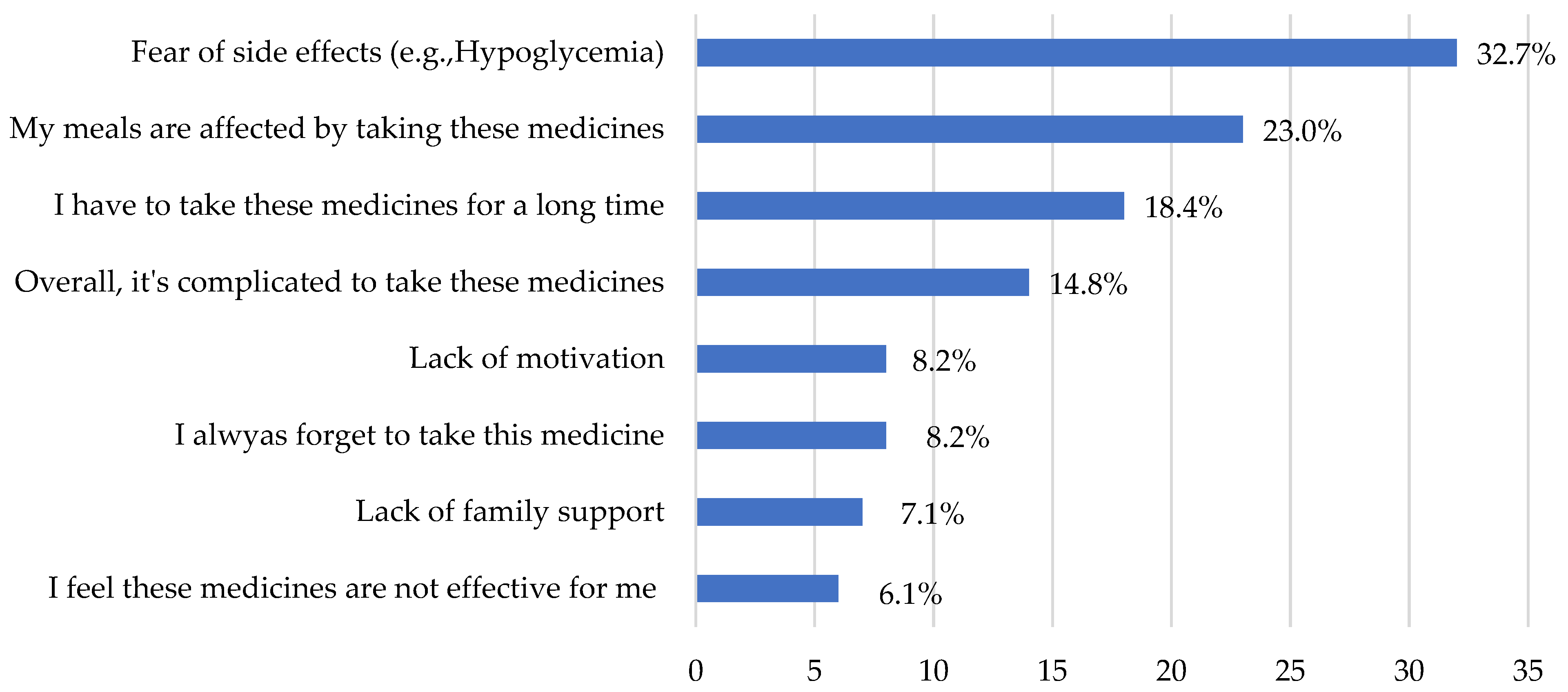
3.4. Reasons of Not Taking the Medications as Recommended from Health Provider
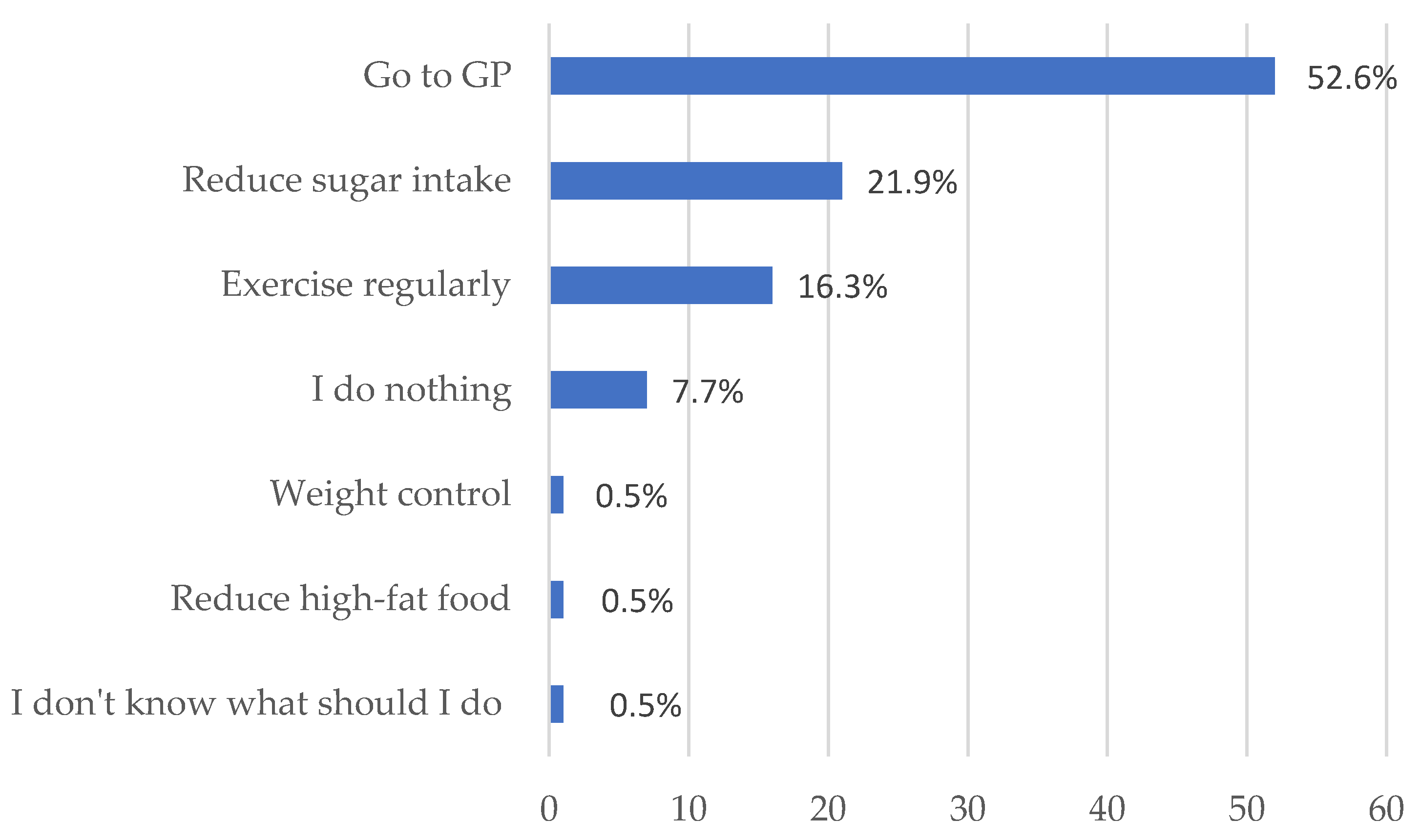
3.5. Concern
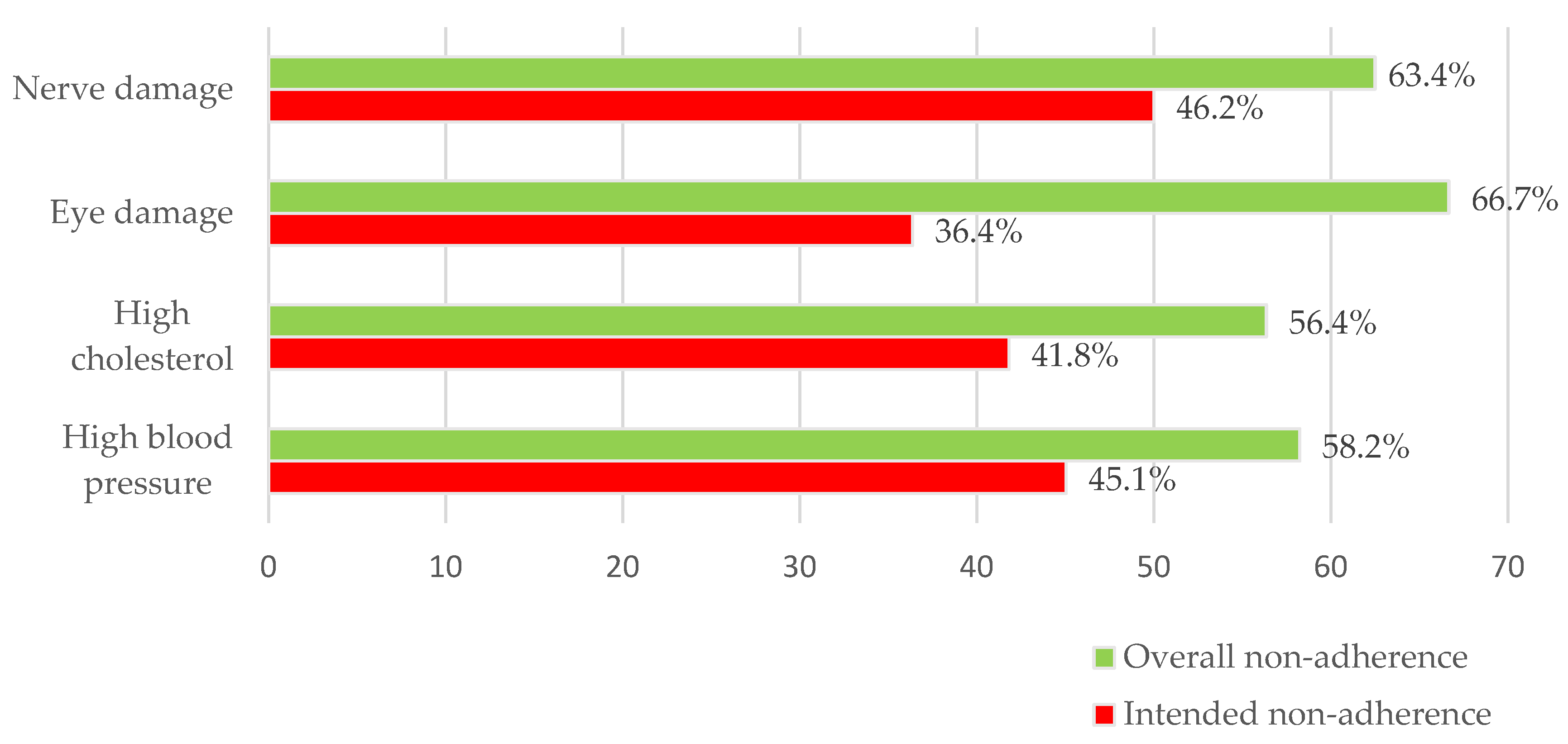
3.6. Percentage of Non-Adherence in Certain Complication
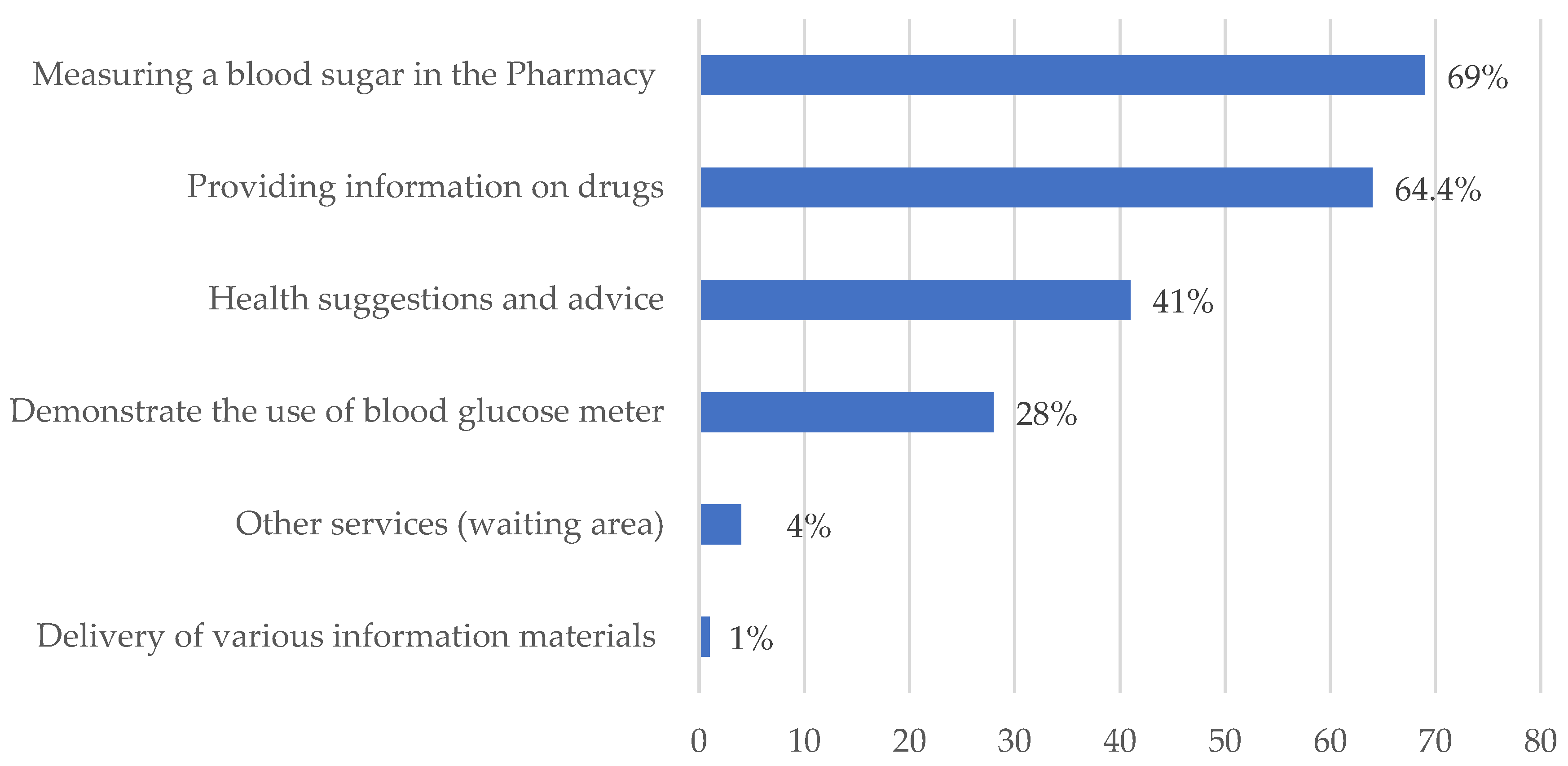
3.7. Views of Patients Regarding the Accessibility and Skill of Services Provided by Local Pharmacists
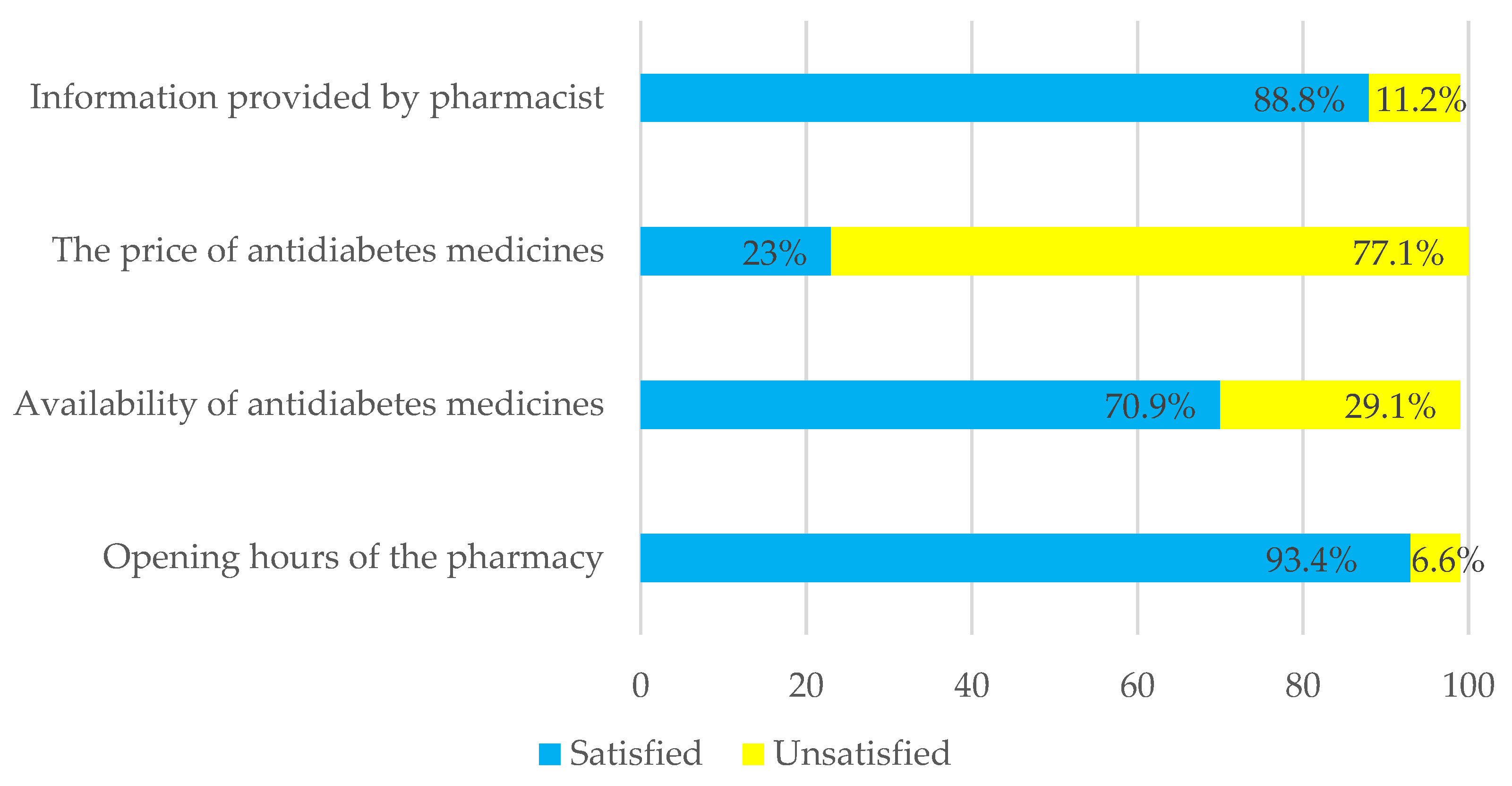
3.8. Percentage of the Overall Population Satisfaction with the Services Provided by Their Local Pharmacy
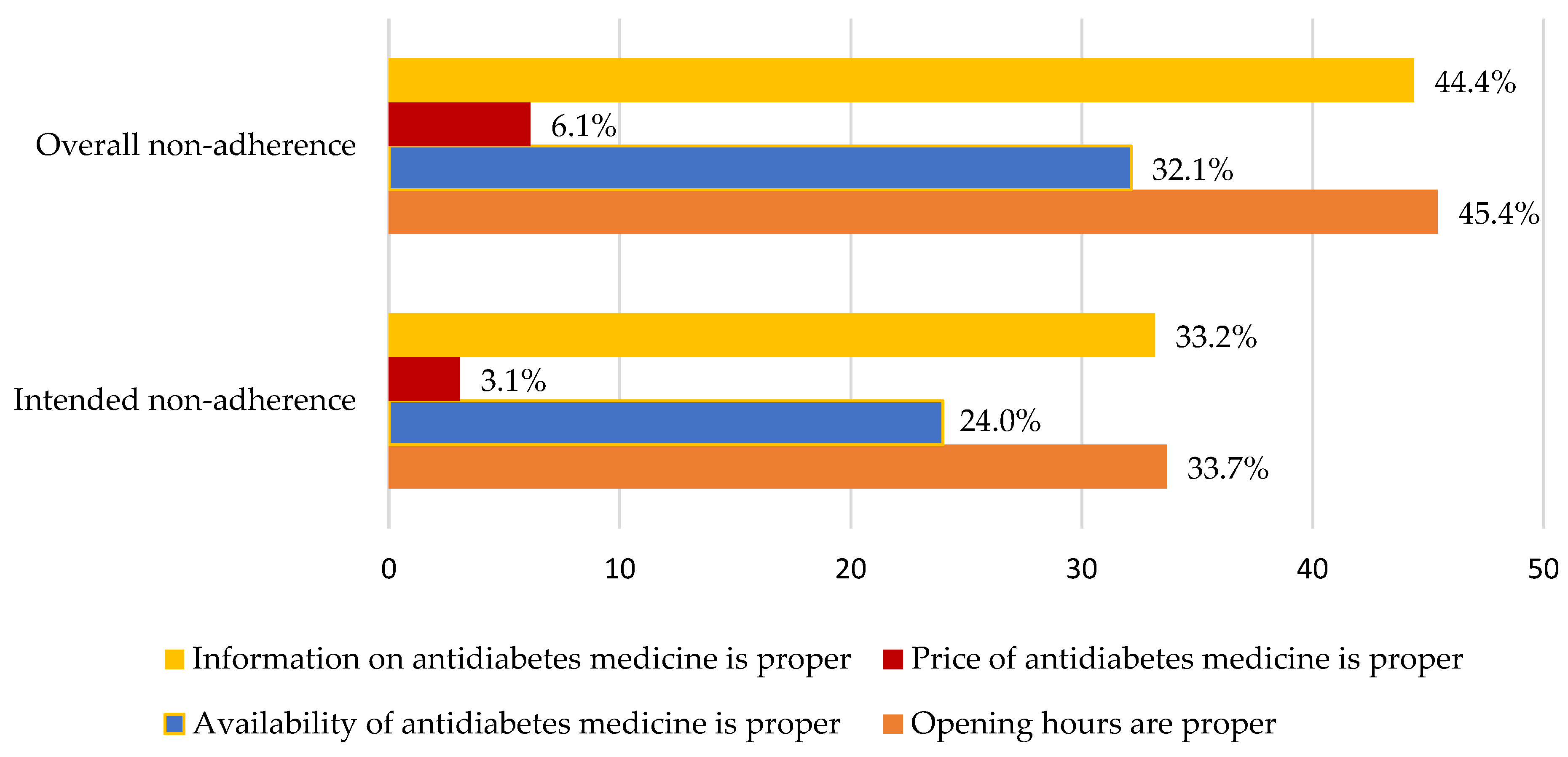
3.9. Percentage of Non-Adherent Patients’ Satisfaction with the Services Provided by Community Pharmacist
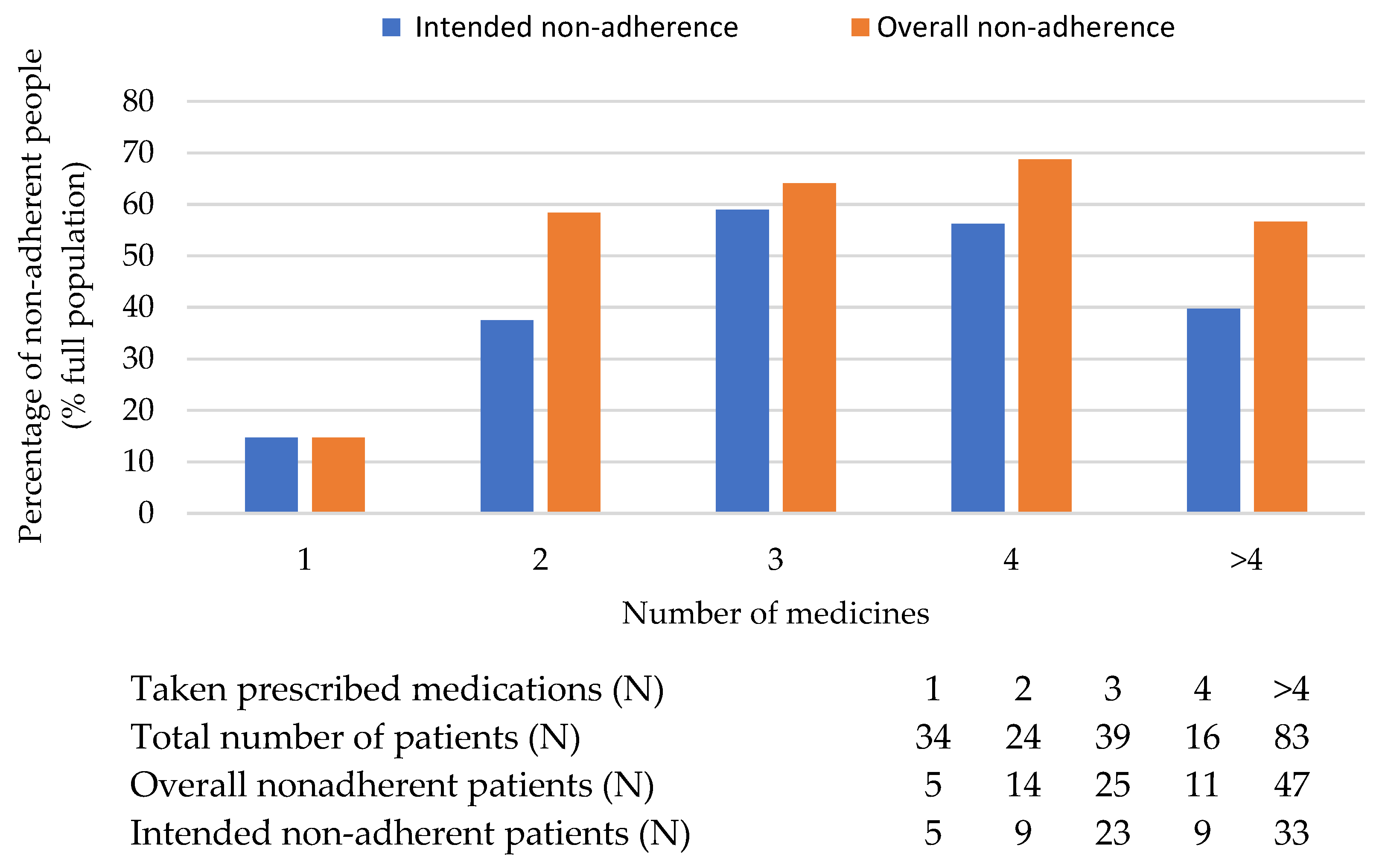
3.10. The Relationship between the Complexity of the Treatments and Patients’ Adherence
4. Discussion
Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association. Standards of medical care in diabetes—2013. Diabetes Care 2013, 36, S11–S66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrivastava, S.R.; Shrivastava, P.S.; Ramasamy, J. Role of self-care in management of diabetes mellitus. J. Diabetes Metab. Disord. 2013, 12, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tripathi, B.K.; Srivastava, A.K. Diabetes mellitus: Complications and therapeutics. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2006, 12, Ra130–Ra147. [Google Scholar]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- Al Busaidi, N.; Shanmugam, P.; Manoharan, D. Diabetes in the Middle East: Government Health Care Policies and Strategies that Address the Growing Diabetes Prevalence in the Middle East. Curr. Diabetes Rep. 2019, 19, 8. [Google Scholar] [CrossRef]
- IDF Diabetes Atlas 10th Edition Scientific Committee. IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar]
- El-Kebbi, I.M.; Bidikian, N.H.; Hneiny, L.; Nasrallah, M.P. Epidemiology of type 2 diabetes in the Middle East and North Africa: Challenges and call for action. World J. Diabetes 2021, 12, 1401–1425. [Google Scholar] [CrossRef]
- Sahloul, L.; Bouri, F.; Bsso, E.; Saleh, A.; Darwish, E.; Yaseen, L.; Mustafa, A.M.; Hatahet, T. Risk assessment of the continuity of essential medications for low socioeconomic patients in Syria: A case study of diabetes mellitus. J. Pharm. Health Serv. Res. 2022, 13, 364–369. [Google Scholar] [CrossRef]
- Murphy, A.; Biringanine, M.; Roberts, B.; Stringer, B.; Perel, P.; Jobanputra, K. Diabetes care in a complex humanitarian emergency setting: A qualitative evaluation. BMC Health Serv. Res. 2017, 17, 431. [Google Scholar] [CrossRef] [Green Version]
- Sen, K.; al Faisal, W. Syria neoliberal reforms in health sector financing: Embedding unequal access? Soc. Med. 2012, 6, 171–182. [Google Scholar]
- Detlef, S. Towards a National Health Insurance System in Syria: Documents, Materials and Excerpts; Ministry of Health: Damascus, Syria, 2003. [Google Scholar]
- Aljadeeah, S.; Nagel, E.; Wirtz, V.J. Outpatient cardiovascular diseases and diabetes medicines dispensing in the population with government health insurance in Syria between 2018 and 2019: A retrospective analysis. BMC Health Serv. Res. 2021, 21, 1088. [Google Scholar] [CrossRef]
- Khan, Y.; Albache, N.; Almasri, I.; Gabbay, R.A. The Management of Diabetes in Conflict Settings: Focus on the Syrian Crisis. Diabetes Spectr. A Publ. Am. Diabetes Assoc. 2019, 32, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.D.; Wibowo, Y.; Sunderland, B.; Hoti, K. The role of the pharmacist in the management of type 2 diabetes: Current insights and future directions. Integr. Pharm. Res. Pract. 2017, 6, 15–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nau, D.P.; Ponte, C.D. Effects of a Community Pharmacist-Based Diabetes Patient-Management Program on Intermediate Clinical Outcome Measures. J. Manag. Care Pharm. 2015, 8, 48–53. [Google Scholar] [CrossRef] [Green Version]
- Patwardhan, A.; Duncan, I.; Murphy, P.; Pegus, C. The value of pharmacists in health care. Popul. Health Manag. 2012, 15, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Firkus, D.; McCoy, R.G.; Matulis, J., III; Kessler, M.; Mara, K.; Herges, J. Evaluation of pharmacist consults within a collaborative enhanced primary care team model to improve diabetes care. PLoS ONE 2023, 18, e0280654. [Google Scholar] [CrossRef] [PubMed]
- Mouhtadi, B.B.; Alame, M.M.; Malaeb, B.; Hallit, S. Physician-community pharmacist collaborative care in diabetes management: A pilot study. J. Drug Assess. 2018, 7, 61–65. [Google Scholar] [CrossRef] [Green Version]
- Pinto, S.L.; Lively, B.T.; Siganga, W.; Holiday-Goodman, M.; Kamm, G. Using the Health Belief Model to test factors affecting patient retention in diabetes-related pharmaceutical care services. Res. Soc. Adm. Pharm. 2006, 2, 38–58. [Google Scholar] [CrossRef]
- Brewster, S.; Holt, R.; Portlock, J.; Price, H. The role of community pharmacists and their position in the delivery of diabetes care: An update for medical professionals. Postgrad. Med. J. 2020, 96, 473–479. [Google Scholar] [CrossRef]
- Al Assaf, S.; Zelko, R.; Hanko, B. The Effect of Interventions Led by Community Pharmacists in Primary Care for Adults with Type 2 Diabetes Mellitus on Therapeutic Adherence and HbA1c Levels: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 6188. [Google Scholar] [CrossRef]
- Cooney, E.; O’Riordan, D.; McSharry, J. Pharmacists’ perceived role in supporting diabetes education and self-management in Ireland: A qualitative study. HRB Open Res. 2021, 4, 20. [Google Scholar] [CrossRef]
- Katangwe, T.; Family, H.; Sokhi, J. The community pharmacy setting for diabetes prevention: Views and perceptions of stakeholders. PLoS ONE 2019, 14, e0219686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Regina, R.; Pandolfi, D.; Stabile, N.; Beloni, L.; Glisenti, F.; Griggio, P.; La Regina, M.; La Regina, G. A New Case Manager for Diabetic Patients: A Pilot Observational Study of the Role of Community Pharmacists and Pharmacy Services in the Case Management of Diabetic Patients. Pharmacy 2020, 8, 193. [Google Scholar] [CrossRef]
- Bouchaud, L.; Bluze, E.; Dussart, C.; Massoubre, B.; Boulliat, C. The role of the community and hospital pharmacist in public health prevention in France. Ann. Pharm. Fr. 2022, 80, 769–777. [Google Scholar] [CrossRef]
- Chiara, A. The Expanding Role of Pharmacists: A Positive Shift for Health Care; University of Massachusetts Medical School: Worcester, MA, USA, 2019. [Google Scholar]
- Petrelli, F.; Tiffi, F.; Scuri, S.; Nguyen, C.T.T.; Grappasonni, I. The pharmacist’s role in health information, vaccination and health promotion. Ann. Di Ig. Med. Prev. E Di Comunita 2019, 31, 309–315. [Google Scholar] [CrossRef]
- Prudencio, J.; Cutler, T.; Roberts, S.; Marin, S.; Wilson, M. The Effect of Clinical Pharmacist-Led Comprehensive Medication Management on Chronic Disease State Goal Attainment in a Patient-Centered Medical Home. J. Manag. Care Spec. Pharm. 2018, 24, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez de Bittner, M.; Chirikov, V.V.; Breunig, I.M.; Zaghab, R.W.; Shaya, F.T. Clinical effectiveness and cost savings in diabetes care, supported by pharmacist counselling. J. Am. Pharm. Assoc. 2017, 57, 102–108.e104. [Google Scholar] [CrossRef]
- Steeb, D.R.; Joyner, P.U.; Thakker, D.R. Exploring the role of the pharmacist in global health. J. Am. Pharm. Assoc. 2014, 54, 552–555. [Google Scholar] [CrossRef]
- Chevalier, B.A.M.; Watson, B.M.; Barras, M.A.; Cottrell, W.N. Investigating strategies used by hospital pharmacists to effectively communicate with patients during medication counselling. Health Expect. 2017, 20, 1121–1132. [Google Scholar] [CrossRef]
- Okada, H.; Onda, M.; Shoji, M.; Kotani, K.; Nakayama, T.; Nakagawa, Y.; Sakane, N. Effects of lifestyle intervention performed by community pharmacists on glycemic control in patients with type 2 diabetes: The community pharmacists assist (compass) project, a pragmatic cluster randomized trial. Pharmacol. Pharm. 2016, 7, 124–132. [Google Scholar] [CrossRef] [Green Version]
- Al-Arifi, M.N. Patients’ perception, views and satisfaction with pharmacists’ role as health care provider in community pharmacy setting at Riyadh, Saudi Arabia. Saudi Pharm. J. SPJ Off. Publ. Saudi Pharm. Soc. 2012, 20, 323–330. [Google Scholar] [CrossRef] [Green Version]
- Awad, A.I.; Al-Rasheedi, A.; Lemay, J. Public Perceptions, Expectations, and Views of Community Pharmacy Practice in Kuwait. Med. Princ. Pract. 2017, 26, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Bawab, N.; Zuercher, E.; Carron, T.; Chinet, L.; Bugnon, O.; Berger, J.; Peytremann-Bridevaux, I. Interest in and use of person-centred pharmacy services—A Swiss study of people with diabetes. BMC Health Serv. Res. 2021, 21, 216. [Google Scholar] [CrossRef]
- Cavaco, A.M.; Dias, J.P.; Bates, I.P. Consumers’ perceptions of community pharmacy in Portugal: A qualitative exploratory study. Pharm. World Sci. 2005, 27, 54–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Ung, C.O.L.; Chi, P.; Wu, J.; Tang, D.; Hu, H. Consumers’ Perceptions About Pharmaceutical Care Provided by Community Pharmacists in China in Relation to Over-the-Counter Drugs: A Qualitative Study. Inquiry 2018, 55, 46958018793292. [Google Scholar] [CrossRef] [PubMed]
- Mehralian, G.; Sheikhi, S.; Peiravian, F. Diabetic Patients’ Views on Services Provided by Community Pharmacies. J. Pharm. Health Serv. Res. 2018, 9, 335–340. [Google Scholar] [CrossRef]
- Spadea, T.; Onorati, R.; Baratta, F. Monitoring adherence to pharmacological therapy and follow-up examinations among patients with type 2 diabetes in community pharmacies. Results Exp. Italy. 2021, 16, e0256478. [Google Scholar] [CrossRef]
- Wang, J.; Pei, Y.; Yu, F. Understandings, Attitudes, and Barriers About Diabetes Care: Analysis of Factors Influencing Community Pharmacists in China. Diabetes Metab. Syndr. Obes. Targets Ther. 2021, 14, 1999–2009. [Google Scholar] [CrossRef]
- Presley, B.; Groot, W. Pharmacists’ and patients’ perceptions about the importance of pharmacist services types to improve medication adherence among patients with diabetes in Indonesia. BMC Health Serv. Res. 2021, 21, 1227. [Google Scholar] [CrossRef]
- Fialko, L.; Garety, P.A.; Kuipers, E.; Dunn, G.; Bebbington, P.E.; Fowler, D.; Freeman, D. A large-scale validation study of the Medication Adherence Rating Scale (MARS). Schizophr. Res. 2008, 100, 53–59. [Google Scholar] [CrossRef]
- Presser, S.; Couper, M.P.; Lessler, J.T.; Martin, E.; Martin, J.; Rothgeb, J.M.; Singer, E. Methods for Testing And Evaluating Survey Questions; Wiley: Hoboken, NJ, USA, 2004; pp. 1–22. [Google Scholar]
- Awad, A.; Waheedi, M. Community Pharmacists role in obesity treatment in Kuwait: A cross-sectional study. BMC Public Health 2012, 12, 863. [Google Scholar] [CrossRef] [Green Version]
- Elnaem, M.H.; Nuffer, W. Diabetes care and prevention services provided by pharmacists: Progress made during the COVID-19 pandemic and the need for additional efforts in the post-pandemic era. Explor. Res. Clin. Soc. Pharm. 2022, 6, 100137. [Google Scholar] [CrossRef] [PubMed]
- Stergachis, A.; Maine, L.L.; Brown, L. The 2001 National Pharmacy Consumer Survey. J. Am. Pharm. Assoc. 2002, 42, 568–576. [Google Scholar] [CrossRef] [PubMed]
- Wirth, F.; Tabone, F.; Azzopardi, L.M.; Gauci, M.; Zarb-Adami, M.; Serracino-Inglott, A. Consumer perception of the community pharmacist and community pharmacy services in Malta. J. Pharm. Health Serv. Res. 2011, 1, 189–194. [Google Scholar] [CrossRef]
- Eades, C.E.; Ferguson, J.S.; O’Carroll, R.E. Public health in community pharmacy: A systematic review of pharmacist and consumer views. BMC Public Health 2011, 11, 582. [Google Scholar] [CrossRef] [Green Version]
- Farris, K.B.; Fernandez-Llimos, F.; Benrimoj, S.I. Pharmaceutical care in community pharmacies: Practice and research from around the world. Ann. Pharmacother. 2005, 39, 1539–1541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kharjul, M.; Braund, R. The influence of pharmacist-led adherence support on glycaemic control in people with type 2 diabetes. Int. J. Clin. Pharm. 2018, 40, 354–359. [Google Scholar] [CrossRef]
- Presley, B.; Groot, W.; Pavlova, M. Pharmacy-led interventions to improve medication adherence among adults with diabetes: A systematic review and meta-analysis. Res. Soc. Adm. Pharm. 2019, 15, 1057–1067. [Google Scholar] [CrossRef]
- El Hajj, M.S.; Mekkawi, R.; Elkaffash, R.; Saleh, R.; El Awaisi, A.; Wilbur, K. Public attitudes towards community pharmacy in Arabic speaking Middle Eastern countries: A systematic review. Res. Soc. Adm. Pharm. 2021, 17, 1373–1395. [Google Scholar] [CrossRef]
- Roborel de Climens, A.; Pain, E.; Boss, A.; Shaunik, A. Understanding Reasons for Treatment Discontinuation, Attitudes and Education Needs Among People Who Discontinue Type 2 Diabetes Treatment: Results from an Online Patient Survey in the USA and UK. Diabetes Ther. Res. Treat. Educ. Diabetes Relat. Disord. 2020, 11, 1873–1881. [Google Scholar] [CrossRef]
- Jimmy, B.; Jose, J. Patient medication adherence: Measures in daily practice. Oman Med. J. 2011, 26, 155–159. [Google Scholar] [CrossRef]
- DiMatteo, M.R.; Haskard, K.B.; Williams, S.L. Health Beliefs, Disease Severity, and Patient Adherence: A Meta-Analysis. Med. Care 2007, 45, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Caetano, I.; Santiago, L.M.; Marques, M. Impact of written information on control and adherence in type 2 diabetes. Rev. Da Assoc. Med. Bras. 2018, 64, 140–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type 2 Diabetes Respondents | Number (%) |
|---|---|
| Gender | |
| Male | 109 (55.6%) |
| Female | 87 (44.4%) |
| Age | |
| 18–30 | 3 (1.5%) |
| 31–45 | 30 (15.3%) |
| 46–60 | 86 (43.9%) |
| 61–70 | 77 (39.9%) |
| Place of residence | |
| Country side | 30 (15.3%) |
| City center | 147 (75%) |
| Village | 19 (9.7%) |
| Level of education | |
| Elementary | 36 (18.4%) |
| High school (intermediate) | 98 (50%) |
| College or higher | 62 (31.6%) |
| Duration of diabetes disease | |
| Less than 6 months | 22 (11.2%) |
| More than 6 month | 174 (88.8%) |
| Family member had diabetes | |
| Yes | 144 (73.5%) |
| No | 52 (26.5%) |
| Any complications of diabetes | |
| Yes | 122 (62.2%) |
| No | 74 (37.8%) |
| Questions | Yes (%) | No (%) |
|---|---|---|
| Daily medication is a problem for many. Is this a problem for you in your everyday life? | 71 (36.2%) | 125 (63.8%) |
| Do you often forget to take your medication? | 49 (25%) | 147 (75%) |
| Is your doctor advising you to take anti-diabetic medicines for your diabetes? | 195 (99.5%) | 1 (0.5%) |
| Have you stopped taking your diabetes medicine(s) because you are suspected of feeling ill from taking this medicine(s)? | 25 (12.8%) | 171 (87.7%) |
| Have you stopped or discontinued your diabetes medication(s) because your condition has not improved and you are discouraged from taking this medication(s)? | 37 (18.9%) | 159 (81.1%) |
| When you feel that your diabetes is in balance, do you stop taking the medicine(s) for your diabetes? | 43 (21.9%) | 153 (78.1%) |
| Do you stop taking your diabetes medicine(s) if your friend/relative/neighbor is taking the same medicines as you and has experienced any side effects? | 35 (17.9%) | 161 (82.1%) |
| Is it a problem to ask GP about the drug therapy of diabetes? | 9 (4.6%) | 187 (96.9%) |
| Is it a problem to ask the pharmacist about the drug therapy of diabetes? | 19 (9.7%) | 177 (90.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Assaf, S.; Kleiner, D.; Zelkó, R.; Hankó, B. Type 2 Diabetes Patients’ Views of Local Pharmacists and Fulfilment with Pharmaceutical Diabetes Care in Syria’s Latakia Governorate: An Online Survey Research. Healthcare 2023, 11, 1720. https://doi.org/10.3390/healthcare11121720
Al Assaf S, Kleiner D, Zelkó R, Hankó B. Type 2 Diabetes Patients’ Views of Local Pharmacists and Fulfilment with Pharmaceutical Diabetes Care in Syria’s Latakia Governorate: An Online Survey Research. Healthcare. 2023; 11(12):1720. https://doi.org/10.3390/healthcare11121720
Chicago/Turabian StyleAl Assaf, Sarah, Dénes Kleiner, Romána Zelkó, and Balázs Hankó. 2023. "Type 2 Diabetes Patients’ Views of Local Pharmacists and Fulfilment with Pharmaceutical Diabetes Care in Syria’s Latakia Governorate: An Online Survey Research" Healthcare 11, no. 12: 1720. https://doi.org/10.3390/healthcare11121720